World Health
Organization
\VHOiSS106.2046
ENGLISH ONLY
-
EXPERT COMNflTTEE ON BIOLOGICAL STANDARDIZATION
Geneva, 23 to 27 October 2006
6
2%
-Gp
CALIBWTION OF THE PROPOSED WHO 2nd INTERIVATIONAL STANDARD FOR
PROTEIN S IN PLASMA, HUMAN (031228)
Anthony R Hubbard, Lynne J Weller and *Alan B Heath
Haemostasis Section and *Biostatistics Section, National Institute for Biological
Standards and Control, Blanche Lane, South Mjmms, Potters Bar, Herts. EN6 3QG
United Kjngdom
O World Health Organization 2006
+
,
-
All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20
Avenue Appia, 1211 Geneva 27, Switzertand {tel.: +41 22 791 3264; fax: +42 22 791 4857; e-mail: [email protected]). Requests
for permission to reproduce or translate WHO publications -whether for sale or for noncommercial distribution - should be addressed
to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]).
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion
whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its
authorities: or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for
which there may not yet be full agreement.
The mention of specific wmpanies or of certain manufacturers' products does not imply that they are endorsed or recommended by
the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted. the
names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication.
However, the published material is being distributed vvithout warranly of any kind, either expressed or implied. The responsibility for
the interpretation and use of the materiat lies with the reader. In no event shall the Worfd Health Organization be liable for damages
arising from its use. The named auUlors [editors] alone are responsible for the views expressed in this publication.
WEIOilBS/O6*204S
Page 3
PROPOSAL
It is proposed that the WHO 2nd IS Protein S Plasma (03/228) be assigned the mean estimates
calculated relative to the NTHO1 st IS as follows:
0.83 1U;ampoule
Total antigen
Free antigen 0.8 1 IUiampoule
Function
0.77 IUiampoule
PRODUCT SGTMMRYFOli THE PRUPOSEI) Ct;:HO 2nd IS PROTEIN S PLASM4
{03/228)
Presentation
sealed glass 5vlzL DIN ampoules
l . Cm-adenine anticoagulant
2. HEPES buffer 40 mmol/L Jinal
concentration
3. Glq'cine 0.96% (w/v)Jirzal concentration
CoefJicient of variation of the liquid fill
0.09 % based on 70 check-weight ampoules
Liquid filling weight (g)
mean 1.0063 g (range 1.0042 g - 1.0086 g)
Residual moisture after lq'opl-tilisationand
secondary desiccation (%)
mean 0.064 % {n = 6)
Dry weight (g)
mean 93.0 mg (n = 6)
Reconstitution volume and fluid
1.0 ntL of distilled wafer
Storage temperature
Address ofprocessi~lgfacilidy
-20 "C
LVIBSC,Potfers Bar, EAr6 3QG
Address of storcrgefaciliQ
ATBSG, Potters Bar, EX6 3QG
WHOIBS106.2046
Page 4
1
INTRODUCTION AKI) OBnCTIVES
Protein S is a vitamin K-dependent plasma protein which acts as a cofactor for the anticoagulant
hnction of activated Protein C (1,2). Congenital deficiency of Protein S is associated with a predisposition for recurrent thrombosis and therefore the measurement of plasma Protein S is
included in the investigation of "thrornbophilic"conditions (3,4,5). Protein S exists in plasma as
a free rnolecule and also bound to the C4b-binding protein but only the free molecule acts as a
cofactor for activated Protein C (3.6). Three methods are routinely used to characterise Protein S
in plasma: total antigen methods measure both free and bound Protein S whereas &ee antigen and
hnctional methods measure only free Protein S. The W O 1st Intemational Standard (931590)
was calibrated for ail three analytes (7). In addition to the diagnosis of "tlzrumbophifia" the
estimation of Protein S is also under consideration, by the European Phamacopoeia, for the
quality control of a therapeutic product, vims-inactivated fresh frozen human plasma.
The WHO 1st International Standard Protein S Plasma (931590) was established by WHO in
1995 (7). This standard was calibrated relative to locally collected normal plasma pools and
assigned a value in International Units where 1 IU represents the amount of Protein S in 1 m1 of
pooled normal plasma, Values were assigned for the three analytes: total antigen, free antigen
and function. As a result of the similarity of the consensus mean values the same value (0.90
IU/ampoule) was adopted for all three analytes. The WHO l st IS has been used steadily over the
last l l years with annual despatch between 200 and 300 ampoules. The current stocks consist of
approximately 200 ampoules and it is therefore necessary to calibrate a replacement preparation.
This standard is intended to be used in the in vitvo diagnostics field and relates to case 4 of the
principles set out in IS0 17511.
This report presents the results of the calibration exercise for the proposed WHO 2nd IS Protein S
Plasma (031228). In common with the approach used for other U7H0 International Standards this
study included the assay of the proposed M O 2nd IS relative to both the current WHO 1st IS
(for continuity of the IU) and relative to locally collected normal plasma pools (as a check for
drift of the IU). In addition. a third lyophilised plasma preparation was also included in the study
(SSG:IS'TH Secondary Coaglation Standard Lot #3, SSC Lot #3) in order to check its calibration
for Protein S and also to evaluate the inter-laboratory variability of Protein S estimates in a
common test sample relative to the W O 1st IS and proposed WHO 2nd IS. This comparison
also addresses the issue of commutabilitlyI for the primary intended use of the proposed UXO 2nd
IS, the calibration of secondary reference plasmas, by allowing a comparison of different test
methods on a common test smiple.
@p=*g
WHOiSS/06.2046
Page 5
2
MATERIALS
2.1
WHO 1st IS Protein S Plasma (931590) - study code A
The WHO 1st IS was prepared in 1993 from a plasma pool derived from 17 normal healthy
donors and consists of sealed glass ampoules each containing 1.0 m1 of pooled plasma, freezedried. The WHO I st IS was established in 1995 with assigned values of 0.90 IUiampoule for
total antigen. free antigen and function (7).
2.2
Candidate WHO 2nd IS Protein S Plasma (031228) - study code B
Bulk Material The Proposed WHO 2nd IS u a s prepared from a plasma pool derived from 24
normal healthy donors (United Kingdom Blood Service, North London Blood Transfusion
Centre). Blood was collected using conventional venepuncture into CPD-adenine anticoagulant
at a nominal ratio of 63 m1 anticoagulant to 450 m1 whole blood. Each donation underwent
leuko-filtration followed by tsvo centrifugation steps after which the plasma was stored at -70 'C
until the day of filling. On the morning of the fill the plasma units were thawed in a waterbath at
37 'C and pooled. The final pool was buffered by the addition of HEPES m-12Hydroxyethyllpiperazine-NI-12-ethanesulfonic acid]) (final concentration 39 mmol/L) and
G1ycine (final concentration 0.96% w/v).
Safety Testing Individual donations were tested and found negative for HBsAg, antibodies to
HIV-I and -2 and antibodies to HCV. The donations were also tested as mini-pools and found
negative for the presence of HCV RNA using a PCR technique. The final freeze-dried
preparation has been tested and found negative for HBsAg: antibodies to HIV-l and -2 and HCV
RNA.
r$-""
+*
*S&>
Ampoule filling Filling was carried out in February 2004 by the Centre for Biological Reference
Materials. NIBSC, Pot-ters Bar. UK. Each glass ampoule received 1 m1 of the pool, followed by
freeze-dving and secondary desiccation according to the requirements for International
Biological Standards (8). The ampoules mere sealed in an atmosphere of dry nitrogen gas and
placed into storage at -20 'C on 10 March 2004. The precision of the liquid fill ttas estimated
using 70 check-weight ampoules spaced evenly throughout the fill. The mean filI weight was
1 .0063 g and the range was 1 .a042 - 1 .a086 g with a coefficient of variation of 0.09 %.
