Anuncio

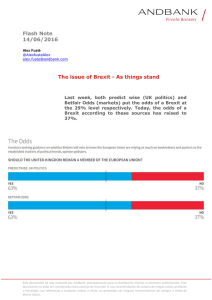
Documento descargado de http://www.elsevier.es el 21/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. Rev Esp Med Nucl Imagen Mol. 2012;31(5):237–242 Original article Lymphoscintigraphy for differential diagnosis of peripheral edema: Diagnostic yield of different scintigraphic patterns夽 J.R. Infante a,∗ , L. García a , P. Laguna b , C. Durán a , J.I. Rayo a , J. Serrano a , M.L. Domínguez a , R. Sánchez a a b Servicio de Medicina Nuclear, Complejo Hospitalario Universitario de Badajoz, Badajoz, Spain Servicio de Cirugía Vascular, Complejo Hospitalario Universitario de Badajoz, Badajoz, Spain a r t i c l e i n f o Article history: Received 17 October 2011 Accepted 21 November 2011 Keywords: Edema Lymphoedema Lymphoscintigraphy Scintigraphy patterns a b s t r a c t Edema of the limbs is a common reason for medical consultation, for which the lymphoscintigraphy is considered to be a reliable method for its differential diagnosis. Objective: To evaluate the usefulness of radionuclide studies in the differential diagnosis of edema, and the diagnostic yield of different scintigraphic patterns. Material and methods: A total of 61 patients, mean age 43 years, referred to our department in the last 3 years for suspected lymphoedema, were considered. One patient was discarded due to lack of diagnosis, 56 had lower limb edema and 4 upper limb edema. After intradermal injection of two doses of 99m Tc-nanocolloid, scintigraphic scans were made at 30 and 120 min. The final diagnosis was based on imaging tests, clinical course, and response to treatment. We calculated the parameters of the diagnostic yield of four different scintigraphic patterns (presence of dermal backflow, asymmetry-alteration in inguinal/axillary nodes, presence of collateral pathways, and visualization of intermediate lymph nodes), considering them individually and jointly. Results: The best diagnostic yield was achieved by considering dermal backflow and asymmetry in inguinal/axillary nodes (accuracy 88.9%, specificity 96.4%, PPV 95.5%). Evaluation of intermediate lymph nodes and presence of collateral pathways contributed little to the diagnostic yield, showing poor sensitivity and high false positive rates. Conclusion: The lymphoscintigraphy had high diagnostic yield, allowing early treatment of lymphoedema. The dermal backflow and asymmetry in inguinal/axillary nodes had the greatest diagnostic accuracy. Evaluation of intermediate lymph nodes and visualization of collateral pathways contributed little to improving the diagnosis. © 2011 Elsevier España, S.L. and SEMNIM. All rights reserved. Linfogammagrafía en el diagnostico diferencial del edema. Rendimiento diagnóstico de diferentes patrones gammagráficos r e s u m e n Palabras clave: Edema linfedema linfogammagrafía patrones gammagráficos El edema de extremidades constituye un motivo frecuente de consulta médica, considerándose la linfogammagrafía un método fiable para su diagnóstico diferencial. Objetivo: valorar la utilidad del estudio isotópico en el diagnóstico diferencial del edema y el rendimiento diagnóstico de diferentes patrones gammagráficos encontrados. Material y Métodos: se consideraron 61 pacientes remitidos a nuestro Servicio en los últimos tres años por sospecha de linfedema, descartándose uno por falta de diagnóstico. La media de edad fue de 43 años. 56 de los pacientes presentaban edema en miembros inferiores y 4 en superiores. Tras inyección intradérmica de dos dosis de 99m Tc-nanocoloide, se realizaron rastreos gammagráficos de extremidades a los 30 y 120 minutos de su administración. El diagnóstico definitivo se basó en pruebas de imagen, evolución clínica y respuesta a tratamiento. Se calculó el rendimiento diagnóstico de cuatro diferentes patrones gammagráficos (presencia de flujo dérmico, asimetría-alteración en ganglios inguinales/axilares, presencia de vías colaterales y visualización de