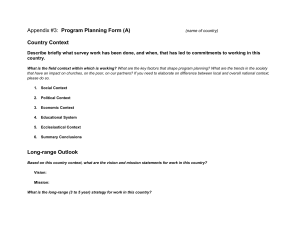
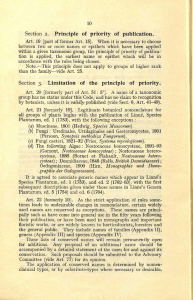
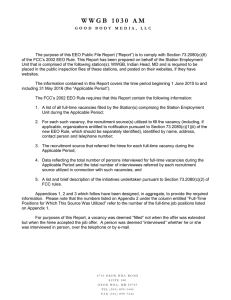
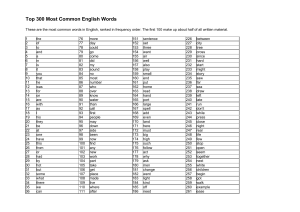
Appendectomy Namir Katkhouda, MD, FACS,* and Andreas M. Kaiser, MD, FACS† A lmost exactly 300 years after the first description of appendicitis by Heister (1683), Semm performed the first laparoscopic incidental appendectomy by transsecting the appendix between two endoloops (1982).1,2 Laparoscopic surgery has since rapidly evolved and established itself in surgical practice and has become fairly routine. Although there is still ongoing debate about indications and technical refinements in various surgical fields, there has been ample documentation in the literature that laparoscopic appendectomy for acute appendicitis is at least equally safe as conventional open appendectomy. Despite the initial lack of a statistical advantage of the laparoscopic approach compared to open appendectomy, the most recent data seem to corroborate a solid benefit trend, with faster recovery, fewer complications, and improved cosmesis after laparoscopic appendectomy.3,4 This benefit has been shown through all age groups, but elderly patients in particular experience an advantage with the minimally invasive approach.5 Indications The laparoscopic approach does not result in a change of indications. Any patient who, based on the overall assessment, requires and qualifies for a surgical exploration for suspected acute appendicitis is a likely candidate for the laparoscopic procedure. In addition, there are a number of patients in whom, despite multiple tests, diagnostic uncertainty persists; in these patients, a diagnostic laparoscopy with possible appendectomy may be indicated to clarify and treat the causative pathology. Another group of patients for whom a laparoscopic approach is recommended are those requiring an interval appendectomy and whose initial acute episode was treated nonoperatively, for example, by means of percutaneous drainage of an appendiceal abscess combined with antibiotics. *Department of Surgery, Keck School of Medicine, University of Southern California, Los Angeles, CA. †Department of Colorectal Surgery, Keck School of Medicine, University of Southern California, Los Angeles, CA. Address reprint requests to Namir Katkhouda, MD, Department of Surgery, Keck School of Medicine, University of Southern California, 1510 San Pablo Street, Suite 514, Los Angeles, CA 90033. E-mail: nkatkhouda@ surgery.usc.edu 8 1524-153X/05/$-see front matter © 2005 Elsevier Inc. All rights reserved. doi:10.1053/j.optechgensurg.2004.12.004 Surgical Technique Operating Room Setup and Port Placement After induction of general anesthesia, the patient is placed in the supine position with at least the left arm (or both arms) tucked to give both the surgeon and the assistant comfortable working space. A Foley catheter and lower-extremity sequential pneumatic compression devices are placed routinely. Insertion of a gastric tube for decompression depends on the patient’s presentation. The abdomen is prepared and draped in a sterile fashion, exposing the entire abdomen from the epigastrium to the pubis and including both groins. Standard laparoscopic equipment is usually sufficient, as long as it includes some atraumatic graspers, Babcock forceps, scissors, suction/irrigation, and a harvest bag. Although the surgeon’s assistant initially stands on the opposite side until the ports have been inserted and the pneumoperitoneum has been established, eventually both the surgeon and first assistant will be on the left side of the patient facing the monitor placed on the right side (Fig. 1). A pneumoperitoneum is created in a standard fashion, with either the Veress needle technique, the open Hasson technique, or by insertion of a nontraumatic bladeless Optiview port (Ethicon Endosurgery, Cincinnati, OH). “Port planning” means the steps and considerations taken before inserting the actual ports to optimize the usability of the placed ports, ie, maximizing safety while minimizing morbidity and negative aesthetic impact. Considerations not only include the patient’s habitus and anatomic landmarks (eg, epigastric vessels), but also aesthetic expectations and the presence and location of scars from previous abdominal operations. As a result of the planning, the surgeon should have a clear concept of where the ports will be inserted, the size of ports needed, and the intended use of a particular port, for example, insertion of a stapling device or specimen retrieval bag will typically require a larger port than insertion of grasping instruments and endoloops alone. Care must be taken to avoid a “knitting needle” effect between instruments and the laparoscope, that is, all ports should be placed in such a manner that they have free movement and do not interfere with each other. We prefer insertion of the ports in symmetric triangulation. The laparoscope is at the umbilicus. Two further ports are inserted symmetrically in the left and right lower quadrant. In a male patient, these are at McBurney’s point and at the corresponding point on the left side (Fig. 2A). In a female patient, it is advisable for cosmetic reasons to move the port positions down toward the pubic Appendectomy 9 Figure 1 Patient positioning. Figure 2 Trocar placement in male (A) and female (B) patients. 