- Ninguna Categoria
Striatal Hand & Foot Deformities in Parkinson's Disease
Anuncio
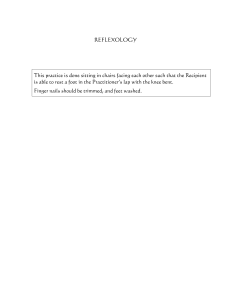
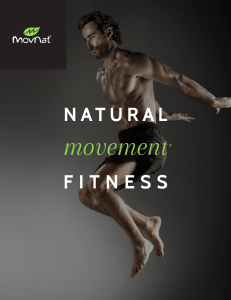
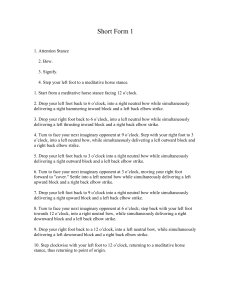
Review Striatal deformities of the hand and foot in Parkinson’s disease Ramsey Ashour, Ron Tintner, Joseph Jankovic Striatal deformities of the hand and foot are abnormal postures that are common in patients with advanced Parkinson’s disease (PD); they can present in the early stages of PD and in other parkinsonian disorders. Over a century ago, Charcot and Purves-Stewart recognised these deformities, which cause substantial functional disability and discomfort. The term striatal is used because pathology in the neostriatum (putamen and caudate) has been suggested to cause the deformities, but the pathogenesis is unknown. Misdiagnosis of the deformities is common— particularly when they occur early and in the absence of cardinal parkinsonian signs, such as tremor, bradykinesia, and rigidity—because the hand deformities are similar to those in rheumatoid arthritis, equinovarus foot deformity typically suggests an orthopaedic problem, and toe extension may be thought to be the Babinski sign of upper-motorneuron syndromes. Here we review the background and clinical features of these deformities to highlight these commonly unrecognised and poorly understood parkinsonian signs. Introduction Various abnormal postures and movements have been associated with pathology in the neostriatum, a combination of putamen and caudate.1 The terms “striatal hand” and “striatal foot” were originally used by Charcot2 and Purves-Stewart3 to report the distal limb deformities typically associated with Parkinson’s disease (PD). Striatal limb deformities might not be easily differentiated from dystonia, a well-recognised movement disorder in patients with PD and other parkinsonian disorders.1 By contrast with fixed striatal hand and foot deformity, dystonia commonly begins during activity and can be associated with dystonic tremor. In patients with PD who are treated with levodopa and have motor fluctuations, dystonia, such as painful fixed inversion of the foot and flexion of the toes, can be part of the wearing-off process.4 If untreated, dystonia can develop into a fixed contracture, although the fixed posture is generally different from that of striatal hand or foot. Fixed deformity is rarely isolated, except for complex regional pain syndrome, particularly after trauma.5 Although striatal deformities have been reported in 10% of patients with untreated, advanced PD,1 prevalence has not been systematically studied. Because the deformities are commonly wrongly diagnosed—eg, rheumatoid arthritis, Dupuytren’s contractures,6,7 flexor tendon entrapment of the digits (also referred to as trigger finger and trigger thumb or de Quervain’s tenosynovitis8), Babinski sign, and other pseudodystonic disorders—we discuss the clinical associations of striatal deformities. The primary aim of this review is to draw attention to these commonly unrecognised signs and to consider possible pathogenetic mechanisms and treatment. Striatal hand In the late 19th century, Charcot described a “digital deformation simulating that of primitive chronic articular rheumatism” in which fingers were “alternately flexed and extended at their several articulations”.2 He http://neurology.thelancet.com Vol 4 July 2005 noted that the deformities in his “paralysis agitans” patients were “neither the articular tumefaction and stiffness, nor the osseous deposits and cracking sounds of nodose rheumatism”. Indeed, unlike rheumatoid arthritis, local signs of joint involvement, such as pain, tenderness, heat, and swelling, are absent in striatal hand. Also, rheumatoid arthritis tends to occur bilaterally, whereas focal dystonia before PD tends to be unilateral, with tremor, rigidity, and bradykinesia developing on the ipsilateral side (table 1).1,9 In the “paralysis agitans” section of his Manual of Diseases of the Nervous System, Gowers10 included illustrations of striatal hand accompanied by a description of the abnormal posture: “. . .[the fingers] are flexed at the metacarpophalangeal joints and extended at the others. . .the digits deviate toward the ulnar side, as in chronic rheumatoid arthritis”. Purves-Stewart also briefly mentioned the “interosseal attitude” of the hands in his patients.3 Many years later, Gortvai11 expanded on the early observations, describing four stages of hand deformity in PD—progression from moderate metacarpophalangeal flexion and interphalangeal extension to severe proximal interphalangeal Lancet Neurol 2005; 4: 423–31 Parkinson’s Disease Center and Movement Disorders Clinic, Department of Neurology, Baylor College of Medicine, Houston, TX, USA (R Ashour BS, R Tintner MD, J Jankovic MD) Correspondence to: Prof Joseph Jankovic, Director of Parkinson’s Disease Center and Movement Disorders Clinic, Department of Neurology, Baylor College of Medicine, Suite 1801, 6550 Fannin, Houston, TX 77030, USA [email protected] Features Rheumatoid arthritis Striatal abnormalities Pathophysiological features Joints Radiographic changes Proliferative synovitis, autoimmunity, microbial initiator Swollen, warm, painful, pannus formation Joint effusions, juxta-articular osteopenia with erosions, narrowed joint space with loss of cartilage Morning stiffness, decreased range of motion (active and passive) Generally symmetrical joint involvement, polyarticular Association with HLA DR4 or DR1 Non-inflammatory, dystonic features, soft-tissue elastic changes Painful, contractures Normal Mobility Distribution Genetics Extra-articular features Cutaneous and visceral rheumatoid nodules, increased serum rheumatoid factor, synovial cysts, vasculitis, episcleritis Fixed deformity, may respond to levodopa or botulinum toxin In most cases develops on one side with ipsilateral emergence of cardinal PD signs Seems to be more common in juvenile-onset PD Rigidity, bradykinesia, tremor Table 1: Striatal deformity and rheumatoid arthritis9 423 Review hyperextension with distal phalangeal subluxation, leading to distal interphalangeal flexion. Clinical and radiological findings prompted Gortvai to comment that the hand joints of his patients with PD were healthy, even after many years of deformed posture.11 He