Retroperitoneal Hematoma Management in Trauma Laparotomy
Anuncio

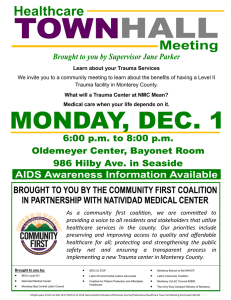
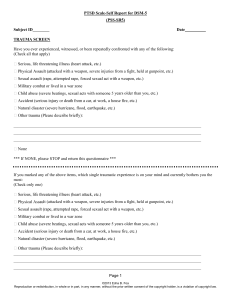
G Model JINJ-5631; No. of Pages 6 Injury, Int. J. Care Injured xxx (2014) xxx–xxx Contents lists available at ScienceDirect Injury journal homepage: www.elsevier.com/locate/injury The management of retroperitoneal haematoma discovered at laparotomy for trauma§ N. Manzini, T.E. Madiba * Department of Surgery, University of KwaZulu-Natal, King Edward VIII Hospital, Durban, South Africa A R T I C L E I N F O A B S T R A C T Article history: Accepted 25 January 2014 Aim: To review our local experience with presentation and management of retroperitoneal haematomas (RPH) discovered at laparotomy and factors affecting outcome. Methods: Patients with retroperitoneal haematomas (RPHs) were identified from a prospective database. Data collected included demographics, clinical presentation, zones and organs involved, management and outcome. Results: Of a total of 488 patients with abdominal trauma, 145 (30%) with RPH were identified 136 of whom were male (M:F = 15:1). Mean age was 28.8 (SD 10.6) years and median delay before surgery was 7 h. The injury mechanisms were firearms (109), stabs (24), and blunt trauma (12). Twenty-four patients (17%) presented with shock. There were 58 Zone I, 69 Zone II, and 38 Zone III haematomas. The median injury severity score (ISS) was 9. Fifty-two patients (36%) developed complications and 26 (18%) patients died. Sixty-four (44%) patients required ICU with median ICU stay of 3 days. All Zone I injuries were explored; Zones II and III were explored selectively. The mortality for Zones I, II, III and IV was 14%, 4%, 29% and 35%, respectively. Mortality was highest for blunt trauma and lowest for stabs (p = 0.146). Twelve of 24 patients with shock died (50%) compared to 14 of 121 (12%) without shock (p < 0.0001). Eighteen of 64 patients with <6-h delay before surgery died (28%) compared to 8 of 81 (10%) with >6-h delay (p < 0.017). Mortality increased with increasing ISS. Median hospital stay was 8 days. Conclusion: RPH accounted for 30% of abdominal trauma. Injury mechanism, presence of shock, delay before surgery and ISS showed a significant association with mortality. ß 2014 Elsevier Ltd. All rights reserved. Keywords: Retroperitoneal Haematomas Blunt trauma Penetrating trauma Introduction The retroperitoneal area is a wide space lying posterior to the peritoneal cavity and contains completely or envelops anteriorly a number of visceral and vascular structures in the gastrointestinal, genitourinary, vascular, musculoskeletal, and nervous systems [1]. It is bounded posteriorly by the transversalis fascia and extends from the diaphragm to the pelvic inlet. A retroperitoneal haematoma (RPH) results from injury to gastrointestinal, genito-urinary, vascular and muscular structures within this space [1,2]. Kudsk and Sheldon [3] first introduced a location-based classification of traumatic RPH as central–medial (Zone I), flank or peri-renal (Zone II), and pelvic (Zone III). This principle was § Presented at Congress of the Surgical Research Society of Southern Africa, Stellenbosch, 12–13 July 2012. * Corresponding author at: Department of Surgery, University of KwaZulu-Natal, Private Bag 7, Congella 4013, South Africa. Tel.: +27 31 260 4219; fax: +27 31 260 4389. E-mail address: [email protected] (T.E. Madiba). immediately accepted and became a standard treatment policy for RPH [4]. A Zone I haematoma is bounded superiorly by the central diaphragm, by the medial borders of the psoas muscles at its sides and the pelvis inferiorly. Injuries of the great vessels of the abdomen, pancreas and duodenum are the commonest aetiologies [5]. A Zone II haematoma lies lateral to the psoas muscles, above the iliac wings and under the diaphragm and may result from injuries to the ascending or descending colon, duodenum, kidney, genito-urinary vascular