Tests on the freeze-dried material Mean dry weight from 6 estimates was 0.0930 g (CV 0.12
$4). Residual moisture was estimated using Karl Fischer titration and a mean of 0.064 % (CV
4.29 %f \.;as calculated from 6 estimates.
Number of ampoules and storage A total of 5.380 ampoules are stored at -30"C at the
National Instikrte for Biological Standards and Control, Potters Bar.UK.
WHOiBSi06.2046
Page 6
2.3
SSCiISTH Secondaq Coagulation Standard Lot fit3 - study code C
The SSCIISTI-I Secondary Coagulation Standard Lot $3 fSSC Lot 83) was prepared by a
commercial manufacturer from a pool of 55 litres of normal plasma collected using apheresis.
SSC Lot # 3 consists of rubber-sealed, scre~v-cappedvials each containing 1 m1 of pooled normal
pIasma, freeze-dried.
2.4
Locally collected Normal Plasma Pools - study code NI, Nz
Participants were requested to prepare two plasma pools according to the instructions in the
protocol (Appendix I); pool NI for inclusion in assays l and 2; pool Nzfor inclusion in assays 3
and 4. It was requested where possible that the local pools should be used freshly for all assay
methods. If this was not possible the use of frozen aliquots for the estimation of total and free
antigen was allowed. Details on the status of the normal pools used by each laboratory are given
in Appendix 2. In summary the following pools were used:
Total antigen: I l labs used frozen pools, 5 labs used fresh pools, l lab (number 1 1) used fresh
pools for assays 1 and 2 and frozen aliquots for assays 3 and 4, 1 lab (number 4) used a
lyophilised pool. A total of 404 donors were used to prepare the fresh and frozen pools.
Free antigen: l 0 labs used frozen pools, 6 labs used fresh pools, l lab (number 11) used fresh
pools for assays l and 2 and frozen aliquots for assays 3 and 4, 1 lab (number 15) used a fresh
pool for assay 1 and a frozen aliquot for assay 2, 1 lab (number 4) used a lyophilised pool. A
total of 466 donors were used to prepare the fresh and frozen pools.
Function: 4 labs used frozen pools, 6 labs used fresh pools, 1 lab (number 1 1) used fresh pools
for assays 1 and 2 and frozen aliquots for assays 3 and 4. A total of 329 donors were used to
prepare the pools.
3
COLLABORATIVE STUDY
3.1
Participants
Twenty three laboratories from 12 countries agreed to join the calibration exercise and each
laboratory was assigned a study code number to retain confidentiality. Results were returned by
20 laboratories from 1 1 countries and these are listed in Appendix 3 (list order not consistent with
code number). The participants comprised 15 clinical laboratories, 4 manufacturers of diagnostic
calibrant plasmas or therapeutics and l regulatory institute.
w-HOiBS/O6.204d
Page 7
3.2
Assay methods and study design
Laboratories were requested to use their routine assay methodology as far as possible and to
foHow balanced assay designs as described in the study protocol (Appendix 1). A detailed
description of the assay methods used by each laboratory is given in Appendix 2. A summsy of
the methods is given in Table 1.
Table 1
Summav of assay methods used in the calibration exercise.
Measuremer?t
Assay merhod
EL IS4 (1S), ii~2muno-fztrbidimet~-ic
(a,Electro-inznaunodiffusioi"~
Total antigen
If)
g+%#G&
-53
Free antigen
Funcfioil
ELISA - PEGpreciaitation (7,ELISA - monoctovtal antibodies (6)
Immuno-turbidimeaic (51, Electro-imrnt~raod~fi~sio~
(1)
Clotting ~netlzods:Prufein S Ac (21, Pro S/Profein S (S), StacZot (4)
Participants were requested to carry out four independent assays for each method using fresh
samples of A, B and C and locally collected normal plasma pools (X1and N2) in each assay. It
was requested that N I be included in assays l and 2 and N2 be included in assays 3 and 4. Where
a laboratory used two methods it was necessary to use the same samples for both methods.
Where a laboratory used three methods two sets of samples A, B and C were provided.
3.3
Statistical analysis
Wherex~erpossible assays were analysed as parallel line bioassays (9), relating assay response to
log concentration. This analysis requires linear response (or transfomed response) lines, when
plotted against log concentration, which are parallel for all preparations included in the assay. AI1
results were plotted and the validity of the assays assessed both visually and by analysis of
variance.
*
S
*
g$$y
X*&
In most cases all of the returned data was included in the construction of the dose-response
relationships and yielded satisfactory linearity and parallelism. In a small number of cases some
data points at the extreme ends of the dose-response relationships were deleted to achieve
linear&. Subject to this minor manipulation ail but 5 assays were considered valid and inciuded
in the study, Estimates were calculated relative to the assigned value of 0.90 Itiiampoule for a11
ana1q.tes on the WHO 1st IS (sample A) and relative to an arbitray value of 1.0 uniu'ml for the
normal pools {sample H), Estimates of SSCiISTH Lot #3 were calculated relative to the
proposed VSXO2nd IS using an arbitray value of 100%.
In one case there was insuficient data to allow parallel line analysis ( h c t i o n assags for
Laboratorl; number 21). In this case the results have been based on the Iaboratory's own
estimates,
WHOiBSIO6.2046
Page 8
Variability within laboratories (between assays) and between Iaboratories was measured by
calculating geometric coeMicients of variation (GCV) (10). Results of assays both within and
between laboratories were combined to give the geometric mean. Detection of outlying results
was performed using Duncan's test ( l l).
4
RESULTS
4.1
Number of assays and acceptabilitjr of data
The overall performance of the laboratories was good with satisfactory parallelism between doseresponse relationships. Only 5 out of a total of 189 assays were excluded from the analysis (see
below). Estimates of intra-laboratory variability for the Proposed WHO 2nd IS were acceptably
low and similar for estimates calculated relative to both the WHO 1st IS and the normal pools:
the GCVs for 52 out of 96 estimates were below 5% and 80 out of 96 estimates were below 10%.
4.2
TOTAL PROTEIN S ANTIGEN
A total of 7 1 assays were returned from 18 laboratories. All four assays from one laboratory
(number 20) were excluded from the study on the basis of extreme variability between duplicate
samples and the lack of a valid dose-response relationship. All laboratories performed 4 assays
except for laboratory 3 which performed 3 assays.
4.2.1 Estimates for the Proposed WHO 2nd IS
Estimates relative to the WHO 1st IS (n=17) ranged from 0.77 to 0.93 IUiml with an overall
mean of 0.83 IUiml and inter-laboratory variability (GCV) of 5.62 % (Table 2 and Figure la).
Estimates relative to the normal pools (n=16) ranged from 0.61 to 0.97 units per m1 with an
overall mean of 0.82 units per m1 and inter-laboratory variability (GCV) of 12.05 % (Table 2 and
Figure I b). There were no outlying estimates and there was no significant difference between the
estimates calculated relative to the W O 1st IS and the nomal pools. Comparison of the
estimates obtained relative to either the fresh or frozen normal pools (mean estimates 0.82 and
0.80 unitsiml respectively) indicated no significant difference (Table 2). A thorough comparison
of the different methods used was compromised by the predominance of the ELISA method for
14 out of 17 estimates. However, no sipifrcant differences were detected bemeen the different
methods (Table 2).
