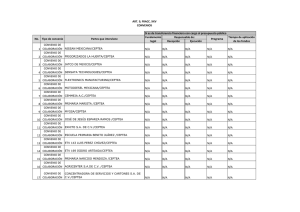
Guías Latinoamericanas de Hepatitis B
Anuncio

Guías Latinoamericanas de Hepatitis B Dra. Lucy Dagher Centro medico Docente La Trinidad Caracas-Venezuela @lucydagher Hepatitis B en Latinoamérica Prevalencia del HbsAg en Latinoamerica < 2% – Baja (0,3-2%) 2–7% – Intermedia (2,2-7%) > 8% – Alta (8-15%) Incidencia del HbsAg en Latinoamerica 0.7% >10% Ropero et al. J Clin Virol 2005; 34:S14-S19 Vacunación de ninos en Latinoamerica Cobertura de la Vacuna >90% 80-90% <80% No data (begun at 2005) Not implemented yet © J.M. Echevarría, 2008 Ropero et al. J Clin Virol 2005; 34:S14-S19 Genotipos VHB latinoamerica MV Alvarado-Mora 2013 Historia natural inmunoeliminación Treatment criteria for chronic hepatitis B: Comparison of Guidelines HBeAg Positive Guidelines HBeAg Negative HBV DNA (IU/mL) ALT HBV DNA (IU/mL) ALT APASL 2008 ≥ 20000 > 2 x ULN ≥ 2000 > 2 x ULN US Algorithm 2008 ≥ 20000 > ULN or positive biopsy ≥ 2000 > ULN or positive biopsy EASL 2009/2012 > 2000 > ULN > 2000 > 1 x ULN NIH Consensus Conference 2009 > 20000 > 2 x ULN or positive biopsy ≥ 20000 ≥ 2 x ULN or positive biopsy AASLD 2009 > 20000 > 2 x ULN or positive biopsy ≥ 20000 ≥ 2 x ULN or positive biopsy ALEH 2011 >2000 >ULN or positive biopsy >2000 >ULN or positive biopsy Objetivos del tratamiento • Major endpoints of treatment are[Lok 2009]: o Reduction of HBV DNA to undetectable levels (virologic response) o Loss of HBeAg with or without the appearance of antibodies to HBeAg (serologic response) o Reduction of ALT to levels considered normal (biochemical response) o Reduction in liver necroinflammation with or without an improvement of liver histology • Loss of HBsAg from serum, accompanied by the appearance of antibodies to HBsAg, is an additional goal, but is rarely achieved[Perrillo 2006] • Improvement in liver histology may occur with long-term use of nucleos(t)ide analogues[Marcellin 2013; Chang 2010; Schiff 2011] Goals of Therapy: 2 Distinct Patient Populations HBeAg positive (wild type) • HBeAg loss seroconversion • Suppression of HBV DNA • ALT normalization HBeAg negative (precore and core promoter mutants) • HBeAg seroconversion not an endpoint • Suppression of HBV DNA • ALT normalization Elección del tratamiento 1. Probabilidad de respuesta. 2. Edad. 3. Comorbilidades. 4. Presencia de cirrosis. 5. Potencia. 6. Resistencia a las drogas. 7. Costo de las drogas. 8. Efectos colaterales. 9. Preferencia del paciente. Indicacion de tratamiento ALT Carga Viral Histologia Recommended Dosing of Anti‐HBV Agents Agent Recommended Dosing Rout e Adult Children Interferon alfa SQ 5 MU daily or 10 MU 3 x per wk 6 MU/m2 3 x per wk (max: 10 MU) Peginterferon alfa-2a SQ 180 µg/wk Not approved Lamivudine PO 100 mg QD*† 3 mg/kg/day (max: 100 mg/day) Adefovir PO 10 mg QD* Not approved‡ Entecavir PO 0.5 mg QD (no previous LAM) 1.0 mg QD (if refr/resist to LAM)* Not approved Telbivudine PO 600 mg QD* Not approved Tenofovir PO 300 mg QD* Not approved *Dose adjustment needed if eGFR < 50 mL/min. †Persons coinfected with HIV should receive 150 mg BID. Should only be used in combination with other antiretrovirals. ‡Approved for ages 12 and older. Lok AS, et al. Hepatology. 