structures, ureters and muscular vessels [5,6]. A Zone III haematoma is located in the pelvis limited with the dome of the bladder at the front, sacral promontory at the rear and iliac wings at both sides [5]. The majority of pelvic haematomas arise from injury to the pre-sacral or pre-vesical veins; other less common causes include arterial bleeds and haemorrhage from a variety of pelvic fracture sites [1,7]. Bleeding of venous origin may stop spontaneously when local venous pressure and the pressure of the retroperitoneal space equalise [7]. Fig. 1 shows a CT scan of a patient with a Zone II retroperitoneal haematoma with medial extension in to Zone I area. Despite adequate data regarding the management of RPH in developed countries, data emanating from developing countries are scarce. We hypothesised that this condition occurs with equal 0020–1383/$ – see front matter ß 2014 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.injury.2014.01.026 Please cite this article in press as: Manzini N, Madiba TE. The management of retroperitoneal haematoma discovered at laparotomy for trauma. Injury (2014), http://dx.doi.org/10.1016/j.injury.2014.01.026 G Model JINJ-5631; No. of Pages 6 N. Manzini, T.E. Madiba / Injury, Int. J. Care Injured xxx (2014) xxx–xxx 2 employed in stable patients following blunt trauma. Haemodynamic instability or shock is defined as systolic blood pressure below 90 mmHg despite administration of 2000 ml crystalloids or 2 units packed red blood cells [7]. All haemodynamically unstable patients are resuscitated; if they respond to resuscitation they are assessed regarding the need for emergency laparotomy. Patients with equivocal signs are managed by regular clinical evaluation and CT scan where indicated. Patients who do not respond to resuscitation undergo emergency laparotomy. This study therefore includes patients with refractory shock or haemodynamic instability, and stable patients with signs of intra-peritoneal haemorrhage or injury who require immediate laparotomy. The severity of injuries was measured using the injury severity score (ISS) [9]. The severity of organ injury was graded according to American Association for the Surgery of Trauma [10]. The management of RPH at laparotomy depended on the site and behaviour of the haematoma, and the haemodynamic status of the patient. All Zone I injuries were explored by ‘opening’ the haematoma after vascular control was achieved and the various organs were managed on their merit. Zones II and III haematomas were selectively explored, the indications for exploration being a pulsating or expanding haematoma, overt bleeding and evidence of hollow visceral injury. If the patient was unstable and there was no other identifiable cause of bleeding, the haematoma was explored regardless of the site. The management of all injured organs followed standard management protocols for the various organ injuries. Data were collected on a proforma datasheet and were subsequently transferred into a Microsoft Excel1 spreadsheet. Fractions were rounded off to one decimal place. Percentages were rounded off to the nearest whole numbers. Statistical analysis was carried out using the Statistical Package for the Social Sciences version 21 (SPSS-SA, Cape Town, South Africa). The chi-squared test with Yates’ continuity correction was used for shock, hollow visceral injury and delay. The chi-squared test was used for type of trauma, ISS category and zone. Fig. 1. CT scans showing retroperitoneal haematoma. (A) An axial CT scan with the haematoma designated by solid arrows. The hollow arrow shows traumatic injury to the right kidney. (B) is a sagittal CT scan of the same patient. frequency regardless of income level and that management principles are the same. The purpose of the study therefore was to document local experience with traumatic retroperitoneal haematomas discovered at laparotomy and to establish factors that may affect outcome. Patients and