Insuficiencia mitral:
aspectos prácticos.
José Alberto de Agustín Loeches
Servicio de Cardiología
Hospital Clínico San Carlos
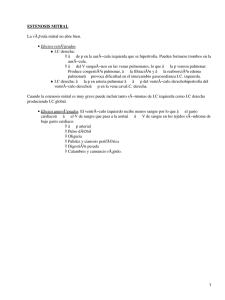
Insuficiencia mitral
Valvas
Anillo mitral
Cuerdas
tendinosas
Músculo
papilar
Insuficiencia Mitral: Etiología
v Degenerativa
v Reumática
v Síndrome
de prolapso mitral
v Cardiopatia
Isquémica
v Miocardiopatia
v Endocarditis
dilatada
bacteriana
Fisiopatologia
v
Disminución de la
resistencia al vaciado
ventricular.
v
Sobrecarga de volumen y
dilatación progresiva del VI
IM
Medtronic.Inc
FISIOPATOLOGIA
INSUFICIENCIA
MITRAL
Sobrecarga
de Volumen
Disfunción VI
Dilatación VI
Remodelado
Ventricular
Supervivencia
Insuficiencia mitral: Hª Natural
IM
Dilatación
progresiva del VI
Disfunción
VI
Síntomas
Años
CLINICA
v Gran
variabilidad dependiendo de:
Ø Severidad.
Ø Progresión.
Ø Presiones
AI, PSAP, PVC.
Ø Taquiarritmias
Ø Cardiopatía
auriculares.
isquémica, miocardiopatía, otra
valvulopatía concurrente
CLINICA
IM AGUDA
IM CRÓNICA
AUMENTO
PRESIONES
RETROGRADAS
SINTOMAS POR
BAJO GASTO
• Edemas agudo de
pulmón
• Hepatomegalia,
edema,ascitis.
• Fatiga
• Debilidad
Insuficiencia Mitral Crónica
Bien tolerada.
Pueden pasar años desde que sea severa hasta que
desarrollen síntomas o se deteriore la función sistólica.
Síntomas
Ling NEJM 1996
Dilatación VI
Circulation 1994; 89:191
FEVI
Circulation 1994;90:833
Exploración Física
• Auscultación cardiaca
– Primer ruido débil (IM evita tensión del aparato
valvular)
– Soplo pansistólico (Borra 2º tono). Irradiado a axila.
– Tercer tono (llenado abrupto VI)
– Soplo de llenado por hiperaflujo.
– Desdoblamiento del 2º tono por cierre precoz de la
válvula aortica.
Auscultación
Soplos sistolicos
• Estenosis aortica
• Insuficiencia mitral
• Prolapso mitral
• Insuficiencia tricuspide
Soplos diastolicos
• Insuficiencia aórtica
• Estenosis mitral
S1
S2
S1
PRUEBAS COMPLEMENTARIAS
ECG:
• Crecimiento AI.
• FA
RX TORAX:
• Cardiomegalia
• Aumento de AI, VI
• Signos de IC
Ecocardiograma
v Detectar
la presencia de IM
v Cuantificar
la su severidad
v Determinar
la etiología
v Valorar
la repercusión sobre AI y VI
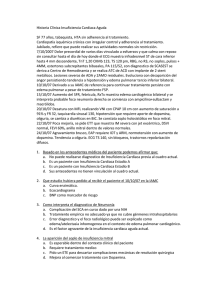
Criterios de IM severa
Ø AREA DE
ORIFICIO REGURGITANTE EFECTIVO
Ø DIAMETRO
DE PISA ( VEL DE ALISING 30+-5 cm/seg)
>40 MM 2
>10 mm
Ø VOLUMEN
REGURGITANTE
>60 cc
Ø FRACCION
REGURGITANTE
50 %
Ø IMAGEN
DE AREA COLOR
Ø VENA CONTRACTA
Ø INVENSION
Ø JET
>40%
> 0.5 CM
DE FLUJO SISTOLICO EN VENAS PULMONARES
DE REGURGITACION MITRAL QUE LLEGA ALTECHO DE LA AI
Ø CHORRO
DE DOPPLER CONTINUA DENSO
Tratamiento
v Tratamiento
Ø
Ø
Ø
Ø
Diuréticos
Vasodilatadores
Digital si FA
Anticoagulanción si FA
v Tratamiento
Ø
Ø
Médico
quirúrgico
Plastia (reconstrucción) mitral
Prótesis
X
¿Por qué reparar?