4.2.2 Estimates for the SSCflSTH Standard Lot ff3 relative to the Proposed WHO 2nd IS
Estimates were calculated relative to a nominal value of 100% assigned to the Proposed WHO
2nd IS and ranged from 93.3 to 108.7 Oib with an overall mean of 104.3 % ( ~ 1 7 md
) interlaboratory variabilil?; (GCV) of 3.82 % (Table 3 and Figure 2). There were no outlying results,
Re-calculation of the mean estimate relative to the proposed assigned value for the Proposed
\;tiNOiSSi06.2046
Page 9
'l+'HO 2nd IS (0.83 Iti'iml) gave a mean value for the SSC Lot #3 of 0.87 1Uiml. No significant
differences were found bemeen the different methods (Table 3).
4.2.3 Variabiliw of the local normal plasma pooIs
Estimates for total antigen in the frozen pools, relative to the WHO 1st IS, ranged from 0.90 1.35 IUiml with a mean of l .04 IUiml (n-l l). Estimates for the fresh pools ranged from 0.92 1.22 1U!ml with a mean of 1 .O1 1U:ml (n=6). There was no significant difference bemeen the
fresh and frozen pools. Combining the estimates for fresh and frozen pools gave an overall mean
value of 1.01 IUlml.
Ea*$- ~ ~ $
-#$*
4.3
FR_EE PROTEIN S ANTIGEN
A total of 74 assays were returned from 19 laboratories. One assay was excluded (lab 20) from
the study on the basis of extreme variability between duplicate samples and the lack of a valid
dose-response relationship. All laboratories performed 4 assays except for laboratory 15 which
performed 2 assays.
4.3.1
--*ez
Q$
Estimates for the Proposed WHO 2nd IS
Estimates relative to the WHO 1st IS (n=19) ranged from 0.71 to 1.03 IU/ml with an overall
mean of 0.8 1 IUlml and inter-laboratory variability (GCV) of 9.02 % (Table 4 and Figure 3a).
Estimates relative to the normal pools (n=18) ranged from 0.65 to 0.97 units per m1 with an
overall mean of 0.81 units per m1 and inter-laboratory variability (GCV) of 13.16 % (Table 4 and
Figure 3b). There u7ereno outlying estimates and there was no significant difference between the
estimates calculated relative to the W130 1st IS and the normal pools. Comparison of the
estimates obtained relative to either the fresh or frozen normal pools (mean estimates 0.8 1
unitsirnl for both) indicated no significant difference (Table 4). There were no significant
differences between the different types of method used for estimates relative to either the W O
1 st IS or the normal pools (Table 4).
4.3.2 Estimates for the SSClLSTH Standard Lot #3 relative to the Proposed %'NO 2nd IS
Estimates u7ere~alculatedrelative to a nominal value of 100% assigned to the Proposed W O
2nd IS and ranged from 98.4 to 1 28.6 96 u ith an overall mean (n= 19) of l 13.7 $41and interlaboratory variability (GCV) of 6.5 1 % (Table 5 and Figure 4). There were no outlying results.
Re-calcutation of the mean estimate relative to the proposed assigned value for the Proposed
WHO 2nd IS (0.8 l Iti'iml) gave a mean value for the SSC Lot 83 of 0.92 IC!ml. There were no
significant differences between the different types of method used for estimates relative to the
proposed i W O 2nd IS (Table 5).
WHOfBSf06.2046
Page 10
4.3.3 Variabiliv of the loeal normal plasma pools
Estimates for free antigen in the frozen pools, relative to the M%O 1 st IS, ranged from 0.91 1.20 ILJirnl with a mean of 1.03 IU!ml (n=12). Estimates for the fresh pools ranged from 0.81 1.16 IlJiml with a mean of 0.98 IU1ml (n=8). There was no significant difference bemeen the
fresh and frozen pools. Combining the estimates for fresh and frozen pools gave an overall mean
value of l .OO IUlml.
4.1
PROTEIN S FUNCTION
A total of 43 assays from 1l laboratories were returned and none were excluded from the study.
4.4.1 Estimates for the Proposed WHO 2nd IS
Estimates relative to the WHO 1st IS (n=l I ) ranged from 0.73 to 0.82 lU/ml with an overall
mean of 0.77 IUiml and inter-laboratory variability (GCV) of 3.33 % (Table 6 and Figure 5a).
Estimates relative to the normal pools (n-l I) ranged from 0.67 to 0.89 units per m1 with an
overall mean of 0.75 units per m1 and inter-laboratory variability (GCV) of 7.88 % (Table 6 and
Figure 5b). There were no outlying estimates and there was no significant difference between the
estimates calculated relative to the W O 1st IS and the normal pools. Comparison of the
estimates obtained relative to either the fresh or frozen normal pools (mean estimates 0.75
unitsiml for both) indicated no significant difference (Table 6). There were no significant
differences between the different types of method used for estimates relative to either the W O
l st IS or the normal pools (Table 6).
4.4.2 Estimates for the SSCIISTH Standard Lot #3 relative to the Proposed WHO 2nd IS
Estimates were calculated relative to a nominal value of 100% assigned to the Proposed W O
2nd IS and ranged from 97.2 to 108.9 % with an overall mean (n=l l ) of 102.0 % and interlaboratory variability (GCV) of 4.35 % (TabIe 7 and Figure 6). There ~ ~ eno
r eoutlying results.
Re-calculation of the mean estimate relative to the proposed assigned value for the Proposed
WHO 2nd IS (0.77 IUiml) gave a mean value for the SSC Lot ff3 of 0.79 lU/ml. Comparison of
estimates, relative to the proposed WHO 2nd IS, indicated a significant difference between
laboratories using the ProsiProtein S kits (mean 105.9 %} and the Staclot kit (mean 98.9 %; p =
0.028) (Table 7).
4.4.3 Variabiliv of the local normal plasma pools
Es~imatesfor function in the frozen pools, relative to the B-0 1st IS, ranged from 0.97 - 1.18
fU:rnI with a mean of 7 .O3 Itiiml (n=5). Estimates for the fresh pools ranged from 0.83 - l . l 7
ItiimI ivith a mean of 1.02 IUml (n=7). There was no simificant difference between the fresh
and frozen pools, Combining the estimates for fresh and frozen pools gave an overaII mean value
of t '02 IUiml.
WHOiBSi06.2046
Page 11
5
STABILITY STUDIES
Stability of the Iyophilised proposed % X 0 2nd IS is under continuous assessment &rough both
accelerated degradation and real-time studies. Both studies commenced on 0 1 March 2006 and
will continue for the lifetime of the standard.
p3%*
Considerable data is available to support the long-term stability of Protein S in lyophilised pooled
normal human plasma when stored at -20 'C. Studies on the WHO 1 st IS Protein S Plasma
(93/590) reported no loss of total antigen, free antigen or fknction in ampoules stored at -20 'C
after 7.5 years of storage (in comparison to ampoules stored at -1 50 'C) and accelerated
degradation studies produced valid predictions indicating less than 0.1 % loss per year for all 3
analytes (Appendix 4). In addition. data on a second lyophilised normal pooled plasma, the
SSClTSTH Secondary Coagulation Standard Lot #2, has indicated no significant difference in
Protein S values between the original calibration exercise in 1999 and re-testing in 2005
(Appendix 5). Similar good stability can be expected from the proposed WHO 2nd IS when we
consider the similarity of sourcing, processing and physical properties between the WHO 1st IS
and proposed WHO 2nd IS.