methods Ethics approval was attained from the University of KwaZuluNatal’s Biomedical Ethics Research Committee (E057/98). A database of patients with abdominal trauma [8] was established in 1998 in a single surgical ward at King Edward VIII Hospital, a tertiary hospital with three surgical wards, situated in Durban, on the south coast of the KwaZulu-Natal Province of South Africa. The database spanned a period of seven years (1998–2004) and excluded all paediatric patients (age < 12 years) as they are managed separately by the paediatric surgeons. From a dedicated proforma data were subsequently transferred onto an Excel database and included demographics, clinical presentation, findings at surgery, management and outcome. Patients who were found to have retroperitoneal haematoma at laparotomy were extracted and analysed for the purpose of this study. The management of abdominal trauma in our institution adheres to the following protocol. All patients with trauma are resuscitated according to Advanced Trauma Life Support principles. Computed Tomography (CT) scan is the first investigation Results There were 488 patients with abdominal trauma of whom 145 (30%) had RPH, with 136 males giving a male: female ratio of 15:1. The mean age was 28.8 (SD 10.6) years. One hundred and thirty three injuries were due to penetrating trauma (firearms 109, stabs 24) and 12 were due to blunt trauma. Twenty-four patients (17%) presented with haemorrhagic shock. The median delay before surgery was 7 h with an interquartile range (IQR) of 5.5 (the 25th centile was 4.5 and the 75th centile was 10). There were 58 Zone I, 69 Zone II, 38 Zone III haematomas. Twenty of these patients had involvement of more than one zone (Zone IV). The median ISS was 9 with an interquartile range of 7 (25th centile was 9 and the 75th centile was 16). The individual organ injuries and their management are shown in Table 1. The most commonly injured organs were the colon, kidney, duodenum, pancreas, urinary bladder, and rectum in that order. Twenty-one (64%) of 33 injured kidneys were salvaged with only 12 (36%) undergoing nephrectomy. Eleven nephrectomies (41%) followed firearms injuries. Twenty-two (96%) of 23 pancreatic injuries were managed by simple drainage. Sixty-one of 64 injuries in Zone I (95%) required some form of surgical intervention such as repair, drainage or ligation. Sixty of 75 injuries in Zone II (80%) required surgical intervention and all Zone III injuries (100%) required intervention. Fifty-two (36%) patients developed complications (Table 2). There were eleven patients with fistulae [pancreatic (4), enterocutaneous (3), colo-cutaneous (1), gastro-cutaneous (1), rectovesical (1) and colo-vesico-cutaneous (1)]. Six patients developed Please cite this article in press as: Manzini N, Madiba TE. The management of retroperitoneal haematoma discovered at laparotomy for trauma. Injury (2014), http://dx.doi.org/10.1016/j.injury.2014.01.026 G Model JINJ-5631; No. of Pages 6 N. Manzini, T.E. Madiba / Injury, Int. J. Care Injured xxx (2014) xxx–xxx Table 1 Number of organs injured in each zone and their management in 145 patients. Organ injury Surgical intervention Conservative management Zone I Duodenum (n = 27)a Pancreas (n = 23)b Inferior vena cava (n = 8)c Aorta (n = 4)d Superior mesenteric vessel (n = 1)e Gonadal vessel (n = 1)f 24 23 8 4 1 1 (88%) (100%) (100%) (100%) (100%) (100%) 3 (12%) 0 0 0 0 0 Zone II Kidney (n = 33)g Colon (n = 36)h Ureters (n = 6)i 18 (55%) 36 (100%) 6 (100%) 15 (45%) 0 0 Zone III Bladder (n = 19)j Rectum (n = 18)k 19 (100%) 18 (100%) a b c d e f g h i j k 0 0 Table 3 Mortality with respect to different parameters. Parameter n (died) Mortality (%) p Shock (n = 24) No shock (n = 121) HVI (n = 109) No HVI (n = 36) Delay < 6 h (n = 64) Delay > 6 h (n = 81) Stabs (n = 24) Firearms (n = 109) Blunt (n = 12) ISS < 9 (n = 86) ISS = 10–20 (n = 40) ISS > 20 (n = 19) Zone I only (n = 41) Zone II only (n = 