ganglios intermedios) considerándose de manera individual y conjunta. Resultados: el mayor rendimiento diagnóstico se alcanzó considerando el flujo dérmico y la asimetría en ganglios inguinales/axilares (exactitud 88,9%, especificidad 96,4%, VPP 95,5%). La valoración de ganglios intermedios y presencia de vías colaterales aportó escaso rendimiento diagnóstico, con baja sensibilidad y elevada tasa de falsos positivos. Conclusión: la linfogammagrafía presentó un alto rendimiento diagnóstico, permitiendo un tratamiento precoz del linfedema. El flujo dérmico y asimetría en ganglios inguinales/axilares mostraron la mayor exactitud diagnóstica. La valoración de ganglios intermedios y visualización de vías colaterales no aportaron mejoría al diagnóstico. © 2011 Elsevier España, S.L. y SEMNIM. Todos los derechos reservados. 夽 Please cite this article as: Infante JR, et al. Linfogammagrafía en el diagnóstico diferencial del edema. Rendimiento diagnóstico de diferentes patrones gammagráficos. Rev Esp Med Nucl Imagen Mol. 2012;31(5):237–42. ∗ Corresponding author. E-mail address: [email protected] (J.R. Infante). 2253-8089/$ – see front matter © 2011 Elsevier España, S.L. and SEMNIM. All rights reserved. Documento descargado de http://www.elsevier.es el 21/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. 238 J.R. Infante et al. / Rev Esp Med Nucl Imagen Mol. 2012;31(5):237–242 Introduction Edema of the extremities is a frequent reason for medical consultation, including an etiology of lymphatic origin in the differential diagnosis. Lymphedema is defined as tumefaction of a part of the body caused by the accumulation of abnormal fluid in the subcutaneous interstitial spaces secondary to malformation or malfunction of the lymphatic system.1 Lymphedema may be classified as primary or secondary. In the first case its appearance is generally spontaneous or, more rarely, after a trigger caused by congenital absence or abnormal development of the lymphatic system. In turn, primary lymphedema may be hereditary (Milroy’s disease) or non-hereditary and, according to the abnormality found, aplastic, hypoplastic or hyperplastic. The cause of secondary edema may be obstruction or interruption of the lymphatic system due to different diseases (infectious, following oncologic treatment, traumatism).2 Apart this classification there is other based on clinical stages proposed in the Congress of Lymphology held in 2001 in Génova, Italy.3 The prevalence of lymphedema is significant. In developed countries it has been estimated that 10 million persons are affected as a consequence of oncologic treatments in the breast or pelvis, while 90 million are affected worldwide due to parasite infections.4 Despite this prevalence this disease frequently remains undiagnosed and is treated too late or not at all. The diagnosis of lymphedema is based on examination, biochemical data and imaging studies. The examinations include inspection, palpation and determination of an increase in volume in the extremity affected as well as evaluation of the Stemmer and Godet sign.5 The analytical data (including the determination of total proteins, albumin, creatinine and ions in blood or urine) allow differential diagnosis in edema of systemic causes (cardiac or renal insufficiency or hypoalbuminemia). Echo-Doppler, CT and MR are among the imaging studies used, with lymphoscintigraphy currently being the technique of choice in the diagnosis of this disease.6 Nonetheless, review of the literature has shown a lack of consensus in regard to the protocols used in the isotopic studies and in the interpretation of the studies.7,8 Thus, the aim of the present study was to evaluate the utility of lymphoscintigraphy in the differential diagnosis of edema as well as determine the diagnostic performance of the different scintigraphic patterns found. Material and methods We performed a prospective study from January 2008 to January 2011 including 