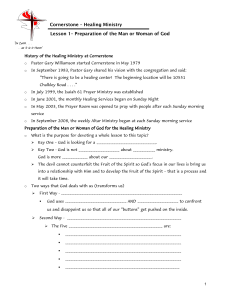
Send Orders for Reprints to [email protected] Endocrine, Metabolic & Immune Disorders-Drug Targets, 2022, 22, 911-926 911 REVIEW ARTICLE Advancement in Nanoformulations for the Management of Diabetic Wound Healing Shailendra Singh Bhadauria1 and Rishabha Malviya1,* 1 Department of Pharmacy, School of Medical and Allied Sciences, Galgotias University, Greater Noida, Uttar Pradesh, India ARTICLE HISTORY Received: July 6, 2021 Revised: December 1, 2021 Accepted: January 7, 2022 DOI: 10.2174/1871530322666220304214106 Abstract: People with diabetes have a very slow tendency for wound healing. Wound healing is a vast process where several factors inhibit the sequence of healing. Nano-formulations play a major role in acute and chronic wound healing. The present manuscript aims to discuss the role of nanoformulations for diabetic wound healing treatment. Diabetes is a common disease that has harmful consequences which over the time lead to serious damage to many of the body's systems, especially the nerves and blood vessels. During the literature survey, it was observed that nanotechnology has significant advantages in the treatment of diabetic wound healing. The present manuscript summarized the role of nanomaterials in wound healing, challenges in diabetic wound healing, physiology of wound healing, limitations that come during wound repair, and treatments available for wound healing. After a comprehensive literature survey, it can be concluded that health worker needs more focus on the area of wound healing in diabetic patients. Medical practitioners, pharmaceutical, and biomedical researchers need more attention towards the utilization of nano-formulations for the treatment of wound healing, specifically in the case of diabetes. Keywords: Nano-formulation, diabetic wound healing, nanomaterial, diabetes, patient care, drug delivery. 1. INTRODUCTION Diabetes is usually associated with diet and the gastrointestinal system. This disease causes consequences during wound healing with significant clinical problems when left untreated. Diabetic wounds are characterized by excessive inflammation, which damages healthy tissue and prevents effective immune response as well as a healing process [1]. Patients suffering from diabetes are also much more vulnerable to an open wound in their lower extremities due to peripheral neuropathy associated with type II diabetes [2]. There are currently 35 million patients with type II diabetes in the United States, which is expected to rise to 55 million by 2030 [3]. IDF DIABETES ATLAS 9th issue 2019 provides contemporary information about diabetes. Diabetes affects nearly 463 million people (20-79 years old) worldwide, and this figure is expected to rise to 700 million by 2045. 79% of people with diabetes live in lower and middle-income countries. One out of five patients over 65 years of age suffer from diabetes. 1 or 2 out of 232 million patients with diabetes have not been diagnosed. 4.2 million deaths have been reported due to diabetes. The minimum amount spent for the treatment of diabetes in 2019 was 760 billion USD, 10 % of the total expenditure *Address correspondence to this author at the Department of Pharmacy, School of Medical and Allied Sciences, Galgotias University, Plot No. 2, Sector 17A, Greater Noida, Uttar Pradesh, India; Tel: +91-9450352185; E-mails: [email protected], [email protected] 1871-5303/22 $65.00+.00 for adults. Upwards of 1.1 million children and young adults have type 1 diabetes, over 20 million natively (1 in 6 natively) are affected by diabetes during pregnancy, with 374 million patients at higher risk for developing type II diabetes [4]. Diabetic wounds are also linked to increased complications, gangrene, and amputation, including higher rates of infection [5, 6]. Throughout diabetic conditions, impaired wound healing has also been attributed to the deterioration of several physiological processes, including keratinocyte and fibroblast migration and proliferation, angiogenesis, collagen accumulation, growth factor production, epidermal barrier function, and extracellular matrix (ECM) production and remodeling imbalances [7]. The dysfunctional reaction by macrophages, the main initiators, and arbitrators of wound healing, are also linked to the impaired progression of wounds in the diabetic state [8]. Fig. (1) represents a comparison between normal wound healing and diabetic wound healing. 2. NANOMATERIALS USE FOR WOUND HEALING As the researcher explained, wound healing had a serpentine 4-stage process that involved hemostasis, inflammation, proliferation, and remodeling. The rationality of any substance was relevant to the process as well as the duration of its therapeutic effect, dose, and mechanism of action. Various nano-based perspectives examine the application for wound healing. Researchers have made an effort to develop products that come up with humid circumstances and have antibacterial activity. Diversification with natural or synthetic materials or © 2022 Bentham Science Publishers 912 Endocrine, Metabolic & Immune Disorders-Drug Targets, 2022, Vol. 22, No. 9 Bhadauria et al. Fig. (1). Comparison between normal and diabetic wound. (A higher resolution/colour version of this figure is available in the electronic copy of the article). their amalgamation has also been put together for specific pathways of wound healing. Herein, natural polymers have been applied generalship due to their important biological functions and innumerable wound healing. Collagen is considered as a visionary healing scaffold with a superlative condition and moderately strong mechanical properties, a fundamental clot that reduces bleeding like silk fibroin was used due to its structural strength. Keratin is another example that is widely used to treat wounds with nanomaterials. The nanomaterials are used due to their potential to encourage a selfhealing framework that may imitate reincarnation. However, the variety of wounded tissues requires a thorough understanding of the mechanics influencing these nanomaterials and their cell cascade for different wound-healing applications. Nanoparticles can be used efficiently in this field of research because of their superior surface-to-volume ratio. Metal nanoparticles such as gold, silver, and zinc possess excellent movables, along with wound healing activation and antibacterial activity trying to make them ideal for assimilation into wound dressings [9]. Table 1 describes the multiple types of nano-formulations used in wound healing and their properties. Fig. (2) represents various types of nanomaterials used in diabetic wound healing. Fig. (2). Various nanomaterials used for the wound healing. (A higher resolution/colour version of this figure is available in the electronic copy of the article). Table 1. Multiple types of nano-formulations with their properties are summarized. Nano-Formulation Properties Nano-scaffolds Mimic the properties of extracellular matrix (fibrous nature and nanoscales features) Nanofibers Create favorable conditions for cell attachment and cell drug interaction by replacing artificial dermal analogs Other Lipid particles Controlled drug release and versatility of administration Liposomes Provide sustained drug release and a moist environment on the wound surface. Polymeric particles Prevent drug release and ensure controlled release against wound protease degeneration. Inorganic nanoparticles Its intrinsic property displays similar benefits and strong antibacterial effects in wound healing treatment. Silver nanoparticles can regulate the release of anti-inflammatory cytokines and encourage fast injury closure without increasing scarring. The propagation of keratinocytes can also stimulate epidermal reepithelization [10]. Gold nanoparticles (AuNPs) have the ability to promote cures and inhibit microbial colonization. However, at lower AuNP concentrations, they can stimulate keratinocyte growth and differentiation [11]. Zinc oxide nanoparticles (ZnONPs) are effective anti-bacterial agents modulating the perforation of the bacterial cell membrane in hydrogel-based wound dressings. [12]. Overall, time is increased and keratinocyte migration is endorsed and re-epithelialization is therefore improved [10]. Throughout the relationship, even the delivery of the wound dressing vectors has potent antimicrobial and epithelial properties for polymeric nanoparticles (for example, hyaluronic Advancement in Nanoformulations Endocrine, Metabolic & Immune Disorders-Drug Targets, 2022, Vol. 22, No. 9 913 ácid, Chitosan, Cellulose, Alginate). Alginate absorbs water and produces moist alginate easily. Wound conditions also limit wound identification [13]. Due to its hygroscopic nature, Hyaluronic acid controls cell adhesion or adhesion during wound healing [14]. An interpretation of the vascular endothelial growth factors has been significantly enhanced by endothelial cell proliferation, motility, and angiogenesis [15]. Cellulose triggers the closure of the wound by several growth factors, including the epidermal growth factor or the local release of the fundamental fibroblast growth factor [10]. The postulant is also completely comprehensive in polyurethane, PLGA, PCL PEG, and PLA. Eventually, there may be another alternative to produce wound scaffolds that imitate the qualities of the extracellular matrix. Nanofiber polymers can also focus on the improvement of fibroblast adhesion on wounds with their development [12]. Different types of nanoparticles are described below. 2.1. Organic Nanomaterials 2.1.1. Micelles In a hydrophobic inner core, micelles have been circumambient by an aqueous hydrophilic shell, creating respectively hydrophilic or hydrophobic agents. Contemporary polymer micelles have ideal colloidal stability, high load capacity, biocompatibility, toxicity, and controlled drug release [16]. Curcumin-loaded hydrogel related to PEG-PCL hydrogel exists in both linear and full-thickness wound models with blank (13.3 ± 2.9 mg-1) and control (11.3 ± 1.8 mg -1) administered in mice. They show significantly higher granulation (4.17 ± 0.41) and wound strength of character in mice with the linked PEG-PCL hydrogel (22.4 ± 2.2 μg−1) than the curcumin-loaded (Cur-M) (16.9 ± 2.3 μg mg−1) and control (11.3 ± 1.9 mg−1) [17]. The encapsulation of silver sulfadiazine in chitosan oleate micelles was also a copy. The connection demonstrated throughout the personification that not only drug levels surface-to-volume ratios and dispersions were enhanced, while the drug concentrations were also increased. It is also intended to prevent the cytotoxic effects of the drug by coating human cells without affecting its antimicrobials properties. Researchers proved that silver sulfadiazine micelles augmented the antimicrobial activity against Staphylococcus aureus and Escherichia coli strains (with MIC values of 50 μg mL−1 and 25.8 50 μg mL−1, respectively) compared to the control suspension (150 50 μg mL−1 for S. aureus and 37.5 for S. aureus) 50 μg mL−1 E. coli [18]. Curcumin-loaded anti-diabetes and injury therapeutic properties of chitosan-based mixed polymeric micelles, alginate-maltodextrin, pluronic F127, P123, and Tween-80 were also reviewed recently through studies in diabetic rats. These have come to an end that perhaps formulations prosper with the highest curcumin levels (over 48, 74 ppm) can stimulate wound healing response, demonstrating significant improvements in wound closure on the 14th day, lowering aerial blood glucose or lipid profile, clearly demonstrates its potential as a diabetes-controlling and wound healing agent [19]. Another auspicious example is PluroGel R focusing mostly on technology, including its micelle matrix, made up of a cell-friendly surfactant, and claims to maintain humid content of the wound which control the loss of fluids, that helps in the protection of the wound injury and allowing slighter painful removal [16]. 