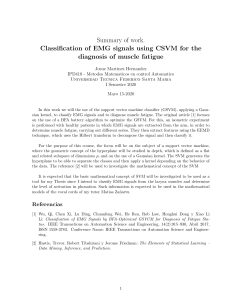
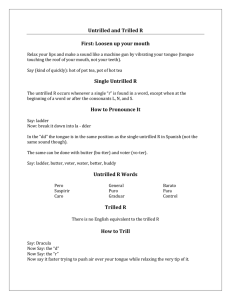
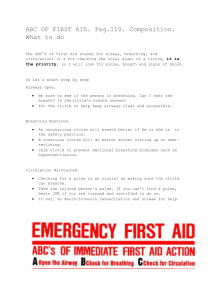
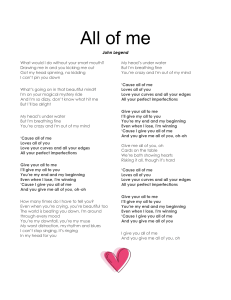
RESEARCH ARTICLE Effect of changes in the breathing mode and body position on tongue pressure with respiratory-related oscillations Shigeki Takahashi, DDS,a Takashi Ono, DDS, PhD,b Yasuo Ishiwata, DDS, PhD,c and Takayuki Kuroda, DDS, PhDd Tokyo, Japan The purpose of this study was to examine whether tongue pressure on the lingual surface of the mandibular incisors shows respiratory-related changes, with particular attention paid to its relationship to genioglossus electromyographic activity, and to determine the effect of changes in the mode of breathing and body position on tongue pressure. Tongue pressure was recorded with a miniature pressure sensor incorporated in a custom-made intraoral appliance in nine male subjects in different breathing modes and body positions. Electromyographic activity of the genioglossus muscle and respiratory-related movement were recorded simultaneously. Tongue pressure showed respiratory-related cyclic oscillations, with a maximum value during expiration and a minimum value during inspiration. In contrast, the activity of the genioglossus muscle showed a maximum amplitude during inspiration and a minimum amplitude during expiration. The maximum tongue pressure during oral breathing was significantly greater (P < .01) than during nasal breathing in both the upright and supine positions. Changes in body position significantly affected the maximum tongue pressure during oral breathing. The activity of the genioglossus muscle changed significantly with different breathing modes and body positions. Changes in the position of the hyoid bone produced by changes in the breathing mode and body position appear to have a critical role in determining tongue pressure. (Am J Orthod Dentofacial Orthop 1999;115:239-46) S oft tissues in the orofacial region exert weak but consistent forces on the teeth according to the classical equilibrium theory,1 which has been reevaluated.2,3 Tongue pressure is considered to be a particularly important factor in the diagnosis and prognosis of orthodontic treatment. The genioglossus (GG) muscle is the main protruder of the tongue, and also acts as an accessory respiratory muscle. Contraction of the GG muscle advances the base of the tongue and dilates the upper airway. Rhythmic electromyographic (EMG) activity of the GG muscle in pace with respiration has been reported in both animals and human beings.4-7 Therefore, we would expect that tongue pressure should show respiratory-related changes. In addition, increased GG EMG From the Faculty of Dentistry, Tokyo Medical and Dental University, Tokyo, Japan. This work was supported by Grants-in-Aid for Scientific Research Projects, (07407060 and 09470467) from the Japanese Ministry of Education, Science and Culture. aGraduate student, Department of Maxillo-Facial Orthognathics, Division of Life Science of Maxillo-Facial Systems, Graduate School of Dentistry. bAssistant Professor, Second Department of Orthodontics. cPart-time lecturer, Second Department of Orthodontics. dProfessor and Head, Second Department of Orthodontics. Reprint requests to: Shigeki Takahashi, DDS, Second Department of Orthodontics, Tokyo Medical and Dental University, 5-45 Yushima 1-chome, Bunkyo-ku, Tokyo, 113-8549 Japan; E-mail, [email protected] Copyright © 1999 by the American Association of Orthodontists. 0889-5406/99/$8.00 + 0 8/1/91723 activity in the supine body position has been reported in human beings.8,9 Considering these functional characteristics, respiratory-related changes in GG EMG activity may contribute to changes in tongue pressure on the lingual surface of the mandibular incisors. Consequently, tongue pressure may depend on the breathing mode and body position. The effects of changes in the head position and mode of breathing on intraoral pressure have been investigated in several previous studies.10-12 Archer and Vig11 reported that the tongue pressure on the lingual surface of the mandibular incisors tended to decrease with head extension and to increase with head flexion in subjects with Class I malocclusions. They pointed out that the tongue played an important role in producing skeletodental morphologic variation associated with altered head position. Hellsing