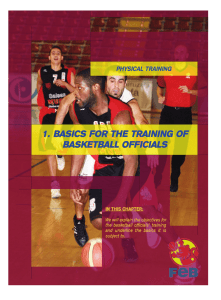
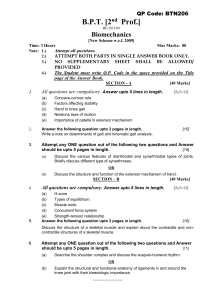
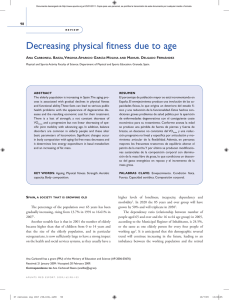
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/323192054 Impact of blood flow-restricted bodyweight exercise on skeletal muscle adaptations Article in Clinical Physiology and Functional Imaging · February 2018 DOI: 10.1111/cpf.12509 CITATIONS READS 22 648 7 authors, including: Jesper Emil Jakobsgaard Peter Sieljacks Aarhus University Aarhus University 6 PUBLICATIONS 71 CITATIONS 15 PUBLICATIONS 275 CITATIONS SEE PROFILE SEE PROFILE Jakob Wang Thomas s. Groennebaek Aarhus University Aarhus University 3 PUBLICATIONS 52 CITATIONS 11 PUBLICATIONS 169 CITATIONS SEE PROFILE Some of the authors of this publication are also working on these related projects: Muscle mechanotransduction View project Conditioning-Based Intervention Strategies View project All content following this page was uploaded by Kristian Vissing on 12 April 2019. The user has requested enhancement of the downloaded file. SEE PROFILE Clin Physiol Funct Imaging (2018) 38, pp965–975 doi: 10.1111/cpf.12509 Impact of blood flow-restricted bodyweight exercise on skeletal muscle adaptations J. E. Jakobsgaard1 1 , M. Christiansen1, P. Sieljacks1, J. Wang1, T. Groennebaek1, F. de Paoli2 and K. Vissing1 Section for Sport Science, Department of Public Health, and 2Department of Biomedicine, Aarhus University, Aarhus, Denmark Summary Correspondence Kristian Vissing, Section for Sport Science, Department of Public Health, Aarhus University, Dalgas Avenue, 4 DK-8000, Aarhus C, Denmark E-mail: [email protected] Accepted for publication Received 6 December 2017; accepted 16 January 2018 Key words angiogenesis; blood flow occlusion; low-intensity resistance training; muscle metabolism; strength training This study ascertains the ability of bodyweight blood flow-restricted (BFR) exercise training to promote skeletal muscle adaptations of significance for muscle accretion and metabolism. Six healthy young individuals (three males and three females) performed six weeks of bodyweight BFR training. Each session consisted of five sets of sit-to-stand BFR exercise to volitional failure with 30-second interset recovery. Prior to, and at least 72 h after training, muscle biopsies were taken from m. vastus lateralis to assess changes in fibre type-specific cross-sectional area (CSA), satellite cell (SC) and myonuclei content and capillarization, as well as mitochondrial protein expression. Furthermore, magnetic resonance imaging was used to assess changes in whole thigh muscle CSA. Finally, isometric knee extensor muscle strength was evaluated. An increase in knee extensor whole muscle CSA was observed at middle and distal localizations after training (32% and 35%, respectively) (P<005), and a trend was observed towards an increase in type I fibre CSA, whereas muscle strength did not increase. Additionally, the number of SCs and myonuclei associated with type I fibres increased by 657% and 20%, respectively (P<005). No significant changes were observed in measures of muscle capillarization and mitochondrial proteins. In conclusion, six weeks of bodyweight-based BFR exercise promoted myocellular adaptations related to muscle accretion, but not metabolic properties. Moreover, the study revealed that an appropriate total training volume needs further investigation before recommending bodyweight BFR to patient populations. Introduction Efficient strategies towards counteracting muscle wasting and/ or promoting muscle accretion are potentially desirable in many clinical settings. Such settings may include individuals recovering from acute incidents (such as stroke or surgery), chronic inflammatory diseases (such as rheumatoid arthritis) and/or increased age (Evans, 2010; Cohen et al., 2015). Resistance exercise has been extensively proven to constitute an effective mean in promoting muscle myofibrillar protein accretion and muscle hypertrophy (Folland & Williams, 2007). In this regard, high-intensity resistance exercise (HRE) (i.e. ≥70% of 1 repetition maximum) is traditionally recommended as the optimal approach (American College of Sports Medicine, 2009). However, utilization of high mechanical loads may not be readily applicable in some of the abovementioned clinical settings. It is therefore interesting that lowintensity resistance exercise (LRE), with and without simultaneous blood flow restriction (BFRE), has been shown effective in promoting muscle hypertrophy and gains in muscle strength when performed to volitional failure (Scott et al., 2014; Fahs et al., 2015). Furthermore, BFRE has been proposed as an effective, yet mechanically gentle strategy to promote muscle accretion (Scott et al., 2014), as it requires substantially less work performed compared to free-flow LRE (Farup et al., 2015b). This efficiency of BFRE has been suggested to partly rely on an accelerated proliferation of myogenic stem cells (satellite cells, SC) and subsequent addition of myonuclei (Nielsen et al., 2012). In accordance, maintenance or expansion of the myocellular SC pool may be of importance for counteracting muscle wasting (Pallafacchina et al., 2013). Importantly, improvements of muscle function do not exclusively rely on accretion of myofibrillar proteins, as proteins related to muscle metabolic properties also contribute to attainment of such improvements. In accordance, the impact of HRE on metabolic muscle adaptations has received relatively less attention (Groennebaek & Vissing, 2017). Yet, recent studies suggest that HRE can stimulate mitochondrial protein synthesis (Wilkinson et al., 2008) and © 2018 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 38, 6, 965–975 965 966 Bodyweight blood flow-restricted exercise, J. E. Jakobsgaard et al. mitochondrial respiration (Pesta et al., 2011; Porter et al., 2015). Consequently, it can be assumed that even intermittent alterations in muscle oxygen availability and/or myocellular