showed the role of small muscle contraction in the production of the deformities, observing that ulnar-nerve block with a local anaesthetic stopped the deformity in patients whereas ulnar-nerve stimulation produced the abnormal posture in healthy people. Since Gortvai’s research, several reports have described many “typical” hand deformities associated with parkinsonism with different patterns of flexion or extension at the various digital articulations.12–18 The most typical deformity associated with striatal hand is characterised by flexion of the metacarpophalangeal joints, extension of the proximal interphalangeal joints, flexion of the distal interphalangeal joints, and ulnar deviation (figure 1).19 Some features of striatal hand in patients with untreated PD are common to other well-described forms of dystonia. Striatal hand must be differentiated from: dystonia in primary dystonic states; dystonia contributing to a differential phenotypic expression of the same disease, as in dystonia-parkinsonism syndromes; dystonia as a complication of pharmacotherapy;4,20–22 and dystonia associated with an ablative lesion or high-frequency, deep-brain stimulation.23–25 In addition, striatal hand must be differentiated from entrapment neuropathies and cervical myelopathies.26 Although striatal hand (metacarpophalangeal flexion, interphalangeal extension, ulnar deviation) is similar to the swan-neck deformities that occur in some arthritic disorders, other postures have been described that more closely parallel the opposite boutonnière deformity (metacarpophalangeal extension, proximal interphalangeal flexion, distal interphalangeal extension). Postures with features intermediate between these two prototypical positions also occur and are common in advanced disease.12,13,15,17 A claw-hand deformity has also been described in PD.13 Whereas metacarpophalangeal flexion and interphalangeal extension, due to contraction of the lumbricals and interossei respectively, seem to be the earliest signs of striatal hand, hyperextension and subluxation of the terminal phalanges are thought to be signs of more advanced deformity.11 In addition to disfigurement, striatal hand can cause pain or discomfort and can affect daily activities such as writing, eating, and buttoning. Severe Figure 1: Striatal hand in a patient with typical PD 424 flexion of the fingers can lead to pressing of fingernails into the palm of the hand, causing abrasion and secondary infection (figure 2). Such contractures are typical in advanced PD and other parkinsonian disorders, but they can occur even in early stages and also secondary to reactive fibrosis resulting from treatment with an ergot dopamine agonist (eg, bromocriptine, pergolide),14 which can also cause fibrosis in the lungs, heart, and other tissues.27 Although hand deformities are accepted as a common complication in patients with advanced, treated PD, less attention has been given to the frequency of striatal hand as an early sign in patients who have not been treated.18 We have seen a mild flexion of the metacarpophalangeal joint in the hands of many patients with early PD, even before other parkinsonian features present. This flexion is typically on the side initially affected by tremor, rigidity, or bradykinesia. Although prospective studies must validate this observation, clinicians should search for this sign as evidence of the side of the initial presentation. Striatal foot In a lecture on the symptoms of “paralysis agitans” in 1877, Charcot gave an account of two patients whose feet were “stiff, extended, and turned in, simulating the malformation known as talipes equines (varus) clubfoot”.2 Claw-like “extension of the first and concomitant flexion of the second phalanges” were seen in both patients. Gowers10 also noted in his discussion of “paralysis agitans” that “[rigidity] may extend to the feet, and even cause talipes equinovarus, and distortion of the toes—extension of the first, and flexion of the other phalanges so as to cause a claw-like deformity”. Similar posturing (hallucal hyperextension, flexion of the other toes, ankle inversion) was described 10 years later in five of 28 patients with “paralysis agitans” who were observed for 2 years.3 This “toe curling” symptom with pain and cramps was unpredictably associated with walking and preceded all other symptoms by up to 2 years in three of the five patients. Several studies done before the era of levodopa treatment attributed foot and other deformities to PD.11,12 In 1972, Duvoisin and colleagues28 noted that “this dystonic phenomenon is an intrinsic feature of PD”. By use of the term “striatal foot”, they described the typical features, including big-toe extension, flexion of the other toes, equinovarus foot positioning, and pain.28 Striatal foot deformity can cause pain and impair the ability to stand, walk, and wear shoes. If untreated, skin ulceration and bone erosion can happen (figure 3). Equinovarus foot positioning produces inadequate support, hinders early and mid-stance dorsiflexion, and prevents the tibia from moving over the stationary foot.29,30 Thus, the stance phase of gait is shortened, and push-off propulsion and forward propulsion are http://neurology.thelancet.com Vol 4 July 2005 Review Figure 2: Typical striatal hand deformity and severe flexion contracture Left and middle: typical striatal hand deformity in the right hand. Right: marked flexion of fingers resulting in severe flexion-contracture in the left hand. hindered.31 Early swing-phase limb advancement and foot clearance are also affected. Pressure is increased over the lateral aspect of the foot and ankle instability occurs.29,31 Over the years, different terms have been used to describe the striatal foot deformity, including the dystonic foot response of parkinsonism,32 dystonic claudication,33 striatal toe,34,35 hitchhiker’s great toe,29 pseudo-rheumatoid deformity,36 and pseudo-Babinski.35 The all-encompassing term foot dystonia is commonly used to describe dystonic posturing of the legs and feet that happens in various clinical settings including PD and other Parkinson-plus syndromes.19,33,37–43 Furthermore, striatal toe and equinovarus foot are used to describe clinical patterns of motor dysfunction, such as upper-motor-neuron syndrome, that are visually similar or identical to