and L’Estrange12 showed changes in lip pressure during extension and flexion of the head and changes in the mode of breathing and predicted that intraoral pressure could affect the inclination and position of the incisors. However, there has been no report of the possible effect of rhythmic changes in intraoral pressure associated with respiration. The purpose of this study was twofold: (1) to examine whether tongue pressure on the lingual surface of the mandibular incisors showed respiratory-related changes, with particular attention to its relationship 239 240 Takahashi et al Fig 1. Occlusal view of a custom pressure-recording appliance on a plaster model. Thickness of the appliance at pressure sensor is approximately 1 mm. Arrow indicates surface of pressure sensor. with GG EMG activity, and (2) to determine the effect of changes in the mode of breathing and body position on tongue pressure. MATERIAL AND METHODS Subjects This study was carried out in 10 skeletal Class I men with a mean age of 27.3 ± 1.9 (mean ± standard deviation [SD]) years. Subjects with an ongoing respiratory infection or who were taking any medication known to affect muscle activity were excluded from the study. All of the subjects had complete dentition with the exception of the third molars. Each subject had a normal overjet and overbite. Informed consent was obtained from each subject before the study. Methods Pressure from the tongue on the lingual surface of the lower anterior teeth was measured with a pressure sensor (PS-A type, Kyowa Co., Tokyo, Japan) incorporated in a lingual flange of a custom-made intraoral appliance (Fig 1) made of silicon rubber impression paste (Exafine putty type, GC Co., Tokyo, Japan). Temperature effect on output of the transducer is 0.1%/°C. The thickness (ca 1 mm) of the appliance13,14 and the location of the transducers were carefully standardized. The sensitivity of the sensor was calibrated before and after each experimental session. The EMG activity of the right GG muscle was recorded monopolarly with a stainless steel fine-wire electrode inserted through the lingual sulcus following the method of Sauerland and Harper.8 A neutral electrode was placed on the right ear lobe. The wire elec- American Journal of Orthodontics and Dentofacial Orthopedics March 1999 Fig 2. A, Typical simultaneous recording of chest wall movement; B, GG EMG activity; C, integrated GG EMG activity; and D, tongue pressure on lingual surface of mandibular incisors in supine subject during oral breathing. Vertical bar represents 50 µV for raw GG EMG activity, and 5 g/cm2 for tongue pressure (insp, inspiration; exp, expiration). trodes were 0.03 mm in diameter and insulated with urethane. The tip of the electrode was bared approximately 2 mm. The EMG activity of the GG muscle was identified by (1) tonic burst activity during tongue protrusion and (2) rhythmic phasic activity coinciding with inspiration. Respiratory movement of the chest wall was simultaneously recorded by an inductance band (TR-751T, Nihon-Kohden, Tokyo, Japan). Before each experimental session, EMG activities of the suprahyoid muscles and the anterior temporal muscle were recorded with surface electrodes; one subject who showed respiratory-related EMG activity in the anterior temporal muscle was excluded. If the respiratoryrelated EMG activity was found in the anterior temporal muscle, it would be considered that the jaw position is changed.15 Thus, the final study group consisted of nine subjects. Protocol The subjects sat in a reclining chair with a headrest in an upright position; they were instructed to remain awake with both eyes open. At least 5 minutes after setting up the intraoral appliance and electrodes, respiratory movement, tongue pressure, and GG EMG activity were recorded simultaneously over 20 respiratory cycles during quiet breathing through the nose with the mouth shut. Recordings were then repeated while the subject quietly breathed through the mouth with the nose completely occluded with a clip. The chair was Takahashi et al 241 American Journal of Orthodontics and Dentofacial Orthopedics Volume 115, Number 3 Fig 3. Temporal relationship between peak inspiratory effort (abscissa) and maximum tongue pressure (ordinate). Straight lines indicate regression lines along with equations for four subjects. then reclined, and the subject lay down in