homoeostasis with HRE can drive muscle mitochondrial biogenesis. In this regard, Burd et al. (2012) observed increased mitochondrial protein synthesis after single-bout LRE performed to volitional fatigue, which can be presumed to accentuate the magnitude of metabolic stress compared to HRE. In accordance, as BFRE entail both low intensity and more pronounced ischaemia (Downs et al., 2014), it can be speculated that BFRE conducted to a state of fatique possess substantial ability to stimulate mitochondrial biogenesis. This contention is supported by observations that BFRE can improve muscular endurance capacity (Kacin & Strazar, 2011). Moreover, such adaptations may be partly reliant on alterations in the capacity of peripheral blood flow and oxygen delivery to the trained muscle through increased angiogenesis (Takarada et al., 2002; Evans et al., 2010; Kacin & Strazar, 2011), with vascular endothelial growth factor (VEGF) proposed to play a central role in exercise-induced angiogenesis (Hoier & Hellsten, 2014). Previous BFRE strategies have predominantly involved isolated exercises such as knee extensions, knee flexions and leg press (Loenneke et al., 2012), which require the use of sophisticated training equipment. However, from a socioeconomic and safety point of view, it would entail perspective if bodyweight-based BFRE could be successfully practiced at home during patient rehabilitation. However, as the effects of bodyweight BFRE have not been thoroughly investigated, the purpose of this study was therefore to explore the feasibility of this approach in healthy individuals. More specifically, we aimed to investigate the skeletal muscle adaptational effects of bodyweight BFR training, using a simple sit-to-stand exercise model. Our hypothesis was that prolonged bodyweight BFRE is capable of driving adaptations of importance for muscle metabolic as well as muscle contractile properties. Materials and methods Participants Six healthy young subjects were included in the study [male n = 3, female n = 3; age 258 years (242; 275); height 174 cm (173; 176); body mass 734 kg (701; 767)] (values are means and 95% confidence intervals). None of the subjects had participated in resistance-type training for a minimum of 6 months prior to enrolment in the study. All included female participants were using oral contraceptives during the intervention period. Each participant was informed of the risks associated with the study, and a written informed consent was obtained from each subject prior to participation. The study was performed in accordance with the Declaration of Helsinki and approved by The Central Denmark Region Committees on Health Research Ethics (j. no. 49769). Study design In total, the duration of the study was 8 weeks. Prior to, and following the 6 weeks of training, the subjects underwent a one-week testing protocol designed to evaluate changes in exercise capacity and in morphological and myocellular properties. The training period consisted of total 19 sessions with an average of three weekly sessions dispersed over a six-week period with at least 24-48 h of recovery between exercise sessions (i.e. progression from two to four sessions per week). Biopsies were taken from m. vastus lateralis 1 week prior to the first training session and at least 72 h after the last training session. Whole muscle CSA was measured by magnetic resonance imaging (MRI). Strength tests consisted of maximal unilateral isometric knee extensor contractions performed on a dynamometer. Biopsies, MRI and strength tests were performed on three separate days in the stated order both preand postintervention, to prevent interference of the strength test with morphological and myocellular measures. Training protocol Each exercise session began with a 5 minute light-moderate intensity warm-up on a stationary bike ergometer (Monark Ergomedic 818E, Monark, Varberg, Sweden). Following the warm up, a curved 10-cm-wide tourniquet cuff (VBM Medizintechnik, GmbH, Germany) was wrapped around the proximal most portion of the thigh on each subject. The cuffs were then inflated by a digital tourniquet system with automatic regulation of pressure (Digital Tourniquet 9000, VBM, Medizintechnik, GmbH, Germany). Each exercise session was supervised and consisted of five sets of sit-to-stand BFR exercise with repetitions to voluntary failure and 30 s of inter-set recovery. The sit-to-stand exercise was performed by squatting down to a chair and standing up again. The subjects were instructed to keep their chest high, back straight and to control the pace of the movement. The chair was simply used as a marker of depth and safety precaution, making the subjects only lightly touching the chair before commencing the upward movement of the exercise. The height of the chair was individually set by placing plates under the feet of the participants, securing a 90-degree movement of the knee joint for all subjects. A metronome was set to 60 beats per minute, and the subjects were instructed to perform each repetition in a four-second duty cycle, making the downward and upward phases last 2 s each. A set was finished when a subject could not voluntarily initiate upward movement of another repetition. During the first training sessions, the cuffs were inflated to a cuff pressure of 100 mmHg (Nielsen et al., 2012; Farup et al., 2015b). However, as this cuff pressure entailed a high number of repetitions, it was seemingly not able to sufficiently reduce arterial occlusion pressure (AOP) in an upright body position (see Discussion). Therefore, during later training sessions (session 11–19), a higher pressure of 180 mmHg © 2018 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 38, 6, 965–975 Bodyweight blood flow-restricted exercise, J. E. Jakobsgaard et al. 967 was applied in the first 2 sets, whereupon it was lowered to 150 mmHg for remaining three sets. sections (2/3) of the femur length, defined from the top of caput femoris