but aetiologically distinct from striatal foot in PD.29 As with striatal hand, striatal foot must be differentiated from other well-described forms of dystonia commonly attributed to dopaminergic therapy, such as off-period and biphasic dystonia.4 Striatal foot in PD is part of the primary disease process and can be one of the earliest signs in untreated patients.1,3,19,28,32,33,36–45 When striatal foot is a secondary (symptomatic) dystonia in patients with PD, it might be mistaken for a primary dystonic state (sporadic or familial), particularly when the classic parkinsonian signs are absent. Primary adult-onset dystonia rarely involves the feet, and thus the possibility of PD should be considered in all adults who present with isolated foot dystonia.1 Striatal toe is a type of striatal foot, but without the equinovarus foot. Electromyographic analyses have shown a different pattern of muscle contraction in striatal foot from that in the Babinski response;28 http://neurology.thelancet.com Vol 4 July 2005 however, the exact differences need further study. Striatal toe has been differentiated from the Babinski sign according to toe fanning and flexion synergy of other muscles in the same leg, which are both features of the Babinski response.35 Other disorders with limb abnormalities similar to striatal foot include peripheral vascular disease, lumbar canal stenosis, familial paroxysmal exercise-induced dystonia, and exerciseinduced hypocalcaemic-tetanic spasms.43 Classification and diagnosis Although the term striatal is used to describe these deformities, it is inaccurate because it implies a nonspecific lesion in the striatum (eg, neostriatum, paleostriatum, and corpus striatum) even though there Figure 3: Striatal foot with severe skin ulceration and bone erosion 425 Review is little evidence that a striatal lesion is needed to produce the posture. Furthermore, traumatic, vascular, or other lesions in the striatum rarely produce striatal deformities.46 Moreover, the term does not adequately account for the range of extrastriatal lesions that could lead to these postural deformities. We suggest use of the terms striatal hand and striatal foot to help with recognition of the clinical entity of distal limb deformity in parkinsonism. Although in this review we focus on striatal hand and striatal foot associated with PD, there are many other parkinsonian disorders in which striatal hand occurs, including multiple system atrophy,40,47,48 corticobasal degeneration,49 progressive supranuclear palsy,50–52 NBIA (neurodegeneration of the brain with iron accumulation),53 and parkinsonism-dementia seen in western Pacific regions.54 The relation between parkinsonism and coexistent abnormal postures, such as striatal hand, striatal foot, bent spine, scoliosis, and camptocormia, is not well understood. Camptocormia—a disorder characterised by pronounced flexion of the thoracolumbar spine, which is most prominent on standing and walking and relieved in the supine position—is associated with various musculoskeletal and neurological causes, including parkinsonism, dystonia, and other neurological and non-neurological disorders.55 In patients with idiopathic PD, camptocormia is increasingly identified and should not be confused with bent spine syndrome seen in axial myopathies.1,55–59 Camptocormia associated with active contraction of the rectus abdominus can be treated with injection of botulinum toxin into that muscle.60 Scoliosis is a lateral curvature of the spine accompanied by vertebral rotation that results in asymmetrical deformity of the trunk. Scoliosis is more common in patients with PD61–63 than in elderly people of similar age to those with PD.63–65 Epidemiology Striatal hand and foot deformities might present in up to 10% of untreated patients with advanced PD;1 however, neither the true prevalence nor the relation of these deformities with age and sex has been systematically studied. Although many reports support the high prevalence of dystonia in patients with idiopathic, untreated PD,1,19,20,37,66 few have questioned the relation, some even noting a similar prevalence of focal dystonia in untreated PD and the general population.38 Patients who develop dystonia before or with PD tend to be younger than the general population of patients with PD.1 Similarly, patients with early-onset PD, particularly those with PARKIN mutations, are more likely to have dystonia.67 Foot dystonia develops in 20–40% of patients with PD receiving sustained levodopa treatment,42 and some studies have found that striatal foot precedes treatment in 2·4–8·0% of patients.32,68 In a series of 426 86 parkinsonian patients, which was done before levodopa treatment was available, 34 (~40%) had some deformity of the hands, including 14 (~24%) of 58 patients with PD.12 By contrast with this finding, only three cases of hand deformity in patients with PD were recorded during 12 months in a “busy” neurology department; however, a formal epidemiological study was not done.15 Pathophysiology Early reports attributed the characteristic postural deformities in PD to muscular rigidity.2,3 Later studies on striatal foot suggested an extrapyramidal origin, differentiating the deformity from similar but unrelated frontal release, such as the “grasp”, and proprioceptively mediated flexion synergy in mesial frontal-lobe lesions.32,69 Various lesions disrupting striatopallidothalamic projections produce focal dystonia in human beings;20,46,70–72 research with animal models has given insights as well. For example, foot dystonia similar to that seen in early PD has been reported in studies of parkinsonism in monkeys induced by 1-methyl-4phenyl-1,2,3,6-tetrahydropyridine (MPTP).73 Also, the abnormal posture and compulsive circling behaviour in dogs74 and cats75,76 after unilateral ablation of the caudate nucleus77 suggest that asymmetrical degenerative changes in the caudate—through disruption of its tonic effect on posture and locomotion—contribute to the development of scoliosis in patients with PD and in patients with postencephalitic parkinsonism. Furthermore, rats with hemiparkinsonism, induced by unilateral injection of 6-hydroxydopamine into the left ventralis tegmenti, showed strong ipsilateral deviation;78 the severity of scoliosis was closely related to the decrease in extracellular