5.1
Accelerated degradation study
This study involves the potency estimation of ampoules stored at elevated temperatures (4,20, 37,
45 'C) and the bulk storage temperature (-20 'C) relative to ampoules stored at -70 'C. The
observed relative loss of potency at elevated temperatures is analysed using the Arrhenius
equation in order to provide a prediction of loss per year for ampoules stored at various
temperatures (12). Testing is performed at various sampling times, typically after 3 months
(June '06), 6 months (September '06) and 1 year (March '07) of storage. Thereafter sampling is
performed every year or two years depending on the observed rate of loss.
Ampoules were placed into storage on 01 March 2006 and this report covers the initial testing
performed after 14 weeks storage by NIBSC. At least four independent estimates for total
antigen (ELISA method). free antigen (Immuno-turbidimetric method) and function (clotting
method) for each storage temperature were obtained using fresh ampoules in each assay. Mean
relative estimates for ampoules stored at 20, 37 and 45 'C are presented in Table 8 as a % of the
ampoules stored at -70 'C.
Storage for 14 weeks at the highest temperatures used in the accelerated degradation study
resulted in smlafl amounts of loss for all 3 analytes and there was insuscient data to enable a
vatid prediction of loss for total antigen. However, valid predictions of loss were obtained Ebr
free antigen (0.063 ?4per year at -20 "C) and firnetion (0,226 96per year at -20 'C). Considering
the short period of storage, at elevated temperatures, these initial predictions are encouraging
particularly for free antigen where the estimate is similar to that obtained for the WHO 1st IS
f 0.040 016 per year at -20 "C) (Appendix 4). The low level of observed degradation coupled with
the limited amount of data early in the stability study is typically associated with larger
confidence l irnils for the mean predictions of loss (upper limits 1.190 94and 3.1 19 % per year for
WHOBS106.2046
Page 12
free antigen and function respectively). Experience has indicated that we can expect reductions
in both the mean predicted loss and the upper 95 % confidence limits as data from more timepoints and storage temperatures are added. Further testing will be carried out after 6 and 12
months storage and this will additionally include ampoules stored at +4 'G. This additional data
will allow the generation of more precise predictions of stability to support the long-term use of
the WHO 2nd IS.
5.2 Real-time stability
The ability to compare ampoules stored at the bulk storage temperature (-20 'C) relative to
ampoules stored at -70 'C will also provide an objective real-time assessment of the stability of
the standard at -20 'G. Such comparisons are only meaninghl after several years of storage,
however, they can provide increased confidence in the validity of using a current standard to
calibrate the replacement preparation as demonstrated for the WHO I st IS (Appendix 4).
5.3
Stability after reconstitution
It is useful to indicate a suitable period of use after reconstitution of the standard. However, it is
impossible to take into consideration the large variation in local storage conditions and ambient
temperature experienced by users. For this reason the post-reconstitution stability of the standard
has been investigated under one set of conditions which should be easily reproducible by users this requires the transfer of reconstituted standard into a stoppered plastic tube which is stored in
melting ice. Investigations performed at NIBSC have indicated that, under these conditions,
there is no detectable loss of total antigen, free antigen or function for assays which are
commenced up to 4 hours post-reconstitution. This period is sufficient for numerous assays of
Protein S to be commenced. This information will be included in the Instructions For Use and
users will be advised that local validation will be necessary if the reconstituted standard is stored
under different conditions.
'
The use of frozen aliquots of the proposed WHO 2nd IS cannot be recommended since the effect
of freezing and thawing, under local conditions, is unpredictable.
The main objective of the present study is the calibration of a replacement WHO International
Standard for Protein S in plasma. In common with the precedent es~blishedwith other WHO IS
the calibration exercise included the assay of the proposed WHO 2nd IS relative to both the
cunent %%WO 1st IS and to tocatty collected nomal plasma pools. The former comparison
allows for the evaluation ofcontinuiq between the WHO 1st and 2nd IS whereas the second
comparison provides a check for the possibilit33 of drift in the IU from its original definition
against Local nomat pools when originalIy calibrated in 1995 (7). Confidence in the use of the
lVHO 1st IS for the calibration of the proposed WHO 2nd IS relies on the demonstration of its
stability and hence the continued t~alidityof its assigned value. This has been provided through
stability assessments based on acceIerated degradation studies and also real time comparison of
WHOiBS106.2046
Page 13
ampoules stored at -20 'C with ampoules stored at -1 50 "C {Appendix 4). This data indicates that
the WHO I st IS has been extremely stable and has exhibited no detectable degradation.
@
<G
&
*&
b*
A major consideration in the suitability of locally collected normal pools. as a check for drift of
the IU. is the use of a sufficient number of donors in order that the mean estimates will
approximate to the population mean. The number of individual donors used to prepare the local
normal pools in the present study ranged from 329 - 466 and this compares favourably with the
original calibration of the WHO 1 st IS where approximately 260 donors were used (7). In
common with previous calibration exercises the participants were asked to use fresh local normal
plasma pools rather than frozen aliquots wherever possible, particularly in the assays of hnction.
This request was based on the concern that freeze-tha~vingof local pools may lead to the
degradation of Protein S so invalidating the use of frozen pools. Hosvever, the results in the
present study indicated no significant difference between estimates relative to the fresh or frozen
pools with the mean estimates relative to both almost identical for all three analytes, This is a
strong indication that the Protein S has not been affected by freeze-fiawing and that the
combination of estimates from both fresh and frozen local normal pools is valid. Combined
mean estimates for all 3 analytes in the local normal pools, relative to the WHO 1st IS, ranged
from 1.OO to 1.02 IUiml. This is an extremely encouraging finding since it supports and
reproduces the original definition of the IU established in 1995 when the WHO 1st IS was
calibrated relative to local normal pools.
The quality of the data returned from participants was generally high and only 5 assays were
excluded from the entire study. This is apparent from the estimates of intra-laboratory variability
(GCV) which were less than 10% for 80 out of 96 estimates. There was overall good agreement
behveen laboratories for estimates of all 3 analytes and this is apparent from the estimates of
inter-laboratory variability which ranged from 3.33 - 9.02 % vs the WHO 1st IS and from 7.88 13.16 % vs the local normal pools. The latter estimate of variability is particularly encouraging
considering that each laboratory used a different normal plasma pool.
No outlying estimates were identified and there were no significant differences between the types
of method used for all three analytes. However, in common with the calibration of the WHO I st
IS it is apparent that the inter-laboratory variability was greatest for the estimates of free antigen
and this is in large part due to the methods using PEG precipitation which were the most variable
for any method type (GCV 12 O h vs W O l st IS and 18.5 % vs local normal pools).
For all three analytes there were no significant differences behveen estimates calculated relative
to the U%O l st IS and the local normal pools. In fact the overall mean rlalues from both routes
of caleuiation were almost identical (0.83 vs 0.82 for total antigen; 0.8 1 vs 0.8 1 for free antigen;
0.77 vs 0.75 for function). This is a very encouraging result for tcvo reasons:
- it supports the original definition of the Itl used to calibrate the KWO 1st IS by reproducing an
identical value in the present study.
it supports the stability data which indicate that the I W O 1st IS has remained stable since its
estabIishment in 1985.