50) Zone III only (n = 34) Zone IV (n = 20) 12 14 21 4 18 8 1 22 3 10 7 9 8 3 8 7 50 12 19 11 28 10 4 20 25 12 18 47 20 6 24 35 <0.0001 0.324 0.017 0.146 0.001 0.021 HVI, hollow visceral injury; ISS, injury severity score. Primary repair (19), pyloric exclusion (5). Drainage (22), duct ligation (1). Repaired (7), ligated (1). All repaired. Repaired. Ligated. Nephrectomy (12), renorrhaphy (6). All primary repair. All primary repair. Primary repair (12), suprapubic catheter (7). Primary repair (8), colostomy (10). trauma and lowest for stabs (p = 0.146). Eighteen (28%) patients with delay of <6 h before surgery died compared to seven (10%) with a delay >6 h (p = 0.017). Factors influencing mortality are shown on Table 3. The median hospital stay was 8 days with an IQR of 11 (25th centile 5; 75th centile 16). Discussion peritonitis; turbid sero-sanguinous fluid was discovered at laparotomy in four patients and purulent peritonitis in two (one with multiple solid organ injuries and the other with gastric injury in addition to other solid organ injuries). Sixty-four (44%) patients were managed in the ICU with a median ICU stay of 3 days and IQR of 5.3 (25th centile = 1.8; 75th centile 7). Twenty-six patients died, giving a mortality rate of 18%. Causes of death were MODS (15), hypovolaemic shock (6), sepsis (4) and one died from overwhelming tuberculous infection. Eight of 41 patients with Zone I only haematomas died (20%); three of these had associated major vascular injury. Three of 50 patients with Zone II only haematomas died (6%) none of whom had associated major vascular injury. Eight of 34 patients with Zone III only haematomas died (24%) none of whom had major vascular injury. Seven of 20 patients with haematoma involving more than one zone (Zone IV) died (35%) of whom two had major vascular injury. In summary vascular injury contributed 19% to the mortality; among central haematomas vascular injury contributed 38%. Three of 12 (25%) patients with blunt trauma died compared to 23 of 133 (17%) with penetrating trauma. Twelve of 24 patients with shock on presentation (50%) died compared to 14 of 121 (12%) without shock (p < 0.0001). Mortality was highest for blunt Table 2 Complications in 145 patients with RPH. Complication n % Chest infection MODS Wound sepsis Fistulae Peritonitis Intestinal obstruction Shock Bleeding Sepsis Intra-abdominal abscess Deep venous thrombosis Anastomosis dehiscence 20 15 14 11 6 6 6 5 4 1 1 1 14 10 10 8 4 4 4 3 3 1 1 1 MODS, multiple organ dysfunction syndrome. 3 RPH accounted for 30% of patients with abdominal trauma in this series, with males predominating, whereas the incidence of RPH based on aetiology is quoted at 44–80% for blunt trauma and 6–33% for penetrating trauma [1,2,5,11–13]. Firearms were responsible for 81% of penetrating trauma which is higher than the reported 64% [14]. These differences are not surprising inasmuch as clinical presentation is determined by the organ involved, the severity of the injury and the causative mechanism [13]. The variation in the prevalence further attests to the differing trends in penetrating and blunt trauma in various centres, which is dependent upon the environment of the receiving institution [14]. This fact was highlighted by Muckart et al. who demonstrated a change in trauma patterns over two consecutive decades in the KwaZulu-Natal Province of South Africa [15]. Patients with RPH can be categorised into (i) patients with refractory shock or haemodynamic instability, (ii) stable patients with signs of intra-peritoneal haemorrhage and (iii) asymptomatic patients [2]. Patients in this series included only the first and second categories and immediate laparotomy was therefore mandatory and preoperative investigations were not an option. In patients with haemodynamic instability timely resuscitation is a vital component of initial management [16,17]. Where haemodynamic stability and metabolic correction cannot be established