a supine position. After at least 5 minutes, the protocol was repeated. EMG signals were amplified and band-pass filtered at 30 Hz to 1 kHz. After conversion of the signals through an A/D converter (Maclab/8S, ADinstruments, Castle Hill, Australia), they were stored in a personal computer (Macintosh Performa 5270, Apple Computer, Cupertino, Calif) for data analysis. Signals from the pressure sensor were amplified with preadjusted and calibrated gains and stored in the same manner as EMG signals. Data Analysis Time lags (Fig 2) between the maximum tongue pressure and the peak inspiratory effort were measured and plotted for five consecutive respiratory phases that were randomly selected in four subjects while they were breathing through the mouth in the supine position. We tested correlation between the timing of the peak inspiratory effort and that of maximum tongue pressure with a linear regression analysis in four subjects randomly selected from nine subjects. In each subject, five respiratory phases were randomly selected during breathing through the mouth and nose in both the upright and supine positions. The maximum values of tongue pressure were measured and averaged. GG EMG signals that had been stored in the personal computer in selected phases were integrated Fig 4. Comparisons of maximum tongue pressure among different breathing modes and body positions. (UPNB, nasal breathing in the upright position; UPOB, oral breathing in the upright position; SUPNB, nasal breathing in the supine position; SUPOB, oral breathing in the supine position; **P < .01) with a time constant of 200 ms; the maximum and minimum EMG amplitudes in each phase were measured and averaged. The average EMG amplitude in each subject was normalized to the mean expiratory EMG amplitude during nasal breathing in an upright position. A one-way repeated analysis of variance (ANOVA) and Contrasts were used to compare the maximum values of tongue pressure and GG EMG activity among the different breathing modes and body positions. RESULTS Inspiratory activation of the GG muscle was observed in five subjects during nasal and oral breathing in both the upright and supine positions. Fig 2 shows a typical simultaneous recording of chest wall movement, GG EMG activity, and tongue pressure on the lingual surface of the mandibular incisors in a subject during oral breathing in the supine position. Tongue pressure showed respiratory-related cyclic oscillation, with a maximum value during expiration and a minimum value during inspiration. On the other hand, GG EMG activity showed a maximum value during inspiration and a minimum value during expiration. This cyclic oscillation in tongue pressure was observed in all nine subjects. Fig 3 shows a strong correlation between the timing of the peak inspiratory effort and that of the maximum tongue pressure in all of the four subjects tested. Thus, the oscillation in tongue pressure is respiratory related. 242 Takahashi et al Fig 5. Comparisons of GG EMG activity during inspiration among different breathing modes and body positions. (UPNB, nasal breathing in the upright position; UPOB, oral breathing in the upright position; SUPNB, nasal breathing in the supine position; SUPOB, oral breathing in the supine position; *P < .05). Note: GG EMG activities were normalized to the expiratory GG EMG activity during nasal breathing in the upright position. In eight of the nine subjects, negative pressure was recorded during nasal breathing. These negative values were regarded as 0 g/cm2 for the data analysis, because the tip of the tongue does not touch the surface of the pressure sensor when negative pressure occurs. The maximum tongue pressure in different breathing modes and body positions is illustrated in Fig 4. Significant differences were found between nasal breathing in the upright position and both oral breathing in the upright position (P < .01) and oral breathing in the supine position (P < .01). Significant differences were also found between oral breathing in the upright and supine positions (P < .01) and between nasal and oral breathing in the supine position (P < .01). Thus, the maximum tongue pressure during oral breathing was significantly greater than that during nasal breathing in either body position. In addition, changes in body position had a significant effect on the maximum tongue pressure during