61 patients referred to our department for suspicion of lymphedema. All the patients had previously undergone clinical evaluation, determination of biochemical parameters and imaging studies, with a minimum time of evolution following diagnosis of 6 months. One patient was ruled out because of the impossibility of achieving a definitive diagnosis. Thus, the study group consisted of 60 patients, 16 males and 44 females with a mean age of 43 years (range from 1 to 84). Fifty-six of the patients presented edema in the lower extremities and 4 in the upper limbs. The time of clinical evolution varied greatly, being from 3 months to 15 years. Table 1 shows the demographic characteristics of the patients included, the clinical history and most significant clinical findings as well as the results of the imaging tests performed. The results expressed in the Echo-Doppler column only refer to the presence or not of vascular disease. The protocol of the scintigraphic study consisted in the intradermic injection of two doses of 99m Tc-nanocolloid in the first and second interdigital spaces of the hands and feet with an activity of 37 MBq per injection in a volume of 0.1 mL and posterior massage in the area. Image acquisition was obtained at 30 min and 120 min after the administration of the radiotracer by scan of the extremities at a speed of 8 cm per minute using dual-head gamma cameras (Millennium VG and Elscint Helix commercialized by General Electric, Symbia T2 distributed by Siemens) with low energy collimators and high resolution, a matrix of 256 × 1024 and an energy peak centered on 140 keV (window of 20%) (Fig. 1). Interpretation of the images was independently performed by two nuclear medicine physicians with more than 10 years of experience. Five different scintigraphic patterns were considered: the presence of dermic fluid, asymmetry-alteration in inguinal/axillary lymph nodes, the presence of collateral pathways, visualization of intermediate lymph nodes (in ankle, popliteal fossa or in the elbow) and the absence of migration. There was no discordance between the two professionals in the interpretation of the images. The definitive diagnosis was based on the clinical examination, imaging studies (Echo-Doppler, CT or MR), clinical evolution and the response to the treatment implemented. Considering all these data together one group was constituted of 32 patients with lymphedema and another group included 28 subjects without lymphedema. Based on this diagnosis the diagnostic performance (sensitivity, specificity, positive predictive value, negative predictive value and diagnostic precision) of 4 of the different scintigraphic patterns referred was calculated individually and together (sum of factors, with or without mandatory presence). Six patients showed an absence of tracer migration. Since this scintigraphic pattern obviously excluded the presence of the other 4 patterns these were not considered in the statistical study since they would have constituted false negatives at the time of evaluating the patterns. Results Table 2 shows the definitive diagnoses of the 60 patients in the study population. Table 3 depicts the number of subjects presenting the different scintigraphic patterns evaluated in the two groups in the study. The patterns most frequently found in the population with lymphedema were dermic flow and asymmetry in the axillary/inguinal lymph nodes (21 patients). In the group without lymphedema 4 subjects had intermediate lymph nodes and another 4 showed the presence of collateral pathways. The 6 patients with absence of tracer migration corresponded to patients diagnosed with lymphedema and, as previously commented, were not evaluated. Table 4 shows the different values of diagnostic performance for the 4 scintigraphic patterns considered, both individually and together. In general the results demonstrated a high specificity and PPV for the diagnosis of lymphedema in the