to the knee joint line. Determinations of isometric muscle strength Muscle biopsy Isometric muscle strength of the knee extensors was evaluated using an isokinetic dynamometer (Humac Norm, CSMI, Stoughton, USA). Prior to testing, the same warm-up routine as mentioned above, was performed. Subjects then seated in the dynamometer with 90-degree of hip flexion and restraining straps placed around the torso and hips. The axis of rotation of the knee joint was aligned with the axis of rotation of the lever arm. The lever arm was attached to the subject’s leg about 3 cm proximal to the medial malleolus. The dominant leg was used in all strength tests. With a fully extended knee joint being equal to 0° of flexion, isometric maximal voluntary contraction (MVC) was measured at 30°and 70° of flexion. The subjects were instructed on how to avoid countermovement actions and to contract as fast and forcefully as possible. Subjects were given four trials, interspaced by at least 1 min of recovery. However, if a subject continued to approve, additional attempts were allowed. Verbal and visual encouragement was given during all tests. Torque data were recorded at 200 Hz, and the highest peak torque of the four attempts was used for further analysis. Muscle biopsies were obtained before and after the training period from the middle section of the vastus lateralis muscle on the dominant leg, using the Bergstr€ om needle technique (Bergstrom, 1975) and a part of the sample was then treated for immunohistochemistry, as previously described (Farup et al., 2015a). The rest of the sample was immediately frozen in a bath of liquid nitrogen. Samples were then stored at 80°C until further analysis. Magnetic resonance imaging protocol Whole muscle CSA was determined from the non-dominant leg of the subjects using images obtained via a 3 T magnetic resonance imaging (MRI) scanner (Siemens Skyra, Erlangen, Germany). The non-dominant leg was chosen to ensure that no influence from other tests affected the CSA. The subject was placed in supine position and transported feet first into the scanner. Two 18-element anterior coils were placed over the thighs of the subject. A frontal and sagittal localizer scan was made to localize the knee joint line. Two consecutive transversal multi-slice fast-spin-echo Dixon scans consisting of 30 slices each with a width of 3 mm distanced 7 mm between slices were made to ensure CSAs of the full length of the thighs. Parameters were the following: Field of view = 450 9 267 mm; acquisition matrix = 384 9 182; TR = 979 ms; TE = 100 ms; echo-train-length = 5: pixel bandwidth = 305 Hz/pixel; and number of averages = 1. The CSA was measured using a custom software program (Siswin, v09). Three muscle compartments were defined: (i) the knee extensor compartments (mm. vastus lateralis, vastus medialis, vastus intermedius and rectus femoris); (ii) the knee flexor compartment (mm. semitendinosus, semimembranosus, sartorius and biceps femoris-caput longum and caput breve); and (iii) the hip adductor compartment (mm. adductor magnus, adductor longus and gracilis). Whole muscle CSA of the knee extensor muscle compartment was obtained from slices corresponding to the proximal (1/3), middle (1/2) and distal Immunohistochemistry Satellite cell and myonuclei analysis The preparation of biopsies for immunohistochemestry were performed by readjusting the samples to 18°C in a cryostat (Leica CM-3050-S, Leica Biosystems Nussloch GmbH, Nusslock, Germany). Then, serial cross sections of 10 lm thickness were cut and subsequently placed on microscope glass slides (Thermo Scientific, Menzel-Gl€azer, Superfrost Ultra Plus). Muscle biopsy sections were fixed in Histofix (Histolab, Gothenborg, Sweden) for 4 min and subsequently blocked for 15 h in blocking buffer (2% BSA, 5% FBS, 2% goat serum, 02% Triton x-100, 01% sodium azide). The sections were then incubated overnight at 4°C in Pax7 primary antibody (1:500; cat. # MO15020, Neuromics, Edina, MN) followed by incubation in secondary Alexa flour 568 goat anti-mouse antibody (1:200; cat. # A11034, Invitrogen A/S, Taastrup) for 15 h. Afterwards, sections were incubated in appropriate antibodies for MHC-I (cat. # A4951, Developmental Studies Hybridoma Bank) and Laminin (cat. # Z0097, Dako Norden) both in 1:500 for 2 h and secondary antibodies Alexa-Fluor 488 goat anti-mouse green and Alexa-Fluor 488 goat anti-rabbit green (cat. # A11031 and A11034, Invitrogen A/S, Taastrup, Denmark) both in 1:500 for 1 h. Finally, a mounting media containing 40 ,60 diamidino-2-phenylindole (DAPI) was utilized to visualize nuclei (Molecular Probes Prolog Gold anti-fade reagent, cat. # P36935, Invitrogen A/S, Taastrup, Denmark). The stained sections were stored at 20°C until further analysis. All antibodies where diluted in 1% BSA. SCs were characterized by co-localization of Pax7 and DAPI within the SC-niche between the basal lamina and the sarcolemma of distinct muscle fibres. Only Pax7/DAPI+ nuclei with a geometric centre within the basal lamina was considered myonuclei (Fig. 1). SCs and myonuclei were quantified in a fibre type-specific manner, dependent on association to type I (A4951+) or type II (A4951) and normalized to respective number of fibres counted. Finally, myonuclear content was expressed relative to fibre type-specific CSA as a measure of myonuclear domain. © 2018 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 38, 6, 965–975 968 Bodyweight blood flow-restricted exercise, J. E. Jakobsgaard et al. Figure 1 Immunohistochemistry staining. A representative image of the immunohistochemistry staining on muscle cross sections for Pax7 (red), MHC-I (green) and DAPI (blue). Lower right corner displays a magnified panel with the arrows specifying two identified Pax7+ nuclei (SCs) associated with type I fibres. [Colour figure can be viewed at wileyonlinelibrary.com] All images were obtained at 209 magnification with fluorescents microscope with a Leica DFC450 