-
WfIOR3Sl06.2046
Page 14
Based on these findings it is proposed that the WHO 2nd IS be assigned the mean estimates
calculated relative to the WHO l st IS:
Total antigen
Free antigen
Function
0.83 IUlampoule (GCV 5.6 %)
0.81 IUlampoule (GCV 9.02 9%)
0.77 IUlampouIe (GCV 3.33 %)
The SSC Standard Lot 543 was included in order to evaluate the inter-laboratory variability of
estimates for a common test sample, relative to the proposed WHO 2nd IS. Estimates of interlaboratory variability (GCV) for all 3 analytes were low, ranging from 3.82 - 6.51% relative to
the proposed W O 2nd IS. This finding is encouraging as it demonstrates that the proposed
WHO 2nd IS should maintain good harmonisation in Protein S estimates between different
laboratories for all 3 analytes. As found with the calibration of the proposed WHO 2nd IS, the
largest inter-laboratory variability was associated with estimates of fkee antigen and particularly
with the ELISA methods using PEG precipitation (GCV 10%). No significant differences were
found between the different methods used for the estimation of total and free antigen. However,
a significant difference: at the 5% level, was found between two kits used for the estimation of
function despite overall very low inter-laboratory variability for estimates of function (CCV
4.35%). A similar result was also found for estimates of SSC Lot #3 function calculated relative
to the WHO 1 st IS (results not shown). It is worth emphasising that no such significant
differences, between methods, vr7erefound for estimates of function in the proposed W O 2nd IS
relative to the WHO 1st IS. The low overall inter-laboratory variability for estimates of the
common test sample (SSC Lot #3) relative to the proposed WHO 2nd IS (total antigen GCV
3.82%, free antigen 6.51%, function 4.35%) indicate that the proposed WHO 2nd IS will
continue to rnaintain harmonisation in Protein S estimates between laboratories.
7
PROPOSAL
It is proposed that the WHO 2nd IS Protein S Plasma (031228) be assigned the following mean
estimates calculated relative to the WHO 1st IS (931590):
Total antigen
Free antigen
Function
8
0.83 IUlampoule
0.81 IUlampoule
0.77 IUlampouIe
mSPOF;SES FROM PaTLCIPLYTS AND SSCIISTH
A1I 20 part.icipants have agreed with the proposed assigned potencies.
The calibration report has aIso been circulated to members of the SSCiISTH Plasma Coagulation
Inhibitors sub-committee and presented orally at the annual meeting (Oslo. June 30 2006). The
SSC has approved the submission of this proposal to the Expert Committee on Biological
Standardisation of iVFIO.
WHOiBS/06.2046
Page 15
l.TliiaIker FJ (1 980) Regulation of activated protein C by a new protein. J Biol Chem 255;
5521-4
Walker FJ (198 1) Regulation of activated protein C by protein S. The role of
phospholipid in factor Va inactivation. J Biol Chem 256; 11 128-3 1
Comp PG, Nixon RR, Cooper MR, Esmon CT (1984) Familial Protein S deficiency is
associated with recurrent thrombosis. J Clin Invest 74; 2082-8
Schwarz HP, Fischer M, Hopmeier P, Batard MA, Griffin JH (1984) Plasma Protein S
deficiency in familial thrombotic disease. Blood 64; 1297-300
Broekmans AW, Bertina M, Reinalda-Poot J, Engesser L, Muller HP, Leeuw JA,
Michiels JJ, Brommer EJP, Bri&tE (1985) Hereditary Protein S deficiency and venous
thromboembolism. A study in three Dutch families. Thromb Haemost 5% 273-7
Dahlback B (1 984) Interaction between vitamin K-dependent protein S and the
complement protein C4b-binding protein. Seniin Thromb Hemostas 10; 139-48
Hubbard AR (1 997) Standardisation of Protein S in Plasma: Calibration of the I st
International Standard. Thromb Haemost 78; 1237-4 1
Campbell PJ (1974) International biological standards and reference preparations. 1 .
Preparation and presentation of materials to serve as standards and reference preparations.
J Biol Standardisation 2; 249-67
Finney DJ (1978) Statistical methods in biological assay. 3" edition Charles Griffin.
London.
Kirkkkrood TBL ( l 979) Geometric means and measures of dispersion. Biometrics 35;
908-9
Duncan DB (1975) T-tests and internals for comparisons suggested by the data.
Biometrics 3 1; 339-359
Kirkwood TBL, Tydeman MS ( l 984) Design and analysis of accelerated degradation
tests for the stability of biological standards 11. A flexible computer program for data
analysis. J Biol Standardisation 12; 207-1 4
WHOISSIO6.2046
Page 16
10
INSTRUCTIONS FOR USE
A draft Instructions for Use is presented in Appendix 6
The efforts of the participants in the collaborative study, the members of the Plasma Coagulation
Inhibitors sub-committee and the staff of the Centre for Biological Reference Materials (NIBSC)
are gratehlly acknowledged.
WHO/BS/06,2046
Page 17
* - overall combination excluded lab 4 (lyophiiiised pool) and included a single mean figure for
lab I l which used both frozen and fresh pools
WHOiEZS/06,2046
Page 18
Table 3 Elstirnates for Total Antigen in SSC Lot #3 ( G ) vs Proposed WHO 2nd IS (B)
Estimates are expressed relative to the proposed WHO 2nd IS (assigned 100%)
WMOBS/06,2046
Page 19
Table 1 Estimates for Free Antigen in the Proposed WHO 2nd IS (B)
* - combination excluded lab 4 (Iyophilised poolf and included a single mean f i ~ r for
e labs I I & 15 which used
both frozen and fresh pools
WHOBS/06.2046
Page 20
Table 5 Estimates for Free Antigen in SSC Lot #3 (C) vs Proposed WHO 2nd IS (B)
Estimates are expressed relative to the proposed WHO 2nd IS (assigned 100%)
WHOiBS/06,2046
Page 21
Table 6 Estimates for Function in the Proposed \.WO 2nd IS (B)
gfgfj$&
S
?
?
&
*W
* - combination tncluded a single mean figure for lab 1 1 which used both frozen and fresh pools
WHOntZS106.2046
Page 22
Table 7 Estimates for Function in SSC Lot #3 (C) vs Proposed W O 2nd IS (B)
~stimatesare expressed relative to the proposed WHO 2nd IS (assigl
Table 8 Residual potencies for ampoules stored for 14 weeks at elevated temperatures expressed as a % of
ampoules stored at -70 'C
Storage temp <C)
I
I
Free a~tigen
Residual relative potencies are the means of at least 4 estimates
I
Function
WHOISSf05.2046
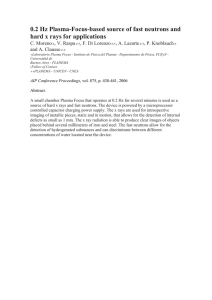
Page 23
Mean iaboratov estimates for total antigen in the Proposed \%%Cl
to a) WHO 1st IS and, b) local normal plasma pools
1: ;
Figure l a
2nd IS Protein S Plasma (031228) relative
Proposed WHO 2nd IS vs WHO 1st IS: Total Antigen
!