2.1.2. Polymeric Nanoparticles Polymeric nanoparticles also consists of biodegradable polymers and copolymers, to which drug can dissolve, trap, encapsulate or attach. The polymers are composed of natural, synthetic, and semi-synthesized polymers such as gelatine, albumin, alginate, chitosan, poly (glycolic acid), and their copolymers (PLGA). It provides the advantage of controlled and sustainable release, high encapsulation levels, increased bioavailability, and biocompatibility of cells and tissue [16]. So many interpretations of polymeric NPs in wound healing are given in the literature. For example, in the thickness of the excisional model, granulation tissue (LL37 activates epidermal cellulose), re-epithelial composition (IL-6), augmented angiogenesis (triggered by the production of VEGFα via upregulation with IL-6) (LL37) and lactate encapsulated with PLGA NPs exhibited greater wound healing property in the mice treated with host protective peptide. In addition, PLGALL37 NPs encoded the inflammatory reaction in the macrophages of the mouse, using the down-regulation aspect of TNF5-007 [20]. Amphotericin B was implemented in the silane-hydrogel nanoparticle vehicle which helps in slaying the effectiveness against Candida. The untreated control and traditional formulation groups were reduced by 72.4-91.1%. Furthermore, wounds treated with amphotericin B nanoparticles significantly decrease the metabolic activity of the fungal biofilm from 80 to 95% [21]. 2.1.3. Dendrimers Dendrimers were synthesized from a radially derived branch of monomers from the central core [22]. The effectiveness of VEGF-coding minicircle plasmid DNA was assessed for wounds on diabetic mice in combination with arginine (Arg)-grafted cationic dendrimer [23]. This results in the polycomplex injection which has managed to heal wounds faster in rapidly sprouting basal cells and abundant deposition of collagen compared to the bare plasmid VEGF. Polyamidoamine (PAMAM) gelatin skin (PAMAM) has also shown relatively high gelatin levels, increased cell adhesion, keratinocyte proliferation, and fibroblasts with increased fibroblast type I gene expression which was correlated with native collagen type. Furthermore, interpretation for angiogenesis modulators such as HIF1 alfa and VEGF was higher in the PAMAM blended gelatin matrix [24]. 2.1.4. Nanoemulsions Nanoemulsions are colloidal type system that consists of emulsified oil and water systems that holds poorly water-soluble drugs dispersed within them. Nanoemulsions are now widely used in cosmetic applications [16]. As drug delivery carriers, they have a high ability to load drugs, also have the capability for improving drug solubility and bioavailability. The main benefits of nanoemulsions as drug suppliers are that they are comparatively simple in preparation and escalation; they also regulate the release of drugs and provide safety from enzyme degradation [16]. In a study, Barroso et al. discussed that after 36 hr of phenytoin-charged alkyd nanoemulsions administration producing 25 and 50 mg of phenytoin mL−1, there had been improvement 914 Endocrine, Metabolic & Immune Disorders-Drug Targets, 2022, Vol. 22, No. 9 in closure activity by creating a 75-82 % "scratch zone" related to phenytoin-concentration solutions [9]. Concentrationup released property help in the maintenance of the optimal level of phenytoin for keratinocyte cell growth [25]. In another study, wound healing outcomes of Eucalyptus Essential Oil (EEO) nanoemulsion formulations were compared to pure EEO and regular gentamycin. Comparable findings were seen during the treatment with the normal gentamycin-optimized formulations. But the quality of the collagen was greatly increased as compared to pure EEO. The EEO nanoemulsion increased the injury contraction substantially from day 12 to 24 to control (P<0.05) [26]. 2.1.5. Liposomes Liposomes are nano-sized vehicles that embrace an inner aqueous compartment enclosed by bilayer phospholipids. Liposomes are healthy, biodegradable, non-toxic, biocompatible, and capable of encapsulating water-soluble as well as lipophilic substance. The most common disadvantages of liposomes are their low stability due to oxidation, hydrolysis of phospholipids, as well as leakage and fusion of embossed drug molecules [27]. Fibroin hydrogel core-based BFGFloaded liposome showed improvement in the strength and acceleration of the BFGF in wound fluid by facilitating the formation of granulation tissue, collagen deposition, angiogenesis, re-epithelialize [28]. In a study, Barroso et al. discussed the advantages of topical application compared to the drug itself and curcuminloaded liposomes [9]. In a study on rats, liposomes containing curcumin improved wound closure on the 14 th day after the lesion was opened (93.67 ± 3.56%), (P ± 0.05) [29]. The recent evidence suggests that the synergistic effect of dual liposomal ointment contains retinoic acid (RAD) and cationic deformable EGF liposomes which help in cell proliferation, migration, stimulated wound closures, enhanced appendix skin formation, and increased collagen development. They also demonstrate the synergistic effect of TRA, which is caused by increasing the expression of EGF and HB-EGF recipients [30]. The use of composite liposome scaffold systems to treat wounds has recently been studied depending on the therapeutic value of liposomes and the mechanical strength of scaffolds [31]. 2.1.6. Other Lipid-Based Nanoparticles Nanostructured lipid carriers (NLCs) and solid lipid NPs were developed as possible alternatives [32]. The preparation of NLCs with phenytoin was described in a previous study. This study aimed at increasing the effectiveness of drug trapping and the continuous release of drugs in the treatment of Diabetic Foot Ulcers (DFU) [33]. Results demonstrate that after administration of phenytoin hydrogel NLC (0.26 ± 0.22 cm2) the wound surface was lowered as compared to the PHThydrogel (0.25 ± 0.89 cm2) and blank (7.24 ± 3.65 cm2). The medicinal potential of topical essential rosemary oil (REO) was started in another study. The infected wound was treated by NLCs. The REO-NLC shows their antibacterial activity against the epidermis of S. aureus, monocytogenes steria. The MIC values for E. coli, Pseudomonas aeruginosa ranged from 5.34 ± 1.7 to 10.13 to 1.67 mg mL−1. In addition, IL-3, IL-10, Bhadauria et al. and VEGF (P < 0.001), neovascularization (P < 0.05), infiltration by fibroblast, collagens deposition and re-epithelization were increased simultaneously [34]. Similarly, assessments of the curcumin and ampicillin SLN semi-solid formulations as burn wound healing agents were performed in in vitro and in vivo studies. Semi-solid formulations simultaneously increased the wound treatment rate with the use of the synergistic effects of ampicillin and provided better antibacterial effects [35]. Diabetic wound mice played an important role in the assessment of abnormal and regulated healing processes, whereas overproduction of TNF-α can reduce chronic inflammation and promote wound closure. Researchers also examined the siRNA-loaded lipids for wound healing purposes. The topical application of TNF-α causes gene silencing of approximately 50%, nearly approaching traditional baseline levels of normal glycemic mice, resulting in a reduced wound area and a quicker closure within 13 days [36]. 2.2. Inorganic Nanomaterials 2.2.1. Magnetic Nanoparticles Magnetic NPs such as magnetite (Fe3O4) were used due to their distinctive characteristics i.e. magnetic field susceptibility [37]. Surface modifications of magnetic NPs have been thoroughly examined in the medical field [38]. To analyze the effect on Candida albicans, colonization rates and biofilm development of nano-coated wound dressings containing magnetite NPs were studied and the results showed that it strongly inhibits fungal adherence [39]. Smililarly, the timber-based Fe3O4 NPs dressing inhibition efficacy has been also demonstrated [40]. 2.2.2. Silica Nanoparticles Studies revealed the controlled oxidation rate of silica nanoparticles which occurs due to its vital component, in addition to its antimicrobial, in inflame, cell proliferation, ECM deposition, geosynthetics, and reshaping of matrix properties [12]. The higher antimicrobial effect against P. aeruginosa and E. coli was shown by NO-releasing silica (SiO2) NPs (with ~5 killing logs for both Gram-negative species) while optimal efficiency to discourage C. Albicans (3 biofilm destroying logs) and biofilm showed the lowered efficacy against gram-positive bacteria such as S. aureus, and S. epidermidis (2 biofilm bacteria logs) [41]. Further research has revealed the effects of silica NPs as sources of silica acid on the proliferation and migration of fibroblasts. According to the researchers, fibroblasts are easily internalized in silica NPs (charged positively), resulting in the silica-acid intracellular release. Molecules also stimulate the migration of cells and gradually help in wound healing [42]. The efficacy of hydrophilic chitosan-silica hybrid sponge not only promotes proliferation, migration, endothelial cell proliferation but also helps in secretion. Growth factors like TGF-β in a porcine model show improved deposition in collagen and angiogenesis [43]. With the murine model, nanostructured PVP (polyvinylpyrrolidone) gel SiO2 resulted in increased cell proliferation and cell migration (due to moisture), advanced 9-day reepithelization (652.9 ± 142.6 vessels/mm2 vs. 489.3 ± 207 vessels/mm3). Advancement in Nanoformulations Endocrine, Metabolic & Immune Disorders-Drug Targets, 2022, Vol. 22, No. 9 915 3. THE WOUND HEALING PROCESS AND WOUND CATEGORIES skin [61, 62]. Figs. (3 and 4) represent various factors involved in acute and chronic wound healing factors, respectively. 3.1 Wound Categories The skin break or abnormalities caused by injuries or by any physiological/medical conditions are known as wounds. Damage of the skin and loss of it’s physiological functions often occur under these circumstances. In general, the wounds come under two categories: acute wounds and chronic wounds; acute wounds are caused by mechanical injuries or exposure to intense warmth, irradiation, electric shock, chemical agents. These wounds recover in a very short period if adequate wound care is utilized [32, 44, 45]. Chronic wounds usually cause complications for certain particular illnesses, such as diabetes, which are well-known for the horrific occurrence of ulcers. These injuries need a longer time for healing and may become critical if not treated properly [45]. Wounds can be divided into three different wound depths: surface wounds (with only a portion of the epidermis), partial thick wounds (with epidermis and deeper skin layers), and subcutaneous wounds (with epidermis) (subcutaneous fat and deeper tissue are disrupted) [46]. 