scintigraphic study. Fourteen of the 26 values found were above 90% and of these, 11 achieved 100%. As a single pattern, dermic flow and the alteration in inguinal/axillary lymph nodes showed the best results (precision 88.9%). Evaluation of the intermediate lymph nodes and the presence of collateral pathways contributed scarce diagnostic performance, having a low sensitivity and an elevated rate of false positives. The greatest diagnostic performance was found considering the dermic flow and the asymmetry in the inguinal/axillary lymph nodes together (precision 92.6%). The sum of the other two patterns did not improve this performance. Lastly, no significant differences were observed on comparing the scintigraphic images acquired at 30 min and those obtained at 120 min, presenting similar patterns of tracer distribution in both studies and in each patient. Documento descargado de http://www.elsevier.es el 21/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. J.R. Infante et al. / Rev Esp Med Nucl Imagen Mol. 2012;31(5):237–242 239 Table 1 Characteristics of the study group. Genre Age Woman Woman Man Woman Woman Woman Woman Woman Woman Woman Woman Woman Woman Man Woman Woman Man Woman Woman Man Woman Woman Woman Woman Man Man Man Woman Woman Man Woman Woman Man Man Woman Woman Woman Woman Man Man Woman Woman Woman Woman Man Woman Woman Woman Woman Man Woman Woman Woman Man Woman Woman Woman Man Woman Woman 41 50 58 35 32 58 43 50 49 51 29 30 42 46 40 40 63 12 70 73 24 54 70 64 2 48 49 70 28 30 33 10 58 48 33 32 67 9 33 49 68 58 53 40 55 47 48 54 84 62 41 40 23 44 55 68 23 1 26 7 Relevant history Ankle fracture Ankle traumatism Relevant findings Echo-Doppler Cellulitis Normal Pathologic Pathologic Pathologic Normal Normal Normal Pathologic Normal Pathologic Pathologic Pathologic Pathologic Pathologic Normal Normal Pathologic Normal Normal Normal Normal Pathologic Pathologic Normal Normal Normal Normal Normal Normal Normal Normal Normal Normal Pathologic Normal Pathologic Pathologic Normal Pathologic Normal Normal Pathologic Normal Normal Normal Normal Pathologic Normal Normal Normal Normal Normal Pathologic Normal Normal Normal Pathologic Normal Pathologic Normal Venous thrombosis Venous thrombosis Ankle traumatism Breast neoplasm Stemmer sign Venous thrombosis Cellulitis Ankle traumatism Elephantiasis Neurofibromatosis Varices Dermatitis Stemmer sign Claudication Stemmer sign Knee traumatism Prostate neoplasm Foot traumatism Venous thrombosis Venous thrombosis Breast neoplasm Inguinal surgery for adenitis Prostate neoplasm Knee prosthesis surgery Elephantiasis Parestesias Dermatitis Bladder neoplasm Foot traumatism Venous thrombosis Morbid obesity Telangiectasias Venous thrombosis Myopathy Venous thrombosis Uterine neoplasm Venous thrombosis Cellulitis Hypothyroidism Prostate neoplasm Foot amputation Breast neoplasm Breast neoplasm Foot traumatism Discussion Early diagnosis of lymphedema is important to implement early treatment which will allow a reduction in the symptoms and prevent disease progression and the appearance of infections. Scintigraphy was first introduced in 1953 by Sherman and Ter-Pogossian9 and is currently considered the most useful technique for this diagnosis, allowing differential diagnosis with venous edema as well as that of systemic origin and lipomatosis.10 Clearance of excess fluid in the interstitial spaces is the main function of the lymphatic system, constituting an accessory route toward the blood circulation. An increase in lymphatic load above Venous thrombosis Stemmer sign Hypothyroidism Cardiac insufficiency Cardiac insufficiency Morbid obesity Renal insufficiency Morbid obesity Venous thrombosis Venous thrombosis Stemmer sign MR or CT Pathologic Pathologic Pathologic Pathologic Pathologic Pathologic Pathologic Normal Pathologic Pathologic Pathologic Normal its capacity of transportation leads to the accumulation of proteins and cellular metabolites