camera attachment utilizing Leica Application Suite and subsequently analysed using ImageJ software (v. 149). To ensure reliable numbers of SCs and myonuclei, a mean of 145 [130; 160] and 93 [86; 100] fibres for each subject at each time point were assessed, respectively (mean and 95% confidence interval). area and capillarization quantification, a mean number of 395 fibres [382; 408] for each subject at each time point was analysed. The same blinded investigator conducted the quantification of SC’s and myonuclei content as well as CSA and capillaries to ensure a uniform procedure. Fibres situated on the edge of the cross sections as well as fibres characterized by poor morphological integrity where excluded from quantification. Fibre area and capillarization With regard to fibre CSA and capillary analysis, biopsies were prepared as initially described above. After the initial blocking, the sections were incubated overnight at 4°C in primary antibody for MHC-I (1:1000; cat. # A4951, Developmental Studies Hybridoma Bank). Subsequently, sections were incubated with Alexa-fluor 568 goat anti-mouse red (1:500; Molecular Probes, cat. no A11001, Invitrogen A/S, Taastrup, Denmark) and Alexa-fluor 488 mouse-anti-Human Collagen IV green secondary antibodies (1:100; cat. # 53-9871, Affymetrix, CA, US). Finally, a cover slip was applied onto the glass slides using a mounting medium not containing DAPI (Molecular Probes Gold anti-fade reagent, cat # P36930, Invitrogen A/S). Samples were stored at 20°C until further analysis. All antibodies where diluted in 1% BSA. Images were captured at 910 magnification with a Leica fluorescent microscope, and analysis was carried out using Leica QWin software (v. 351). Fibre CSA for two major fibre types were assessed and expressed as mean values relative to both type I and type II fibres, separately. The capillaries around each fibre were assessed both relative to total number of fibres counted and in a fibre type-specific manner. Furthermore, the total number of capillaries was expressed relative to fibre type CSA as a measure of capillary density. For fibre type Immunoblotting Preparation of muscle lysates and determination of protein concentration was conducted as previously described (Rahbek et al., 2015). Equal amounts of protein were separated by SDSPAGE on precast Stain-Free 4%–15% gels (Bio-Rad, CA, USA) running for approximately 45 min at 160 V. Proteins were then electro-blotted onto PVDF membranes (Bio-Rad, CA, USA) using a Trans-Blot Turbo system (Bio-Rad, CA, USA). Control for equal loading was performed using the Stain-Free technology as previously described (Gilda & Gomes, 2013; Gurtler et al., 2013). Membranes were then blocked for 2 h in 01% I-block (Applied Biosystems, CA, USA) diluted in TBST and incubated overnight with the respective primary antibodies. The following primary antibody was purchased from Cell Signaling Technology (Danvers, MA, USA) and utilized as follows: COXIV (cat. # 4844, rabbit polyclonal, conc. 1:1000 in 5% skim milk). The following primary antibodies were purchased from ABCAM (Cambridge, UK) and utilized as follows: CPT1B (cat. # AB134135, rabbit monoclonal, conc. 1:1000 in 5% BSA), Citrate Synthase (cat. # AB96600, rabbit polyclonal, conc. 1:1000 in 5% BSA), VEGF-A (cat. # AB46154, rabbit polyclonal, conc. 1:500 in 5% BSA), b-HAD (cat. # AB81492, rabbit polyclonal, conc. 1:1000 in 5% BSA). With regard to © 2018 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 38, 6, 965–975 Bodyweight blood flow-restricted exercise, J. E. Jakobsgaard et al. 969 secondary antibodies, membranes were then incubated 1 h with Horseradish peroxidase-conjugated goat anti-rabbit (cat. # 2054, Santa Cruz, TX, USA) conc. 1:5000 in 1% BSA. All antibodies were diluted in TBST. Proteins were visualized by chemiluminiscence (Thermo Scientific, MA, USA) and quantified with UVP VisionWorks LS software (UVP, CA, USA). Precision Plus Protein All Blue standards were used as markers of molecular weight (Bio-Rad, CA, USA). Arbitrary intensity data of each target were normalized to total protein obtained from the Stain-Free blotting technology (Gurtler et al., 2013). Statistical analysis Differences from pre- to post-intervention in repetitions, muscle strength, knee extensor whole muscle CSA, protein expression, capillary, myonuclei and SC were determined using a paired t-test. With regard to analysis of protein expression, arbitrary intensity data of each target were normalized to total protein obtained from the Stain-Free blotting technology (Gurtler et al., 2013) before being log-transformed to reach normal distribution prior to analysis. Statistical analysis was performed using SigmaPlot (v120, Systat Software, San Jose, CA). Alpha level was set to P≤005. Results Training progression All six subjects completed all training sessions. Fig. 2 shows total repetitions during the first and last training session in each period (i.e. session 1–10 and sessions 11–19 with 100 mmHg and 180 mmHg of applied cuff pressure, respectively). An increase of 119 [41; 197] and 80 [6; 155] in the total number of performed repetitions was observed from the first to the last training session for the 100 mmHg and 180 mmHg periods, respectively (P<005). Muscle growth and strength An increase in knee extensor whole muscle CSA was observed after training, at both the middle (+24 cm2 [13 cm2; 35 cm2]) and distal (+25 cm2 [11 cm2; 38 cm2]) sections, corresponding to increases of 32% and 35%, respectively (P<001). No changes were observed at the proximal section (Fig. 3a). Also, no changes in whole muscle CSA of the adductor and flexor muscle groups were observed at any of the measured localizations (not presented). With regard to muscle fibre area, no changes were observed from pre- to post-intervention of either type I or type II muscle fibres (Fig. 3b). No changes in isometric knee extensor strength were observed at either joint angle (Fig. 3c). SCs and myonuclei We