4. CHALLENGES IN DIABETIC WOUND HEALING Despite significant progress in the last 25 years, extreme assessment of diabetic foot ulcers (DFUs) will be performed in the future. The mean time in the healing of a diabetic wound 3.2. Wound Healing Process Wound cure involves various cells, mediators, extracellular (ECM) elements, development factors, and proteinases. It's a physiological complex and dynamic process [47]. In particular, the disease can be divided into three interlaced phases: inflammation, proliferation, re-epithelial/remodeling [48, 49]. The inflammatory cycle usually lasts for 2-5 days after skin injury. If there is an accident, intravascular platelets cause the hemostasis to form coagulation and minimizing bleeding immediately [50]. Platelet thrombin is also triggered to release several growth factor factors, including EPD, IG F-1, PDGF, Fibroblast growth factor (FGF), TgF-α, and TGF-β (TGF). In addition, activation of the platelet activates the thrombin and leads to the release of several growth factors [51, 52]. Growth factors were dispersed into the injured tissue and it is also served as biological signals to attract, further, mediate inflammation and protect the skin from infection. [53, 54]. In proliferation, it generally takes 3 to 2 days to complete cell proliferation and migration [55]. Approaching new blood vessels or capillaries gradually, proangiogenic factors such as PDGF released by platelets encourages the inflammatory cells in the wound region [56]. Stimulation of PDGF and FGF causes the relocation of fibroblasts from inflammatory cells to granulated tissue concurrently with angiogenesis [57, 58]. With fibroblast accumulation and proliferation new ECMs consisting of collagen, proteoglycans and elastin are produced. So many fibroblasts become a myofibroblast and play an important role in the contraction of the injury area [59]. Additionally, activate the keratinocytes to fully re-epithelialize and relocate into wounded areas [60]. The re-epithelialization and restructure post-injury process ranges between three weeks to one year. In the newly synthesized ECM, collagen III is slowly replaced by collagen I. The newly produced collagen fibers become more orderly structured in the grid and increase the tensile strength in the cured Fig. (3). Factors involved in the acute healing process. (A higher resolution/colour version of this figure is available in the electronic copy of the article). Fig. (4). Factors involved in the chronic healing process. (A higher resolution/colour version of this figure is available in the electronic copy of the article). 916 Endocrine, Metabolic & Immune Disorders-Drug Targets, 2022, Vol. 22, No. 9 without treatment is approximately 12 weeks, and the risk of amputation is high [63, 64]. After a new DFU, the five-year survival rate is 50%-60% worse than many common cancers [64, 65]. Although there is data showing cardiovascular risk reduction [65], the latest statistics from a Veteran healthcare administration show that only 81%, 69%, and 29 % of the population lived for 1 to 2 and 5 years, respectively. Mortality was larger than any macrovascular disease in the correlation between DFU [66, 67]. Iversen et al. found that even 10 years later, the incidence of a DFU was just an independent mortality indicator [67]. There are still huge prices for wound healing charged by hospitals. Till 2015, diabetes damage management is projected to up to $1.3 billion globally [68]. And up to one-third of expenses on diabetes have also been diagnosed in the United States for lower limb-related problems [69]. The most up-to-date statistics from the UK estimate that the gross annual management costs in respect of DFUs surpass 1 billion pounds (1.32 billion dollars) [70]. 5. TREATMENT STRATEGIES FOR DIABETIC FOOT ULCERS 5.1. Main Preventive Measures-Elimination of Recent DFUs The occurrence of ulcers is quite small in the population. Selected populations of patients suffering from diabetes in the United States, the total incidence is recorded i.e. 5.8 and 6.0% [71-73]. While fewer chosen populations in Europe have been recorded the incidences of Type 2 diabetes are solitary i.e. 2.1% and 2.2 % [74, 75]. The effects of early diabetes screening are unknown, but a shorter decline in early diabetes from total local diabetes populations can be expected. However, the number of DFUs will continue to fall, which will grow in line with the global type 2 diabetes epidemics without causing any significant changes to ulcer prevention. The several risk factors for the development of ulceration have been well recognized [76], there is no consensus on which to prevail, and no studies report currently justifies the adoption of any particular primary prevention for the population selection strategy. In this study, however, the achievement of various measurement systems has been compared [77]. Although the incidence of new skulls may be minimized through the possibility and anticipation of foot care education, the evidence for the use of any elementary education measures is weak, there were just a limited number of RCTs reported, while high-quality benefits were not reported in randomized controlled trials [78, 79]. The cumulative incidence of primary preventive trials with diabetes in unselected populations with new foot ulcers is relatively low [80]. 5.2. DFU Inability to Cure Promptly the First Expert Assessment State of DFU The severe ulceration has a poor prognosis and this is the basis of existing assessment schemes [63, 80, 81]. There is also a statistically significant correlation between recent data [82, 83]. 5.3. The Connection between DFU and Renal Failure There is a similar temporal association between foot ulceration and the beginning of dialysis for renal end-stage disease Bhadauria et al. [84, 85]. While ulceration can be believed in such cases that it has resulted from the degradation of renal function, the final decline in renal function is equally and potentially more likely to be caused by ulceration inflammations [86]. After major amputation, the mortality rate was also 290% higher for dialysis patients. These observations were more commonly observed by nephrologists [87]. 5.4. Recent Ulceration after the Healing Process The ulceration treatments rate is high, with 40% of patients developing new ulcers (on or on the same site) during 12 months. This is an important characteristic of diabetic foot disease as foot disorders should not be considered cured but treated in remission if the ulcer recovers [69]. In this respect, the diabetic foot is directly linked to malignancy. Therefore, the person whose foot is in remission should follow the same structure as everyone who is in remission after cancer therapy. This long-lasting need for expert monitoring should undoubtedly be given more attention from all DFU management fields. The recent DFU surveys may decrease the need for RCTs relatively, but with the highest possible short-term incidence of persistent ulcers, the long-term benefit for both patients and the health professional may be very high. 5.5. Strategies that Reduced Diabetic Foot Ulcer Recurrence Apart from the availability of suitable footwear, a focused target is considered an integral part of secondary prevention for patients with (particularly) plantar ulceration. However, there is conclusive evidence of its effectiveness [88]. In comparison, a single group recorded three studies to show how the foot skin temperature was tracked every day while no other organizations have verified the approaches yet [89]. 6. THE PROBLEM OF WOUND HEALING AND ITS PHENOMENON IN DIABETES The result of the pathophysiological interaction of diabetic impairment includes vascular, neuropathic, immune, and biochemical [90]. Blood vessels and microvascular dysfunction reduces tissue oxygenation, which is associated with hyperglycemia [91]. Diabetic vessel alterations also result in minimization of the relocation of leucocyte to the wound, which is more susceptible to infections that can affect leucocyte function. Peripheral neuropathy can also cause area numbness which results in chronic wounds. This is not detected immediately and lower limbs are treated, particularly the foot, which is more exposed and chronically vulnerable to minor lesions. Modifications to the motor and sympathetic functions also cause a deformation of the physical foot, increased plantar pressure, and unnoticed skin dryness [90]. The chance of diabetic foot ulcers is 15-25% across their lives; 40-80% of people are affected so badly that it involves the bones [92]. Worldwide epidemiological studies show that North America is more dominant in the disease [93]. A large number of incidents of foot ulceration require hospitalization and surgical procedure to separate the concerned body part. Furthermore, after 3 years from the first episode, the recovery rate of a foot ulcer is more than 50% [94]. That is why DM- Advancement in Nanoformulations Endocrine, Metabolic & Immune Disorders-Drug Targets, 2022, Vol. 22, No. 9 917 impaired wound cure is the main health issue and a major economic burden [95, 96]. Wound healing is a physiological process where the integrity of the skin is removed and the barrier function of the skin is affected as well. This can occur very frequently because the skin is exposed to external offenses and a fast defense system is needed to prevent systemic infections [97]. The normal state of the skin is completely recoverable by physiological healing, it only achieves up to 70% of the previous strength of the tensile [62]. The process proceeds in several subsequent phases. Inflammatory, proliferative, and remodeling phases are usually recognized by three successive phases. 6.1. Inflammatory Response The inflammatory stage is preceded by a coagulation stage, which is the first response of the injured skin by activating the coagulation cascade with the recruitment and formation of a fibrin plug [56]. Weathering is also important for the treatment. Additional clot platelets form a basis for the recruitment of inflammatory cells, which are attracted by various cytokines, including PDGF (platelet-based growing factor) and TGF, and attract different types of cells (transforming factor of growth). Neutrophils and monocytes are present and supported by simultaneous vasodilatation. Later, macrophages occur at a very early stage and through the release of growth factors and cytokines, they are considered major contributors to this inflammatory stage. There is a migration of keratinocytes in the injured region which causes a rise in local fibroblasts [98]. These events occur soon, after a few hours of the wound occurrence, and are rapidly help in the formation of the tissue within 48-72 hr, including all types of recruited early granulation tissue [99]. 6.2. Proliferation and Remodeling These steps are intended to assist in the healing of wounds. In this respect, granulated tissue and keratinocyte migration, extracellular matrix formation (ECM) protein formation, as well as myofibroblasts' appearance led to contractedness as one of the primary wound closure events. The main cell type in this phase is fibroblasts, which begin to reconstruct the injured region by releasing collagen. Hypoxia is an instrument that helps in encouraging cell type migration, proliferation, and the release of growth factors that characterizes the former wound healing phases [99]. Hypoxia leads to Hypoxia-inductive factor (HIF)-1α activation and VEGF-A stimulation, which is one of the main target genes in HIF-1α [100]. Endothelial cells, therefore, proliferate actively and are essential to support neo-angiogenesis-based formed tissue. VEGF-A increases the density of the wound and restores the flow of blood that promotes wound healing [101]. Some vessels become durable and mature followed by the recruitment of pericytes, which release vascular and anti-angiogenic factors. The formation of chaotic, abundant vessels characterizes this initial period [102]. For the first time healing is developed by remodeling collagens of type III, to type I (as normal non-injured tissue observed) [103]. The new skin contains neovascularisation [104] and the wound repair method is restored the physiological skin texture [48]. A chronic wound appears when the physiological repair process fails, or an excessive repair occurs through a hypertrophic scar or a keloid. The presence of hypertrophic scars usually implies patient predisposition and occurs temporarily usually within 6 months. Keloids, is a coverage area that extends far beyond original skin damage, is present in patients with genetic disorders, and is permanent. Ulcers also occur in ischemic conditions, which causes a delay in the disease treatment [97]. 