leading to dynamic insufficiency with an elevation of osmotic and hydrostatic pressure. Posteriorly, the presence of mononuclear cells conditions the appearance of an accompanying chronic inflammatory process.5 Delayed diagnosis of lymphedema carries a delay in treatment, diminishing its efficacy and physically and psychologically affecting the patient, thus, the importance of isotopic studies in this disease. Considering the characteristics of our study group, which was mostly made up of women (44 of the 60 patients), with unilateral involvement (46 patients) and of the lower extremities (56 subjects), these data agree with other results reported in the Documento descargado de http://www.elsevier.es el 21/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. 240 J.R. Infante et al. / Rev Esp Med Nucl Imagen Mol. 2012;31(5):237–242 Fig. 1. Scintigraphy of lower extremities; delayed images. (a) Normal study. (b) Absence of tracer migration in the left extremity. (c) Asymmetry in inguinal lymph nodes (thick arrow) and presence of dermic flow (thin arrow). (d) Visualization of intermediate lymph node (arrow). A—anterior image, P—posterior image. literature and allow this group to be considered as representative of the population with the disease studied.11 On the other hand, the number of patients with lymphedema secondary to neoplastic treatment was reduced (9 patients). The use of the sentinel lymph node technique and careful patient selection for radiotherapy treatment may explain this and has also been described in the Table 2 Definitive diagnoses. Pathology Lymphedema (32 patients) Primary Post-therapy (surgery/radiotherapy) Traumatisms Mixed (phlebolymphedema) Infections Unclear causes No lymphedema (28 patients) Local venous-vascular origin Systemic (cardiac/renal insufficiency) Obesity (lipedema) Mixedema No pathology N: number of patients. N 6 9 7 3 3 4 14 3 3 2 6 literature.12,13 Lastly, tumoral degeneration of the lymphedema has been described, albeit rarely, as a lymphoangiosarcoma.14 None of our patients presented this complication during the study. The study protocol carried out (intradermic injection, low tracer volume, massage following injection, request that patient do physical activity, double image acquisition) was that used and recommended by numerous authors.15 The acquisition of early and delayed images was considered of special importance since evaluation of only the first could carry a reduction in diagnostic performance.16 In our study the scintigraphic patterns found in the two studies performed at 30 min and 120 min after the injection of the tracer were similar with no significant differences among all the patients except for one. This Table 3 Presence of the different scintigraphic patterns in the two study groups. Scintigraphic patterns Lymphedema (32 patients) No lymphedema (28 patients) Total Dermic flow Lymph node asymmetry Collateral pathways Intermediate lymph nodes Absence of migration 21 21 9 13 6 1 1 4 4 0 22 22 13 17 6 Documento descargado de http://www.elsevier.es el 21/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. J.R. Infante et al. / Rev Esp Med Nucl Imagen Mol. 2012;31(5):237–242 241 Table 4 Diagnostic performance of the four scintigraphic patterns considered. Dermic flow-A Lymph node asymmetry-B Collateral pathways-C Intermediate lymph nodes-D A and B A and C A and D B and C B and D C and D A, B and C A, B and D A, C and D B, C and D A, B, C and D A or B A or C A or D B or C B or D C or D A or B or C A or B or D A or C or D B or C or D A or B or C or D Sensitivity Specificity PPV NPV 80.8 80.8 33.3 50.0 69.2 30.8 46.2 30.8 46.2 15.4 26.9 42.3 15.4 15.4 15.4 92.3 84.6 84.6 84.6 84.6 69.2 92.3 92.3 88.5 88.5 92.3 96.4 96.4 85.7 85.7 100 100 100 100 100 100 100 100 100 100 100 92.9 82.1 82.1 82.1 82.1 71.4 78.6 78.6 71.4 71.4 64.3 95.5 95.5 69.2 76.5 100 100 100 100 100 100 100 100 100 100 100 92.3 81.5 81.5 81.5 81.5 69.2 80.0 80.0 