laparotomy remains part of resuscitation. CT of the abdomen and pelvis is the mainstay of diagnosis for abdominal injury in the haemodynamically stable patient [6,7,14,18]. As in other series [2] the most commonly injured organ was the colon. The management of specific injuries was according to standard management principles. In total 64% of injured kidneys were salvaged. The majority of pancreatic injuries were managed conservatively by simple drainage (96%), which supports the local trend of conservative surgical management of pancreatic injuries [19,20]. Ninety-five per cent of injuries in Zone I required some sort of surgical intervention such as repair, drainage or ligation. This strongly supports the need for exploration of Zone I injuries. The proportion of haematomas harbouring injuries requiring similar intervention was 80% and 100% for Zones II and III respectively. These figures again send a very clear argument for exploration of RPHs following penetrating trauma. Please cite this article in press as: Manzini N, Madiba TE. The management of retroperitoneal haematoma discovered at laparotomy for trauma. Injury (2014), http://dx.doi.org/10.1016/j.injury.2014.01.026 G Model JINJ-5631; No. of Pages 6 4 N. Manzini, T.E. Madiba / Injury, Int. J. Care Injured xxx (2014) xxx–xxx Morbidity and mortality rates associated with traumatic RPH remain high despite improvements in pre-hospital care, transport, and intensive care [4]. The complication rate of 36% was slightly higher than the reported 28% but the mortality rate of 18% compared favourably to the reported 18–60% [1,2,12,13,21–23]. This mortality rises to 90% in patients who are in extremis on arrival in hospital [22]. The main mechanism of death in patients with RPH is either exsanguination from uncontrollable haemorrhage or MODS as an inevitable consequence of devastating injury and the resultant instability [13]. The ISS was a significant predictor of mortality suggesting that the severity of injury is a reliable predictor of MODS and death. However, some authors have failed to show an association between ISS and mortality [23]. Shock, as previously reported in a local study [8], was associated with mortality in this series signifying the role played by haemodynamic instability in the mechanism of death. Other features of physiological instability which have been shown to influence mortality are massive transfusion, metabolic acidosis, hypothermia and coagulopathy [8,21]. The number of injured organs has also been shown to be directly related to mortality [8,21]. Hollow visceral injury did not influence mortality suggesting that the involvement or sparing of hollow viscera had no influence. Blunt trauma was associated with a higher mortality rate compared to penetrating trauma but this association did not reach statistical significance in this study although Mnguni et al. showed a positive relationship between injury mechanism and mortality in abdominal trauma [8]. The lack of significant difference in mortality between zones attests to the fact that the cause of mortality is the organ injury rather than the anatomical location of the haematoma. Bleeding in more than one retroperitoneal compartment results from trauma to a larger surface area and multiple organs; hence the high mortality associated with more than one zone seen in this and other series [2]. The higher mortality for early presenters was surprising in this study. Intuitively one would expect that a longer delay before surgery would be associated with a higher mortality. This aberration can be explained by the concept of ‘‘self-triage’’ whereby delays in reaching definitive care would select those with lesser severity of injury who are more likely to survive. Unfortunately, even within an urban environment, delays in reaching definitive surgical care are common in our practice with inter-hospital transfer times frequently exceeding 8 h [24]. The management of RPH depends on