lUlml
Figure Ib Proposed WHO 2nd IS vs normal pools: Total Antigen
E ELISk
lmmunoturb
Immunodiffusion
WHOR3S/05.2046
Page 24
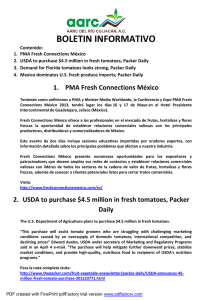
FIGURE 2
Mean taborator?. estimates for total antigen in the SSCIISTH Seeondav Coagulation Standard Lot #3 relative
to the Proposed W-O 2nd IS Protein S Plasma
60
70
80
90
100
110
120
130
% of proposed WHO 2nd IS
ELBA
lmmunoturb
lmmunodiffusion
140
150
WHOISS106.2046
Page 25
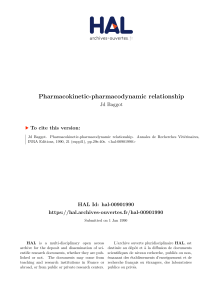
Mean l a b o r a t o ~estimates for free antigen in the Proposed W O 2nd IS Protein S Plasma @3/2ZS) relative to
a) WHO 1st IS and, b) local normal plasma pools
Figure 3a Proposed WHO 2nd 1s vs WHO 1st IS: Free Antigen
12
7
ii
i
Figure 3b Proposed WHO 2nd IS vs normal pools: Free Antigen
', 1
06
07
OF,
C9
*!l
ijn~tsiml
m ELISA Mab
ELISA PEG
2 Immunoturb
m lmmunodtffusion
WH01BSi06.2046
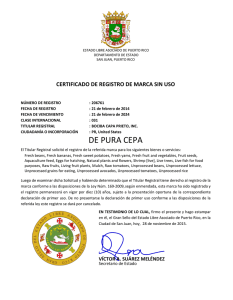
Page 26
Mean laboratory estimates for free antigen in the SSCIISTH Secondary Coagulation Standard Lot #3 relative
to the Proposed W710 2nd IS Protein S PIasma
% of proposed WHO 2nd IS
ELISA Mab
ELlSA PEG
lmmunotu&
lmmunodiffusion
WHOif3Si06.2046
Page 27
FIGURE 5
Mean laboratorl). estimates for function in the Proposed WHO 2nd IS Protein S PIasrna (031228) relative to a)
WHO 1st IS and, b) local normal ptasma pools
Figure 5a Proposed VVHO 2nd IS vs WHO 1st IS : Function
Figure 5b Proposed WHO 2nd IS vs normal pools: Function
L ProSiProtern S
ljStadot
Protein SAC
WHOfBS106.2046
Page 28
Mean laboratay estimates for function in the SSCIISTH Seconday Coagulation Standard Lot #3 relative to
the Proposed WHO 2nd IS Protein S Plasma
"50
60
70
80
90
100
%
- of
ProSfProtein S
110
120
sample
Staclot
Protein SAC
130
140
150
WHOIBSIO6.2046
Page 29
APPENDIX 1
PROPOSED WHO 2nd INTEWATIONAL S T m D A m PROTEIX S PLASMA (0312281
PROTOCOL FOR THE COLLDOR4TIVE STUDY
1
A
B
C
N I , N2
2
SAMPLES INCLUDED IN THE ASSAYS
- WHO l st IS Protein S Plasma (93/590)
- Proposed WHO 2nd IS Protein S Plasma (031228)
- SSC1ISTE-I Secondary Coagulation Standard Lot #3
- fresh normal plasma pools prepared locally (see section 5)
STORAGE AND RECONSTITUTION OF SAMPLES A, B and C
Store the unopened ampoules and vials of A, B and C at -20°C or below. Allow the ampoules
and vials to warm to room temperature before reconstitution. Tap gently to ensure that all of the
contents are in the lourer part of the ampoules and vials. Reconstitute by adding I .O m1 of
distilled water. Dissolve the contents with gentle agitation at room temperature. When
reconstitution is complete transfer the entire contents to stoppered plastic tubes and store at 4OC
during the assay period.
3
GENERAL PLAN OF THE STUDY
You are requested to carry out 4 assays by each method using fresh ampoules and vials for each
assay. If you are performing one or two methods then only 4 ampoules1vials of A, B and C are
provided and it will therefore be necessary to carry out estimates by both methods on the same
ampoules and vials (where applicable). If you are performing 3 different methods then two sets
of ampoules and vials will be provided.
AI1 assays shouId be carried out on freshly reconstituted ampouleslvials and fresh normal
plasma pools (Pil, NZ). If this is not possible you may use frozen aliquots of the normal pools
@ I ,NZ)for estimation of Total and Free antigen. Estimates of Protein S hnction must be
performed on fresh samples.
The 4 assays should be spread over 2 separate days1sessions as foIlows:
If you are unable to prepare the two fresh local pools W,,
NZ)you map alternatively inelude a single local
frozen piasma pool in all 4 assays.
WHOISS105.2OJS
Page 30
4
ASSAY DESIGN
All four preparations (A, B, C and N) are included in each of the 4 assays. A minimum of 3
ditutions of each preparation should be tested, in replicate, within each assay. Please follow a
balanced assay design such as the optimal 24-pIace assay described below. In the follo~iing
design, each letter refers to a separate set of three or more dilutions and A, A* and B, B* etc.
refer to fresh sets of dilutions (replicates) made from the same ampoule.
D e s i ~ nfor 24-place assay
Assay l
Assay 2
Assay 3
Assay 4
5
A
B
G
N2
B
C
B
B
C
NI
A
A
NI
A
N2
C
NI*
A*
N2*
C*
G*
NI*
A*
A*
B*
G*
B*
B*
A*
B*
C*
NZ*
COLLECTION OF F m S H NORMAL PLASMA
Collect fresh normal plasma on two separate days to prepare pools N1 and N2. The method of
collection for the fresh normal plasma is an important part of the study and should be
standardised as far as possible according to the following protocol.
Doptors
Normal healthy volunteers, excluding pregnant women, women taking oral
contraceptives and known carriers of the FV Leiden allele. Take blood from as many different
individuals as possible, on two separate days. If possible, use a minimum of 8 different donors
for each pool; if this is not possible, some of the same individuals can be used again, but the aim
is to have as many diEerent donors as possible from each laboratory.
A~zticoagulartt
0.109 moliL tri-sodium citrate or a mixture of tri-sodium eitrate and citric
acid with a total citrate concentration of 0.109 moliL. Add 9 volumes of blood to l volume of
anticoaelant.
Ce~trifugation
Blood should be centrifuged at 4'C as soon as possible after collection
either at 50,000 g for 5 minutes or at 2:000 g for 20 minutes.
Storage
Keep the plasma pool in a plastic stoppered tube at if°C dwing the assay session.
Freeze aliquots of each pool (NI,NZ)for subsequent assays of antigen where it is not possible to
perfom the testing on fresh samples.
!VIIOIBS/06.2046
Page 31
Please return your raw assay data on the enclosed results sheets to allow analysis at NIBSC.
PIease ensure that your results are presented as true raw data (eg. optical densiv) rather than as %
or units relative to an in house standard. You are also invited to calculate your own estimates for
B relative to A and NI .Nzif you wish (see enclosed results sheet). Please return the results
sheets and questionnaire to:
Dr A R Hubbard. Division of Haematology, NIBSC, Blanche Lane, South Mimms, Potters Bar,
Herts. EN6 3QG United Kingdom
Fax: 1.44 (0) 1707 646730 E-mail: [email protected]
L~rhNo
l
3
3
4
5
6
7
8
J!
I0
II
13
IJ
l5
18
IY
20
21
2.2
23
Totcrl Antige I?
Method
ELISA (Rtikr:,uatihodies)
--
EL1,SA
(Asserc~hrcrm'Total PS Stugo)
Ellcrctm-~mmzanodifusio~t
(EIDI~IAY
Tcachnoclone)
EIAIS.4(Uako antibodies)
E;LISA (Dcrko untihodies)
ELISA
(As~.er~zchram
Total PS Stczgo)
ELISA
(~fs.sercachromTotal PS Stago)
_E%IkTA(D~ikoai.rtibo&es)
L;I,lSA (Ijaku anfihoclie.~)
ELISIil
(/4,sscrachrom Total P?r Stugo)
ELILSA (Dzko nntihodies)
It?rt?tzmo-ltlrbidi~~jefric
Liulest Stcrgo
lmrrzu~~u-turhidi~tietric
Lzatest LStagn
ELISA (Reaak)
ELI'SA (Llako ~rntihodies)
EIdiSA (Duku arttibodies)
ELdlSA (Duko antibociiea
Pools
Frozen
--
Fresh
Free Antigen
Method
ELISA i.PEG (Duko antibodies)
--
ELISA
(As.serachrorn Free PS Stago)
Lj~oplzilised Electro-immunod~if~sio~?