7 WHAT ARE THE LIMITATIONS IN DIABETES DURING WOUND REPAIRING? The diabetes healing procedure is usually inflammatory and the antigenic process is disrupted. The number of endothelial progenitors in cells has decreased and the extracellular matrix prescription has become imbalanced. Furthermore, chemical chemokines containing neutrophils and macrophages help in physiological wound repair, which quickly enters the lesion area. The factor of tumor necrosis α (T NFFα) for which the levels will not be increased during the initial inflammation phase of acute repair but will remain at higher concentrations in an injured area over a longer-term [105]. The production of many growth factors in diabetes is affected during the treatment. In injured tissue, insulin levels such as IGF-1 (growth factor-1) and β-Growth (TGFβ) were decreased in both diabetic animals and humans. IGF-1 involves in cell granulation and wound reepithelization [106]. In TGF, angiogenesis and ECM formation are also involved which helps in immune cells, keratinocytes, fibroblasts, and vascular cell formation [107]. However, the equilibrium between the formation and maturation of new vessels is troubled in diabetes. In high-glucose endothelial cells, angiogenesis is dysfunctional and the capillary wound area is insufficient. HIF-1α target genes such as VEGF are being suppressed for their stability and activity [108]. In diabetes animal models, the primary source for VEGF macrophages shows phagocytic activity with disability of the modified phenotype, which leads to failure in tissue repair [8]. As a result, DB/DB mice are compared with the control mice in which the VEGF-A mRNA and protein levels have fallen sharply [109]. An early leaky, misformed vasculature and large local edema is the characteristic of the accelerated closeup of the injury and VEGF-A treatment, which was very obvious until the VEGF-A treatment stopped [110]. The decreasing population of endothelial parent cells in bone marrow results due to dysregulation production in both the proangiogenic and the vascular maturation factors found in diabetes [111]. This causes alterations in angiogenic germs and finally vascular aberrant architecture in diabetic wounds [112, 29]. Diabetes also aids in the healing of the wound's ripening phase. Factors contributing to mature vascular phenotype (for example, Angiopoietin (ANG) 1 and 2 and PDGF) are developed in line with competition [113, 30]. In streptozotocin-induced diabetic mouse table model and DB/DB mouse, the topical application of ANG 1 and PDGF improved wound healing, respectively [113, 114]. Finally, diabetes interferes with ECM regulation, which is developed by metalloproteinase (MMP) and metalloproteinase tissue inhibitors (TIMPs). In diabetic wounds, higher MMP levels were detected, possibly due to the high glycolysis caused by developing MMP and reducing TIMP, which can interfere with the 918 Endocrine, Metabolic & Immune Disorders-Drug Targets, 2022, Vol. 22, No. 9 Bhadauria et al. healing process [115]. In a range of wound treatment phases, MMPs are involved in cell migration through degraded ECM, leukocyte invasion, and multiple cytokines processing to ensure no distortion of the scaffolding structure necessary for correct wound healing, equilibriums between MMPs and TIMPs [116]. Table 2 represents the physiology of insulin in normal patient and diabetic patient [117]. a healthy tissue that helps in the exposure to repair the wounded area [48]. There are many forms of debriding including enzymes based on auto-activation of mechanical or operational fibrin enzymes. This is the most effective way of eliminating and preventing necrotic tissue from spreading. Table 2. Physiology of insulin in the normal population and diabetic patient. The process of dressing the wound in diabetic patient is an important factor represented a Fig. (5). 8.1. Dressings Insulin Phases Physiology of Normal Physiology of Population Diabetic Population Coagulation -> fibrin plug TGF-β, PDGF-> recruitment Inflammatory phase of neutrophils and macrophages Chronic inflammation-> Higher IL-1 β and TNFα Inflammation-> IL-1β growth factors Dysfunction macrophages Migration of fibroblast and keratinocytes Hypoxia-> HIFα-> VEGF-> Neoangiogeneses Proliferative phase Extracellular matrix deposition Decreased angiogenesis Disequilibrium between MMPs and TIMPs -> altered ECM Granulation tissues formation Vascular maturation Decreased pericyte Fig. (5). Schematic representation of dressing in the treatment of diabetic wound healing. (A higher resolution/colour version of this figure is available in the electronic copy of the article). 8.2. Antidiabetic Drugs Treatment of diabetes, especially in a patient suffering from a wound, is a critical step and requires medical supervision (Fig 6). function Collagen remodeling Remodeling phase Reduced vascular Wound edge concentration maturation Migration of fibroblasts and keratinocytes Decreased wound strengthening 8. TREATMENT AVAILABLE FOR WOUND HEALING The normal wound healing procedure involves controlling infection, removal of strain, and preservation of moist wound beds. Infections can also be controlled by debridement. The primary objective is always to prevent infection and clean the area of non-viable tissue in the treatment of chronic wounds. Infections can easily occur as a consequence of loss of inborn blockage in the skin, which can also impair the healing process by pathogens in the area of damaged tissue or debridements, which also allows the cell to migrate and proliferate in Fig. (6). Steps involved in the use of antidiabetic drug use for the treatment of diabetic wound healing. (A higher resolution/colour version of this figure is available in the electronic copy of the article). Advancement in Nanoformulations Endocrine, Metabolic & Immune Disorders-Drug Targets, 2022, Vol. 22, No. 9 919 8.3. Growth Factors Diabetic wound healing can be treated by using growth factors. Fig (7) represents the role and application of growth factors in the treatment of diabetic wound healing. 9.3. Drug Phenytoin. 9.3.1. Effect on Wound Healing Phenytoin has antibacterial activity, proliferation of the fibroblast, granulating tissue enhanced liberating VEGF and angiogenesis activities. 9.3.2. Evidence from Human Studies Enhanced cure for a range of wounds. There are several randomized but methodologically poor clinical trials are available. 9.3.3. Administration The topical administration of Phenytoin [121]. 9.4. Drug Statins. 9.4.1. Effect on Wound Healing Statins have anti-inflammatory, angiogenesis properties. 9.4.2. Evidence from Human Studies Fig. (7). Schematic representation of the role of growth factors used for the treatment of diabetic wound healing. (A higher resolution/colour version of this figure is available in the electronic copy of the article). Mevastatin reverses various changed molecular pathways in ex vivo specimens that are derived from diabetic foot ulcers on the non-healing rim. 9.4.3. Administration Statins were administered topically [122,123]. 9. THE DRUG WHICH HAS A REPARATIVE EFFECT IN IMPAIRED WOUND HEALING 9.5. Drug- β-Blockers 9.1. Drug- DPP-4 Inhibitors 9.5.1. Effect on Wound Healing 9.1.1. Effect on Wound Healing DPP-4 inhibitors have proliferation, angiogenesis, keratinocyte migration wound realigning properties and also possess anti-inflammatory, anti-oxidant, endothelial cell precursor's propagation activity. 9.1.2. Evidence from Human Studies In diabetic patients, it improves wound cure and chronic foot ulcers activity. 9.1.3. Administration Systemic administration of DPP-4 inhibitors [118,119]. 9.2. Drug- Metformin 9.2.1. Effect on Wound Healing β-blockers have proliferation characteristics. 9.5.2. Evidence from Human Studies Data is provided based on the animal study. 9.5.3. Administration β-blockers were administered topically. 9.6. Drug ACE-inhibitors. 9.6.1. Effect on Wound Healing ACE-inhibitors have anti-oxidative properties. 9.6.2. Evidence from Human Studies Data provided based on the animal study. Metformin possesses anti-inflammatory, anti-oxidant, proliferation, ECM organization angiogenesis collagen deposition, and endothelial cell precursor activity. 9.6.3. Administration- 9.2.2. Evidence from Human Studies 9.7. Drug Improved healing in traumatic wounds and ulcers. ACE-inhibitors were administered topically. Estrogen. 9.2.3. Administration 9.7.1. Effect on Wound Healing Metformin was administered topically [120]. Estrogen has angiogenesis and proliferation of keratinocytes properties. 920 Endocrine, Metabolic & Immune Disorders-Drug Targets, 2022, Vol. 22, No. 9 9.7.2. Evidence from Human Studies Data provided based on the animal study. 9.7.3. Administration Estrogen was administered through topical/systemic route. 10. THE APPROACH OF NANOTECHNOLOGY IN WOUND HEALING AND MANAGEMENT 10.1. Nanosensors There are some contemporary gaps in glucose monitoring that how glucose monitoring is implemented. The patient is selected for a separate time point and insulin is administered as necessary within the open-end system to measure the blood glucose concentration. The obstacle is that glucose levels constantly fluctuate in the blood and discreet samples do not have the data needed for the productive treatment of these fluctuating levels. This challenge has been explained by biosensors using Glucose Oxidase (GOx) for the quantification of glucose response in the blood to glucose acid and H2O2 by an electrode in the vicinity [124]. This idea is enhanced by a few different strategies through nanotechnology. To increase the efficiency of electrodes, nanotubes or nanopaths are used [125]. Nanoparticles use electron conductors which are the most popular electron transport strategy between GOx and electrode. The popular choice in this application is carbon nanotubes (CNT), due to their unique surfaces and their ability to conduct electrics. In particular, nanoparticles and biological molecules such as GOx have been used with a variety of other nanomaterials. A major disadvantage of immobilized GOx systems is biodegradability. The sensors can provide excellent longevity and stability. In addition to this, chitosan stability in the GOX-coated film showed 80% activity which is maintained after 20 days at less than 60oC temperature [126]. However, a silent sensor should be replaced. It is also possible to respond to electrochemical changes in the blood because of pharmaceuticals like acetaminophen and diets. Thus it is used to synthesize hollow nanoparticles, which are work at electrochemical potential [127]. 