the haematoma location and its behaviour as described by Kudsk and Sheldon [3]. Traditional RPH management strategies have recommended mandatory exploration of all Zone I haematomas discovered at laparotomy because of the high possibility of major vascular or visceral injury and selective exploration of Zones II and III haematomas depending on the cause and its behaviour, the main indication for exploration being a pulsating or expanding haematoma and possible visceral and vascular injury [1,2,12,13,23]. Exploration permits direct control of bleeding and management of hollow visceral injuries [25]. Surgical exploration of the injured organs, however, necessitates retroperitoneal access with the attendant risk of uncontrollable haemorrhage [5,7]. The limitation of this approach has been the assumption that blunt and penetrating trauma behave similarly. This classic tri-compartment model has been recently modified, however, to reflect the understanding that the fascia separating the spaces is laminar, variably fused, and potentially expandable as a result of embryologic partial fusion of the dorsal mesenteries [4]. Inter-fascial communication exists between the retroperitoneal spaces and retroperitoneal haemorrhage or rapidly expanding fluid collections have been shown to spread via these inter-fascial connections [4,6]. Ishikawa et al. cautions that rather than explore all central haematomas blindly an attempt should be made to determine the bleeding source and the possible extension by means of inter-fascial planes [4]. For example bleeding that oozes from Zone II into Zone I may not necessarily need to be managed as Zone I haematoma [4]. The working algorithm shown in Fig. 2 is our suggested protocol for the management of RPH and is similar to previous suggestions but it incorporates the modifications suggested by Feliciano et al. [1] and Ishikawa et al. [4]. All central haematomas regardless of aetiology must be explored after proximal and distal vascular control because of the possibility of major vascular injury. The selective approach is advisable for Zones II and III haematomas due to blunt injuries. Lateral haematoma due to blunt trauma is generally not explored and exploration is advised after renovascular control only if the haematoma is pulsatile or expanding or in the presence of severe medullary injury, urinary extravasation, polar avulsion or blunt rupture. The para-duodenal and pericolonic haematomas require special attention, especially following penetrating trauma, because they may house hollow visceral injuries [1,2,4]. We advocate that these so-called medio-lateral haematomas should be explored for this reason. However, as opposed to opening the whole haematoma, there is a place for opening the haematoma along the tract of the missile to exclude injury to hollow visceral structures. In patients with pelvic haematoma the status of the femoral pulses should always be assessed before a decision is made on how to address the haematoma. The management of active retroperitoneal haemorrhage depends on the source of the haemorrhage. The surgical interventions to achieve haemostasis include surgical exploration of the vessels, use of fixation devices, and damage control surgery [7]. Pelvic haemorrhage from sites of fractures is not usually amenable to direct surgical control but may be slowed or stopped by fracture stabilisation [1]. Haemorrhage from venous plexuses or smaller veins will be tamponaded by the intact retroperitoneum [1]. Active venous bleeding can be stopped by extra-peritoneal packing and active arterial bleeding needs direct control or transarterial embolisation [4,7,22]. Where haemodynamic stability cannot be achieved at laparotomy by addressing the cause of pelvic haemorrhage damage control can be achieved by packing to control venous bleeding [4,7,12,16,22,26–29]. In patients with associated pelvic fracture additional pelvic stabilisation will assist in diminishing