2009;50:661‐662. Tratamiento de los pacientes Hbe(+) • Drogas de primera línea: o ETV, TDV, PegIFN a2a • El uso de lamivudina no esta recomendado debido a la alta resistencia – • En caso de no disponer de drogas de primera línea se pudiera indicar Lvd, Adv o Ldt, controlando periodocamente la respuesta virologica Tratamiento de los paciente Hbe (‐) Las drogas recomendada de primera línea son: • ETV, TDV y Peg IFN a2a • PegIFNa2a: o Pacientes jóvenes o Sin comorbilidades o Criterios de buena respuesta al tratamiento: • ALT elevada • niveles bajos de HBV DNA • En pacientes con niveles altos de HBV DNA: ETV o TDV • Ante la ausencia de respuesta primaria o respuesta suboptima durante el primer año considerar otra opción debido al riesgo de resistencia Peginterferon vs. Nucleos(t)ide Analogues Peginterferon Pro -Finite course of treatment -No resistance -Higher rate of HBeAg loss in 1 yr -Higher rate of HBsAg loss with short duration therapy Nucleos(t)ide analogues Con -SQ administration -Frequent AEs -Contraindicated in patients with decompensated cirrhosis, acute hepatitis, and immunosuppressed Pro -PO admin -Infrequent AEs -TDF/ETV approved for patients with decompensated disease Con -Need for longterm or indefinite therapy -Potential for drug resistance EASL Clinical Practice Guidelines: Management of chronic hepatitis B. J Hepatol 2009;50:227-242. Lok A, McMahon J. AASLD Practice Guidelines. Chronic hepatitis B: Update 2009. Hepatology 2009;50:1-36, ALEH 2011.19 When should PEG IFN be considered for HBV therapy? • Predictors of response – – – – – – ALT > 2-3 x UNL Low HBV DNA (< 107-8 log10 IU/mL) High histologic activity index Genotypes A or B > C or D Younger age Female Sex Absence of comorbidities/Patient preference/HCV co-infection EASL Clinical Practice Guidelines: Management of chronic hepatitis B virus infection. J Hepatol (2012), http://dx.doi.org/10.1016/j.jhep.2012.02.010. Lok A, McMahon J. AASLD Practice Guidelines. Chronic hepatitis B: Update 2009. Hepatology 2009;50:1-36. Scaglione SJ, Lok A. 20 Gastroenterology 2012;142:1360-1368. ALEH 2011. Undetectable* HBV DNA After 1 Yr of Treatment Undetectable* HBV DNA (%) Not head‐to‐head trials; different patient populations and trial designs HBeAg Positive 100 100 76 80 60 60 HBeAg Negative 80 67 88 90 93 60-73 63 51-63 60 40-44 40 20 40 13-21 25 LAM ADV LdT PegIFN 20 0 ETV TDF 0 LAM ADV LdT ETV *By PCR-based assay (LLD ~ 50 IU/mL) except for some LAM studies. Lok AS, et al. Hepatology. 2007;45:507-539. Lok AS, et al. Hepatology. 2009;50:661-662. TDF PegIFN Undetectable HBV DNA Over Time in HBeAg-Negative Patients Not head-to-head trials; different patient populations and trial designs Undetectable HBV DNA (%) Extended Treatment With Nucleos(t)ide Analogues vs Limited Duration (1 Yr) Peginterferon Treatment 100 90 96 93 80 100* 91 87 Entecavir Tenofovir Peginterferon 63 60 40 20 15 NA 0 *Single center study. 16 1 Yr 2 Yrs 3 Yrs Lok AS, et al. Hepatology. 2009;50:661-662. Marcellin P, et al. AASLD 2008. Abstract 146. Marcellin P, et al. AASLD 2009. Abstract 481. Marcellin P, et al. Gastroenterology. 2009;136:2169-2179. Baqai S, et al. AASLD 2009. Abstract 476. Lai CL, et al. Hong Kong International Liver Congress 2006. HBeAg Loss and Seroconversion in HBeAg+ Patients After 1 Yr of Treatment Not head‐to‐head trials; different patient populations and trial designs HBeAg Loss Outcome (%) 100 100 80 80 60 60 40 17-32 24 26 30 40 21 20 20 NA 0 LAM ADV LdT HBeAg Seroconversion ETV TDF PegIFN 22 12-18 22-27 23 21 21 LdT ETV TDF 0 LAM ADV PegIFN Lok AS, et al. Hepatology. 