oral breathing. GG EMG activity during inspiration in different breathing modes and body positions is illustrated in Fig 5. Significant differences were found between nasal breathing in the upright position and oral breathing in the supine position (P < .05), and between nasal and oral breathing in the supine position (P < .05). American Journal of Orthodontics and Dentofacial Orthopedics March 1999 Fig 6. Comparisons of GG EMG activity during expiration among different breathing modes and body positions. (UPNB, nasal breathing in the upright position; UPOB, oral breathing in the upright position; SUPNB, nasal breathing in the supine position; SUPOB, oral breathing in the supine position; *P < .05). Note: GG EMG activities were normalized to the expiratory GG EMG activity during nasal breathing in the upright position. GG EMG activity during expiration in different breathing modes and body positions is illustrated in Fig 6. Significant differences were found between nasal breathing in the upright position and oral breathing in the supine position (P < .05) and between nasal breathing in the upright and supine positions (P < .05). The reproducibility of maximum tongue pressure in different breathing modes and body positions was examined in three subjects on different days (Table I). The values during oral breathing consistently tended to be greater than those during nasal breathing in the upright position, whereas values during oral breathing were greater than those during nasal breathing in the supine position. DISCUSSION Method Considerations Although several researchers have emphasized the importance of intraoral pressure,10-14,16-23 tongue pressure has been studied less than pressure exerted by the lip and cheek. The tongue pressure on the lingual surface of the mandibular incisors in the present study ranged between 0.35 g/cm2 during nasal breathing in the upright position and 8.88 g/cm2 during oral breathing in the supine position. Proffit et al16 reported a tongue pressure of 5.9 g/cm2 on the mandibular incisors. However, they did not define the mandibular Takahashi et al 243 American Journal of Orthodontics and Dentofacial Orthopedics Volume 115, Number 3 Table I. Means and standard deviations of the maximum tongue pressure in three subjects on different days Nasal breathing Subject Upright Supine 1 2 3 1 2 3 Oral breathing Day l Day 2 Day l Day 2 0.00 ± 0.00 1.69 ± 0.47 1.73 ± 0.53 0.00 ± 0.00 0.00 ± 0.00 0.36 ± 0.73 0.00 ± 0.00 0.98 ± 0.54 1.72 ± 1.12 0.10 ± 0.23 0.00 ± 0.00 0.10 ± 0.14 4.83 ± 1.33 3.91 ± 0.51 2.91 ± 0.28 7.68 ± 0.53 6.48 ± 1.81 6.78 ± 0.33 5.36 ± 0.44 3.99 ± 1.22 3.26 ± 0.53 7.20 ± 1.77 6.85 ± 2.24 7.26 ± 0.53 Unit: g/cm2. position and their appliances that carried transducers were thicker than ours. The thickness of appliance has substantial effects on intraoral pressure measurement. Lear et al20 reported that even a 1.5 mm thickness of the transducer caused an appreciable increase in mean forces. Gould and Picton13,14 studied the distance between the surface of teeth and the pressure sensor, and they concluded that the distance should be less than 1 mm to measure correct pressure. The spatial relationship between the lingual surface of mandibular incisors and the pressure sensor that was incorporated in our appliance satisfied with their postulation. Fröhlich et al17 measured a tongue pressure of –0.1 g/cm2 on the mandibular incisors with a device based on an extraoral pressure transducer incorporated in a waterfilled system to neglect the inevitable effect of the thickness of the transducer. We also recorded negative pressures in the present study. However, because the pressure transducer in the present study cannot accurately measure negative pressure, absolute values were not completely comparable. Kato et al18 and other investigators20-23 discussed the effect of temperature on the intraoral pressure measured by strain gauges. Because the pressure sensor in the present study incorporates a strain gauge, it is possible that changes in temperature coinciding with respiration could affect the measurement of tongue pressure. Lear et al20 reported that temperature variations during speech were slight and their effects on the measurement were negligible. Temperature variations in the present study in which subjects breathed quietly would be less than theirs. If a change in temperature