haemorrhage, provide easier nursing and allow early mobilisation [17,28– 30]. If bleeding persists after packing the site of bleeding is most likely arterial in origin [12]. Trans-arterial embolisation should be reserved for those patients who remain haemodynamically unstable and acidotic and require further transfusions after packing [4,7,16,22,28,29,31]. Ligation of one or both hypogastric arteries has been suggested in patients who are too unstable to wait for angiographic embolisation [12,32]. Pelvic fixation devices, which are thought to facilitate venous haemostasis are complementary to arterial embolisation [7]. There are some limitations in this study. Firstly, whereas our approach is similar to that depicted in Fig. 1, we concede that the data on blunt trauma in this study are based on only 12 patients and this figure is too small to give a generalisation with regard to the management of RPH following blunt trauma. Secondly the data were collected up to and including 2004 and are thus dated. We believe, however, that the principles enunciated in the paper are valid and are valuable to the trauma surgeon. In conclusion, penetrating trauma accounts for the majority of injuries in our setting. Haemodynamic instability, injury mechanism and high ISS are associated with a high mortality rate. Paradoxically, a delay in surgery had an inverse relationship to mortality. Please cite this article in press as: Manzini N, Madiba TE. The management of retroperitoneal haematoma discovered at laparotomy for trauma. Injury (2014), http://dx.doi.org/10.1016/j.injury.2014.01.026 G Model JINJ-5631; No. of Pages 6 N. Manzini, T.E. Madiba / Injury, Int. J. Care Injured xxx (2014) xxx–xxx 5 Fig. 2. Suggested algorithm for the management of retroperitoneal haematoma (* in penetrating trauma just following the tract is adequate to exclude injury. In blunt trauma exploration can be achieved by mobilisation of the colon and/or duodenum by means of right or left visceral rotation and Kocher’s manoeuvre). Please cite this article in press as: Manzini N, Madiba TE. The management of retroperitoneal haematoma discovered at laparotomy for trauma. Injury (2014), http://dx.doi.org/10.1016/j.injury.2014.01.026 G Model JINJ-5631; No. of Pages 6 N. Manzini, T.E. Madiba / Injury, Int. J. Care Injured xxx (2014) xxx–xxx 6 Conflict of interest Both authors do not have any conflict of interest. Acknowledgement The authors would like to thank Professor DJJ Muckart, Head of the Trauma Unit, Inkosi Albert Luthuli Central Hospital, for providing us with the picture of a CT scan taken from a patient with a retroperitoneal haematoma. References [1] Feliciano DV. Management of traumatic retroperitoneal hematoma. Ann Surg 1990;211(2):109–23. [2] Sultan J, Bilal BB, Kiran H, Bilal HB, Yusuf A. Management of retroperitoneal haematoma. Professional Med J 2005;12:230–6. [3] Kudsk KA, Sheldon GF. Retroperitoneal hematoma. In: Blaisdell FWT, editor. Abdominal trauma. New York: Thieme-Stratton; 1982. p. 279–93. [4] Ishikawa K, Tohira H, Mizushima Y, Matsuoka T, Mizobata Y, Yokota J. Traumatic retroperitoneal hematoma spreads through the interfascial planes. J Trauma 2005;59(3):595–607. discussion 607–8. [5] Muftuoglu MA, Topaloglu U, Aktekin A, Odabasi M, Ates M, Saglam A. The management of retroperitoneal hematomas. Scand J Trauma Resusc Emerg Med 2004;12:152–6. [6] Daly KP, Ho CP, Persson DL, Gay SB. Traumatic retroperitoneal injuries: review of multidetector CT findings. Radiographics 2008;28(6):1571–90. [7] Geeraets T, Chhor V, Cheisson G, Martin L, Bessoud B, Ozanne A, et al. Clinical review: initial management of blunt pelvic trauma patients with haemodynamic instability. Crit Care 2007;11(1):1–9. [8] Mnguni MN, Muckart DJ, Madiba TE. Abdominal trauma in Durban, South Africa: factors influencing outcome. Int Surg 2012;97(2):161–8. [9] Boyd CR, Tolson MA, Copes WS. Evaluating trauma care: the TRISS method. Trauma Score and the Injury Severity