v
Menor mortalidad operatoria
v
Mejor preservación de FEVI
v
No precisa anticoagulación
v
Menos complicaciones valvulares
v
Menor incidencia de endocarditis
v
Major supervivencia a largo plazo
Circulation 1995; 91: 1022-28
Reparación mitral
Factibilidad de la reparación
FACIL
PROLAPSO POSTERIOR P2
INTERMEDIO
PROLAPSO DE VALVA ANTERIOR
DIFICIL
PROLAPSO DE AMBOS VELOS
PROLAPSO DE LAS COMISURAS
IM REUMATICA
IM ISQUEMICA
¿Cuando operar?
IM
Si
¿Síntomas?
DTSVI >50 mm
FEVI deprimida
Cirugía
No
VI normal
Tratº médico
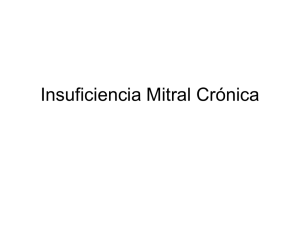
Volume 352:875-883
March 3, 2005
Number 9
Kaplan-Meier Estimates of the Mean ({+/-}SE) Rates of Overall Survival among Patients
with Asymptomatic Mitral Regurgitation under Medical Management, According to the
Effective Regurgitant Orifice (ERO)
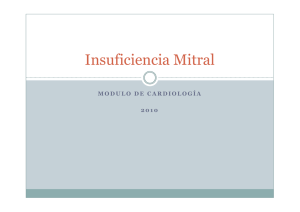
Volume 352:875-883
March 3, 2005
Number 9
Kaplan-Meier Estimates of the Mean ({+/-}SE) Rates of Cardiac Events among
Patients with Asymptomatic Mitral Regurgitation under Medical Management,
According to the Effective Regurgitant Orifice (ERO)
Supervivencia
Insuficiencia mitral: Hª Natural
IM
Dilatación/
Disfunción VI
Cirugía
Síntomas
Años
ACC/AHA guideline: Indications for surgery in severe
chronic organic mitral regurgitation.
Class IIa
1. MV repair is reasonable in experienced surgical centers for asymptomatic patients with chronic
severe MR* with preserved LV function (ejection fraction greater than 0.60 and end-systolic
dimension less than 40 mm) in whom the likelihood of successful repair without residual MR is
greater than 90%. (Level of Evidence: B)
2. MV surgery is reasonable for asymptomatic patients with chronic severe MR,* preserved LV
function, and new onset of atrial fibrillation. (Level of Evidence: C)
3. MV surgery is reasonable for asymptomatic patients with chronic severe MR,* preserved LV
function, and pulmonary hypertension (pulmonary artery systolic pressure greater than 50 mm
Hg at rest or greater than 60 mm Hg with exercise). (Level of Evidence: C)
4. MV surgery is reasonable for patients with chronic severe MR* due to a primary abnormality of the
mitral apparatus and NYHA functional class III–IV symptoms and severe LV dysfunction (ejection
fraction less than 0.30 and/or end-systolic dimension greater than 55 mm) in whom MV repair is
highly likely. (Level of Evidence: C)
Data from Bonow, RO, Carabello, BA, Chatterjee, K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease. A
report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing committee to revise the 1998
guidelines for the management of patients with valvular heart disease). J Am Coll Cardiol 2006; 48:e1.
ESC guideline: Indications for surgery in severe chronic organic
mitral regurgitation.
¿What to do?
Personalized treatment
Factores que afectan la decisión de
operar o no
Síntomas
Severidad de la IM
Dimensiones de VI
FEVI
FA. HTP.
Decision de operar
Probabilidad de
reparación
Edad
Riesgo operatorio del
paciente
¡¡ MUCHAS GRACIAS !!
 0
0