did occur, the temperature on the pressure sensor during expiration would be higher than that during inspiration because of the difference in temperature between the air in the lung and that in the experimental room.20 However, the pressure decreased during inspiration when the temperature on the surface of the pressure sensor increased. Therefore, we conclude that changes in temperature coinciding with respiration did not affect the measurement of tongue pressure in the present study. The Maximum Tongue Pressure We hypothesized that the tongue pressure on the lingual surface of the mandibular incisors would change coinciding with respiratory-related activity of the GG muscle. We also hypothesized that tongue pressure shows its maximum value during inspiration because GG EMG activity shows its maximum amplitude during inspiration. However, the timing of the peak GG EMG activity corresponded with the minimum tongue pressure rather than with the maximum value. This suggests that respiratory-related GG EMG activity does not have a substantial effect on tongue pressure. The GG muscle exhibits phasic inspiratory activity that is superimposed on a ubiquitous tonic activity. The physiologic function of enhanced GG EMG activity during inspiration is to maintain the efficiency of the upper airway against respiratoryrelated collapse. Nakagawa et al24 used cineradiography to demonstrate that the anterior wall of the upper airway and the hyoid bone were positioned posteriorly in the inspiratory phase during quiet nasal breathing. This indicates that the base of the tongue moves posteriorly because of negative intraluminal pressure during inspiration even though increased GG EMG activity would be expected to pull the tongue forward. Kobayashi et al25 used video x-ray fluoroscopy and found in laryngectomized subjects that forward movement of the tongue was observed concomitant with augmented GG EMG activity during inspiration. However, because laryngectomized subjects were evaluated in their study, changes in intraluminal pressure that might affect upper airway patency did not occur, indicating that the tongue base moved forward solely due to contraction of the GG muscle during inspiration. Thus, it is likely that posterior movement of the tongue base during inspiration is accompanied by posterior migration of the tongue tip, which subse- 244 Takahashi et al Fig 7. Speculative schematic illustration of factors that may affect tongue pressure during inspiration (A) and expiration (B) in the upright position. During inspiration, vector sum of negative intraluminal pressure (a) and phasic GG EMG activity (b) may induce posterior movement of the tongue accompanied by posterior migration of the tongue tip (c), resulting in a decrease in tongue pressure. In contrast, the vector sum of tonic expiratory GG EMG activity (b’) and positive intraluminal pressure (a’) may induce anterior movement of the tongue accompanied by anterior migration of the tongue tip (c’), resulting in an increase in tongue pressure. quently decreases tongue pressure on the lingual surface of the mandibular incisors (Fig 7A). There is less GG EMG activity during expiration than during inspiration, and the two values are almost equal in subjects who do not show phasic activity. However, intraluminal pressure is positive during expiration and negative during inspiration.26 This suggests that the tongue base is positioned more anteriorly during expiration than during inspiration by positive intraluminal pressure and GG EMG activity, resulting in an increased tongue pressure (Fig 7B). Altered Breathing Mode and Tongue Pressure We hypothesized that changes in GG EMG activity in association with changes in breathing mode would affect the maximum tongue pressure. Because tongue pressure shows its maximum value in the expiratory phase, GG EMG activity during expiration may be related to the maximum tongue pressure. However, significant differences in expiratory GG EMG activity were only found between nasal breathing in the upright position and oral breathing in the supine position, and between nasal breathing in the upright and supine positions in the present study (Fig 6). Likewise, Douglas et al4 demonstrated that the breathing mode had no significant effect on GG EMG activity during expiration. Thus, expiratory GG EMG activity by itself cannot explain the change in