observed an increase of 004 [000; 008] in SCs per type I fibre from pre- to postintervention, corresponding to an increase of 657% (P<005) (Fig. 4a). No changes in SC per type II fibre were observed. With regard to myonuclei, an increase of 032 [001; 063] in mean number of myonuclei associated with type I muscle fibres was observed from pre to post, corresponding to an increase of 20% (P<005). No changes for myonuclei associated with type II fibres were observed (Fig. 4c). A decrease of 361 lm [699 lm; 23 lm] (107%) in myonuclear domain for type I fibres was also observed (P<005), with no changes for type II fibre myonuclear domain (Fig. 4d). Angiogenesis No changes were observed in capillary density or in number of capillaries per fibre ratio (Fig. 5). Metabolic proteins and VEGF-A Western blots are shown in Fig. 6a. No changes were observed with training in protein content for any of the protein targets (Fig. 6b). Discussion Figure 2 Total repetitions as training progression. Total repetitions performed in the first and last training session in each period (100 mmHg and 180 mmHg, respectively). Data are presented as mean SEM. *Denotes a difference between the first and last session with same pressure (P<005). The purpose of the current study was to investigate a potential dual effect of 6 weeks of bodyweight-conducted BFRE on adaptations of significance for skeletal muscle contractile and metabolic properties. The study population comprised healthy young individuals as a model to provide a preliminary investigatory platform for future studies on how to counteract decay in muscle health in populations experiencing skeletal muscle loss. The main finding of the current study was that our approach was capable of promoting phenotype-specific adaptations related to muscle growth, with type I fibres exhibiting the more pronounced adaptations. Contrary, little effect was © 2018 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 38, 6, 965–975 970 Bodyweight blood flow-restricted exercise, J. E. Jakobsgaard et al. Figure 3 Muscle growth and maximal isometric strength. Mean SEM (bars) and individual changes (lines) in knee extensor whole muscle CSA as measured by MRI (a), and mean SEM and individual changes of fibre type-specific area as determined by immunohistochemistry (b). Maximal isometric knee extensor muscle strength measured at 30° and 70° knee flexion pre- and postsix weeks of bodyweight sit-to-stand exercise under BFR (c). Values are presented as mean SEM (bars) and individual changes (lines). **Denotes a change from pre to post (P<.01). observed on adaptations related to skeletal muscle metabolism. Additionally, our study simultaneously advances some questions on how a bodyweight BFRE protocol should be designed to minimize the work volume required to produce such muscle adaptations. Impact of bodyweight BFRE on muscle protein accretion and strength The training protocol provoked a significant increase in whole muscle knee extensor CSA measured at the middle and distal locations (32% and 35%, respectively), with no changes observed at the proximal portion. Such increases in whole muscle CSA of the knee extensors are within range of what has previously been observed after single-joint BFRE exercises in studies using comparable magnitude of training (Wernbom et al., 2008). A lack of, or impaired growth in whole muscle knee extensor CSA at the proximal portion of the femur, has previously been observed by Kacin & Strazar (2011) and Ellefsen et al. (2015) after knee extensor BFRE. This prompts speculations on whether the external pressure of the cuff itself may somehow negate localized muscle growth in the proximity of the cuff. Furthermore, the lack of muscle hypertrophy in knee flexor and hip adductor compartments indicates that the work load was primarily imposed on the knee extensor compartment, which immediately question if the occlusion was equally restricting blood flow to the different muscle compartments and/or if the BFRE sit-to-stand exercise alone is sufficient to affect thigh flexor and adductor compartments. On muscle fibre level, no significant changes in CSA were observed, although a non-significant ~85% mean increase in type I fibre area was observed, with four of the subjects displaying even more pronounced increases in type I fibre CSA. The observed magnitude of discrepancy between changes in whole muscle CSA and fibre CSA is similar to previous observations (Aagaard et al., 2001; Farup et al., 2012), thus supporting that the observed increase type I fibre CSA is indeed valid. The increases in CSA likely resemble true increases in muscle myofibrillar protein accretion, as water retention has previously been observed to return to baseline within few hours after BFRE (Farup et al., 2015b). Given the volume of lowintensity work in the present model, the muscle fibre © 2018 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 38, 6, 965–975 Bodyweight blood flow-restricted exercise, J. E. Jakobsgaard et al. 971 Figure 4 Satellite cells (SC) and myonuclei. Mean number of SC per fibre type is presented as mean SEM (a) and individual data (b). Mean number of myonuclei per fibre type is presented as mean SEM (bars) and individual changes (lines) (c). Measures of myonuclear domain (fibre area per myonuclei) are presented as mean SEM and individual changes (d). *Denotes a change from pre to post (P<005). Figure 5 Angiogenesis. Measures of capillary density represented as mean SEM (bars) and individual changes (lines). Mean number of capillaries per fibre ratio is presented as mean SEM and individual changes (b). recruitment may have relied greatly on type I fibres, providing a feasible explanation for a hypertrophic response in this fibre type. Furthermore, the finding of a clear increase in the number of myonuclei supports that type I fibre hypertrophy did indeed occur. Accordingly, one possible explanation for increased myonuclear number relates to a myocellular