74.2 74.2 70.6 84.4 84.4 57.1 64.9 77.8 60.9 66.7 60.9 66.7 56.0 59.6 65.1 56.0 56.0 56.0 92.9 85.2 85.2 85.2 85.2 71.4 91.7 91.7 87.0 87.0 90.0 Precision 88,9 88,9 60.0 68.5 85.2 66.7 74.1 66.7 74.1 59.3 64.8 72.2 59.3 59.3 59.3 92.6 83.3 83.3 83.3 83.3 70.4 85.2 85.2 79.6 79.6 77.8 PVV: positive predictive value/NPV: negative predictive value. Values expressed in %. case corresponded to a patient diagnosed with lymphedema of the lower left extremity after traumatism. The only difference observed between the two studies was the appearance of an intermediate popliteal lymph node showing dermic flow and asymmetry in the inguinal lymph nodes at 30 min and 120 min. These findings suggested the possibility of ruling out one of the studies since no modifications were produced in the diagnostic performance. Nonetheless, we believe a greater number of studies should be evaluated before making any conclusions. Scintigraphy is a simple technique with scintigraphic patterns of normality which are easily interpretable (symmetric tracer migration, early visualization of proximal lymph nodes, among others)6 and.17 The patterns of abnormality vary and do not seem to present the same diagnostic value. The publication of studies including a high number of subjects and which consider that neither the scintigraphic pattern nor the use of quantitative studies is able to differentiate between primary and secondary lymphedema is of note.6,16 We therefore did not take this differentiation into account but rather considered all the studies in each patient as a whole. Neither did we apply quantitative methods of evaluation since, although they may be a useful tool, qualitative analysis of the images shows a high sensitivity and specificity.6,17 Analyzed as a whole, our values of sensitivity and specificity in the isotopic study coincide with those in the literature reporting a sensitivity of 73% and 97% and a specificity of 100%.1 Considering each scintigraphic pattern separately, other authors have also described the presence of dermic flow as the most important criterion while the visualization of intermediate lymph nodes is assessed as an unspecific sign8 and.18 The absence of tracer migration was observed in 6 patients. Although they were not considered in the study, it is of note that the pattern evaluated alone presented a specificity and positive predictive value of 100%. One sufficiently established use of scintigraphy in lymphedema is the evaluation of response to treatment.19 In our case, the studies requested for this indication were not taken into account because their evaluation was not one of the objectives of this study. Other diagnostic imaging methods have been used in the study of edema. Lymphography with radiologic contrast is currently limited to establishing the adequate surgical treatment approach due to its complexity and the possible appearance of secondary effects.20 Along this line, it has recently been described that the different scintigraphic patterns would be of use to indicate the most adequate type of microvascular surgery for lymphedema.21 Magnetic resonance provides precise anatomical information of the lymph nodes and of alterations in soft tissues. Recent studies have reported a greater sensitivity and precision with dynamic lymphoangiography by MR with the use of paramagnetic contrast compared to lymphoscintigraphy.22 Nonetheless, future studies will or will not confirm these results. In conclusion, lymphoscintigraphy presented a high diagnostic performance with a minimally invasive technique and scarce discomfort to the patients and allowed early treatment of lymphedema. Apart from the absence of migration in the scintigraphic pattern, the presence of dermic flow and asymmetry of the inguinal/axillary lymph nodes demonstrated the greater diagnostic precision of this technique. Evaluation of the intermediate lymph nodes or the visualization of collateral pathways does not improve the diagnosis. Conflict of interest The authors declare no conflict of interests. References 1. Tiwari A, Cheng KS, Button M, Myint F, Hamilton G. Differential diagnosis, investigation, and current treatment of lower limb lymphedema. Arch Surg. 2003;138:152–61. 