10.2. Nanoparticles For patients to improve their quality of life, the emergence of drug delivery systems through nanoparticles mediate a significantly improved supply of small molecular drugs. The nanotechnologies are more assured than conventional forms of dosage, as they represent chronic diseases with several more comorbidities by providing a site-specific supply of drugs with a higher bioavailability and reduced dose regimes. Intensive research was carried out for the oral administration of nanoparticles with peptides such as glucagon. The nanoparticles also allow changes in encapsulation of microparticles, glycol (PEG)-PEGyulation, and actively targeted ligands. In addition to the provision of medicinal products, it is directly relevant to diabetics; nanoparticles could also be used to diagnose other co-morbid conditions such as non-healing wounds. Oligonucleotide-function lipid nanoparticles are used topically [128] at lipid-target cells [129]. The FDA have announced that these nanoparticles are used in the treatment of diabetic injuries. Bhadauria et al. Nanoparticles have the shape and size that allows high surface areas on which reactions with the particle surface and functional biomolecules can occur. Mostly they have antibacterial characteristics associated with antibacterial molecules to mitigate infection and heal injuries quickly. It can spread into the 3-D medium to eliminate harmful biofilms synthesized by a certain pathogenic bacteria survival mechanism [41]. A multitude of coatings or groups were used in conjunction with nanoparticles to enhance the treatment of injury or chronic injury. For example, nanoparticles in gold epigallocatechin (EGCG) and a-lipoic acid combined antioxidant in which gold stimulates angiogenesis and reduces macrophage activity [130]. Poly nanoparticles (LACGA) were coated with VEGF, curcumin, and antibiotic molecules [131-133]. The adaptability of nanoparticles as a delivery vehicle is therefore marvelously demonstrated. In combination with other nanomaterials such as nanofibers, nanoparticles have been used to produce a range of nanocomposite wound dressings that promote the correct healing process and prevent infections [134, 135]. Various manufacturing strategies are based on the composition of the nanoparticles. Nanoparticles based on polymers often use self-build processes like desolation [136, 137]. Desolation dissolves the material in a solvent and adds an anti-solvent to nanoparticles (miscible in the solvent but unable to dissolve the nanoparticle material). This anti-solvent generates and precipitates the nanoparticles. Emulsion-based methods provide another way for the self-build polymers and lipids [138, 139]. Due to hydrophobic interactions of nanoparticles material to the aqueous solution, emulsion results in the selfbuild of nanoparticles. The nanoparticle size can be controlled by how much energy is added to a solution by homogenization or sonication during preparation. The resultant nanoparticles are solid or shell-based and being prepared by single or double emulsions [140, 141]. 10.3. Nanofibers Nanofibers are attractive wound healing technology for both weather and cellular regeneration [142]. Nanofibers have the core concept of developing injury clothing that imitates ECM functioning. Nanofibers are commonly found as molecules that occur within the ECM of the skin. Examples include collagen, gelatin, fibrin, hyaluronic acid, silk fibroin, chitosan, cellulose, and many more [143, 144]. In addition, a study on other popular nonbiological nanomaterials including polylactic acid, polycaprolactone, polyurethane, polyvinyl alcohol, polyethylene oxide, glycol, and PLGA has been conducted [145, 146]. Nanofibers have advantages in terms of their permeability and they also have the capability of 3-D dressings which act as a local medicine supply system [147, 148]. In addition to nanofibres, nanomats, and nanogels, the weather potential is matched to the technology that has been adapted for the treatment of several wound types which is associated with diseases by loading the network with development factors [149]. The solution could even include several nano-fiber polymers for core-shell preparation with drugs [150, 151]. CONCLUSION Inflammation, proliferation, and remodeling are three stages in the wound healing process. Internal and external Advancement in Nanoformulations Endocrine, Metabolic & Immune Disorders-Drug Targets, 2022, Vol. 22, No. 9 921 causes include altered cellular and cytokine responses, poor vascularization, microorganism infection and it also interrupts the physiology of the healing process in DFU. This review focuses on nanoparticle-based therapeutics that deliver peptides, nucleic acids, antibiotics, and antioxidants through polymeric and natural nanostructures, hydrogels, and nanofibers which have shown impressive outcomes in chronic diabetic wound re-epithelialization, collagen fibers deposition, tissue regeneration, and ultimately a faster rate of wound closure. The use of nanoparticles and biopolymers in the form of a nanocomposite has a great impact on tissue repairing and the wound healing process. While nanomaterials have been extensively studied for wound healing, further research is needed in this field. Overall, nanoparticles have appeared as a promising agent in diabetic wound healing. [9] [10] [11] [12] [13] CONSENT OF PUBLICATION Not applicable. [14] FUNDING None. CONFLICT OF INTEREST [15] The authors declare no conflict of interest, financial or otherwise. ACKNOWLEDGEMENT [16] Authors are highly thankful to the Department of Pharmacy, School of Medical and Allied Sciences, Galgotias University, Greater Noida, India, for providing a library facility for the literature survey. [17] REFERENCE: [1] [2] [3] [4] [5] [6] [7] [8] Smith, R.A. Nanotechnology in the future treatment of diabetic wounds. Rev. Diabet. Stud., 2020, 16(1), 1-12. http://dx.doi.org/10.1900/RDS.2020.16.1 PMID: 32876648 Turabelidze, A.; Dipietro, L.A. Inflammation and Wound Healing.Oral wound heal; Larjava, H., Ed.; John Wiley and Sons, 2013, pp. 39-56. http://dx.doi.org/10.1002/9781118704509.ch3 Rowley, W.R.; Bezold, C.; Arikan, Y.; Byrne, E.; Krohe, S. Diabetes 2030: Insights from yesterday, today, and future trends. Popul. Health Manag., 2017, 20(1), 6-12. http://dx.doi.org/10.1089/pop.2015.0181 PMID: 27124621 International diabetic federation. 2021. Available from: https://www.idf.org/aboutdiabetes/what-is-diabetes/facts-figures.html Snyder, R.J.; Hanft, J.R. Diabetic foot ulcers - Effects on quality of life, costs, and mortality and the role of standard wound care and advanced-care therapies in healing: A review. Ostomy Wound Manage., 2009, 55, 28-38. PMID: 19934461 Bhatnagar, S.; Bharara, M.; Armstrong, D.G. Innovations in diabetic foot care: Prevention, education and treatment. Am. Fam. Physician, 1998, 1-4. Brem, H.; Tomic-Canic, M. Cellular and molecular basis of wound healing in diabetes. J. Clin. Invest., 2007, 117(5), 1219-1222. http://dx.doi.org/10.1172/JCI32169 PMID: 17476353 Khanna, S.; Biswas, S.; Shang, Y.; Collard, E.; Azad, A.; Kauh, C.; Bhasker, V.; Gordillo, G.M.; Sen, C.K.; Roy, S. Macrophage dysfunction impairs resolution of inflammation in the wounds of diabetic mice. PLoS One, 2010, 5(3), e9539. http://dx.doi.org/10.1371/journal.pone.0009539 PMID: 20209061 [18] [19] [20] [21] [22] Barroso, A.; Mestre, H.; Ascenso, H.; Simoes, S.; Reis, C. Nanomaterials in wound healing: From material sciences to wound healing applications. Nano Sel., 2020, 1(5), 443-460. http://dx.doi.org/10.1002/nano.202000055 Vijayakumar, V.; Samal, S.K.; Mohanty, S.; Nayak, S.K. Recent advancements in biopolymer and metal nanoparticle-based materials in diabetic wound healing management. Int. J. Biol. Macromol., 2019, 122, 137-148. http://dx.doi.org/10.1016/j.ijbiomac.2018.10.120 PMID: 30342131 Lu, S.; Xia, D.; Huang, G.; Jing, H.; Wang, Y.; Gu, H. Concentration effect of gold nanoparticles on proliferation of keratinocytes. Colloids Surf. B Biointerfaces, 2010, 81(2), 406-411. http://dx.doi.org/10.1016/j.colsurfb.2010.06.019 PMID: 20801623 Hamdan, S.; Pastar, I.; Drakulich, S.; Dikici, E.; Tomic-Canic, M.; Deo, S.; Daunert, S. Nanotechnology-driven therapeutic interventions in wound healing: Potential uses and applications. ACS Cent. Sci., 2017, 3(3), 163-175. http://dx.doi.org/10.1021/acscentsci.6b00371 PMID: 28386594 Mogoşanu, G.D.; Grumezescu, A.M. Natural and synthetic polymers for wounds and burns dressing. Int. J. Pharm., 2014, 463(2), 127136. http://dx.doi.org/10.1016/j.ijpharm.2013.12.015 PMID: 24368109 Voigt, J.; Driver, V.R. Hyaluronic acid derivatives and their healing effect on burns, epithelial surgical wounds, and chronic wounds: A systematic review and meta-analysis of randomized controlled trials. Wound Repair Regen., 2012, 20(3), 317-331. http://dx.doi.org/10.1111/j.1524-475X.2012.00777.x PMID: 22564227 Wang, T.; Zheng, Y.; Shi, Y.; Zhao, L. pH-responsive calcium alginate hydrogel laden with protamine nanoparticles and hyaluronan oligosaccharide promotes diabetic wound healing by enhancing angiogenesis and antibacterial activity. Drug Deliv. Transl. Res., 2019, 9(1), 227-239. http://dx.doi.org/10.1007/s13346-018-00609-8 PMID: 30519937 Alberti, T.; Coelho, D.S.; Voytena, A.; Pitz, H.; de Pra, M.; Mazzarino, L.; Kuhnen, S.; Ribeiro-do-Valle, R.M.; Maraschin, M.; Veleirinho, B. Nanotechnology: A promising tool towards wound healing. Curr. Pharm. Des., 2017, 23(24), 3515-3528. http://dx.doi.org/10.2174/1381612823666170503152550 PMID: 28472915 Gong, C.; Wu, Q.; Wang, Y.; Zhang, D.; Luo, F.; Zhao, X.; Wei, Y.; Qian, Z. A biodegradable hydrogel system containing curcumin encapsulated in micelles for cutaneous wound healing. Biomaterials, 2013, 34(27), 6377-6387. http://dx.doi.org/10.1016/j.biomaterials.2013.05.005 PMID: 23726229 Dellera, E.; Bonferoni, M.C.; Sandri, G.; Rossi, S.; Ferrari, F.; Del Fante, C.; Perotti, C.; Grisoli, P.; Caramella, C. Development of chitosan oleate ionic micelles loaded with silver sulfadiazine to be associated with platelet lysate for application in wound healing. Eur. J. Pharm. Biopharm., 2014, 88(3), 643-650. http://dx.doi.org/10.1016/j.ejpb.2014.07.015 PMID: 25128852 Akbar, M.U.; Zia, K.M.; Akash, M.S.H.; Nazir, A.; Zuber, M.; Ibrahim, M. In-vivo anti-diabetic and wound healing potential of chitosan/alginate/maltodextrin/pluronic-based mixed polymeric micelles: Curcumin therapeutic potential. Int. J. Biol. Macromol., 2018, 120(Pt B), 2418-2430. http://dx.doi.org/10.1016/j.ijbiomac.2018.09.010 PMID: 30195611 Chereddy, K.K.; Her, C.H.; Comune, M.; Moia, C.; Lopes, A.; Porporato, P.E.; Vanacker, J.; Lam, M.C.; Steinstraesser, L.; Sonveaux, P.; Zhu, H.; Ferreira, L.S.; Vandermeulen, G.; Préat, V. PLGA nanoparticles loaded with host defense peptide LL37 promote wound healing. J. Control. Release, 2014, 194, 138-147. http://dx.doi.org/10.1016/j.jconrel.2014.08.016 PMID: 25173841 Sanchez, D.A.; Schairer, D.; Tuckman-Vernon, C.; Chouake, J.; Kutner, A.; Makdisi, J.; Friedman, J.M.; Nosanchuk, J.D.; Friedman, A.J. Amphotericin B releasing nanoparticle topical treatment of Candida spp. in the setting of a burn wound. Nanomedicine, 2014, 10(1), 269-277. http://dx.doi.org/10.1016/j.nano.2013.06.002 PMID: 23770066 Abbasi, E.; Aval, S.F.; Akbarzadeh, A.; Milani, M.; Nasrabadi, H.T.; Joo, S.W.; Hanifehpour, Y.; Nejati-Koshki, K.; Pashaei-Asl, R. Dendrimers: synthesis, applications, and properties. Nanoscale Res. Lett., 2014, 9(1), 247. 