10 N. Katkhouda and A.M. Kaiser Figure 3 Exposure of the appendix and creation of a window in the mesoappendix. hair (Fig. 2B). Other settings (eg, left lower quadrant plus suprapubic midline port or a port right under the right costal margin) are not recommended because they have functional disadvantages or may be cosmetically inappropriate. Exposure of the Appendix After insertion of the ports, a quick diagnostic laparoscopy is performed to either confirm the diagnosis or assess other pathology (eg, female organs, diverticulitis, inguinal hernias, liver/gallbladder disease, carcinomatosis). The sur- Figure 4 Mobilization of the cecum for retrocecal location of the appendix. geon’s assistant and camera holder then moves to the patient’s left side, cephalad to the surgeon. The patient is brought into the Trendelenburg position with the right side elevated to facilitate the exposure of the right lower quadrant. The surgeon’s left hand operates a Babcock grasper (Ethicon Endosurgery, Cincinnati, OH) to retract the cecum and subsequently to expose the appendix (if the appendix is in its usual paracecal position). Particularly if the appendix is significantly inflamed and friable, it is advisable not to grasp Appendectomy 11 Figure 5 Endoloop technique: transection of the appendix between two loops. the appendix itself but rather to place the Babcock around it or at the level of the mesoappendix (Fig. 3). Occasionally, an endoloop can be placed around the appendix and mesoappendix to create a handle to hold the appendix. The surgeon’s right hand operates a Kelly grasper or electrical scissors to create a window in the mesoappendix (Fig. 3). If the appendix is not clearly identifiable because it is retrocecal, the cecum needs to be mobilized and retracted medially (Fig. 4). Transsection Techniques Once the appendix has been completely skeletonized, it is amputated at the base. In general, there is no need for inversion of the appendiceal stump, but it is of crucial importance to divide the appendix in healthy appearing tissue, if necessary at the level of the cecum, to avoid a breakdown of the ligation or stapler line. There are two possibilities to divide the appendix and the mesoappendix—the endoloop technique and the stapling technique. The former is cheaper and requires only a 5-mm port on the left side; however, it requires more skill and may initially take more time. The stapling technique needs less skill and initially saves time, but it is more expensive and it will require a 12-mm port. Endoloop Technique In this technique, the mesoappendix is first divided by means of cautery, and the appendix is subsequently divided between two endoloops. The appendix should be clearly visible from tip to base. Special bipolar cautery forceps are used to cauterize and “crush” the mesoappendix. Care has to be taken not to touch and burn adjacent loops of bowel with the hot forceps. Portions of the mesoappendix are cauterized and subsequently cut with the scissors until the base of the appendix is identified and completely freed. Two endoloops are inserted and tied at the base, leaving sufficient space to trans- sect the appendix. After transsection, the appendiceal stump mucosa is cauterized carefully (Fig. 5). Stapling Technique In this technique, a 30-mm white vascular endostapler (Ethicon Endosurgery) is used to divide the mesoappendix, and a 30-mm blue endostapler is employed for the appendix as close as possible to the cecum, leaving only a very short stump. A window is created at the base of the mesoappendix in the avascular plane between the base of the appendix and the appendiceal artery. The first stapler with appropriate cartridge (white for vessel, blue for bowel) is inserted and fired (Fig. 6), followed by a second stapler for completion of the transection (Fig. 7). Care should be taken to avoid a “junk yard” by losing unused staples into the surgical field. After firing, the staplers should therefore be opened very carefully, just enough to release the tissue, but then they immediately should be closed again before dropping the unused staples. Specimen Retrieval Care is needed to avoid contamination of the abdomen and port site wounds; the appendix is therefore placed in a retrieval bag before removing it from the abdomen. Alternatively, if the appendix is not too large, it can be pulled into the port and withdrawn with the port. Rupture of the retrieval bag within the abdominal wall because of an inadequate fascial gap should be avoided under any circumstances. If delivery of the endobag is difficult, it is advisable to widen the fascial incision. Irrigation and Drainage The purpose of irrigation is to remove all debris, purulent fluid collections, and blood from the surgical area. In early phlegmonous appendicitis without any pus, there is no ad- 12 N. Katkhouda and A.M. Kaiser Figure 6 Stapler technique: transection of the mesoappendix. vantage to irrigation but rather risks spreading contaminated fluid throughout the abdomen. Otherwise, with the appendix removed, a thorough lavage of the area is performed. In particular, the pelvis has to be well exposed and any residual contaminated fluid should be aspirated and irrigated by retracting the sigmoid colon and exposing the pouch of Douglas. In the overwhelming majority of cases, a drain is not nec- Figure 7 Stapler technique: transection of the appendix. essary. However, if residual contaminated fluid is to be left in the peritoneal cavity or if the appendiceal/cecal stump is of suboptimal quality, placement of a small drain may be prudent. It should be brought in through a separate 4- to 5-mm incision in the right lower quadrant, that is, not through one of the trocar sites, and laid along the cecum into the pelvis to drain those dependent areas. The drain can be removed after