+ PEG
(EIDFIX Technoclone)
Frozen
ELISA + PEG (Uako antibodies)
Frozen
ELISA + PEG (Dako antibodies)
Frozen
Imrrzuno-ttirbidirnetric
(IL Test Free Protein S kitj
Frozen
ELISA
(Asserachrt~mFree PS Stugo)
Fresh
ELISA
(Coaliza Protein S-Free)
Frozen
ELISA + PEG (Dako antibodies)
Fresh 1/2 ELISA
Eiozen 3/4 (Asseraehrom Free PS Stago)
Fresh
ELISA + PEG (Dako antibodies)
Fresh
Irrzmtmo-turhidii~zetric
(IL Test Free Protein S kit)
-Ittzmuno-turbidimetric
(Liatest Free PS Stugo)
Frozen
Imntzmo-tnrbidimetric
(Liatest Free PS Stago)
Frozen
ELISA (Reaads - Monoclona(j
Frozen
ELISA + PEG (Dako arftibodies)
Frozen
ELISA + PEG (Duko antibodies)
Frozen
Immuno-turbidimetric
(IL Test Free Protein S kit)
Fresl?
ELISA (Reaads - &noclonal)
Pools
Frozen
-Fresh
Fzinctiorr
Method
-Dude Behring kit Protein SAC
Stago ,Ttaclot kit
m-
Fresh
Fresh
Lyophilised
--
Frozen
Frozen
kkozen
--IL Hernosil Pro S
Frozen
Frozen
Hetnosil Protein S
Frozen
Fresh
--
Frozen
Fresh 1/2
Frozen 3/4
Fresh
Fresl?
Fresh1
Frozen 2
Frozen
Frozen
Frozen
Frozen
Fresh
Dude Behring kit Protein SAC
Stago Staclot kit
IL Hemosil Pro S
--
--
Fksh
Fresh I/2
Frozen 3/41
Frcsl?
-Stago Staclot kit
Frozen
--
--
IL lIemo,sil Pro S
IL Iiernosil Pro S
ELIS4 (AfF~rilJi
Biologicals
Fresh
Stugo Stuclot kit
atrtihodi'esi
APPENDIX 2
Details of inethodology and status of normal plasma pools used by the participants
Frozen
Fresh
WWOiBSi06.2046
Page 33
APPENDIX 3
LIST OF PARTICIPANTS
Dr E Bigurrzi ,' D Asti
A Bianchi Bonomi
Hemophilia & Thrombosis Center
Milan, Italy
Dr P Baker
Dept of Haematology
John Radcliffe Hospital
Oxford. United Kingdom
Dr M Stegnar
Dept of Angiology
University Medical Centre
Lubijana, Slovenia
4
\
.
f@#@
*.
Mr A Smith
Royal Liverpool University Hospital
Liverpool, United Kingdom
Dr h4 Johnston
Hemostasis Reference Laboratory
Henderson Research Center
Hamilton ON
Canada
Dr B Kerbl
Technoclone GmbH
Vienna, Austria
Dr M Smith
Dept of 13aematology
Canterbury District Health Board
Christchurch, New Zealand
@$
L
-
Dr A R Hubbard / MS L J Weller
Haemostasis Section
Biotherapeutics Group
NIBSC
Potters Bar, United Kingdom
Dr J C J Eikenboom
Dept of Haematology
Leiden Cniversity Medical Centre
Leiden, The Netherlmds
Dr R Marlar
Veteran Affairs Medical Center
Oklahoma Ciry, OK
United States of America
WHOPBS105.2046
Page 34
Professor I Pabinger
Haematology & Haemostaseolo~
University Clinic for Internal Medicine
Vienna, Austria
Dr R Zadro
Div of Haematology (4;r Coagulation
Clinical Hospital Center
Zagreb, Croatia
Dr K Mertens Mrs J Rentenaar
Dept. of Blood Coagulation
Sanquin Blood Supply Foundation
h s t e r d a m . The Netherlands
Dr J Patzke
Dade Behring
Marburg, Germany
Dr D D Castellone
Dept of Special Coagulation
New York Presbyterian Hospital
New York, XY
United States of America
MS S Berrier / Dr M-0 Couche
QC Laboratory
Diagnostica Stago
Franconville, F r a n ~ e
Mr S Lees
Dept of Haematology
University of Wales
Cardiff, United Kingdom
Mr P Cooper i Dr S Kitchen
Coagulation Unit
Royal Hallamshire Hospital
Sheffield, United Kingdom
Dr J Conkie
Dept of Haematology
Royal Infimarq.
Glasgow. United Kingdom
Dr C Legnani ' Dr G Palareti
Dept of h g i o l o g y & Blood Coagulation
University Hospital S Orsola
Bologna. Italy
FVNOIBSI06.2046
Page 35
Summary of stability data for WHO 1st IS Protein S plasma (931590)
1
Real-time stability
Ampoules from the bulk storage temperature (-20 'C) were tested, in 6 separate assays,
directly relative to ampoules which have been stored at -1 50 'C for 7.5 years. The results
are consistent with no significant relative loss for ampoules stored at -20 'C.
Relative potency (as 7-6 o f - 150 "Cantpoules)
Total antigen
99
95
94
I04
97
101
Mean 98 %
95% cl (94 % - I02 %)
Free antigen
I0I
I02
I00
99
I0I
97
Mean 100 %
95% cl (98 % - I02 %,l
Mean 99 %
95% cl (94 % - I03 %)
2
Accelerated degradation study
Ampoules have been stored at elevated temperatures (-1-4,+20 'C) for 7.5 years. A
prediction of the degradation rate has been calculated from the observed loss relative to
ampoules stored at -1 50 'C by fitting to the Arrhenius equation.
Storage temp ("C)
-20
L‘$
+20
Predicted % loss per
year at -20 "C
-
iWean residual potency (% vs I50 "Campoules)
Total antigen
98 3
96 8
84 8
Free antigen
I00 0
93 3
65 9
0.039 %
0.040 %
3
Conefusions
Results from both the real-time comparison and the accelerated degradation study over
7.5 years indicate that the ?VHO 1st IS Protein S Plasma (931590) is extremely stable
when stored at the bulk storage temperature of -20 "C. These findings therefore validate
the use of the WHO I st IS to calibrate the proposed WHO 2nd IS Protein S Plasma
(031228).
WHOiSS106.2046
Page 36
APPENDIX 5
Comparison of estimates (It'lml) for Protein S in the SSClISTH Secondary
Coagulation Standard Lot #2 from the original calibration in 1999 and re-testing in
2005.
Parameter
Calibi.ation 1999
Re-testing 2005
Total antigen
Free anrigen
Functior?