striatal dopamine and to the development of postsynaptic dopamine receptor supersensitivity. A similar mouse model showed the development of dyskinesias and abnormal posture after 6-OHDA injection into the sensorimotor striatum.79 Of the basal ganglia, the lentiform nucleus (putamen and globus pallidus) is commonly involved when dystonia and parkinsonism coexist.1 Lenticular lesions are also associated with the development of camptocormia.55,59 Thalamic relay nuclei have been associated with contralateral symptomatic hemidystonia,20,69 and lesions in the posterior and posteriolateral thalamus, red nucleus, and subthalamic nucleus have been reported to cause various dystonias.1,23–25,46,50–52,70–72 Dystonia in PD includes a range of focal dystonias— eg, cervical dystonia, limb dystonia, blepharospasm and other cranial dystonias, and hemidystonia.1,19–21,37,38,80,81 Although striatal hand and foot overlap with other forms of dystonia, comparison of the clinical features of these deformities with those in primary (idiopathic) dystonia shows substantial differences (table 2).19,38,80 http://neurology.thelancet.com Vol 4 July 2005 Review Why some patients with PD develop striatal deformity and others do not is not clear, and there is no predictor of striatal deformity in patients with PD. In one study,12 the frequency of striatal hand was associated with the amount of generalised rigidity but not with the amount or duration of tremor. Severe rigidity has also been suggested to contribute.15 Study of limb contractures in patients with PD by use of transcranial magnetic stimulation found that central motor conduction time is lower in the limb that is more severely affected; shorter central motor conduction time reflects decreased excitability in cortical-inhibitory circuits and has been suggested to contribute to overactive and inappropriate muscle contraction in the hand.17 Qualitative research findings that striatal hand is more common in women than in men could be explained by more ligament laxity in women than in men—ie, by an interaction between a central tone disturbance and a peripheral, predisposing state.16 Epidemiological studies82–84 reporting much higher rates of anterior cruciate ligament injury in females than males participating in the same sports have prompted investigation of non-contact mechanisms and risk factors to explain the difference.85–87 The effects of female hormones on connective-tissue structure have been studied,82,83,88,89 and some have shown that collagen structure and tensile properties vary with hormonal fluctuations in women.90,91 Similarly, studies have identified transcripts for oestrogen and progesterone receptors in normal connective tissue in women.90,92 In rats, oestrogen increases elastin in connective tissue93–95 and decreases collagen in tendons and fascias.88 The cyclically released hormone relaxin changes collagen metabolism through an effect on the secretion of procollagenases by tissue fibroblasts.96,97 Although these findings provide clues to the sex-specific factors that predispose or perhaps contribute to joint and soft-tissue pathology, particularly for sports-related trauma, their role in the development of striatal-limb deformities in PD is speculative. Observations that these deformities are associated with sex must be substantiated by formal epidemiological studies; the deformities could be caused by many factors with anatomical, sociological, and hormonal differences modifying the course of disease in individual patients. A pathophysiological model for parkinsonism and dystonia, such as observed in levodopa-related, offperiod dystonic processes, has been proposed to involve dopaminergic hypofunction with concurrent or compensatory cholinergic hyperfunction.42 Improvement in patients treated with baclofen has led some to posit a contributory role for other neurotransmitter systems (specifically glutamate and GABA) in dystonia as well.32 Furthermore, a hypothesised rostrocaudal gradient of decreased dopaminergic and increased GABA-ergic function across a somatotopically organised striatum42 might underlie the dystonic complications in the feet of patients with PD. http://neurology.thelancet.com Vol 4 July 2005 Distinguishing features* Striatal deformities Primary idiopathic dystonia Fixed or mobile Pain Relatively fixed Typically painless When present Typically present at rest Concomitant parkinsonism signs and symptoms (tremor, rigidity, bradykinesia) Typically affects the hands, but can also affect the feet and other parts of the body Typically persists during sleep Mobile, but can evolve into contractures if left untreated Typically painless, but some dystonias (eg, cervical) are associated with local pain Commonly induced by action Other symptoms Anatomy Sleep association Commonly other dystonic features are present Dystonia affecting legs and feet is very rare at onset in adults; if present, dystonia is commonly associated with parkinsonism Not present during sleep, except when associated with contractures *These features are not absolute and are given as a guide. Table 2: Striatal deformities and primary idiopathic dystonia19,38,80 Progression of striatal-limb deformities from abnormal contraction to fixed contracture results in further functional disability in patients already coping with PD symptoms. Particularly distressing is the rapid, unpredictable development of contractures in levodoparesponsive patients. In previous studies on hand contractures in PD, the progression of deformity to fixed contracture happened over periods of 2 weeks,14 2 months,15 2 weeks to 2 months,17 and 6 months.98 In most of the patients with PD in these studies, contractures developed after several years of disease with a strong (but not fully understood) female preponderance. The combination of long-lasting, fixed posture, and sustained muscle contraction associated with hypertonia reduces the number of sarcomeres in the affected muscle groups.99 Furthermore, torque measurements during imposed constant-velocity muscle-contraction cycles have been used to show secondary changes in the mechanical properties of affected muscles and their surrounding tissues in patients with long-standing spasticity.100 In particular, alterations in soft-tissue plasticity and viscoelasticity are thought to cause atrophy and