922 Endocrine, Metabolic & Immune Disorders-Drug Targets, 2022, Vol. 22, No. 9 [23] [24] [25] [26] [27] [28] [29] [30] [31] [32] [33] [34] [35] [36] http://dx.doi.org/10.1186/1556-276X-9-247 PMID: 24994950 Kwon, M.J.; An, S.; Choi, S.; Nam, K.; Jung, H.S.; Yoon, C.S.; Ko, J.H.; Jun, H.J.; Kim, T.K.; Jung, S.J.; Park, J.H.; Lee, Y.; Park, J.S. Effective healing of diabetic skin wounds by using nonviral gene therapy based on minicircle vascular endothelial growth factor DNA and a cationic dendrimer. J. Gene Med., 2012, 14(4), 272-278. http://dx.doi.org/10.1002/jgm.2618 PMID: 22407991 Maji, S.; Agarwal, T.; Maiti, T.K. PAMAM (generation 4) incorporated gelatin 3D matrix as an improved dermal substitute for skin tissue engineering. Colloids Surf. B Biointerfaces, 2017, 155, 128-134. http://dx.doi.org/10.1016/j.colsurfb.2017.04.003 PMID: 28419941 Teo, S.Y.; Yew, M.Y.; Lee, S.Y.; Rathbone, M.J.; Gan, S.N.; Coombes, A.G.A. In vitro evaluation of novel phenytoin-loaded alkyd nanoemulsions designed for application in topical wound healing. J. Pharm. Sci., 2017, 106(1), 377-384. http://dx.doi.org/10.1016/j.xphs.2016.06.028 PMID: 27522920 Alam, P.; Shakeel, F.; Anwer, M.K.; Foudah, A.I.; Alqarni, M.H. Wound healing study of Eucalyptus essential oil containing nanoemulsion in rat model. J. Oleo Sci., 2018, 67(8), 957-968. http://dx.doi.org/10.5650/jos.ess18005 PMID: 30012898 Applications in the prevention and treatment of skin disorders. In: Ascenso, A; Simoes, S; Ribeiro, H; Ascenso., , Eds.; Carrier-Mediated Dermal Delivery, 1st ed; Jenny Stanford Publishing, 2017; p. 586. http://dx.doi.org/10.4324/9781315364476 Xu, H.L.; Chen, P.P.; ZhuGe, D.L.; Zhu, Q.Y.; Jin, B.H.; Shen, B.X.; Xiao, J.; Zhao, Y.Z. Liposomes with silk fibroin hydrogel core to stabilize bFGF and promote the wound healing of mice with deep second-degree scald. Adv. Healthc. Mater., 2017, 6(19), 1700344. http://dx.doi.org/10.1002/adhm.201700344 PMID: 28661050 Choudhary, V.; Shivakumar, H.; Ojha, H. Curcumin-loaded liposomes for wound healing: Preparation, optimization, in-vivo skin permeation and bioevaluation. J. Drug Deliv. Sci. Technol., 2019, 49, 683-691. http://dx.doi.org/10.1016/j.jddst.2018.12.008 Lu, K.J.; Wang, W.; Xu, X.L.; Jin, F.Y.; Qi, J.; Wang, X.J.; Kang, X.Q.; Zhu, M.L.; Huang, Q.L.; Yu, C.H.; You, J.; Du, Y.Z. A dual deformable liposomal ointment functionalized with retinoic acid and epidermal growth factor for enhanced burn wound healing therapy. Biomater. Sci., 2019, 7(6), 2372-2382. http://dx.doi.org/10.1039/C8BM01569D PMID: 30916681 Cheng, R.; Liu, L.; Xiang, Y.; Lu, Y.; Deng, L.; Zhang, H.; Santos, H.A.; Cui, W. Advanced liposome-loaded scaffolds for therapeutic and tissue engineering applications. Biomaterials, 2020, 232, 119706. http://dx.doi.org/10.1016/j.biomaterials.2019.119706 PMID: 31918220 Wang, W.; Lu, K.J.; Yu, C.H.; Huang, Q.L.; Du, Y.Z. Nano-drug delivery systems in wound treatment and skin regeneration. J. Nanobiotechnology, 2019, 17(1), 82. http://dx.doi.org/10.1186/s12951-019-0514-y PMID: 31291960 Motawea, A.; Abd El-Gawad, A.E.H.; Borg, T.; Motawea, M.; Tarshoby, M. The impact of topical phenytoin loaded nanostructured lipid carriers in diabetic foot ulceration. Foot, 2019, 40, 14-21. http://dx.doi.org/10.1016/j.foot.2019.03.007 PMID: 30999080 Khezri, K.; Farahpour, M.R.; Mounesi Rad, S. Accelerated infected wound healing by topical application of encapsulated Rosemary essential oil into nanostructured lipid carriers. Artif. Cells Nanomed. Biotechnol., 2019, 47(1), 980-988. http://dx.doi.org/10.1080/21691401.2019.1582539 PMID: 30857435 Ghaffari, S.; Alihosseini, F.; Rezayat Sorkhabadi, S.M.; Arbabi Bidgoli, S.; Mousavi, S.E.; Haghighat, S.; Afshar Nasab, A.; Kianvash, N. Nanotechnology in wound healing; semisolid dosage forms containing curcumin-ampicillin solid lipid nanoparticles, in-vitro, exvivo and in-vivo characteristics. Adv. Pharm. Bull., 2018, 8(3), 395400. http://dx.doi.org/10.15171/apb.2018.046 PMID: 30276135 Kasiewicz, L.N.; Whitehead, K.A. Lipid nanoparticles silence tumor necrosis factor α to improve wound healing in diabetic mice. Bioeng. Transl. Med., 2018, 4(1), 75-82. http://dx.doi.org/10.1002/btm2.10123 PMID: 30680320 [37] [38] [39] [40] [41] [42] [43] [44] [45] [46] [47] [48] [49] [50] [51] [52] [53] Bhadauria et al. Mihai, M.M.; Preda, M.; Lungu, I.; Gestal, M.C.; Popa, M.I.; Holban, A.M. Nanocoatings for chronic wound repair-modulation of microbial colonization and biofilm formation. Int. J. Mol. Sci., 2018, 19(4), 1-20. http://dx.doi.org/10.3390/ijms19041179 PMID: 29649179 Natarajan, S.; Harini, K.; Gajula, G.P.; Sarmento, B.; Neves-Petersen, M.T.; Thiagarajan, V. Multifunctional magnetic iron oxide nanoparticles: Diverse synthetic approaches, surface modifications, cytotoxicity towards biomedical and industrial applications. BMC Mat., 2019, 1(1), 1-22. http://dx.doi.org/10.1186/s42833-019-0002-6 Anghel, I.; Grumezescu, A.M.; Holban, A.M.; Ficai, A.; Anghel, A.G.; Chifiriuc, M.C. Biohybrid nanostructured iron oxide nanoparticles and Satureja hortensis to prevent fungal biofilm development. Int. J. Mol. Sci., 2013, 14(9), 18110-18123. http://dx.doi.org/10.3390/ijms140918110 PMID: 24009022 Rădulescu, M.; Andronescu, E.; Holban, A.; Vasile, B.; Iordache, F.; Mogoantă, L.; Mogoșanu, G.; Grumezescu, A.; Georgescu, M.; Chifiriuc, M. Antimicrobial nanostructured bioactive coating based on fe3o4 and Patchouli oil for wound dressing. Metals (Basel), 2016, 6(5), 1-10. http://dx.doi.org/10.3390/met6050103 Hetrick, E.M.; Shin, J.H.; Paul, H.S.; Schoenfisch, M.H.; Hetrick, E.M.; Shin, J.H.; Paul, H.S.; Schoenfisch, M.H. Anti-biofilm efficacy of nitric oxide-releasing silica nanoparticles. Biomaterials, 2009, 30(14), 2782-2789. http://dx.doi.org/10.1016/j.biomaterials.2009.01.052 PMID: 19233464 Quignard, S.; Coradin, T.; Powell, J.J.; Jugdaohsingh, R. Silica nanoparticles as sources of silicic acid favoring wound healing in vitro. Colloids Surf. B Biointerfaces, 2017, 155, 530-537. http://dx.doi.org/10.1016/j.colsurfb.2017.04.049 PMID: 28494431 Park, J.U.; Jeong, S.H.; Song, E.H.; Song, J.; Kim, H.E.; Kim, S. Acceleration of the healing process of full-thickness wounds using hydrophilic chitosan-silica hybrid sponge in a porcine model. J. Biomater. Appl., 2018, 32(8), 1011-1023. http://dx.doi.org/10.1177/0885328217751246 PMID: 29357774 Whitney, J.D. Overview: Acute and chronic wounds. Nurs. Clin. North Am., 2005, 40(2), 191-205, v. http://dx.doi.org/10.1016/j.cnur.2004.09.002 PMID: 15924889 Upton, D.; Solowiej, K.; Hender, C.; Woodyatt, K.Y. Stress and pain associated with dressing change in patients with chronic wounds. J. Wound Care, 2012, 21(2), 53-54, 56, 58 passim. http://dx.doi.org/10.12968/jowc.2012.21.2.53 PMID: 22584524 Calo, E.; Khutoryanskiy, V.V. Biomedical applications of hydrogels: A review of patents and commercial products. Eur. Polym. J., 2015, 65, 252-267. http://dx.doi.org/10.1016/j.eurpolymj.2014.11.024 Han, G.; Ceilley, R. Chronic wound healing: A review of current management and treatments. Adv. Ther., 2017, 34(3), 599-610. http://dx.doi.org/10.1007/s12325-017-0478-y PMID: 28108895 Madhumathi, K.; Sudheesh Kumar, P.T.; Abhilash, S.; Sreeja, V.; Tamura, H.; Manzoor, K.; Nair, S.V.; Jayakumar, R. Development of novel chitin/nanosilver composite scaffolds for wound dressing applications. J. Mater. Sci. Mater. Med., 2010, 21(2), 807-813. http://dx.doi.org/10.1007/s10856-009-3877-z PMID: 19802687 Moura, L.I.F.; Dias, A.M.A.; Carvalho, E.; de Sousa, H.C. Recent advances on the development of wound dressings for diabetic foot ulcer treatment--a review. Acta Biomater., 2013, 9(7), 7093-7114. http://dx.doi.org/10.1016/j.actbio.2013.03.033 PMID: 23542233 Martin, P. Wound healing--aiming for perfect skin regeneration. Science, 1997, 276(5309), 75-81. http://dx.doi.org/10.1126/science.276.5309.75 PMID: 9082989 Braund, R.; Hook, S.; Medlicott, N.J. The role of topical growth factors in chronic wounds. Curr. Drug Deliv., 2007, 4(3), 195-204. http://dx.doi.org/10.2174/156720107781023857 PMID: 17627493 Gainza, G.; Villullas, S.; Pedraz, J.L.; Hernandez, R.M.; Igartua, M. Advances in drug delivery systems (DDSs) to release growth factors for wound healing and skin regeneration. Nanomedicine, 2015, 11(6), 1551-1573. http://dx.doi.org/10.1016/j.nano.2015.03.002 PMID: 25804415 Kiritsy, C.P.; Lynch, A.B.; Lynch, S.E. Role of growth factors in cutaneous wound healing: A review. Crit. Rev. Oral Biol. Med., 1993, 4(5), 729-760. Advancement in Nanoformulations [54] [55] [56] [57] [58] [59] [60] [61] [62] [63] [64] [65] [66] [67] [68] Endocrine, Metabolic & Immune Disorders-Drug Targets, 2022, Vol. 22, No. 9 923 http://dx.doi.org/10.1177/10454411930040050401 PMID: 8292715 Eming, S.A.; Krieg, T.; Davidson, J.M. Inflammation in wound repair: Molecular and cellular mechanisms. J. Invest. Dermatol., 2007, 127(3), 514-525. http://dx.doi.org/10.1038/sj.jid.5700701 PMID: 17299434 Singer, A.J.; Clark, R.A. Cutaneous wound healing. N. Engl. J. Med., 1999, 341(10), 738-746. http://dx.doi.org/10.1056/NEJM199909023411006 PMID: 10471461 Velnar, T.; Bailey, T.; Smrkolj, V. The wound healing process: An overview of the cellular and molecular mechanisms. J. Int. Med. Res., 2009, 37(5), 1528-1542. http://dx.doi.org/10.1177/147323000903700531 PMID: 19930861 Malinda, K.M.; Sidhu, G.S.; Banaudha, K.K.; Gaddipati, J.P.; Maheshwari, R.K.; Goldstein, A.L.; Kleinman, H.K. Thymosin alpha 1 stimulates endothelial cell migration, angiogenesis, and wound healing. J. Immunol., 1998, 160(2), 1001-1006. PMID: 9551940 Tettamanti, G.; Grimaldi, A.; Rinaldi, L.; Arnaboldi, F.; Congiu, T.; Valvassori, R.; de Eguileor, M. The multifunctional role of fibroblasts during wound healing in Hirudo medicinalis (Annelida, Hirudinea). Biol. Cell, 2004, 96(6), 443-455. http://dx.doi.org/10.1016/j.biolcel.2004.04.008 PMID: 15325073 Li, B.; Wang, J.H. Fibroblasts and myofibroblasts in wound healing: Force generation and measurement. J. Tissue Viability, 2011, 20(4), 108-120. http://dx.doi.org/10.1016/j.jtv.2009.11.004 PMID: 19995679 Ehrlich, H.P.; Keefer, K.A.; Myers, R.L.; Passaniti, A. Vanadate and the absence of myofibroblasts in wound contraction. Arch. Surg., 1999, 134(5), 494-501. http://dx.doi.org/10.1001/archsurg.134.5.494 PMID: 10323421 Stadelmann, W.K.; Digenis, A.G.; Tobin, G.R. Physiology and healing dynamics of chronic cutaneous wounds. Am. J. Surg., 1998, 176(2A)(Suppl.), 26S-38S. http://dx.doi.org/10.1016/S0002-9610(98)00183-4 PMID: 9777970 Armstrong, D.G.; Lavery, L.A.; Harkless, L.B. Validation of a diabetic wound classification system. The contribution of depth, infection, and ischemia to risk of amputation. Diabetes Care, 1998, 21(5), 855-859. http://dx.doi.org/10.2337/diacare.21.5.855 PMID: 9589255 Morbach, S.; Furchert, H.; Gröblinghoff, U.; Hoffmeier, H.; Kersten, K.; Klauke, G.T.; Klemp, U.; Roden, T.; Icks, A.; Haastert, B.; Rümenapf, G.; Abbas, Z.G.; Bharara, M.; Armstrong, D.G. Longterm prognosis of diabetic foot patients and their limbs: Amputation and death over the course of a decade. Diabetes Care, 2012, 35(10), 2021-2027. http://dx.doi.org/10.2337/dc12-0200 PMID: 22815299 Armstrong, D.G.; Wrobel, J.; Robbins, J.M. Guest Editorial: Are diabetes-related wounds and amputations worse than cancer? Int. Wound J., 2007, 4(4), 286-287. http://dx.doi.org/10.1111/j.1742-481X.2007.00392.x PMID: 18154621 Young, M.J.; McCardle, J.E.; Randall, L.E.; Barclay, J.I. Improved survival of diabetic foot ulcer patients 1995-2008: Possible impact of aggressive cardiovascular risk management. Diabetes Care, 2008, 31(11), 2143-2147. http://dx.doi.org/10.2337/dc08-1242 PMID: 18697900 Brennan, M.B.; Hess, T.M.; Bartle, B.; Cooper, J.M.; Kang, J.; Huang, E.S.; Smith, M.; Sohn, M.W.; Crnich, C. Diabetic foot ulcer severity predicts mortality among veterans with type 2 diabetes. J. Diabetes Complications, 2017, 31(3), 556-561. http://dx.doi.org/10.1016/j.jdiacomp.2016.11.020 PMID: 27993523 Iversen, M.M.; Tell, G.S.; Riise, T.; Hanestad, B.R.; Østbye, T.; Graue, M.; Midthjell, K. History of foot ulcer increases mortality among individuals with diabetes: Ten-year follow-up of the NordTrøndelag Health Study, Norway. Diabetes Care, 2009, 32(12), 2193-2199. http://dx.doi.org/10.2337/dc09-0651 PMID: 19729524 Bommer, C.; Heesemann, E.; Sagalova, V.; Manne-Goehler, J.; Atun, R.; Bärnighausen, T.; Vollmer, S. The global economic burden of diabetes in adults aged 20-79 years: A cost-of-illness study. Lancet Diabetes Endocrinol., 2017, 5(6), 423-430. http://dx.doi.org/10.1016/S2213-8587(17)30097-9 PMID: 28456416 [69] [70] [71] [72] [73] [74] [75] [76] [77] [78] [79] [80] [81] Armstrong, D.G.; Boulton, A.J.M.; Bus, S.A. Diabetic foot ulcers and their recurrence. N. Engl. J. Med., 2017, 376(24), 2367-2375. http://dx.doi.org/10.1056/NEJMra1615439 PMID: 28614678 Diabetes UK. Putting feet first: Diabetes UK position on preventing amputations and improving foot care for people with diabetes. 