2. Szuba A, Rockson SG. Lymphedema: classification, diagnosis, and therapy. Vasc Med. 1998;3:145–56. 3. Bernas MJ, Witte Cl, Witte MH, ISL Executive Committee. The diagnosis and treatment of peripheral lymphedema. Draft revision of the 1995 Consensus document of the International Society of Lymphology executive Committee. XVIII International Congress of Lymphology in Genova, Italy. Lymphology. 2001;34:84–91. Documento descargado de http://www.elsevier.es el 21/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. 242 J.R. Infante et al. / Rev Esp Med Nucl Imagen Mol. 2012;31(5):237–242 4. Campisi C. Global incidence of tropical and non-tropical lymphoedemas. Int Angiol. 1999;18:3–5. 5. Collado G, Laguna VP, Morán AO. Patología linfática: clínica y diagnóstico. In: Vaquero F, Clará A, Laborda E, Samaniego E, editors. Tratado de las enfermedades vasculares, vol. II. Madrid: Viguera; 2006. p. 1075–84. 6. Moshiri M, Katz DS, Boris M, Yung E. Using lymphoscintigraphy to evaluate suspected lymphedema of the extremities. Am J Roentgenol. 2002;178:405–12. 7. Jensen MR, Simonsen L, Karlsmark T, Bülow J. Lymphoedema of the lower extremities—background, pathophysiology and diagnostic considerations. Clin Physiol Funct Imaging. 2010;30:389–98. 8. Yuan Z, Chen L, Luo Q, Zhu J, Lu H, Zhu R. The role of radionuclide lymphoscintigraphy in extremity lymphedema. Ann Nucl Med. 2006;20:341–4. 9. Sherman A, Ter-Pogossian M. Lymph-node concentration of radioactive colloidal gold following interstitial injection. Cancer. 1953;6:1238–40. 10. International Society of Lymphology. The diagnosis and treatment of peripheral lymphedema. 2009 Concensus document of the International Society of Lymphology. Lymphology. 2009;42:51–60. 11. Szuba A, Rockson SG. Lymphedema: classification, diagnosis and therapy. Vasc Med. 1998;3:145–56. 12. Fernandez A, Vidal-Sicart S. El ganglio centinela Concepto y aplicaciones clínicas en neoplasias de mama y melanoma. Rev Esp Med Nucl. 2000;19:371–87. 13. Meek AG. Breast radiotherapy and lymphedema. Cancer. 1998;83:2788–97. 14. Broström LA, Nilsonne U, Kronberg M, Söderberg G. Lymphangiosarcoma in chronic hereditary oedema (Milroy’s disease). Ann Chir Gynaecol. 1989;78:320–3. 15. Szuba A, Shin W, Strauss HW, Rockson S. The third circulation: radionuclide lymphoscintigraphy in the evaluation of lymphedema. J Nucl Med. 2003;44: 43–57. 16. Mandell GA, Alexander MA, Harcke HT. A multiscintigraphic approach to imaging of lymphedema and other causes of the congenitally enlarged extremity. Semin Nucl Med. 1993;23:334–46. 17. Szuba A, Strauss W, Sirsikar SP, Rockson SG. Quantitative radionuclide lymphoscintigraphy predicts outcome of manual lymphatic therapy in breast cancer-related lymphedema of the upper extremity. Nucl Med Commun. 2002;23:1171–5. 18. Scarsbrook AF, Ganeshan A, Bradley KM. Pearls and pitfalls of radionuclide imaging of the lymphatic system Part 2: evaluation of extremity lymphoedema. Br J Radiol. 2007;80:219–26. 19. Williams WH, Witte CL, Witte MH, McNeill GC. Radionuclide lymphangioscintigraphy in the evaluation of peripheral lymphedema. Clin Nucl Med. 2000;25:451–64. 20. Burnand KG, McGuinness CL, Lagattolla NR, Browse NL, El-Aradi A, Nunan T. Value of isotope lymphography in the diagnosis of lymphoedema of the leg. Br J Surg. 2002;89:74–8. 21. Maegawa J, Mikami T, Yamamoto Y, Satake T, Kobayashi S. Types of lymphoscintigraphy and indications for lymphaticovenous anastomosis. Microsurgery. 2010;30:437–42. 22. Liu NF, Lu Q, Liu PA, Wu XF, Wang BS. Comparison of radionuclide lymphoscintigraphy and dynamic magnetic resonance lymphangiography for investigating extremity lymphoedema. Br J Surg. 2010;97:359–65.