fibrosis in both muscle and connective tissue98–100 and could thus compound the effect of sarcomere-loss and muscle shortening in the overall progression of deformity to fixed contracture. Although contracture development has been well characterised in patients with long-standing spasticity, similar changes seem possible in patients with PD—electromyographic analyses show excessive, involuntary motor-unit recruitment in rigid muscles apparently at rest that is not suppressible, and the average area of surface electromyographic readings relates to clinical assessment of rigidity.101 The rapid development of limb contractures in patients with PD taking the ergot dopamine agonist bromocriptine mesilate14 suggests drug-induced reactive fibrosis as a pathogenetic mechanism of contracture. Indeed, in most 427 Review Search strategy and selection criteria References for this review were identified from searches of MEDLINE up to March 1, 2005. The keywords “Parkinson’s disease”, “parkinsonism”, “dystonia”, “primary”, “secondary”, “focal”, “hand deformity”, “foot deformity”, “musculoskeletal deformity”, “striatum”, “contractures”, “dyskinesias”, and “levodopa” were entered in various combinations with the inclusion of all subheadings. The references of each paper were studied for pertinent papers for follow-up, and many additional searches were done up to April 15, 2005. No limits were placed on the dates of publication. Only articles published in English were consulted in the initial review. Other references followed up were reviewed in English only; papers written in other languages in this category were allowed only if an English translation was available. reports of patients with PD who rapidly developed contractures, the patients were being treated with ergot dopamine agonists14,17 or ergolines.98 Furthermore, digital vasospasm,102,103 pleuropulmonary fibrosis,27,104–107 and retroperitoneal fibrosis107–110 have all been reported in patients treated with bromocriptine mesilate as well as other ergot compounds. An interaction between ergot compounds and serotonin receptors could explain the production of tissue fibrosis,14,111–114 and both bromocriptine mesilate and methylsergide are known to interact with 5-HT1 and 5-HT2 receptors.114,115 Serotoninsecreting carcinoid tumours have been linked to endocardial and pulmonary fibrosis.114,116,117 Other fibroblast-modulating substances have been researched, including tachykinins (eg, substance P and substance K)118 and growth factors, including platelet-derived growth factor,119,120 insulin-like growth factors,121 and the transforming growth factor family.117,122 Treatment Dystonia responds variably to treatment with systemic drugs in parkinsonism. The response to antiparkinsonian drugs is less predictable in striatal hand and foot than in primary dystonia, although levodopa and anticholinergic agents have improved dystonia in some cases.32,33,35,36,42–44 We have observed cases in which a complete resolution of striatal-hand dystonia was achieved with levodopa treatment. Anticholinergics, baclofen, and benzodiazepines have also been variously successful in treating foot dystonia in parkinsonism, including striatal foot in PD.123,124 Botulinum-toxin injection is a treatment option. In combination with systemic drugs, botulinum toxin is the preferred treatment for focal dystonias and has been used in the treatment of striatal toes.34,60 The dose injected is guided by electromyographic activity in the affected muscles. Botulinum-toxin injection into the lumbricals and short adductors of the thumb has led to functional improvement and pain relief in patients with PD who 428 have striatal hand with varying amounts of contracture.98 However, the large muscle groups contributing to dystonia in the foot as well as the associated contracture can make botulinum-toxin injections less effective in striatal deformities than in more mobile forms of dystonia.123 Also, chemodenervation of extensor hallucis longus for striatal toe might unmask co-contraction of flexor hallucis longus29 and therefore necessitate further treatment. If conventional, non-operative treatments are unsuccessful, orthopaedic surgical interventions can be attempted. Split anterior tibial-tendon transfer with extrinsic toe-flexor release and percutaneous achillestendon lengthening has been reported to result in substantial functional improvement and plantigrade foot in patients with idiopathic foot dystonia.123 Z-lengthening procedures and capsulotomy have also been used in the treatment of hand deformities in PD.13 Neurosurgical treatments that have been assessed for the treatment of PD and dystonia include stereotactic pallidotomy, thalamotomy, and deep-brain stimulation.1,11,25,125–128 Cooper125–127 described improvement and even complete resolution of striatal hand and foot deformities after occlusion of the anterior choroidal artery and stereotactic thalamotomy in patients with PD. Patients with PD who had combined thalamic lesion in the ventralis intermedius and ventralis oralis nuclei (selective Vim-Vo thalamotomy) for the treatment of dyskinesias showed improvement in limb dystonia.128 Nevertheless, the role of neurosurgery in the treatment of striatal hand and foot requires further study; surgery is generally reserved for patients with other severe symptoms refractory to non-surgical treatments. Conclusion Investigation of the temporal relation between the early development of striatal hand and foot deformities, initially shown with slight flexion of the metacarpophalangeal joint, and the natural history of PD might give insight into the pathogenesis of this sign and its relation to underlying pathology. Future studies should assess whether there are predictors for the development of deformity and whether the deformities are associated with disease severity and progression, symptom laterality, age, sex, and other clinical markers. Acknowledgments We thank the staff at the Mary Moody Medical Library in Galveston, TX, USA, for providing copies of papers published before 1975 for this review. We also thank the National Parkinson Foundation for their support. Authors’ contributions All authors contributed equally to this review. Conflicts of interest We have no conflicts of interest. Role of the funding source No funding source had a role in the preparation of this paper or in the decision to submit it for publication. http://neurology.thelancet.com Vol 4 July 2005 Review References 1 Jankovic J, Tintner R. Dystonia and parkinsonism. Parkinsonism Relat Disord 2001; 8: 109–21. 