the maximum tongue pressure. Previous studies have dealt with the relationship between the breathing mode and the position of the hyoid bone. Meurice et al27 reported that opening of the mouth induced a reduction in the distance between American Journal of Orthodontics and Dentofacial Orthopedics March 1999 Fig 8. Speculative schematic illustration of factors that may affect tongue pressure during nasal breathing (A) and oral breathing (B) in the upright position, and during nasal breathing (C) and oral breathing (D) in the supine position. Contraction of the GG muscle (b1) may be involved in tongue pressure during nasal breathing in the upright position (A). In addition to contraction of the GG muscle (b2), anterior movement of the hyoid bone (h2) may occur during oral breathing in the upright position (B). The sum of b2 and h2 may be greater than b1. During nasal breathing in the supine position (C), contraction of the GG muscle (b4) and anterior movement of the hyoid bone (h4) may overcome gravity (G). The sum of b4 and h4 may be greater than the sum of b3 and h3. the mandibular plane and the hyoid bone even in the absence of oral airflow. Miller et al28 found that geniohyoid EMG activity increased during oral breathing in the rhesus monkey, but they did not study the change in the position of the hyoid bone. This augmented geniohyoid EMG activity28 would pull the hyoid bone anteriorly. Because the tongue is attached to the hyoid bone, forward movement of the hyoid bone would pull the tongue anteriorly en masse, leading to an increase in tongue pressure. As shown in Fig 8, we believe that changes in the position of the hyoid bone with changes in the breathing mode play an important role in determining the maximum tongue pressure. In the upright position, the tongue pressure during nasal breathing may be affected by expiratory GG activity. Tongue pressure during oral breathing may be affected by anterior movement of the tongue that accompanies forward movement of the hyoid bone (Fig 8A and B). Body Position and Tongue Pressure Douglas et al4 demonstrated that GG EMG activity during both inspiration and expiration in the supine Takahashi et al 245 American Journal of Orthodontics and Dentofacial Orthopedics Volume 115, Number 3 position was greater than that in the upright position. Although the breathing mode was not defined, Pae et al10 reported that tongue pressure on the mandibular incisors tended to be lower in the supine position than in the upright position despite a significant increase in tonic GG EMG activity. In the present study, expiratory GG EMG activity during nasal breathing significantly increased when the body position changed from upright to supine (Fig 6). In contrast, the tongue pressure during nasal breathing in the supine position was not significantly different from that in the upright position (Fig 4). On the other hand, the tongue pressure during oral breathing in the supine position was significantly greater than that in the upright position, although expiratory GG EMG activity during oral breathing was not significantly different in the upright and supine positions. Therefore it is not possible to explain the effect of changes in body position on tongue pressure by changes in GG EMG activity alone. Pae et al10 showed that tongue pressure tended to decrease with changes in body position from upright to supine. They suggested that the inferior movement of the tongue occurred as a result of gravity. On the other hand, Yildirim et al29 and Pae et al10,30 reported that the hyoid bone moved anteriorly when the body position changed from upright to supine. Moreover, Pae et al10 reported that suprahyoid EMG activity tended to increase when the subject moved from the upright to supine body position, indicating anterior movement of the hyoid bone. We speculate that changes in the position of the hyoid bone associated with changes in body position may be an important determinant of the maximum tongue pressure, as well as changes in the breathing mode (Fig 8C and D). Gravity would pull the tongue posteriorly with changes in body position from upright to supine. During nasal breathing, this posterior movement of the tongue by gravity may be counteracted by increased GG EMG activity and anterior movement of the hyoid bone, resulting in no significant changes in tongue pressure. During oral breathing