0.88 I t;iml /GC V 4.I %l
0.92 IC'iml (GC V 7. %)
0.73 ILL'mI (GCV 6.8 %)
0.86 ItVmf (GC'-E 6.4 %)
0 88 IUIini (GCV 2.8 %l
0.76 Ib%l fGC V 6.7 %)
WNORSS106.2046
Page 37
APPENDIX 6
DRAFT INSTRUCTIONS FOR USE FOR TEE WHO 2nd INTEWATION;IX,
STANDAW PROTEIN S PLASMA
WHO 2nd INTE&VATIONAL, STANDARD FOR PROTEIN S, PLASMA,
HUMAN
NIBSG code: 031228
Version 01, Dated 07 July 2006
*
S
@##
The 2nd International Standard for Protein S, Plasma, Human, consists of ampoules
(code-labelled 031228) containing l m1 aliquots of pooled fresh human plasma, freezedried. This standard has been assigned potencies for total and free Protein S antigen and
for Protein S function,
Reference to WHOIBS document wili be inserted here
2 CAUTION
#
h
@p
2.1
THIS PREPARATION IS NOT FOR ADMINISTRATION TO H U M m S .
2.2
A 'Material Safety Data Sheet' is included in these Instmctions.
2.3Each individual donation was tested for HBsAg and for antibodies to HCV and HIV-1
and -2 and found to be negative. The donations were also tested for HCV RNA in mini
pools and found to be negative. The final freeze-dried Standard has also been tested for
HBsAg, antibodies to HGV, antibodies to HIV-I and -2 and HCV RNA and found to be
negative. However, as with all preparations of human origin, this material cannot be
assumed to be free from infectious agents. Suitable precautions should be taken in the
use and disposal of the ampoule and its contents. Such safety procedures probably ill
include the wearing of protective gloves and avoiding the generation of aerosols. Care
should be exercised in opening ampoules or vials, to avoid cuts.
USE OF THE STAND
3
ALVPOULE
AND DImCTIONS FOR OPENING THE DIN
Unopened ampoules should be stored at -20 'C or below. Allow ampoules to warn to
room temperature befitre opening.
DIN ampoules have an "easy-open' coloured stress point, where the narrolv ampoule stem
joins the wider ampoule body, Tap the ampoule gently to collect the material at the
bottom (labelled) end, Ensure that the disposable ampoule safety breaker provided is
pushed dokm on the stem of the ampoule and against the shoulder of the ampoule body.
Hold the body of the ampoule in one hand and the disposable mpoule breaker colrering
WHOBS106.2046
Page 38
the ampoule stem between the thumb and first finger of the other hand. Apply a bending
force to open the ampoule at the coloured stress point, primarily using the hand holding
the piastic collar.
Care should be taken to avoid cuts and projectile glass fragments that might enter the
eyes, for example. by the use of suitable gloves and an eye shield. Take care that no
material is lost from the ampoule and no glass falls into the ampoule. Within the ampoule
is dry nit9.ogen gas at slightly less than atmospheric pressure. A new disposable ampoule
breaker is provided with each DIN ampoule.
Reconstitute the total contents of each ampoule of the Standard with 1.0 ml of distilled
water, using gentle shaking. Do not attempt to weigh out any portion of the freeze-dried
material. Transfer the reconstituted Standard to a plastic tube and keep on melting ice.
Under these conditions the Standard has been found to be sufficiently stable to be used
over a 4 hour period. Storage of the reconstituted Standard under different conditions
must be validated locally by users.
4
ASSIIGNEI) ACTIVITIES
The 2nd International Standard was calibrated in an international collaborative study
involving 20 laboratories for Total Protein S antigen, Free Protein S antigen and Protein S
function by assay against the 1st International Standard (931590) and locally collected
normal pooled plasma. The standard was established by the WHO Expert Committee on
Biological Standardisation in October 2006. The following values have been assigned to
the 2nd International Standard:
Total Protein S antigen
Free Protein S antigen
Protein S funetion
0.83 IU per ampoule
0.81 IU per ampoule
0.77 IU per ampoule
Uncertainty: the International Unit of 031228 is assigned without uncertainty. The
uncertainty of the ampoule content of 031228 may be considered to be the coefficient of
l~ariationof the ampoule filling, which was determined to be 0.09 %.
The 2nd International Standard was prepared in February 2004 from a plasma pool
collected from 24 normal healthy donors. Blood was coIIected into CPD-adenine
anticoagulant in plastic packs, at a ratio of 450 m1 blood to 63 rnl anticoagulant. Each
donation undement leuko-filtration and centrifugation before storage at -70 '(1. The
units mere thawed in a waterbath at 37 'G and pooled on the day of filling. The final pool
was buffered by the addition of E P E S m-[2-Hydroxyethylpiperazine-X-[2ethanesulfonic acid]) to a final concentration of 39 mmoliL and Gfycine to a final
concentration of 0.96 % W ~ J .
WHO/%S/OS.2046
Page 39
6
DISTIRIBUTION IIC'TO AMPOULES
The pooled plasma was kept at 4 'C throughout distribution into approximately 5,500
ampoules, then freeze-dried and secondary desiccated according to the requirements for
International Biological Standards (l), The coefficient of variation for the liquid f3I was
0 . 0 M and the mean fill %eight was 1.0063 g (range 1,0042 - 1.0086 g). The final
freeze-dried material has a mean dry weight of 0.093 g and mean residual moisture of
0.063 %.
WOlB5106.2046
Page 40
7
STABILITY
It is the poIicy of WHO not to a s s i g an expiry date to their international reference
materials. They remain valid with the assigned potency and status until withdrawn or
amended. Reference materials are held at NIBSC within assured, temperature-controlled
storage facilities. Reference materials should be stored on receipt as indicated on the
label. Guidance on the stability after reconstitution is given in section 3. Users who have
data supporling any deterioration in the characteristics of any reference preparation are
encouraged to contact NIBSC.
8
CITATION
In all publications including data sheets in which this material is referenced, it is
important that the WHO status of the preparation, specified by the title of the preparation,
the name and address of the WHO International Laboratory for Biological Standards at
NIBSC and the NIBSC code number are cited and cited correctly.
9
PRODUCT LIABILITY
Information emanating from NIBSC is given after the exercise of all reasonable care and
skill in its compilation, preparation and issue, but is provided without liability in its
application and use.
This product is intended for use as a laboratory standard or reference material. It is the
responsibility of the user to ensure that heishe has the necessary technical skills to
determine the appropriateness of this product for the proposed application. Results
obtained from this product are likely to be dependent on conditions of use and the
variability of materials beyond the control of NIBSC.
NIBSC accepts no liability whatsoever for any loss or damage arising from the use of this
product, whether loss of profits: or indirect or consequential loss or otherwise, including,
but not limited to, personal injury other than as caused by the negligence of NIBSC. In
particular, NIBSC accepts no liability whatsoever for:(i) results obtained from this product; andior
(ii) non-delivery of goods or for damages in transit.
In the event of any replacement of goods following loss or damage a customer accepts as
a condition of receipt of a replacement product, acceptance of the fact that the
replacement is not to be construed as an admission of liabilie on NIBSC's behalf.
10
1.
REIFERESCE
Campbell PJ (1974) J Biol Standardization, 2,249-267
WHOiBSi06.2046
Page 41
1l
FURTHER INFOMUTION
Please contact:
standards~~nibsc.ac.uk
National Institute for Biological Smdards and Control
Blanche Lane, South Mimms, Potters Bar, Hertfordshire, EN6 3QC, UK
Telephone: 4-44 (0) 1707 64 1000 Fax:
12
1-44 (0) 1707 64 1050
ACmOWLEDGENENTS
The efforts of the participants in the collaborative study, the members of the Plasma
Coagulation Inhibitors sub-committee and the staff of the Centre for Biological Reference
Materials (NIBSC) are gratefully acknowledged.
WHOISS105.2046
Page 42
13 MATENAL SAFETY SHEET
Toxicological properties
Effects of inhalation:
Effects of ingestion:
Effects of skin absorption:
Not established, avoid inhalation
Not established, avoid ingestion
Not established, avoid contact with skin