2007;45:507-539. Lau GK, et al. N Engl J Med. 2005;352:2682-2695. Marcellin P, et al. N Engl J Med. 2003;348:808-816. Chang TT, et al. N Engl J Med. 2006;354:1001-1010. Lai CL, et al. N Engl J Med. 2007;357:2576-2588. Marcellin P, et al. N Engl J Med. 2008;359:2442-2455. Janssen HL, et al. Lancet. 2005;365;123-129. Other Outcomes in HBeAg‐Positive Patients After 1 Yr of Treatment Not head‐to‐head trials; different patient populations and trial designs 100 ~ 90 ~ 80 77 80 72 74 Outcome (%) 68 68 49‐56 48 40 39 ADV LdT 69 65 60 41‐75 LAM ETV 53 TDF 50‐80 PegIFN 38 20 0 NANA 1 0 0 2 3.2 3 HBsAg Loss ALT Histologic Response Normalization Improvement Durability* *No/short duration consolidation treatment among LAM- and ETV-treated patients; most patients treated with ADV and LdT had consolidation. Lok AS, et al. Hepatology. 2009;50:661-662. Other Outcomes in HBeAg‐Negative Patients After 1 Yr of Treatment Not head‐to‐head trials; different patient populations and trial designs 100 LAM ADV Outcome (%) 80 60 72 74 LdT 78 76 60‐66 60‐79 64 67 70 72 ETV TDF PegIFN 48 38 40 ~ 20 20 < 10 0 ALT Normalization Histologic Improvement ~ 5 NA 3 NA Response Durability Lok AS, et al. Hepatology. 2009;50:661-662. Poblaciones especiales • Co-infección HBV-HCV • No hay evidencias – el tratamiento debe estar dirigido al virus dominante • Co-infección HBV/HDV • Pobres resultados • Dosis altas de IFN estándar (10MUI 3 veces a la semana) + LVD (100 mg/dia) x 48 semanas es mas eficaz que la monoterapia con IFN • PEG IFN ( 25% respuesta) • PegIFN+ ADV • Cirrosis descompensada • IPEG IFN contraindicado • ETV de primera línea, (no debe ser usado en resistencia a LVD) Poblaciones especiales Hemodialisis PegIFN 135 mcg/sc/semanal LVD en pacientes sin respuesta al IFN Inmunosupresión Investigar HbsAg y anti-HBc Si la duración es < 6 meses iniciar LVD 2-4 semanas antes y continuar 6-12 meses despues de terminada • Si la duración > 6 meses ETV o TDV • Anticore positivo solo : observar • IFN esta contraindicado • • • • • • Poblaciones especiales • Pediátricos • VHB crónica asintomática- ALT normal-HVB DNA elevado: inmunotolerancia • El tratamiento esta indicado en niños de 2-18 años con dos HBsAg positivo en dos ocasiones en un intervalo de 6 meses entre ambas. o Hbe(+) : HBV DNA > 105 cp/ml o Hbe(-) : HBV DNA > 104 cp/ml • Biopsia hepática compatible con hepatitis crónica A1F1 • Dos drogas han sido aprobadas : IFN a y LVD Poblaciones especiales • Coinfeccion HIV-HVB • CD4 < 200 células/ml : o o o o puede empeorar la historia natural de la HVB crónica Seroconversion infrecuente Niveles elevados de HBV DNA Severidad histológica • Con HAART : incluir TDV para evitar la emergencia de cepas resistentes a LVD • Sin HAART: usar drogas sin acción anti HIV: ADV o PegIFNa2a • LVD y TDV contraindicado como monoterapia • Indicar tratamiento cuando fibrosis > F2 Poblaciones especiales Resistencia • Reaparición de HVB DNA después de un periodo de indetectabilidad o elevación de > 1 log durante tratamiento después de haber presentado respuesta virológica. • LVD : asociar ADV o TDV • Suspender LVD: Tenofovir + Emtricitabina Resistencia al ADV : cambio a ETV o agregar LVD Resistencia TDV: agregar ETV