necessity to increase transcriptional capacity to maintain a finite protein turnover of a given fibre size (Petrella et al., 2008). Alternatively, increased myonuclear numbers may relate to regenerative processes in response to exerciseinduced muscle micro-damage (Paulsen et al., 2012). In accordance, the fact that we also observe an increase in SCs in type © 2018 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 38, 6, 965–975 972 Bodyweight blood flow-restricted exercise, J. E. Jakobsgaard et al. Figure 6 Immunoblotting results. Blots of all protein targets for all subjects (n = 6) from muscle biopsies obtained before and after training (a). All blots for one target was performed on the same gel. Changes in protein expression of muscle metabolic proteins and VEGF-A are presented as individual and mean fold changes SEM from pre- to post-training (b). CS, citrate synthase; b-HAD, 3-hydroxyacyl-CoA dehydrogenase; COXIV, cytochrome C oxidase subunit IV; CPT1B, carnitine palmitoyltransferase 1B; VEGF-A, vascular endothelial growth factor A. I fibres could reflect ongoing regenerative processes due to the volume of work these fibres were exposed to. Interestingly, different subpools of SCs are believed to have different faiths (Yin et al., 2013), and it has been proposed that increases in myonuclear abundance through SC proliferation can precede substantial myofibre growth, resulting in a temporary decrease of the myonuclear domain (Gundersen, 2016), similar to what we observe in the current study. In this regard, although a previous study from our laboratory demonstrated that unaccustomed BFRE performed to volitional failure could produce muscle-damaging responses, these responses were attenuated upon repeated exposure single-bout BFRE, indicating that muscle damage is negligible in the trained state (Sieljacks et al., 2016). It may seem immediately puzzling that muscle growth was not accompanied by improvement in muscle strength. However, a lack of changes in isometric muscle strength despite muscle growth has previously been demonstrated after lowload BFR training (Kacin & Strazar, 2011), indicating that muscle growth and gains in muscular force capacity as a response to BFRE may not be closely related. Alternatively, the absence of muscle strength development in the early days after completion of BFR training has been suggested to relate to a delay in muscle strength development due to ongoing regenerative processes after BFR training (Nielsen et al., 2017). In accordance, Nielsen et al. observed no changes in slow velocity isokinetic knee extensor MVC 5 days after training, yet an increase to emerge 12 days after training. In this regard, it is important to notice that the training frequency of the Nielsen study comprised 23 sessions dispersed over as little as 19 days of training, which is very different to the three weekly sessions employed in our current study. Consequently, the ability and necessity of the muscle to recover/regenerate seem less influenced in the current study. On the other hand, it cannot be excluded that a different timing of strength testing in the current study would have improved our ability to identify a change. It therefore seems premature to adjudicate bodyweight-based BFRE as an insufficient stimulus to improve strength, especially in individuals with low baseline in muscle strength capacity. In this regard, it is noteworthy that bodyweight-conducted BFRE has been shown capable to promote increased isometric strength in elderly individuals (Yokokawa et al., 2008). Impact of bodyweight BFRE on muscle metabolic-related properties Skeletal muscle angiogenesis, as typically demonstrated by increases in capillary density and number of capillaries per © 2018 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 38, 6, 965–975 Bodyweight blood flow-restricted exercise, J. E. Jakobsgaard et al. 973 muscle fibre, is important to facilitate muscle oxygen and substrate availability and muscle metabolism inherent of aerobe endurance-type exercise (Hoier & Hellsten, 2014). Interestingly, resistance exercise has also been observed to stimulate angiogenesis, with the number of capillaries increasing in proportion to the hypertrophic response, while the capillary density is unaltered, thus maintaining diffusion capacity (McCall et al., 1996; Hoier & Hellsten, 2014; Holloway et al., 2017). Contraction-induced ischaemia inherent of resistance training may adhere to reduced tissue oxygenation (Downs et al., 2014), thus potentially imposing stimulation of angiogenesis through hypoxia-induced signalling pathways (Hoier & Hellsten, 2014). As ischaemia and reduced tissue oxygenation can be assumed to be enhanced with BFRE compared to traditional resistance exercise (Downs et al., 2014), BFRE can be assumed to promote angiogenesis. Yet, in the present study, we observed no changes in capillarization and VEGF-A protein content, but rather a trend towards a decrease in capillary density among type I fibres (P = 0064). Furthermore, we observed no changes in the expression of proteins involved in muscle mitochondrial metabolism. These results are immediately surprising, not least because our subjects displayed marked improvements in endurance capacity, as shown by the gradual increase in total work performed during the training period. To our knowledge, no previous study has examined the impact of BFRE on mitochondrial protein content or mitochondrial respiratory capacity. On the other hand, HRE has previously been reported to produce, concomitant increases in muscle fibre area and enzyme activity of mitochondrial enzymes (Tang et al., 2006). Furthermore, in a recent study by Porter et al. (2015), improvements in mitochondrial function, as measured by high-resolution respirometry (HRR), were observed after 12 weeks of HRE. Thus, the capability of BFRE to enhance muscle mitochondrial biogenesis deserves further investigation. Considerations on usefulness of bodyweight BFRE to