Score. J Trauma 1987;27(4):370–8. [10] Moore EE, Cogbill TH, Malangoni MA, Jurkovich GJ, Champion HR, Gennarelli TA, et al. Organ injury scaling, II: pancreas, duodenum, small bowel, colon, and rectum. J Trauma 1990;30(11):1427–9. [11] Grieco JG, Perry Jr JF. Retroperitoneal hematoma following trauma: its clinical importance. J Trauma 1980;20(9):733–6. [12] Henao F, Aldrete JS. Retroperitoneal hematomas of traumatic origin. Surg Gynecol Obstet 1985;161(2):106–16. [13] Madiba TE, Muckart DJ. Retroperitoneal haematoma and related organ injury – management approach. S Afr J Surg 2001;39(2):41–5. [14] Todd SR. Critical concepts in abdominal injury. Crit Care Clin 2004;20(1):119–34. [15] Muckart DJ, Meumann C, Botha JB. The changing pattern of penetrating torso trauma in KwaZulu/Natal – a clinical and pathological review. S Afr Med J 1995;85(11):1172–4. [16] Midwinter MJ, Woolley T. Resuscitation and coagulation in the severely injured trauma patient. Philos Trans R Soc Lond B Biol Sci 2011;366(1562):192–203. [17] Mohanty K, Musso D, Powell JN, Kortbeek JB, Kirkpatrick AW. Emergent management of pelvic ring injuries: an update. Can J Surg 2005;48(1):49–56. [18] Maull KI, Rozycki GS, Vinsant GO, Pedigo RE. Retroperitoneal injuries: pitfalls in diagnosis and management. South Med J 1987;80(9):1111–5. [19] Chinnery GE, Madiba TE. Pancreaticoduodenal injuries: re-evaluating current management approaches. S Afr J Surg 2010;48(1):10–4. [20] Madiba TE, Mokoena TR. Favourable prognosis after surgical drainage of gunshot: stab or blunt trauma of the pancreas. Br J Surg 1995;82(9): 1236–9. [21] Cherkas D. Traumatic hemorrhagic shock: advances in fluid management. Emerg Med Pract 2011;13(11):1–19. quiz 19–20. [22] Osborn PM, Smith WR, Moore EE, Cothren CC, Morgan SJ, Williams AE, et al. Direct retroperitoneal pelvic packing versus pelvic angiography: a comparison of two management protocols for haemodynamically unstable pelvic fractures. Injury 2009;40(1):54–60. [23] Selivanov V, Chi HS, Alverdy JC, Morris Jr JA, Sheldon GF. Mortality in retroperitoneal hematoma. J Trauma 1984;24(12):1022–7. [24] Cheddie S, Muckart DJ, Hardcastle TC, Den Hollander D, Cassimjee H, Moodley S. Direct admission versus inter-hospital transfer to a level I trauma unit improves survival: an audit of the new Inkosi Albert Luthuli Central Hospital trauma unit. S Afr Med J 2011;101(3):176–8. [25] Costa M, Robbs JV. Management of retroperitoneal haematoma following penetrating trauma. Br J Surg 1985;72(8):662–4. [26] Lee JC, Peitzman AB. Damage-control laparotomy. Curr Opin Crit Care 2006;12(4):346–50. [27] Loveland JA, Boffard KD. Damage control in the abdomen and beyond. Br J Surg 2004;91(9):1095–101. [28] Burlew CC, Moore EE, Smith WR, Johnson JL, Biffl WL, Barnett CC, et al. Preperitoneal pelvic packing/external fixation with secondary angioembolization: optimal care for life-threatening hemorrhage from unstable pelvic fractures. J Am Coll Surg 2011;212(4):628–35. discussion 35–7. [29] Gansslen A, Hildebrand F, Pohlemann T. Management of hemodynamic unstable patients in extremis with pelvic ring fractures. Acta Chir Orthop Traumatol Cech 2012;79(3):193–202. [30] Tosounidis TI, Giannoudis PV. Pelvic fractures presenting with haemodynamic instability: treatment options and outcomes. Surgeon 2013;11(6):344–51. [31] Papakostidis C, Kanakaris N, Dimitriou R, Giannoudis PV. The role of arterial embolization in controlling pelvic fracture haemorrhage: a systematic review of the literature. Eur J Radiol 2012;81(5):897–904. [32] DuBose J, Inaba K, Barmparas G, Teixeira P, Schnuriger B, Talving P. Bilateral internal iliac artery ligation as a damage control approach in massive retroperitoneal bleeding after pelvic fracture. J Trauma 2010;69(6):1507–14. Please cite this article in press as: Manzini N, Madiba TE. The management of retroperitoneal haematoma discovered at laparotomy for trauma. Injury (2014), http://dx.doi.org/10.1016/j.injury.2014.01.026