2015. Available from: https://www.diabetes.org.uk/ Upload/Shared%20practice/Diabetic%20footcare (Accessed 23 March 2021). Ramsey, S.D.; Newton, K.; Blough, D.; McCulloch, D.K.; Sandhu, N.; Reiber, G.E.; Wagner, E.H. Incidence, outcomes, and cost of foot ulcers in patients with diabetes. Diabetes Care, 1999, 22(3), 382-387. http://dx.doi.org/10.2337/diacare.22.3.382 PMID: 10097914 Rice, J.B.; Desai, U.; Cummings, A.K.G.; Birnbaum, H.G.; Skornicki, M.; Parsons, N.B. Burden of diabetic foot ulcers for medicare and private insurers. Diabetes Care, 2014, 37(3), 651-658. http://dx.doi.org/10.2337/dc13-2176 PMID: 24186882 Margolis, D.J.; Malay, S.; Hoffstad, O.; Leonard, C.E.; MaCurdy, T; de Nava, KL; Tan, Y; Molina, T; Siegel, KL Incidence of diabetic foot ulcer and lower extremity amputation among Medicare beneficiaries. 2006. Available from: https:// www.ncbi.nlm.nih.gov/books/NBK65149/ (Accessed 23 March, 2021). Abbott, C.A.; Carrington, A.L.; Ashe, H.; Bath, S.; Every, L.C.; Griffiths, J.; Hann, A.W.; Hussein, A.; Jackson, N.; Johnson, K.E.; Ryder, C.H.; Torkington, R.; Van Ross, E.R.E.; Whalley, A.M.; Widdows, P.; Williamson, S.; Boulton, A.J.M. The North-West diabetes foot care study: Incidence of, and risk factors for, new diabetic foot ulceration in a community-based patient cohort. Diabet. Med., 2002, 19(5), 377-384. http://dx.doi.org/10.1046/j.1464-5491.2002.00698.x PMID: 12027925 Muller, I.S.; de Grauw, W.J.; van Gerwen, W.H.E.M.; Bartelink, M.L.; van Den Hoogen, H.J.M.; Rutten, G.E.H.M. Foot ulceration and lower limb amputation in type 2 diabetic patients in dutch primary health care. Diabetes Care, 2002, 25(3), 570-574. http://dx.doi.org/10.2337/diacare.25.3.570 PMID: 11874949 Crawford, F.; Cezard, G.; Chappell, F.M.; Murray, G.D.; Price, J.F.; Sheikh, A.; Simpson, C.R.; Stansby, G.P.; Young, M.J. A systematic review and individual patient data meta-analysis of prognostic factors for foot ulceration in people with diabetes: The international research collaboration for the prediction of diabetic foot ulcerations (PODUS). Health Technol. Assess., 2015, 19(57), 1-210. http://dx.doi.org/10.3310/hta19570 PMID: 26211920 Monteiro-Soares, M.; Ribas, R.; Pereira da Silva, C.; Bral, T.; Mota, A.; Pinheiro Torres, S.; Morgado, A.; Couceiro, R.; Ribeiro, R.; Dias, V.; Moreira, M.; Mourão, P.; Oliveira, M.J.; Madureira, M.; PaixãoDias, V.; Dinis-Ribeiro, M. Diabetic foot ulcer development risk classifications’ validation: A multicentre prospective cohort study. Diabetes Res. Clin. Pract., 2017, 127, 105-114. http://dx.doi.org/10.1016/j.diabres.2017.02.034 PMID: 28340359 Hoogeveen, R.C.; Dorresteijn, J.A.; Kriegsman, D.M.; Valk, G.D. Complex interventions for preventing diabetic foot ulceration. Cochrane Database Syst. Rev., 2015, 8(8), CD007610. http://dx.doi.org/10.1002/14651858.CD007610.pub3 PMID: 26299991 van Netten, J.J.; Price, P.E.; Lavery, L.A.; Monteiro-Soares, M.; Rasmussen, A.; Jubiz, Y.; Bus, S.A. International Working Group on the Diabetic Foot. Prevention of foot ulcers in the at-risk patient with diabetes: A systematic review. Diabetes Metab. Res. Rev., 2016, 32(Suppl. 1), 84-98. http://dx.doi.org/10.1002/dmrr.2701 PMID: 26340966 Ince, P.; Abbas, Z.G.; Lutale, J.K.; Basit, A.; Ali, S.M.; Chohan, F.; Morbach, S.; Möllenberg, J.; Game, F.L.; Jeffcoate, W.J. Use of the SINBAD classification system and score in comparing outcome of foot ulcer management on three continents. Diabetes Care, 2008, 31(5), 964-967. http://dx.doi.org/10.2337/dc07-2367 PMID: 18299441 Mills, J.L., Sr; Conte, M.S.; Armstrong, D.G.; Pomposelli, F.B.; Schanzer, A.; Sidawy, A.N.; Andros, G. Society for vascular surgery lower extremity guidelines committee. The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: Risk stratification based on wound, ischemia, and foot infection (WIfI). J. Vasc. Surg., 2014, 59(1), 220-34.e1, 2. http://dx.doi.org/10.1016/j.jvs.2013.08.003 PMID: 24126108 924 Endocrine, Metabolic & Immune Disorders-Drug Targets, 2022, Vol. 22, No. 9 [82] [83] [84] [85] [86] [87] [88] [89] [90] [91] [92] [93] [94] [95] [96] [97] NHS Digital. National Diabetes Foot Care Audit Available from: http://content.digital.nhs.uk/catalogue/PUB23525/natidiab-footcare-audit-14-16-rep.pdf ( Accessed March 23, 2021). Smith-Strøm, H.; Iversen, M.M.; Igland, J.; Østbye, T.; Graue, M.; Skeie, S.; Wu, B.; Rokne, B. Severity and duration of diabetic foot ulcer (DFU) before seeking care as predictors of healing time: A retrospective cohort study. PLoS One, 2017, 12(5), e0177176. http://dx.doi.org/10.1371/journal.pone.0177176 PMID: 28498862 Game, F.L.; Chipchase, S.Y.; Hubbard, R.; Burden, R.P.; Jeffcoate, W.J. Temporal association between the incidence of foot ulceration and the start of dialysis in diabetes mellitus. Nephrol. Dial. Transplant., 2006, 21(11), 3207-3210. http://dx.doi.org/10.1093/ndt/gfl427 PMID: 16877485 Ndip, A.; Rutter, M.K.; Vileikyte, L.; Vardhan, A.; Asari, A.; Jameel, M.; Tahir, H.A.; Lavery, L.A.; Boulton, A.J.M. Dialysis treatment is an independent risk factor for foot ulceration in patients with diabetes and stage 4 or 5 chronic kidney disease. Diabetes Care, 2010, 33(8), 1811-1816. http://dx.doi.org/10.2337/dc10-0255 PMID: 20484126 Game, F.L.; Selby, N.M.; McIntyre, C.W. Chronic kidney disease and the foot in diabetes--is inflammation the missing link? Nephron Clin. Pract., 2013, 123(1-2), 36-40. http://dx.doi.org/10.1159/000351813 PMID: 23752138 Lavery, L.A.; Hunt, N.A.; Ndip, A.; Lavery, D.C.; Van Houtum, W.; Boulton, A.J.M. Impact of chronic kidney disease on survival after amputation in individuals with diabetes. Diabetes Care, 2010, 33(11), 2365-2369. http://dx.doi.org/10.2337/dc10-1213 PMID: 20739688 Dorresteijn, J.A.N.; Kriegsman, D.M.W.; Assendelft, W.J.J.; Valk, G.D. Patient education for preventing diabetic foot ulceration. Cochrane Database Syst. Rev., 2014, 12(12), CD001488. http://dx.doi.org/10.1002/14651858.CD001488.pub5 PMID: 25514250 Lavery, L.A.; Armstrong, D.G. Temperature monitoring to assess, predict, and prevent diabetic foot complications. Curr. Diab. Rep., 2007, 7(6), 416-419. http://dx.doi.org/10.1007/s11892-007-0069-4 PMID: 18255002 Greenhalgh, D.G. Wound healing and diabetes mellitus. Clin. Plast. Surg., 2003, 30(1), 37-45. http://dx.doi.org/10.1016/S0094-1298(02)00066-4 PMID: 12636214 Dinh, T.; Elder, S.; Veves, A. Delayed wound healing in diabetes: Considering future treatments. Diabetes Manag. (Lond.), 2011, 1(5), 509-519. http://dx.doi.org/10.2217/dmt.11.44 Geraghty, T.; LaPorta, G. Current health and economic burden of chronic diabetic osteomyelitis. Expert Rev. Pharmacoecon. Outcomes Res., 2019, 19(3), 279-286. http://dx.doi.org/10.1080/14737167.2019.1567337 PMID: 30625012 Zhang, P.; Lu, J.; Jing, Y.; Tang, S.; Zhu, D.; Bi, Y. Global epidemiology of diabetic foot ulceration: A systematic review and meta-analysis †. Ann. Med., 2017, 49(2), 106-116. http://dx.doi.org/10.1080/07853890.2016.1231932 PMID: 27585063 Boulton, A.J.M.; Vileikyte, L.; Ragnarson-Tennvall, G.; Apelqvist, J. The global burden of diabetic foot disease. Lancet, 2005, 366(9498), 1719-1724. http://dx.doi.org/10.1016/S0140-6736(05)67698-2 PMID: 16291066 Raghav, A.; Khan, Z.A.; Labala, R.K.; Ahmad, J.; Noor, S.; Mishra, B.K. Financial burden of diabetic foot ulcers to world: A progressive topic to discuss always. Ther. Adv. Endocrinol. Metab., 2018, 9(1), 29-31. http://dx.doi.org/10.1177/2042018817744513 PMID: 29344337 Ragnarson Tennvall, G.; Apelqvist, J. Health-economic consequences of diabetic foot lesions. Clin. Infect. Dis., 2004, 39(2)(Suppl. 2), S132-S139. http://dx.doi.org/10.1086/383275 PMID: 15306992 Eming, S.A.; Martin, P.; Tomic-Canic, M. Wound repair and regeneration: Mechanisms, signaling, and translation. Sci. Transl. Med., 2014, 6(265), 265sr6. http://dx.doi.org/10.1126/scitranslmed.3009337 PMID: 25473038 [98] [99] [100] [101] [102] [103] [104] [105] [106] [107] [108] [109] [110] [111] [112] [113] Bhadauria et al. Falanga, V. Wound healing and its impairment in the diabetic foot. Lancet, 2005, 366(9498), 1736-1743. http://dx.doi.org/10.1016/S0140-6736(05)67700-8 PMID: 16291068 Falanga, V. The chronic wound: Impaired healing and solutions in the context of wound bed preparation. Blood Cells Mol. Dis., 2004, 32(1), 88-94. http://dx.doi.org/10.1016/j.bcmd.2003.09.020 PMID: 14757419 Liu, L.; Marti, G.P.; Wei, X.; Zhang, X.; Zhang, H.; Liu, Y.V.; Nastai, M.; Semenza, G.L.; Harmon, J.W. Age-dependent impairment of HIF-1alpha expression in diabetic mice: Correction with electroporation-facilitated gene therapy increases wound healing, angiogenesis, and circulating angiogenic cells. J. Cell. Physiol., 2008, 217(2), 319-327. http://dx.doi.org/10.1002/jcp.21503 PMID: 18506785 Okonkwo, U.A.; DiPietro, L.A. Diabetes and wound angiogenesis. Int. J. Mol. Sci., 2017, 18(7), 1-15. http://dx.doi.org/10.3390/ijms18071419 PMID: 28671607 Hirschi, K.K.; D’Amore, P.A. Pericytes in the microvasculature. Cardiovasc. Res., 1996, 32(4), 687-698. http://dx.doi.org/10.1016/S0008-6363(96)00063-6 PMID: 8915187 Haukipuro, K.; Melkko, J.; Risteli, L.; Kairaluoma, M.; Risteli, J. Synthesis of type I collagen in healing wounds in humans. Ann. Surg., 1991, 213(1), 75-80. http://dx.doi.org/10.1097/00000658-199101000-00013 PMID: 1985542 Gurtner, G.C.; Werner, S.; Barrandon, Y.; Longaker, M.T. Wound repair and regeneration. Nature, 2008, 453(7193), 314-321. http://dx.doi.org/10.1038/nature07039 PMID: 18480812 Wetzler, C.; Kämpfer, H.; Stallmeyer, B.; Pfeilschifter, J.; Frank, S. Large and sustained induction of chemokines during impaired wound healing in the genetically diabetic mouse: Prolonged persistence of neutrophils and macrophages during the late phase of repair. J. Invest. Dermatol., 2000, 115(2), 245-253. http://dx.doi.org/10.1046/j.1523-1747.2000.00029.x PMID: 10951242 Brown, D.L.; Kane, C.D.; Chernausek, S.D.; Greenhalgh, D.G. Differential expression and localization of insulin-like growth factors I and II in cutaneous wounds of diabetic and nondiabetic mice. Am. J. Pathol., 1997, 151(3), 715-724. PMID: 9284820 Roberts, A.B. Transforming growth factor-beta: Activity and efficacy in animal models of wound healing. Wound Repair Regen., 1995, 3(4), 408-418. http://dx.doi.org/10.1046/j.1524-475X.1995.30405.x PMID: 17147652 Semenza, G.L. HIF-1: Mediator of physiological and pathophysiological responses to hypoxia. J. Appl. Physiol., 2000, 88(4), 14741480. http://dx.doi.org/10.1152/jappl.2000.88.4.1474 PMID: 10749844 Seitz, O.; Schürmann, C.; Hermes, N.; Müller, E.; Pfeilschifter, J.; Frank, S.; Goren, I. Wound healing in mice with high-fat diet- or ob gene-induced diabetes-obesity syndromes: A comparative study. Exp. Diabetes Res., 2010, 2010, 476969. http://dx.doi.org/10.1155/2010/476969 PMID: 21318183 Galiano, R.D.; Tepper, O.M.; Pelo, C.R.; Bhatt, K.A.; Callaghan, M.; Bastidas, N.; Bunting, S.; Steinmetz, H.G.; Gurtner, G.C. Topical vascular endothelial growth factor accelerates diabetic wound healing through increased angiogenesis and by mobilizing and recruiting bone marrow-derived cells. Am. J. Pathol., 2004, 164(6), 1935-1947. http://dx.doi.org/10.1016/S0002-9440(10)63754-6 PMID: 15161630 Drela, E.; Stankowska, K.; Kulwas, A.; Rość, D. Endothelial progenitor cells in diabetic foot syndrome. Adv. Clin. Exp. Med., 2012, 21(2), 249-254. PMID: 23214290 Sangiorgi, S.; Manelli, A.; Reguzzoni, M.; Ronga, M.; Protasoni, M.; Dell’Orbo, C. The cutaneous microvascular architecture of human diabetic toe studied by corrosion casting and scanning electron microscopy analysis. Anat. Rec. (Hoboken), 2010, 293(10), 1639-1645. http://dx.doi.org/10.1002/ar.21168 PMID: 20687174 Beer, H.D.; Longaker, M.T.; Werner, S. Reduced expression of PDGF and PDGF