in the supine position, posterior movement of the tongue because of gravity may be overcome by increased GG activity and anterior movement of the hyoid bone, resulting in a significant increase in tongue pressure. CLINICAL IMPLICATIONS During oral breathing, the subjects in the present study breathed through the mouth with the nose completely occluded with a clip. Warren et al31 reported that only 2 of 116 otolaryngologically symptomatic and dental patients were total mouth breathers. Thus, most so-called mouth breathers generally do not breathe entirely through the mouth. Therefore findings with respect to oral breathing in the present study do not necessarily account for mouth breathers in a clinical sense. In the present study, tongue pressure during oral breathing was significantly greater than that during nasal breathing. Moreover, tongue pressure during oral breathing in the supine position was significantly greater than that during nasal breathing. It has also been suggested that mouth breathers may compensate for nasal impairment by positioning the tongue forward.31,32 If so, tongue pressure would increase and lead to changes in dentofacial patterns in growing children. Tallgren and Solow33 reported that the position of the hyoid bone is strongly associated with facial morphology. Given that changes in tongue pressure are related to changes in the position of the hyoid bone, this would affect facial morphologic characteristics by means of neuromuscular compensations over the long term. We have not examined the effect of changes in the breathing mode and body position on tongue pressure in subjects with skeletal Class II and III malocclusions. We think, however, that the trend of the changes in tongue pressure associated with alterations in the breathing mode and body position would be the same in skeletal Class I subjects because similar fundamental changes in upper airway patency would occur regardless of skeletal patterns. Yoo et al34 reported that no significant differences were found in the tongue volume between skeletal Class I and III subjects, indicating that the tongue volume was invariable. Therefore differences in the size of oral cavity among different skeletal patterns may affect the maximum value of tongue pressure, although differences in the tongue volume between skeletal Class I and II subjects were unknown. Proffit16 has shown that the labial and lingual forces on the lower incisors are not equal. But the lower incisors are considered to be in a state of equilibrium, because it is probable that the lips provide a constant lingual force and the tongue offers more heavy force intermittently that prevents the teeth from moving lingually. It is not clear whether tongue pressure with respiratory-related oscillations accounts for positions of teeth. Further research on lip pressure is needed. CONCLUSIONS The present study investigated respiratory-related changes in tongue pressure on the lingual surface of the mandibular incisors and the relationships among tongue pressure, breathing mode, and body position. We demonstrated that (1) tongue pressure showed respiratory-related oscillations with a maximum value 246 Takahashi et al during expiration and a minimum value during inspiration, and (2) changes in the breathing mode and body position significantly affected tongue pressure. We are grateful to Dr. Yoshio Nakamura, Dr. Nobuo Katakura and Dr. Yoshiyuki Kato for their valuable suggestions. REFERENCES 1. Weinstein S, Haack DC, Lightle YM, Snyder BB, Attaway HE. On an equilibrium theory of tooth position. Angle Orthod 1963;33:1-26. 2. Lear CSC, Moorrees CFA. Buccolingual muscle force and dental arch form. Am J Orthod 1969;56:379-93. 3. Proffit WR. Equilibrium theory revisited: factors influencing position of teeth. Angle Orthod 1978;48:175-86. 4. Douglas NJ, Jan MA, Yildirim N, Warren PM, Drummond GB. Effect of posture and breathing route on genioglossal electromyogram activity in normal subjects and in patients with the sleep apnea/hypopnea syndrome. Am Rev Respir Dis 1993; 148:1341-5. 5. van Lunteren E, Strohl KP, Parker DM, Bruce EN, Van de Graaff WB, Cherniack NS. Phasic volume-related feedback on upper airway muscle activity. J Appl Physiol 1984;56:730-6. 6. Wiegand L, Zwillich CW, Wiegand D, White DP. Changes in upper airway muscle activation and ventilation during phasic REM sleep in normal men. J Appl Physiol 1991;71:488-97. 