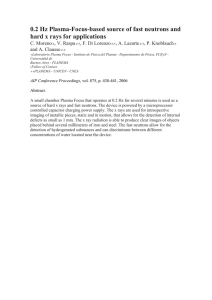
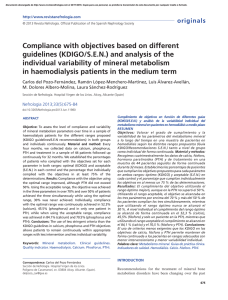
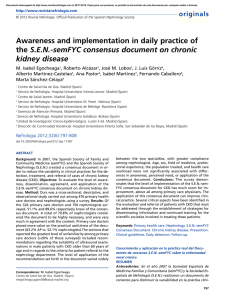
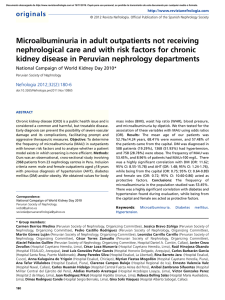
State of the Art Review Journal of Veterinary Emergency and Critical Care 23(2) 2013, pp 122–133 doi: 10.1111/vec.12032 The role of phosphorus in the pathophysiology of chronic kidney disease Rebecca F. Geddes, MA, VetMB, MRCVS; Natalie C. Finch, BVSc, PhD, MRCVS; Harriet M. Syme, BSc, BVetMed, PhD, DACVIM, DECVIM-CA, MRCVS and Jonathan Elliott, MA, VetMB, PhD, DECVPT, MRCVS Abstract Objective – To review the human and veterinary literature on the role of phosphorus in the pathophysiology of chronic kidney disease (CKD) and to explore why control of plasma phosphorus concentration is an important goal in the management of patients with this disease. Data Sources – Human and veterinary studies, reviews, clinical reports, textbooks, and recent research findings focused on phosphate homeostasis and CKD patient management. Human Data Synthesis – Recent studies using rodent models and human patients with CKD have focused on trying to elucidate the role of the phosphatonins, predominantly fibroblast growth factor-23, in phosphate homeostasis and the pathophysiology of secondary renal hyperparathyroidism (SRHP). Fibroblast growth factor-23 is now considered to be a key regulator of plasma phosphorus concentration in people but has only recently been investigated in companion animal species. Veterinary Data Synthesis – Cross-sectional studies of naturally occurring CKD in dogs and cats have shown hyperphosphatemia and SRHP to be highly prevalent and associated with increased morbidity and mortality in these patients. Experimental studies of surgically induced renal impairment in the dog and cat, and cases of naturally occurring CKD have emphasized the ability of renal care diets to modify plasma phosphorus and parathyroid hormone concentrations. Evidence from these studies indicates that maintaining plasma phosphorus concentrations to within the International Renal Interest Society targets for CKD patients improves survival time and reduces clinical manifestations of hyperphosphatemia and SRHP. Conclusions – The maintenance of plasma phosphorus concentrations in to within the International Renal Interest Society targets is recommended in management of CKD patients. The discovery of the phosphatonins has improved understanding of the mechanisms involved in phosphorus homeostasis and SRHP and may lead to improved ability to monitor and manage these patients. (J Vet Emerg Crit Care 2013; 23(2): 122–133) doi: 10.1111/vec.12032 Keywords: cat, diet, dog, FGF-23, hyperparathyroidism, renal Abbreviations From the Department of Veterinary Clinical Sciences, Royal Veterinary College, Hawkshead Lane, North Mymms, Hatfield, AL9 7TA, UK (Geddes, Syme); and Department of Veterinary Basic Sciences, Royal Veterinary College, Royal College Street, Camden, London, NW1 0TU, UK (Finch, Elliott). Dr. Natalie C. Finch’s current address is School of Veterinary Sciences, University of Bristol, Langford, Bristol, BS40 5DU, UK. The Renal Research Clinic at the RVC acknowledges support from Royal Canin for its research on feline hyperphosphataemia and chronic kidney disease. R. Geddes is also in receipt of an Everts Luff Trust Research Training Fellowship. Address correspondence and requests for reprints to Ms. Rebecca Geddes, Department of Veterinary Clinical Sciences, The Royal Veterinary College, Hawkshead Lane, North Mymms, Hertfordshire, AL9 7TA, UK. Email: [email protected] Submitted March 2, 2012; Accepted February 2, 2013. 122 CKD Cr FGF-7 FGF-23 GFR GI IRIS ME MF NPD PTH RF RPD SRHP chronic kidney disease creatinine fibroblast growth factor-7 fibroblast growth factor-23 glomerular filtration rate gastrointestinal International Renal Interest Society metabolizable energy maintenance food normal phosphorus diet parathyroid hormone renal food restricted phosphorus diet secondary renal hyperparathyroidism C Veterinary Emergency and Critical Care Society 2013 Role of phosphorus in the pathophysiology of CKD UPC USG urine protein:creatinine ratio urine specific gravity CKD, starting with phosphorus homeostasis, and explores the importance of control of plasma phosphorus to within the IRIS targets in the management of these cases. Introduction Feline chronic kidney disease (CKD) is a common medical condition and the prevalence increases with advancing age. Thirty-one percent of cats over 15 years of age are reported to be affected,1 and in one study, 30.5% of nonazotemic geriatric cats (≥9 years of age) developed azotemia within 12 months.2 In many cases, the underlying cause of feline CKD is unknown and may not be identified even if histopathology