2 Charcot JM. Lectures on the diseases of the nervous system, lecture V. London: New Sydenham Society, 1877: 140–47. 3 Purves-Stewart J. Paralysis agitans, with an account of a new symptom. Lancet 1898; 2: 1258–60. 4 Jankovic J. Levodopa-related motor fluctuations and dyskinesias: clinical manifestation and classification. Mov Disord 2005; 20 (suppl 11): S11–16. 5 Schrag A, Trimble M, Quinn N, Bhatia K. The syndrome of fixed dystonia: an evaluation of 103 patients. Brain 2004; 127: 2360–72. 6 Gudmundsson K, Arngrímsson R, Sigfússon N, Björnsson A, Jónsson T. Epidemiology of Dupuytren’s disease: clinical, serological, and social assessment—the Reykjavik study. J Clin Epidemiol 2000; 53: 291–96. 7 Saar J, Grothaus P. Dupuytren’s disease: an overview. Plast Reconstr Surg 2000; 106: 125–36. 8 Moore, JS. Flexor tendon entrapment of the digits (trigger finger and trigger thumb). J Occup Environ Med 2000; 42: 526–45. 9 Rosenberg A. Bones, joints, and soft tissue tumors. In: Cotran R, Kumar V, Collins T, eds. Robbins pathologic basis of disease, 6th edn. Philadelphia: WB Saunders Company, 1999: 1248–51. 10 Gowers WR. A manual of diseases of the nervous system. Philadelphia: P Blakiston, Son & Co, 1888: 1003–04. 11 Gortvai P. Deformities of the hands and feet in Parkinsonism and their reversibility by operation. J Neurol Neurosurg Psychiatry 1963; 26: 33–36. 12 Reynolds F, Petropoulous G. Hand deformities in parkinsonism. J Chronic Dis 1965; 18: 593–95. 13 Heinzelmann P, Dow R. Clawhand deformity presumed secondary to Parkinson’s disease. J Hand Surg [Am] 1985; 10: 19–21. 14 Quinn NP, Ring H, Honavar M, Marsden CD. Contractures of the extremities in parkinsonian subjects: a report of three cases with a possible association with bromocriptine treatment. Clin Neuropharmacol 1988; 11: 268–77. 15 Kyriakides T, Langton HR. Hand contractures in Parkinson’s disease. J Neurol Neurosurg Psychiatry 1988; 51: 1221–23. 16 Di Petta G, Del Puente A, Scarpa R, Maglione S, Esposito A, Campanella G. Hand deformities in extrapyramidal disorders. Acta Neurol (Napoli) 1994; 16: 142–46. 17 Hu MTM, Bland J, Clough C, Ellis C, Chaudhuri KR. Limb contractures in levodopa-responsive parkinsonism: a clinical and investigational study of seven new cases. J Neurol 1999; 246: 671–76. 18 Ozcakar L, Bal S, Akinci A. Upper extremity contractures heralding Parkinson’s disease. Joint Bone Spine 2003; 70: 86. 19 Fahn S, Jankovic J. Practical management of dystonia. Neurol Clin 1984; 2: 555–67. 20 Hartmann A, Pogarell O, Oertel WH. Secondary dystonias. J Neurol 1998; 245: 511–18. 21 De Yebenes JG, Pernaute RS, Tabernero C. Symptomatic dystonias. In: Watts RL, Koller WC, eds. Movement disorders, neurologic principles and practice. New York: McGraw-Hill, 1997: 455–75. 22 Metman LV. Recognition and treatment of response fluctuations in Parkinson’s disease: review article. Amino Acids 2002; 23: 141–45. 23 Limousin P, Pollak P, Hoffmann D, Benazzouz A, Perret JE, Benabid AL. Abnormal involuntary movements induced by subthalamic nucleus stimulation in parkinsonian patients. Mov Disord 1996; 11: 231–35. 24 Krack P, Pollak P, Limousin P, Benazzouz A, Deuschl G, Benabid AL. From off-period dystonia to peak-dose chorea: the clinical spectrum of varying subthalamic nucleus activity. Brain 1999; 122: 1133–46. 25 Lang AE. Surgery for Parkinson disease: a critical evaluation of the state of the art. Arch Neurol 2000; 57: 1118–25. 26 Uncini A, Di Muzio A, Thomas A, Lugaresi A, Gambi D. Hand dystonia secondary to cervical demyelinating lesion. Acta Neurol Scand 1994; 90: 51–55. 27 Tintner R, Manian P, Gauthier P, Jankovic J. Pleuropulmonary fibrosis after chronic treatment with dopamine agonists for Parkinson’s disease. Arch Neurol (in press). http://neurology.thelancet.com Vol 4 July 2005 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 Duvoisin RC, Yahr MD, Lieberman J, Antunes J, Rhee S. The striatal foot. Trans Am Neurol Assoc 1972; 97: 267. Mayer N, Esquenazi A, Childers M. Common patterns of clinical motor dysfunction. Muscle Nerve 1997; 20 (suppl 6): S21–35. Fuller DA, Keenan MA, Esquenazi A, Whyte J, Mayer N, Fidler-Sheppard R. The impact of instrumented gait analysis on surgical planning: treatment of spastic equinovarus deformity of the foot and ankle. Foot Ankle Int 2002; 22: 738–43. Esquenazi A. Evaluation and management of spastic gait in patients with traumatic brain injury. J Head Trauma Rehabil 2004; 19: 109–18. Nausieda P, Weiner W, Klawans H. Dystonic foot response of parkinsonism. Arch Neurol 1980; 37: 132–36. Poewe WH, Lees AJ, Stern GM. Dystonia in Parkinson’s disease: clinical and pharmacological features. Ann Neurol 1988; 23: 73–78. Giladi N, Meer J, Honigman S. The use of botulinum toxin to treat “striatal” toes. J Neurol Neurosurg Psychiatry 1994; 57: 659. Winkler AS, Reuter I, Harwood G, Chaudhuri KR. The frequency and significance of ‘striatal toe’ in parkinsonism. Parkinsonism Relat Disord 2002; 9: 97–101. Bissonnette B. Pseudorheumatoid deformity of the feet associated with parkinsonism. J Rheumatol 1986; 13: 825–26. LeWitt P, Burns R, Newman R. Dystonia in untreated parkinsonism. Clin Neuropharmacol 1986; 9: 293–97. Quinn N. Parkinsonism and dystonia, pseudoparkinsonism and pseudodystonia. Adv Neurol 1993; 60: 540–43. Nygaard T, Marsden C, Duvoisin R. Dopa-responsive dystonia. Adv Neurol 1988; 50: 377–84. Rivest J, Quinn N, Marsden C. Dystonia in Parkinson’s disease, multiple system atrophy, and progressive supranuclear palsy. Neurology 1990; 40: 1571–78. Lees AJ, Hardie RJ, Stern GM. Kinesigenic foot dystonia as a presenting feature of Parkinson’s disease. J Neurol Neurosurg Psychiatry 1984; 47: 885. Poewe WH, Lees AJ. The pharmacology of foot dystonia in parkinsonism. Clin Neuropharmacol 1987; 10: 47–56. Katzenschlager R, Costa D, Gacinovic S, Lees AJ. [123I]-FP-CITSPECT in the early diagnosis of PD presenting as exerciseinduced dystonia. Neurology 2002; 59: 1974–76. Bozi M, Bhatia K. Paroxysmal exercise-induced dystonia as a presenting feature of young-onset Parkinson’s disease. Mov Disord 2003; 18: 1545–47. Jankovic