The Use of Microimplants in Lingual
Orthodontic Treatment
Hee-Moon Kyung
Irrespective of the appliance used, anchorage control in orthodontics has
always been a key requirement for successful orthodontic treatment. Conventionally anchorage is derived from dental, muscular, or skeletal components of the dentofacial complex and is often dependent on a high degree of
patient compliance. The recent development of the microscrew implant has
provided the clinician with a source of rigid, stationary bony anchorage not
dependent on patient compliance. These screws are not osseointegrated
and are retained in the bone on a purely mechanical basis. They are inexpensive and easy to place and remove at sites determined by the malocclusion and the quality of bone available at a specific site. This article discusses
the use of microimplants as an adjunct to lingual orthodontics. (Semin
Orthod 2006;12:186-190.) © 2006 Elsevier Inc. All rights reserved.
he development of the edgewise bracket by
Dr Edward Angle in the early part of the
last century provided the clinician with the ability to achieve accurate tooth movement and high
quality orthodontic treatment. For adult and
some adolescent patients, the poor esthetics of
fixed appliance treatment has been a major inhibiting factor in the acceptance of orthodontic
treatment. To counteract this negative feature,
Fujita1 and Kurz2 in the 1970s designed lingual
brackets and initiated the concept of lingual
orthodontics. As with any new technique, in the
beginning there were several problems to overcome and the final results were, in many cases,
unsatisfactory. Since then, with the development
of the indirect bonding technique, bracket positioning has become more accurate3,4 and wire
bending simplified using the concepts of the
straight wire technique.5
T
Department of Orthodontics, Dental School, Kyungpook National University, Daegu, Korea.
Address correspondence to Hee-Moon Kyung, DDS, MS, PhD,
Department of Orthodontics, Dental School, Kyungpook National
University, 188-1, Sam Duk 2 Ga, Jung Gu, Daegu, Korea 700412. Office phone: ⫹ 82-(0)53-420-5947; Cell phone: ⫹82-(0)16504-7996; Fax: ⫹82-(0)53-421-7607; E-mail: hmkyung@
knu.ac.kr
© 2006 Elsevier Inc. All rights reserved.
1073-8746/06/1203-0$30.00/0
doi:10.1053/j.sodo.2006.05.006
186
Anchorage control in conventional labial
techniques has always been a major concern for
orthodontists; this concern is equally applicable
to lingual orthodontic techniques. The use of
extraoral appliances for anchorage reinforcement is highly compliance dependent and esthetically unacceptable for the majority of patients considering lingual orthodontics.6
The development and incorporation of microimplants in orthodontic treatment7 has provided a means of achieving absolute anchorage
for lingual8-11 as well as labial orthodontics.6
This article describes the use of microimplants in lingual orthodontics.
Maxillary Microimplants
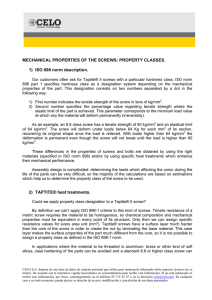
In lingual orthodontic treatment maxillary microimplants can be placed between the roots of
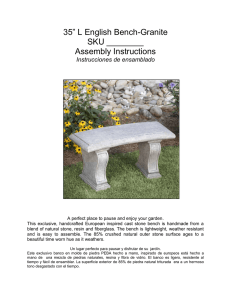
teeth in the palatal alveolar bone (Fig 1) or in
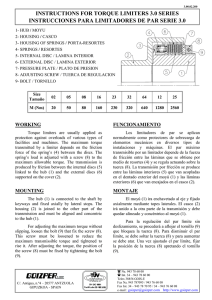
the midpalatal region (Fig 2). In the young patient, the midpalatal suture is still open and in
that situation the microimplant can be placed in
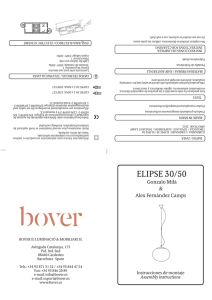
the para-midpalatal region (Fig 3). In certain
cases, it is possible to place the maxillary microimplant in the buccal region, even when using
lingual appliances (Fig 4).