receptors during impaired wound healing. J. Invest. Dermatol., 1997, 109(2), 132-138. http://dx.doi.org/10.1111/1523-1747.ep12319188 PMID: 9242497 Advancement in Nanoformulations [114] [115] [116] [117] [118] [119] [120] [121] [122] [123] [124] [125] [126] [127] Endocrine, Metabolic & Immune Disorders-Drug Targets, 2022, Vol. 22, No. 9 925 Balaji, S.; Han, N.; Moles, C.; Shaaban, A.F.; Bollyky, P.L.; Crombleholme, T.M.; Keswani, S.G.; Kesariwani, S.G. Angiopoietin-1 improves endothelial progenitor cell-dependent neovascularization in diabetic wounds. Surgery, 2015, 158(3), 846-856. http://dx.doi.org/10.1016/j.surg.2015.06.034 PMID: 26266763 Lobmann, R.; Zemlin, C.; Motzkau, M.; Reschke, K.; Lehnert, H. Expression of matrix metalloproteinases and growth factors in diabetic foot wounds treated with a protease absorbent dressing. J. Diabetes Complications, 2006, 20(5), 329-335. http://dx.doi.org/10.1016/j.jdiacomp.2005.08.007 PMID: 16949521 Liu, Y.; Min, D.; Bolton, T.; Nubé, V.; Twigg, S.M.; Yue, D.K.; McLennan, S.V. Increased matrix metalloproteinase-9 predicts poor wound healing in diabetic foot ulcers. Diabetes Care, 2009, 32(1), 117-119. http://dx.doi.org/10.2337/dc08-0763 PMID: 18835949 Spampinato, S.F.; Caruso, G.I.; De Pasquale, R.; Sortino, M.A.; Merlo, S. The treatment of impaired wound healing in diabetes: Looking among old drugs. Pharmaceuticals (Basel), 2020, 13(4), 117. http://dx.doi.org/10.3390/ph13040060 PMID: 32244718 Long, M.; Cai, L.; Li, W.; Zhang, L.; Guo, S.; Zhang, R.; Zheng, Y.; Liu, X.; Wang, M.; Zhou, X.; Wang, H.; Li, X.; Li, L.; Zhu, Z.; Yang, G.; Zheng, H. DPP-4 Inhibitors improve diabetic wound healing via direct and indirect promotion of epithelial-mesenchymal transition and reduction of scarring. Diabetes, 2018, 67(3), 518-531. http://dx.doi.org/10.2337/db17-0934 PMID: 29254987 Marfella, R.; Sasso, F.C; Rizzo, M.R; Paolisso, P.; Barbieri, M.; Padovano, V.; Carbonara, O.; Gualdiero, P.; Petronella, P.; Ferraraccio, F. Dipeptidyl peptidase 4 inhibition may facilitate healing of chronic foot ulcers in patients with type 2 diabetes. Exp Diabetes Res, 2012, 2012, 892706. http://dx.doi.org/10.1155/2012/892706 Zhao, P.; Sui, B.D.; Liu, N.; Lv, Y.J.; Zheng, C.X.; Lu, Y.B.; Huang, W.T.; Zhou, C.H.; Chen, J.; Pang, D.L.; Fei, D.D.; Xuan, K.; Hu, C.H.; Jin, Y. Anti-aging pharmacology in cutaneous wound healing: Effects of metformin, resveratrol, and rapamycin by local application. Aging Cell, 2017, 16(5), 1083-1093. http://dx.doi.org/10.1111/acel.12635 PMID: 28677234 Keppel Hesselink, J.M. Phenytoin repositioned in wound healing: Clinical experience spanning 60 years. Drug Discov. Today, 2018, 23(2), 402-408. http://dx.doi.org/10.1016/j.drudis.2017.09.020 PMID: 28993152 Sawaya, A.P.; Jozic, I.; Stone, R.C.; Pastar, I.; Egger, A.N.; Stojadinovic, O.; Glinos, G.D.; Kirsner, R.S.; Tomic-Canic, M. Mevastatin promotes healing by targeting caveolin-1 to restore EGFR signaling. JCI Insight, 2019, 4(23), 129320. http://dx.doi.org/10.1172/jci.insight.129320 PMID: 31661463 Sawaya, A.P.; Pastar, I.; Stojadinovic, O.; Lazovic, S.; Davis, S.C.; Gil, J.; Kirsner, R.S.; Tomic-Canic, M. Topical mevastatin promotes wound healing by inhibiting the transcription factor c-Myc via the glucocorticoid receptor and the long non-coding RNA Gas5. J. Biol. Chem., 2018, 293(4), 1439-1449. http://dx.doi.org/10.1074/jbc.M117.811240 PMID: 29158265 Gu, Z.; Aimetti, A.A.; Wang, Q.; Dang, T.T.; Zhang, Y.; Veiseh, O.; Cheng, H.; Langer, R.S.; Anderson, D.G. Injectable nano-network for glucose-mediated insulin delivery. ACS Nano, 2013, 7(5), 41944201. http://dx.doi.org/10.1021/nn400630x PMID: 23638642 Wang, Y.; Liu, L.; Li, M.; Xu, S.; Gao, F. Multifunctional carbon nanotubes for direct electrochemistry of glucose oxidase and glucose bioassay. Biosens. Bioelectron., 2011, 30(1), 107-111. http://dx.doi.org/10.1016/j.bios.2011.08.038 PMID: 21959226 Chen, C.; Wang, L.; Tan, Y.; Qin, C.; Xie, F.; Fu, Y.; Xie, Q.; Chen, J.; Yao, S. High-performance amperometric biosensors and biofuel cell based on chitosan-strengthened cast thin films of chemically synthesized catecholamine polymers with glucose oxidase effectively entrapped. Biosens. Bioelectron., 2011, 26(5), 2311-2316. http://dx.doi.org/10.1016/j.bios.2010.09.058 PMID: 21035322 Wang, Z.; Liu, S.; Wu, P.; Cai, C. Detection of glucose based on direct electron transfer reaction of glucose oxidase immobilized on highly ordered polyaniline nanotubes. Anal. Chem., 2009, 81(4), 1638-1645. http://dx.doi.org/10.1021/ac802421h PMID: 19170516 [128] [129] [130] [131] [132] [133] [134] [135] [136] [137] [138] [139] [140] [141] [142] Ghatak, S.; Li, J.; Chan, Y.C.; Gnyawali, S.C.; Steen, E.; Yung, B.C.; Khanna, S.; Roy, S.; Lee, R.J.; Sen, C.K. AntihypoxamiR functionalized gramicidin lipid nanoparticles rescue against ischemic memory improving cutaneous wound healing. Nanomedicine, 2016, 12(7), 1827-1831. http://dx.doi.org/10.1016/j.nano.2016.03.004 PMID: 27033464 Li, J.; Ghatak, S.; El Masry, M.S.; Das, A.; Liu, Y.; Roy, S.; Lee, R.J.; Sen, C.K. Topical lyophilized targeted lipid nanoparticles in the restoration of skin barrier function following burn wound. Mol. Ther., 2018, 26(9), 2178-2188. http://dx.doi.org/10.1016/j.ymthe.2018.04.021 PMID: 29802017 Chen, S.A.; Chen, H.M.; Yao, Y.D.; Hung, C.F.; Tu, C.S.; Liang, Y.J. Topical treatment with anti-oxidants and Au nanoparticles promote healing of diabetic wound through receptor for advance glycation end-products. Eur. J. Pharm. Sci., 2012, 47(5), 875-883. http://dx.doi.org/10.1016/j.ejps.2012.08.018 PMID: 22985875 Chereddy, K.K.; Lopes, A.; Koussoroplis, S.; Payen, V.; Moia, C.; Zhu, H.; Sonveaux, P.; Carmeliet, P.; des Rieux, A.; Vandermeulen, G.; Préat, V. Combined effects of PLGA and vascular endothelial growth factor promote the healing of non-diabetic and diabetic wounds. Nanomedicine, 2015, 11(8), 1975-1984. http://dx.doi.org/10.1016/j.nano.2015.07.006 PMID: 26238081 Chereddy, K.K.; Coco, R.; Memvanga, P.B.; Ucakar, B.; des Rieux, A.; Vandermeulen, G.; Préat, V. Combined effect of PLGA and curcumin on wound healing activity. J. Control. Release, 2013, 171(2), 208-215. http://dx.doi.org/10.1016/j.jconrel.2013.07.015 PMID: 23891622 Hill, M.; Cunningham, R.N.; Hathout, R.M.; Johnston, C.; Hardy, J.G.; Migaud, M.E. Formulation of antimicrobial tobramycin loaded PLGA nanoparticles via complexation with AOT. J. Funct. Biomater., 2019, 10(2), 1-14. http://dx.doi.org/10.3390/jfb10020026 PMID: 31200522 Xie, Z.; Paras, C.B.; Weng, H.; Punnakitikashem, P.; Su, L.C.; Vu, K.; Tang, L.; Yang, J.; Nguyen, K.T. Dual growth factor releasing multi-functional nanofibers for wound healing. Acta Biomater., 2013, 9(12), 9351-9359. http://dx.doi.org/10.1016/j.actbio.2013.07.030 PMID: 23917148 Mohandas, A.; Anisha, B.S.; Chennazhi, K.P.; Jayakumar, R. Chitosan-hyaluronic acid/VEGF loaded fibrin nanoparticles composite sponges for enhancing angiogenesis in wounds. Colloids Surf. B Biointerfaces, 2015, 127, 105-113. http://dx.doi.org/10.1016/j.colsurfb.2015.01.024 PMID: 25660093 Lai, H.J.; Kuan, C.H.; Wu, H.C.; Tsai, J.C.; Chen, T.M.; Hsieh, D.J.; Wang, T.W. Tailored design of electrospun composite nanofibers with staged release of multiple angiogenic growth factors for chronic wound healing. Acta Biomater., 2014, 10(10), 4156-4166. http://dx.doi.org/10.1016/j.actbio.2014.05.001 PMID: 24814882 Zavan, B.; Vindigni, V.; Vezzù, K.; Zorzato, G.; Luni, C.; Abatangelo, G.; Elvassore, N.; Cortivo, R. Hyaluronan based porous nanoparticles enriched with growth factors for the treatment of ulcers: A placebo-controlled study. J. Mater. Sci. Mater. Med., 2009, 20(1), 235-247. http://dx.doi.org/10.1007/s10856-008-3566-3 PMID: 18758917 McCall, R.L.; Sirianni, R.W. PLGA nanoparticles formed by singleor double-emulsion with vitamin E-TPGS. J. Vis. Exp., 2013, 82(82), 51015. http://dx.doi.org/10.3791/51015 PMID: 24429733 Thatipamula, R.; Palem, C.; Gannu, R.; Mudragada, S.; Yamsani, M. Formulation and in vitro characterization of domperidone loaded solid lipid nanoparticles and nanostructured lipid carriers. Daru, 2011, 19(1), 23-32. PMID: 22615636 Trivedi, R.; Kompella, U.B. Nanomicellar formulations for sustained drug delivery: Strategies and underlying principles. Nanomedicine (Lond.), 2010, 5(3), 485-505. http://dx.doi.org/10.2217/nnm.10.10 PMID: 20394539 Xu, J.; Liu, Y.; Li, Y.; Wang, H.; Stewart, S.; Van der Jeught, K.; Agarwal, P.; Zhang, Y.; Liu, S.; Zhao, G.; Wan, J.; Lu, X.; He, X. Precise targeting of POLR2A as a therapeutic strategy for human triple negative breast cancer. Nat. Nanotechnol., 2019, 14(4), 388-397. http://dx.doi.org/10.1038/s41565-019-0381-6 PMID: 30804480 Hangge, P.; Stone, J.; Albadawi, H.; Zhang, Y.S.; Khademhosseini, A.; Oklu, R. Hemostasis and nanotechnology. Cardiovasc. Diagn. Ther., 2017, 7(3)(Suppl. 3), S267-S275. http://dx.doi.org/10.21037/cdt.2017.08.07 PMID: 29399530 926 Endocrine, Metabolic & Immune Disorders-Drug Targets, 2022, Vol. 22, No. 9 [143] [144] [145] [146] [147] Wang, T.; Nie, J.; Yang, D. Dextran and gelatin based photocrosslinkable tissue adhesive. Carbohydr. Polym., 2012, 90(4), 14281436. http://dx.doi.org/10.1016/j.carbpol.2012.07.011 PMID: 22944399 Tchemtchoua, V.T.; Atanasova, G.; Aqil, A.; Filée, P.; Garbacki, N.; Vanhooteghem, O.; Deroanne, C.; Noël, A.; Jérome, C.; Nusgens, B.; Poumay, Y.; Colige, A. Development of a chitosan nanofibrillar scaffold for skin repair and regeneration. Biomacromolecules, 2011, 12(9), 3194-3204. http://dx.doi.org/10.1021/bm200680q PMID: 21761871 Kanmaz, D.; Toprakci, H.A.K.; Olmez, H.; Toprakci, O. Electrospun polylactic acid based nanofibers for biomedical applications. Mater Sci Res India., 2018, 15(3), 224-240. http://dx.doi.org/10.13005/msri/150304 Aldayel, A.M.; Naguib, Y.W.; O’Mary, H.L.; Li, X.; Niu, M.; Ruwona, T.B.; Cui, Z. Acid-sensitive sheddable PEGylated PLGA nanoparticles increase the delivery of TNF-α siRNA in chronic inflammation sites. Mol. Ther. Nucleic Acids, 2016, 5(7), e340. http://dx.doi.org/10.1038/mtna.2016.39 PMID: 27434685 Choi, J.S.; Leong, K.W.; Yoo, H.S. In vivo wound healing of diabetic ulcers using electrospun nanofibers immobilized with human epidermal growth factor (EGF). Biomaterials, 2008, 29(5), 587-596. [148] [149] [150] [151] Bhadauria et al. http://dx.doi.org/10.1016/j.biomaterials.2007.10.012 PMID: 17997153 Zamani, M.; Prabhakaran, M.P.; Ramakrishna, S. Advances in drug delivery via electrospun and electrosprayed nanomaterials. Int. J. Nanomedicine, 2013, 8, 2997-3017. http://dx.doi.org/10.2147/IJN.S43575 PMID: 23976851 Kim, H.S.; Yoo, H.S. In vitro and in vivo epidermal growth factor gene therapy for diabetic ulcers with electrospun fibrous meshes. Acta Biomater., 2013, 9(7), 7371-7380. http://dx.doi.org/10.1016/j.actbio.2013.03.018 PMID: 23528498 Augustine, R.; Zahid, A.A.; Hasan, A.; Wang, M.; Webster, T.J. CTGF loaded electrospun dual porous coreshell membrane for diabetic wound healing. Int. J. Nanomedicine, 2019, 14, 8573-8588. http://dx.doi.org/10.2147/IJN.S224047 PMID: 31802870 Miguel, S.P.; Sequeira, R.S.; Moreira, A.F.; Cabral, C.S.D.; Mendonça, A.G.; Ferreira, P.; Correia, I.J. An overview of electrospun membranes loaded with bioactive molecules for improving the wound healing process. Eur. J. Pharm. Biopharm., 2019, 139, 1-22. http://dx.doi.org/10.1016/j.ejpb.2019.03.010 PMID: 30853442 DISCLAIMER: The above article has been published, as is, ahead-of-print, to provide early visibility but is not the final version. Major publication processes like copyediting, proofing, typesetting and further review are still to be done and may lead to changes in the final published version, if it is eventually published. All legal disclaimers that apply to the final published article also apply to this ahead-of-print version.