J. Pathophysiology and clinical assessment of parkinsonian symptoms and signs. In: Pahwa R, Lyons K, Koller WC, eds. Handbook of Parkinson’s disease. New York: Marcel Dekker Inc, 2003: 71–91. Bhatia KP, Marsden CD. The behavioural and motor consequences of focal lesions of the basal ganglia in man. Brain 1994; 117: 859–76. Wenning GK, Tison F, Ben Shlomo Y, Daniel SE, Quinn NP. Multiple system atrophy: a review of 203 pathologically proven cases. Mov Disord 1997; 12: 133–47. Quinn N. Multiple system atrophy: the nature of the beast. J Neurol Neurosurg Psychiatry 1989; 52 (suppl): 78–89. Vanek Z, Jankovic J. Dystonia in corticobasal degeneration. Mov Disord 2001; 16: 252–57. Rafal RD, Friedman JH. Limb dystonia in progressive supranuclear palsy. Neurology 1987; 37: 1546–49. Jankovic J, Friedman DI, Pirozzolo FJ, McCrary JA. Progressive supranuclear palsy: motor, neurobehavioural and neuroophthalmological findings. Adv Neurol 1990; 53: 293–304. Barclay C, Lang A. Dystonia in progressive supranuclear palsy. J Neurol Neurosurg Psychiatry 1997; 62: 352–56. Jankovic J, Kirkpatrick J, Blomquist K, Langlais P, Bird E. Lateonset Hallervorden-Spatz disease presenting as familial parkinsonism. Neurology 1985; 35: 227–34. Chen K, Chase T. Parkinsonism-dementia. In: Vinken PJ, Bruyn GW, Klawans HL, eds. Handbook of clinical neurology, extrapyramidal disorders. Amsterdam: Elsevier Science, 1986: 167–83. Azher S, Jankovic J. Camptocormia: Pathogenesis, classification and response to therapy. Neurology 2004; 62 (suppl 5): A51. 429 Review 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 82 83 430 Oerlemans W, de Visser M. Dropped head syndrome and bent spine syndrome: two separate clinical entities or different manifestations of axial myopathy. J Neurol Neurosurg Psychiatry 1998; 65: 258–59. Djaldetti R, Mosberg-Galili R, Sroka H, Merims D, Melamed E. Camptocormia (bent spine) in patients with Parkinson’s disease— characterisation and possible pathogenesis of an unusual phenomenon. Mov Disord 1999; 14: 443–47. Holler I, Dirnberger G, Pirker W, Auff E, Gerschlager W. Camptocormia in idiopathic Parkinson’s disease: [123I]-CIT SPECT and clinical characteristics. Eur Neurol 2003; 50: 118–20. Nieves A, Miyasaki J, Lang A. Acute onset dystonic camptocormia caused by lenticular lesions. Mov Disord 2001; 16: 177–80. Jankovic J. Botulinum toxin in clinical practice. J Neurol Neurosurg Psychiatry 2004; 75: 951–57. Duvoisin RC, Marsden CD. Note on the scoliosis of parkinsonism. J Neurol Neurosurg Psychiatry 1975; 38: 787–93. Indo T, Ando K. Studies on the scoliosis of parkinsonism. Clin Neurol 1980; 20: 40–46. Grimes JD, Hassan MN, Trent G, Halle D, Armstrong GW. Clinical and radiographic features of scoliosis in Parkinson’s disease. Adv Neurol 1987; 45: 353–55. Robin G, Span Y, Steinberg R, Makin M, Menczel J. Scoliosis in the elderly: a follow-up study. Spine 1982; 7: 355–59. Vanderpool D, James J, Wynne-Davies R. Scoliosis in the elderly. J Bone Joint Surg Am 1969; 51: 446–55. Carella F, Giovannini P, Girotti F, Testa D, Caraceni T. Dystonia and parkinson’s disease. Adv Neurol 1993; 60: 558–61. Khan NL, Graham E, Critchley P, et al. Parkin disease: a phenotypic study of a large case series. Brain 2003; 126: 1279–92. Kidron D, Melamed E. Forms of dystonia in patients with Parkinson’s disease. Neurology 1987; 37: 1009–11. Denny-Brown D. The nature of apraxia. J Nerv Ment Dis 1958; 126: 9–31. Pettigrew LC, Jankovic J. Hemidystonia: a report of 22 patients and a review of the literature. J Neurol Neurosurg Psychiatry 1985; 48: 650–57. Munchau A, Mathen D, Cox T, Quinn N, Marsden C, Bhatia K. Unilateral lesions of the globus pallidus: report of four patients presenting with focal or segmental dystonia. J Neurol Neurosurg Psychiatry 2000; 69: 494–98. Krystkowiak P, Martinat P, Defebvre L, Pruvo JP, Leys D, Destee A. Dystonia after striatopallidal and thalamic stroke: clinicoradiological correlations and pathophysiological mechanisms. J Neurol Neurosurg Psychiatry 1998; 65: 703–08. Perlmutter J, Tempel L, Black K, Parkinson D, Todd R. MPTP induced dystonia and parkinsonism: clues to the pathophysiology of dystonia. Neurology 1997; 49: 1432–38. Lissitza FM, Pentzik AS. Tonic neck reflexes in lesions of the cerebral cortex in dogs. J Comp Neurol 1934; 60: 185–200. Mettler FA, Mettler CC. The effects of striatal injury. Brain 1942; 65: 242–55. Laursen AM. Movements evoked from the region of the caudate nucleus in cats. Acta Physiol Scand 1962; 54: 175–84. Martin JP. The basal ganglia and posture. London: Pitman, 1967: 100–05. Herrera-Marschiz M, Utsumi H, Ungerstedt U. Scoliosis in rats with experimentally-induced hemiparkinsonism: dependence upon striatal dopamine denervation. J Neurol Neurosurg Psychiatry 1990; 53: 39–43. Lundblad M, Picconi B, Lindgren H, Cenci MA. A model of LDOPA-induced dyskinesia in 6-hydroxydopamine lesioned mice: relation to motor and cellular parameters of nigrostriatal function. Neurobiol Dis 2004; 16: 110–23. Fahn S, Marsden CD, Calne DB. Classification and investigation of dystonia. In: Marsden CD, Fahn S, eds. Movement disorders 2. London: Butterworth, 1987: 332–58. Denny A, Behari M. Motor fluctuations in Parkinson’s disease. J Neurol Sci 1999; 165: 18–23. Hewett TE. Neuromuscular and hormonal factors associated with knee injuries in female athletes. Sports Med 2000; 29: 313–27. Huston LJ, Greenfield MLVH, Wojtys EM. Anterior cruciate ligament injuries in the female athlete. Clin Orthop 2000; 372: 50–63. 