counteract decay in skeletal muscle health in patient populations The motivation of the current study was to identify an effective, gentle (i.e., low load) and practical way to stimulate adaptations related to skeletal muscle growth and metabolism for populations experiencing loss of muscle mass. In accordance, BFRE strategies may entail a socioeconomic benefit, provided it can be self-conducted at home without sophisticated training apparatus or supervision. We considered that the feasibility of such an approach needed to first be addressed in young healthy individuals. Moreover, we were curious to see whether our strategy was indeed capable of inducing robust adaptations even in a rather small and heterogenic population, as this is often most expectedly a challenge to experience when conducting human studies on patient populations. By this deliberate approach, we made some interesting observations. In accordance, all the subjects completed all training sessions without experiencing adverse events. The study also serves to emphasize that efforts to control the training volume necessitate careful considerations on appropriate cuff pressure, to obtain an appropriate relative degree of occlusion and thereby reduce time to exhaustion. In accordance, the current, as well as most previous, studies on BFRE have employed absolute fixed cuff pressures close to 100 mmHg, while some other studies have used above even 200 mmHg (Scott et al., 2014). In consideration on potential discomfort associated with high cuff pressures in future studies on patient populations, we initiated the training with a cuff pressure 100 mmHg. However, due to the rapid progress in work volume, we later questioned whether cuff pressure was sufficiently high to uphold a sufficient relative degree of blood flow occlusion during an exercise such as the sit-to-stand exercise (i.e. multi-joint exercise, involving several muscles of the lower extremity). In accordance, it has been proposed that absolute cuff pressure should better consider the effects of gravity on regional blood pressure in upright compared to supine body positions (Sieljacks et al., 2017). Given small sample size and heterogeneity of the included subjects, the results should be interpreted with some caution. Oppositely, the stimulatory regime is robust enough to produce improvements in a setting that mimics the expected heterogenetic composition of individuals of a clinical population. In accordance, our findings of statistically verifiable increases in whole muscle CSA and myonuclei with training exhibited by similar directions of change in all subjects. In previous studies of our laboratory, we demonstrate that we are indeed experienced and capable in handling the implemented methods and analytic procedures (Farup et al., 2014a,b; Rahbek et al., 2014; Farup et al., 2015a; Larsen et al., 2014). In principle, it could be criticized that the current study did not implement a non-BFRE control group. However, whereas this should be implemented in future studies on a clinical populations, in the current study on healthy young individuals, the work volume would have been inappropriately high. In summary, bodyweight BFRE seems capable of promoting adaptations of significance for muscle contractile properties, whereas further investigation is needed on its potential for promoting adaptations of significance for metabolic properties. Acknowledgments Julie Moeslund and Freja Holm are thanked for their assistance with MRI analysis. Conflict of interest The authors have no conflicts of interest. © 2018 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 38, 6, 965–975 974 Bodyweight blood flow-restricted exercise, J. E. Jakobsgaard et al. References Aagaard P, Andersen JL, Dyhre-Poulsen P, et al. A mechanism for increased contractile strength of human pennate muscle in response to strength training: changes in muscle architecture. J Physiol (2001); 534: 613–623. American College of Sports Medicine. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc (2009); 41: 687–708. Bergstrom J. Percutaneous needle biopsy of skeletal muscle in physiological and clinical research. Scand J Clin Lab Invest (1975); 35: 609–616. Burd NA, Andrews RJ, West DW, et al. Muscle time under tension during resistance exercise stimulates differential muscle protein sub-fractional synthetic responses in men. J Physiol (2012); 590: 351–362. Cohen S, Nathan JA, Goldberg AL. Muscle wasting in disease: molecular mechanisms and promising therapies. Nat Rev Drug Discovery (2015); 14: 58–74. Downs ME, Hackney KJ, Martin D, et al. Acute vascular and cardiovascular responses to blood flow-restricted exercise. Med Sci Sports Exerc (2014); 46: 1489–1497. Ellefsen S, Hammarstrom D, Strand TA, et al. Blood flow-restricted strength training displays high functional and biological efficacy in women: a within-subject comparison with high-load strength training. Am J Physiol Regul Integr Comp Physiol (2015); 309: R767– R779. Evans WJ. Skeletal muscle loss: cachexia, sarcopenia, and inactivity. Am J Clin Nutr (2010); 91: 1123S–1127S. Evans C, Vance S, Brown M. Short-term resistance training with blood flow restriction enhances microvascular filtration capacity of human calf muscles. J Sports Sci (2010); 28: 999–1007. Fahs CA, Loenneke JP, Thiebaud RS, et al. Muscular adaptations to fatiguing exercise with and without blood flow restriction. Clin Physiol Funct Imaging (2015); 35: 167– 176. Farup J, Kjolhede T, Sorensen H, et al. Muscle morphological and strength adaptations to endurance vs. resistance training. J Strength Cond Res (2012); 26: 398–407. Farup J, Rahbek SK, Knudsen IS, et al. Whey protein supplementation accelerates satellite cell proliferation during recovery from eccentric exercise. Amino Acids (2014a); 46: 2503–2516. Farup J, Rahbek SK, Riis S, et al. Influence of exercise contraction mode and protein supplementation on human skeletal muscle satellite cell content and muscle fiber growth. J