When using microimplants at the distal end
of the arch for anchorage purposes, it is difficult
to control the extrusion of the maxillary anterior
Seminars in Orthodontics, Vol 12, No 3 (September), 2006: pp 186-190
Microimplants
Figure 1. Maxillary microimplant placed in the palatal alveolar bone. (Color version of figure is available
online.)
teeth, which can occur during the en masse
retraction due to vertical bowing of the archwire. In cases requiring intrusion of anterior
teeth, a microimplant can be placed in the labial
cortical bone below the anterior nasal spine and
an intrusive force applied with a clear elastomeric ligature. The ligature is tied to the two
central incisors, bonded together with a clear
resin or composite material (Fig 5).
Microimplants are available in different
lengths; as a general guide, for maxillary microimplants at least 6 mm of the screw portion
should be placed into the bone (Fig 6). The
mucosal thickness varies with each patient and at
different sites in the palate; the thickness can be
measured with an anesthetic needle during or
following the injection. The following recommendations are given as a general guide
Figure 2. Microimplant placed in the midpalatal region. (Color version of figure is available online.)
187
Figure 3. Microimplants placed in the para-midline
region. (Color version of figure is available online.)
Palatal mucosal thickness of 6 mm, use a
12-mm screw.
Midpalatal thinner mucosa, use a 6- to 7-mm
screw.
Buccal alveolar region, attached gingivae, use
7- to 8-mm screw.
Adult patients with thick dense cortical bone,
use a 7-mm screw.
Young patients, less dense cortical bone, use
an 8-mm screw.
Labial aspect of maxillary incisors, good quality bone and not subjected to occlusal
forces, use a 6-mm screw.
The diameter of the screw shanks can range
from 1.2 to 2.0 mm. The selection of the screw
diameter can be varied depending on the selected site. The following is offered as a guide.
Figure 4. Microimplants placed in the buccal region
of the maxilla and mandible in a case treated with a
lingual appliance. (Color version of figure is available
online.)
188
H.-M. Kyung
Figure 5. Maxillary anterior microimplant placed in a
case treated with a lingual appliance. An elastomeric
thread is tied from the implant to clear plastic buttons
on the central incisors. (Color version of figure is
available online.)
Maxillary buccal or labial regions, 1.3- to
1.5-mm thickness screw.
Palatal interdental regions, 1.4- to 1.6-mm
thickness screws.
Midpalatal regions, depending on bone density, 1.6- to 2.0-mm thickness screws.
Several head shapes including flat heads and
post heads are available; once again these are
selected depending on the site, access, and projected force applications (Fig 7). If there is a
potential for the screw head to cause soft tissue
irritation, then it is recommended to use a flat
head as opposed to a post type head. Ease of
access for the clinician and consideration regarding the placement of ligature wire, coil
Figure 6. The microimplant should be inserted at
least 6 mm into the maxilla. (Color version of figure is
available online.)
Figure 7. A selection of Absoanchor micro screws
showing different types of heads.
spring, elastomeric thread, or elastomeric chains
all influence the selection of the screw head.
Mandibular Micro Implants
Within the confines of the mandibular arch,
lingually placed microimplants do tend to irritate the tongue; therefore, it is preferable to
select a flat head design rather than a post head
design. Placing lingual mandibular micro implants is technically a difficult procedure. In view
of these drawbacks, it is recommended that mandibular microimplants should be placed in the
buccal or labial regions, even for cases undergoing lingual orthodontic treatment (Fig 4). It is
unlikely that lingual cases require additional
forces for mandibular incisor intrusion; however, if necessary, microimplants may be placed
in the cortical bone below the lower incisors.
As a general guide, at least 5 mm of the screw
shank should be placed in bone (Fig 8). In
patients with good quality cortical bone a 6-mm
screw is adequate; in younger patients with less
dense cortical bone a 7-to 8-mm screw should be
selected. In the retromolar region, the mucosal
thickness may vary widely; it is advisable to mea-
Microimplants
189
cessfully resist a force of 300 g applied immediately after placing the microimplant.
Microimplant Removal
Figure 8. The microimplant should be inserted at
least 5 mm into the mandible. (Color version of figure
is available online.)
sure the thickness with an anesthetic needle.
The labial cortical bone in the mandibular incisor region is generally quite dense; and furthermore, as this region is not subject to occlusal
forces a 5-mm screw should be adequate.