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 100 101 102 103 104 105 106 107 108 109 Messina DF, Farney WC, DeLee JC. The incidence of injury in high school basketball: a prospective study among male and female athletes. Am J Sports Med 1999; 27: 294–99. Wojtys EM, Huston LJ, Lindenfeld TN, Hewett TE, Greenfield MN. Association between the menstrual cycle and anterior cruciate ligament injuries in female athletes. Am J Sports Med 1998; 26: 614–19. Charlton WPH, Coslett-Charlton LM, Ciccotti MG. Correlation of estradiol in pregnancy and anterior cruciate ligament laxity. Clin Orthop 2001; 387: 165–70. Deie M, Sakamaki Y, Sumen Y, Urabe Y, Ikuta Y. Anterior knee laxity in young women varies with their menstrual cycle. Int Orthop 2002; 26: 154–56. Fischer GM. Comparison of collagen dynamics in different tissues under the influence of estradiol. Endocrinology 1973; 93: 1216–18. Hama H, Yamamuro T, Takeda T. Experimental studies on connective tissue of the capsular ligament: influences of aging and sex hormones. Acta Orthop 1976; 47: 473–79. Liu SH, Al-Shaikh RA, Panossian V, Finerman GAM, Lane JM. Estrogen affects the cellular metabolism of the anterior cruciate ligament: a potential explanation for female athletic injury. Am J Sports Med 1997; 25: 704–09. Rasanen T, Messnser K. Estrogen-dependent tensile properties of the rabbit knee medial collateral ligament. Scand J Med Sci Sports 2000; 10: 20–27. Liu SH, Al-Shaikh R, Panossian V, et al. Primary immunolocalization of estrogen and progesterone target cells in the human anterior cruciate ligament. J Orthop Res 1996; 14: 526–33. Fischer GM, Swain ML. Effect of sex hormones on blood pressure and vascular connective tissue in castrated and noncastrated male rats. Am J Physiol 1977; 232: H617–21. Shikata J, Sanada H, Tamamuro T, Takeda T. Experimental studies of the elastic fiber of the capsular ligament: influence of ageing and sex hormones of the hip joint capsule of rats. Connect Tissue Res 1979; 7: 21–27. Yamamuro T, Hama H, Takeda T, Shikata J, Sanada H. Biomechanical and hormonal factors in the etiology of congenital dislocation of the hip joint. Int Orthop 1977; 1: 231–36. Bryant-Greenwood GD, Schwabe C. Human relaxins, chemistry and biology. Endocr Rev 1994; 15: 5–26. Unemori EN, Amento EP. Relaxin modulates synthesis and secretion of procollagenase and collagen by human fibroblasts. J Bio Chem 1990; 25: 10681–85. Cordivari C, Misra VP, Catania S, Lees AJ. Treatment of dystonic clenched fist with botulinum toxin. Mov Disord 2001; 16: 907–13. O’Dwyer NJ, Ada L, Neilson PD. Spasticity and muscle contractures following stroke. Brain 1996; 119: 1737–49. Hufschsmidt A, Mauritz KH. Chronic transformation of muscle in spasticity: a peripheral contribution to increase tone. J Neurol Neurosurg Psychiatry 1985; 48: 676–85. Cantello R, Gianelli M, Civardi C, Mutani R. Parkinson’s disease rigidity: EMG in a small hand muscle at “rest.” Electroencephalography Clin Neurophysiol 1995; 97: 215–22. Duvoisin RC. Digital vasospasm with bromocriptine. Lancet 1976; 2: 204. Wass JA, Thorner MO, Besser GM. Digital vasospasm with bromocriptine. Lancet 1976; 1: 1135. Rinne UK, Krupp P, Le Witt PA, Calne DB. Pleuropulmonary changes during long-term bromocriptine treatment for Parkinson’s disease. Lancet 1981; 1: 44–45. Rinne UK. Early dopamine agonist therapy in Parkinson’s disease. Mov Disord 1989; 4: S86–94. Besser GM, Wass JA. Pleuro-pulmonary shadows on bromocriptine. Lancet 1981; 1: 323. Ward CD, Thompson J, Humby MD. Pleuropulmonary and retroperitoneal fibrosis associated with bromocriptine treatment. J Neurol Neurosurg Psychiatry 1987; 50: 1706–07. Bowler JV, Ormerod IE, Legg NJ. Retroperitoneal fibrosis and bromocriptine. Lancet 1986; 2: 466. Demonet JF, Rostin M, Dueymes JM, Ioualalen A, Montastruc JL, Rascol A. Retroperitoneal fibrosis and treatment of Parkinson’s disease with high doses of bromocriptine. Clin Neuropharmacol 1986; 9: 200–01. http://neurology.thelancet.com Vol 4 July 2005 Review 110 Stecker JF, Rawls HP, Devine CJ, Devine PC. Retroperitoneal fibrosis and ergot derivatives. J Urol 1974; 112: 30–32. 111 Makridis C, Rastad J, Oberg K, Akerstrom G. Progression of metastases and symptom improvement from laparotomy in midgut carcinoid tumors. World J Surg 1996; 20: 900–06. 112 Scott J, Foster R, Moore A. Retroperitoneal fibrosis and nonmalignant ileal carcinoid. J Urol 1987; 138: 1435. 113 Morin LJ, Zuerner RT. Retroperitoneal fibrosis and carcinoid tumor. JAMA 1971; 216: 1647–48. 114 Modlin IM, Shapiro MD, Kidd M. Carcinoid tumors and fibrosis: an association with no explanation. Am J Gastroenterol 2004; 99: 2466–78. 115 Gupta A, Saibil F, Kassim O, McKee J. Retroperitoneal fibrosis caused by carcinoid tumour. QJM 1985; 56: 367–75. 116 Moller J, Connolly H, Rubin J, Seward JB, Modesto K, Pellikka PA. Factors associated with progression of carcinoid heart disease. N Engl J Med 2003; 348: 1005–15. 117 Waltenberger J, Lundin L, Oberg K, et al. Involvement of transforming growth factor-beta in the formation of fibrotic lesions in carcinoid heart disease. Am J Pathol 1993; 142: 71–78. 118 Nilsson J, von Euler AM, Dalsgaard CJ. Stimulation of connective tissue cell growth by substance P and substance K. Nature 1985; 315: 61–63. 119 Funa K, Papanicolaou V, Juhlin C, et al. Expression of plateletderived growth factor beta-receptors on stromal tissue cells in human carcinoid tumors. Cancer Res 1990; 50: 748–53. http://neurology.thelancet.com Vol 4 July 2005 120 Chaudhry A, Papanicolaou V, Oberg K, Heldin CH, Funa K. Expression of platelet-derived growth factor and its receptors in neuroendocrine tumors of the digestive system. Cancer Res 1992; 52: 1006–12. 121 Nilsson O, Wangberg B, McRae A, Dahlstrom A, Ahlman H. Growth factors and carcinoid tumours. Acta Oncol 1993; 32: 115–24. 122 Chaudhry A, Oberg K, Gobl A, Heldin CH, Funa K. Expression of transforming growth factors beta 1, beta 2, beta 3 in neuroendocrine tumors of the digestive system. Anticancer Res 1994; 14: 2085–91. 123 Moore T, Evans W, Murray D. Operative management of foot and ankle equinovarus associated with focal dystonia. Foot Ankle Int 1998; 19: 229–31. 124 Deonna T, Ferreira A. Idiopathic fluctuating dystonia: a case of foot dystonia and writer’s cramp responsive to L-dopa. Dev Med Child Neurol 1985; 27: 819–21. 125 Cooper IS. Ligation of the anterior choroidal artery for involuntary movements of Parkinsonism. Psychiatr Q 1953; 27: 317–19. 126 Cooper IS. Neurosurgical treatment of dyskinesias. Clin Neurosurg 1977; 24: 367–90. 127 Cooper IS, Samra K, Bergmann L. The thalamic lesion which abolishes tremor and rigidity of parkinsonism: a radiologicoclinico-anatomic correlative study. J Neurol Sci 1969; 8: 69–84. 128 Ohye C, Shibazaki T. Lesioning the thalamus for dyskinesia. Stereotact Funct Neurosurg 2001; 77: 33–39. 431
 0
0
Anuncio
Documentos relacionados




Descargar
Anuncio
Añadir este documento a la recogida (s)
Puede agregar este documento a su colección de estudio (s)
Iniciar sesión Disponible sólo para usuarios autorizadosAñadir a este documento guardado
Puede agregar este documento a su lista guardada
Iniciar sesión Disponible sólo para usuarios autorizados