7. Basner RC, Simon PM, Schwartzstein RM, Weinberger SE, Weiss JW. Breathing route influences upper airway muscle activity in awake normal adults. J Appl Physiol 1989;66:1766-71. 8. Sauerland EK, Harper RM. The human tongue during sleep: electromyographic activity of the genioglossus muscle. Exp Neurol 1976;51:160-70. 9. Sauerland EK, Mitchell SP. Electromyographic activity of intrinsic and extrinsic muscles of the human tongue. Tex Rep Biol Med 1975;33:445-55. 10. Pae E, Lowe AA, Sasaki K, Price C, Tsuchiya M, Fleetham JA. A cephalometric and electromyographic study of upper airway structures in the upright and supine positions. Am J Orthod Dentofacial Orthop 1994;106:52-9. 11. Archer SY, Vig PS. Effects of head position on intraoral pressures in Class I and Class II adults. Am J Orthod 1985;87:311-8. 12. Hellsing E, L’Estrange P. Changes in lip pressure following extension and flexion of the head and at changed mode of breathing. Am J Orthod Dentfacial Orthop 1987;91:286-94. 13. Gould MSE, Picton DCA. A method of measuring forces acting on the teeth from the lips, cheeks and tongue. Br Dent J 1962;112:235-42. American Journal of Orthodontics and Dentofacial Orthopedics March 1999 14. Gould MSE, Picton DCA. An evaluation of a method of measuring forces exerted by the tongue on the teeth. Br Dent J 1963;114:175-80. 15. Hollowell DE, Suratt PM. Activation of masseter muscles with inspiratory resistance loading. J Appl Physiol 1989;67:270-5. 16. Proffit WR, McGlone RE, Barrett MJ. Lip and tongue pressure related to dental arch and oral cavity size in Australian aborigines. J Dent Res 1975;54:1161-72. 17. Fröhlich K, Thüer U, Ingervall B. Pressure from the tongue on the teeth in young adults. Angle Orthod 1990;61:17-24. 18. Kato Y, Kuroda T, Togawa T. Perioral force measurement by a radiotelemetry device. Am J Orthod Dentofacial Orthop 1989;95:410-4. 19. Proffit WR. Muscle pressures and tooth position: North American whites and Australian aborigines. Angle Orthod 1975;45:1-11. 20. Lear CSC, Catz J, Grossman RC, et al. Measurement of lateral muscle forces on the dental arches. Arch Oral Biol 1965;10:669-89. 21. Winders RV. Recent findings in myometric research. Angle Orthod 1962;32:38-43. 22. Kydd WL. Maximum forces exerted on the dentition by the perioral and lingual musculature. J Am Dent Assoc 1957;55:641-51. 23. Luffinguham JK. A technique for the measurement of soft tissue pressures acting upon teeth. Arch Oral Biol 1968;13:309-18. 24. Nakagawa F, Ono T, Ishiwata Y, Kuroda T. The morphological changes in the oropharynx in association with the respiratory phase [in Japanese]. J Jpn Orthod Soc 1996;55:337-44. 25. Kobayashi I, Rhymer PJ, Hughes WP, et al. Inspiratory coactivation of the genioglossus enlarges retroglossal space in laryngectomized humans. J Appl Physiol 1996;80:1595-604. 26. Leiter JC, Knuth SL, Bartlett D Jr. Dependence of pharyngeal resistance on genioglossal EMG activity, nasal resistance, and airflow. J Appl Physiol 1992;73:584-90. 27. Meurice J, Marc I, Carrier G, Series F. Effect of mouth opening on upper airway collapsibility in normal sleeping subjects. Am J Respir Crit Care Med 1996;153:431-3. 28. Miller AJ, Vargervik K, Chierici G. Experimentally induced neuromuscular changes during and after nasal airway obstruction. Am J Orthod 1984;85:385-92. 29. Yildirim N, Fitzpatrick MF, Whyte KF, Jalleh R, Wightman AJA, Douglas NJ. The effect of posture on upper airway dimensions in normal subjects and in patients with the sleep apnea/hypopnea syndrome. Am Rev Respir Dis 1991;144:845-7. 30. Pae E. A comparative study of the relationship between airway size, tongue activity, and body position. Master’s Thesis, Vancouver: University of British Columbia 1989. 31. Warren DW, Hairfield WM, Seaton D, Morr KE, Smith LR. The relationship between nasal airway size and nasal-oral breathing. Am J Orthod Dentofacial Orthop 1988;93:289-93. 32. Hinton VA, Warren DW, Hairfield WM. Upper airway pressures during breathing: a comparison of normal and nasally incompetent subjects with modeling studies. Am J Orthod 1986;89:492-8. 33. Tallgren A, Solow B. Hyoid bone position, facial morphology and head posture in adults. Eur J Orthod 1987;9:1-8. 34. Yoo E, Murakami S, Takada K, et al. Tongue volume in human female adults with mandibular prognathism. J Dent Res 1996;75:1957-62.