The diameter of screw selected for the mandibular buccal regions may range from 1.4 to 1.5
mm; and for the mandibular incisal region a
thinner screw, ranging from 1.2 to 1.3 mm,
should be selected.
As a general rule, whether the microimplant
is placed in the maxilla or the mandible, always
try to place it so that the head of the screw is
situated in attached gingivae and not in unattached mucosa. If the screw head is in unattached mucosa, the soft tissues will grow and
embed the screw head. If it is the express intention to place the screw in unattached mucosa,
then a ligature wire hook should be attached to
the head and allowed to protrude through the
unattached mucosa (Fig 9).
Although some osseointegration will take place
between the titanium microimplant and bone,
removal is not difficult. Screws with a diameter
of 1.4 mm or less can be easily removed with less
than 2 to 3 NCm torque force. Only one failure
has been reported when removing a screw of
1.6-mm diameter. For ease of removal, use of
smaller diameter screws is suggested and turning
the hand or motor driver in the opposite direction to that used when inserting the screw. Local
anesthetic is generally not required; occasionally
topical anesthesia may be needed.
Summary
Currently excellent clinical results can and are
being achieved with lingual orthodontics. For
many patients, due to esthetic considerations,
this is their only choice. Certain orthodontists
may still feel reluctant or hesitant to attempt this
form of therapy; however, several articles7-11
have shown that with the indirect bonding techniques available, by using straight wire principles
and making use of microimplants for anchorage, the technique has been greatly simplified
and has introduced significant treatment alternatives in 21st century orthodontics.
Application of Orthodontic Forces
Screws are manufactured from a titanium alloy
and a degree of osseointegration between the
screw and bone does take place. The success of
the micro screw implant is not dependent on
osseointegration, however; it is dependent
purely on the mechanical retention of the screw
in the bone. Research has shown that forces may
be applied immediately after placing the microimplant.12 The mechanical retention can suc-
Figure 9. Microimplants placed in the unattached
alveolar mucosa will become buried in the soft tissue
during treatment. It is necessary to extend a ligature
wire from the head of the microimplant through the
mucosa into the oral cavity. (Color version of figure is
available online.)
190
H.-M. Kyung
References
1. Fujita K: Orthodontic appliance (multiple lingual orthodontic appliance). Japan patent 55-48814, 1976
2. Kurz C: Fixed lingual orthodontic appliance for the
maxillary arch. US patent 256961, 1981
3. Kyung HM: Individual indirect bonding technique
(IIBT) using set-up model. J Korea Dent Assoc 27:73-82,
1989
4. Kyung HM, Park HS, Sung JH: The mushroom bracket
positioner for lingual orthodontics. J Clin Orthod 36:
320-8, 2002
5. Kyung HM, Park HS, Bae SM, Yoon DY: Severe bialveolar
protrusion case treated with lingual plain wire appliance
& micro-implant anchorage. Dental Focus 24:1330-1343,
2004
6. Kyung HM, Kim IB: Case reports of Class I malocclusion
treated with lingual appliance. Korean J Orthod 21:309324, 1991
7. Kyung HM, Park HS, Bae SM, Sung JH, Kim IB: Development of orthodontic micro-implants for intraoral anchorage. J Clin Orthod 37:321-328, 2003
8. Lee JS, Park HS, Kyung HM: Microimplant anchorage
for lingual treatment of a skeletal Class II malocclusion.
J Clin Orthod 35:643-647, 2001
9. Kyung HM, Park CS, Sung JH: Miniscrew anchorage in
lingual orthodontic treatment for severe lip protrusion.
Inf Orthod Kieferorthop 35:259-265, 2003
10. Kyung HM, Park HS, Sung JH, Kim IB: Lingual orthodontic treatment—the development of the mushroom
bracket positioner (MBP) and its application. Int
Orthod 1:21-47, 2003
11. Kyung HM, Park HS, Bae SM, Sung JH, Kim IB: The
lingual plain-wire system with micro-implant anchorage.
J Clin Orthod 38:388-395, 2004
12. Melsen B, Costa A: Immediate loading of implants used
for orthodontic anchorage. Clin Orthod Res 3:23-28,
2000
 0
0