a few days once the quality of the fluid is serosanguinous. Appendectomy 13 Figure 8 Retrograde dissection with transection of the appendiceal base first, followed by its mobilization towards the tip. Technical Variations Retrograde Appendectomy When the tip of the appendix is not clearly visible, a retrograde appendectomy can be performed with the stapler (Fig. 8). The visible base of the appendix is transected after creation of an appropriate window, followed by the mesoappendix, and finally the whole appendix is dissected from the base to the tip. This is performed as in open surgery and does not require specific skills. Difficult Appendicitis When the surgeon encounters a gangrenous or perforated appendicitis or an appendiceal phlegmon, it can be difficult initially to recognize the appendix. In these circumstances, it Figure 9 Fingeroscopy. N. Katkhouda and A.M. Kaiser 14 may be necessary to mobilize the cecum first. This mobilization should be as conservative as possible to avoid opening and contaminating retroperitoneal spaces. The cecum can then be flipped over and the appendix visualized. If this is still not possible, “fingeroscopy” or conversion to an open procedure has to be considered (Fig. 9). The former technique involves removal of the port from the right lower quadrant and insertion of the index finger to restore the tactile sensation and to perform blunt, atraumatic mobilization similar to the open procedure but under laparoscopic guidance.6 This will speed up the procedure and should be considered as the last step in situations where conversion seems inevitable. Fingeroscopy can only be performed if the right lower quadrant incision is close enough to the surgical area (see section on port placement). If still no satisfactory progress is made, the only way forward is to convert to an open operation. The projection of the cecum is marked on the abdominal wall via transillumination of the laparoscope, and an incision is then made appropriate to the operation to be performed. Laparoscopically Assisted Appendectomy In some cases, especially in children where the appendix is extremely long and the working space is small, the “assisted” technique is an easy way of performing an appendectomy. The mesoappendix is first controlled by means of bipolar electrocautery. The right lower quadrant port is then removed with the appendix inside. The whole appendix is exteriorized and ligated outside the abdomen before the cecum is pushed back inside the abdomen. though pregnancy in and of itself is not necessarily a contraindication for the laparoscopic approach,7 the following requirements have to be respected. The surgeon ought to be an experienced laparoscopist, the operation should under no circumstances be prolonged, and the trocars should always be placed via an open access technique. Control of Intraoperative Bleeding Although bleeding complications are relatively rare, they most commonly arise from the appendiceal artery. Bleeding related to trocar placement (eg, epigastric or iliac vessels) should be avoided by careful and visually controlled insertion of the ports. Prompt reaction in a controlled fashion aims at localizing the bleeder and stopping it without delay. Diffuse and uncontrolled cautery use to arrest bleeding should be avoided. It may be helpful to bring in a 2 ⫻ 2 cm radiopaque-labeled gauze to temporarily compress the area. With a suction tip in one hand and a fine grasping instrument in the other, the surgeon must identify and grasp the vessel on which a clip or figure-eight stitch may be placed. If the bleeding cannot be stopped in a timely fashion, the procedure has to be converted to an open operation. Postoperative Care The postsurgical management depends on both the intraoperative findings and the patient’s symptoms. Duration of antibiotics is determined by the extent of the inflammation and the presence of perforation, rather than by the surgical approach. Early ambulation and resumption of an oral diet are encouraged; the latter should be advanced as tolerated. Special Problems Diagnostic Uncertainty and Normal Appendix Encountering a normal appendix occurs in patients in whom either preoperative studies and assessment were inconclusive or proved to be falsely positive. A careful assessment has to be performed of the whole peritoneal cavity, including running the small bowel. If a different intraabdominal pathology is found, that disease process should be appropriately treated and the appendix should be left in place. If no other pathology is found, we recommend removing the appendix and having it assessed by the pathologist. Pregnancy Acute appendicitis with any type of appendectomy carries a risk for the pregnant patient and for her unborn fetus. Al- References 1. Semm K: Endoscopic appendectomy. Endoscopy 15:59-64, 1983 2. Kaiser AM, Corman ML: History of laparoscopy. Surg Oncol Clin N Am 10:483-492, 2001 3. Guller U, Hervey S, Purves H, et al: Laparoscopic versus open appendectomy: outcomes comparison based on a large administrative database. Ann Surg 239:43-52, 2004 4. McKinlay R, Mastrangelo MJ Jr: Current status of laparoscopic appendectomy. Curr Surg 60:506-512, 2003 5. Guller U, Jain N, Peterson ED, et al: Laparoscopic appendectomy in the elderly. Surgery 135:479-488, 2004 6. Katkhouda N, Mason RJ, Mavor E, et al: Laparoscopic finger-assisted technique (fingeroscopy) for treatment of complicated appendicitis. J Am Coll Surg 189:131-133, 1999 7. de Perrot M, Jenny A, Morales M, et al: Laparoscopic appendectomy during pregnancy. Surg Lap Endosc Perc Techn 10:368-371, 2000