Appl Physiol (1985) (2014b); 117: 898–909. Farup J, De Lisio M, Rahbek SK, et al. Pericyte response to contraction mode-specific resistance exercise training in human skeletal muscle. J Appl Physiol (1985) (2015a); 119: 1053–1063. Farup J, de Paoli F, Bjerg K, et al. Blood flow restricted and traditional resistance training performed to fatigue produce equal muscle hypertrophy. Scand J Med Sci Sports (2015b); 25: 754–763. Folland JP, Williams AG. The adaptations to strength training: morphological and neurological contributions to increased strength. Sports Med (2007); 37: 145–168. Gilda JE, Gomes AV. Stain-Free total protein staining is a superior loading control to beta-actin for Western blots. Anal Biochem (2013); 440: 186–188. Groennebaek T, Vissing K. Impact of Resistance Training on Skeletal Muscle Mitochondrial Biogenesis, Content, and Function. Front Physiol (2017); 8: 713. Gundersen K. Muscle memory and a new cellular model for muscle atrophy and hypertrophy. J Exp Biol (2016); 219: 235– 242. Gurtler A, Kunz N, Gomolka M, et al. StainFree technology as a normalization tool in Western blot analysis. Anal Biochem (2013); 433: 105–111. Hoier B, Hellsten Y. Exercise-induced capillary growth in human skeletal muscle and the dynamics of VEGF. Microcirculation (2014); 21: 301–314. Holloway TM, Snijders T, van Kranenburg J, et al. Temporal Response of Angiogenesis and Hypertrophy to Resistance Training in Young Men. Med Sci Sports Exerc (2017); 50: 6–45. Kacin A, Strazar K. Frequent low-load ischemic resistance exercise to failure enhances muscle oxygen delivery and endurance capacity. Scand J Med Sci Sports (2011); 21: e231–e241. Larsen MS, Vissing K, Thams L, et al. Erythropoietin administration alone or in combination with endurance training affects neither skeletal muscle morphology nor angiogenesis in healthy young men. Exp Physiol (2014); 99: 1409–1420. Loenneke JP, Wilson JM, Marin PJ, et al. Low intensity blood flow restriction training: a meta-analysis. Eur J Appl Physiol (2012); 112: 1849–1859. McCall GE, Byrnes WC, Dickinson A, et al. Muscle fiber hypertrophy, hyperplasia, and capillary density in college men after resistance training. J Appl Physiol (1985). (1996); 81: 2004–2012. Nielsen JL, Aagaard P, Bech RD, et al. Proliferation of myogenic stem cells in human skeletal muscle in response to low-load resistance training with blood flow restriction. J Physiol (2012); 590: 4351–4361. Nielsen JL, Frandsen U, Prokhorova T, et al. Delayed Effect of Blood-Flow-Restricted Resistance Training on Rapid Force Capacity. Med Sci Sports Exerc (2017); 49: 1157– 1167. Pallafacchina G, Blaauw B, Schiaffino S. Role of satellite cells in muscle growth and maintenance of muscle mass. Nutr Metab Cardiovasc Dis (2013); 23(Suppl 1): S12– S18. Paulsen G, Mikkelsen UR, Raastad T, et al. Leucocytes, cytokines and satellite cells: what role do they play in muscle damage and regeneration following eccentric exercise? Exerc Immunol Rev (2012); 18: 42–97. Pesta D, Hoppel F, Macek C, et al. Similar qualitative and quantitative changes of mitochondrial respiration following strength and endurance training in normoxia and hypoxia in sedentary humans. Am J Physiol Regul Integr Comp Physiol (2011); 301: R1078– R1087. Petrella JK, Kim JS, Mayhew DL, et al. Potent myofiber hypertrophy during resistance training in humans is associated with satellite cell-mediated myonuclear addition: a cluster analysis. J Appl Physiol (1985) (2008); 104: 1736–1742. Porter C, Reidy PT, Bhattarai N, et al. Resistance Exercise Training Alters Mitochondrial Function in Human Skeletal Muscle. Med Sci Sports Exerc (2015); 47: 1922–1931. Rahbek SK, Farup J, Moller AB, et al. Effects of divergent resistance exercise contraction mode and dietary supplementation type on anabolic signalling, muscle protein synthesis and muscle hypertrophy. Amino Acids (2014); 46: 2377–2392. Rahbek SK, Farup J, de Paoli F, et al. No differential effects of divergent isocaloric supplements on signaling for muscle protein turnover during recovery from muscledamaging eccentric exercise. Amino Acids (2015); 47: 767–778. Scott BR, Loenneke JP, Slattery KM, et al. Exercise with Blood Flow Restriction: An Updated Evidence-Based Approach for Enhanced Muscular Development. Sports Med (2014); 45: 313–325. Sieljacks P, Matzon A, Wernbom M, et al. Muscle damage and repeated bout effect following blood flow restricted exercise. Eur J Appl Physiol (2016); 116: 513–525. © 2018 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 38, 6, 965–975 Bodyweight blood flow-restricted exercise, J. E. Jakobsgaard et al. 975 Sieljacks P, Knudsen L, Wernbom M, et al. Body position influences arterial occlusion pressure: implications for the standardization of pressure during blood flow restricted exercise. Eur J Appl Physiol (2017); 118: 303–312. Takarada Y, Sato Y, Ishii N. Effects of resistance exercise combined with vascular occlusion on muscle function in athletes. Eur J Appl Physiol (2002); 86: 308–314. Tang JE, Hartman JW, Phillips SM. Increased muscle oxidative potential following resistance training induced fibre hypertrophy in young men. Appl Physiol Nutr Metab (2006); 31: 495–501. Wernbom M, Augustsson J, Raastad T. Ischemic strength training: a low-load alternative to heavy resistance exercise? Scand J Med Sci Sports (2008); 18: 401–416. Wilkinson SB, Phillips SM, Atherton PJ, et al. Differential effects of resistance and endurance exercise in the fed state on signalling molecule phosphorylation and protein synthesis in human muscle. J Physiol (2008); 586: 3701–3717. Yin H, Price F, Rudnicki MA. Satellite cells and the muscle stem cell niche. Physiol Rev (2013); 93: 23–67. Yokokawa Y, Hongo M, Urayama H, et al. Effects of low-intensity resistance exercise with vascular occlusion on physical function in healthy elderly people. Biosci Trends (2008); 2: 117–123. © 2018 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 38, 6, 965–975 View publication stats