of renal tissue is carried out. In one report, over 50% of cases had a morphological diagnosis recorded as chronic tubulointerstitial nephritis of unknown cause.3 CKD is less prevalent in dogs and the age at onset is more variable due to a number of breed-associated diseases affecting the canine kidney. In one study of dogs presenting at 24 primary care veterinary practices in the United Kingdom, 111 cases were confirmed to have kidney dysfunction from a total of 10,700 cases presented for vaccination (1%).4 Confirmation of kidney dysfunction in this study was based on plasma urea and creatinine concentrations, urinary protein, and urine sediment evaluation. Renal histological material was available for 76 of the 111 cases; 52% of cases were found to have glomerular disease and 48% to have nonglomerular disease.4 Reduction in the number of functioning nephrons affects the homeostasis of a number of solutes primarily excreted in the urine, including phosphorus. Hyperphosphatemia is thought to be the initiating factor in the development of secondary renal hyperparathyroidism (SRHP), which is considered a common complication, with parathyroid hormone (PTH) concentrations reported to be increased in 84% of cats and 76% of dogs with CKD.5, 6 Plasma phosphorus concentration is associated with survival of cats and dogs with CKD,5, 7–11 and is therefore an important consideration when treating these cases. The International Renal Interest Society (IRIS) provides a staging system for use in dogs and cats with CKD. This staging system is based on fasting plasma creatinine concentrations in the stable CKD patient, using creatinine as a marker for glomerular filtration rate (GFR), with substaging based on urine protein:creatinine ratio and blood pressure. In 2006, recommendations for the control of plasma phosphorus in cats and dogs with CKD were proposed by a group of veterinary nephrologists, and targets for plasma phosphorus were established for each IRIS stage (Table 1). This review discusses the current knowledge regarding the role of phosphorus in the pathophysiology of C Veterinary Emergency and Critical Care Society 2013, doi: 10.1111/vec.12032 Phosphorus hypothesis homeostasis and the “trade-off” Inorganic phosphorus is an important component of living cells and is an essential structural component of bones and teeth in mammals. Phosphorus homeostasis requires a balance between dietary intake, exchange of phosphorus between extracellular and bone storage pools, and renal excretion. The physiological regulation of phosphorus is incompletely understood. It is interlinked with calcium homeostasis; both minerals are subject to control by the calcitropic hormones, PTH and calcitriol, and an increase in plasma phosphorus concentration causes a reciprocal decrease in ionized calcium concentration via the law of mass action. Calcitriol (1,25dihydroxycholecalciferol) increases phosphorus and calcium absorption from the gastrointestinal (GI) tract. PTH increases phosphorus and calcium resorption from bone and acts to increase calcium reabsorption and decrease phosphorus reabsorption from the glomerular filtrate in the renal tubules. Increased plasma phosphorus concentration stimulates increased PTH secretion and inhibits formation of calcitriol in the kidney, forming homeostatic feedback loops. However, over the last 11 years a number of phosphorus-regulating hormones, termed the “phosphatonins” have been proposed, and research is just beginning to be published on the role of these hormones in veterinary species. A more detailed discussion of phosphatonins can be found elsewhere in this issue.12 In the healthy kidney, phosphate ions are freely filtered at the glomerulus and their excretion is controlled by an overflow mechanism; in people, if plasma inorganic phosphorus concentrations fall below approximately 1 mmol/L (3.1 mg/dL), all of the phosphate ions in the glomerular filtrate are reabsorbed,13 whereas above this threshold, the rate of phosphate loss is directly proportional to the plasma inorganic phosphorus concentration, with GFR determining the steepness of this relationship. PTH reduces proximal tubular capacity to reabsorb phosphate ions (mediated by type II sodiumdependent phosphate transporters, NaPi-IIa), reducing the threshold plasma concentration at which phosphate ions appear in the urine and thereby rapidly increasing phosphate ion loss in urine (see Figure 1). The phosphatonin fibroblast growth factor-23 (FGF-23) has the same action on NaPi-IIa, as discussed below. In CKD, GFR decreases as the number of functioning nephrons declines and this reduces the excretion 123 R. F. Geddes et al. Table 1: The International Renal Interest Society (IRIS) targets for plasma phosphorus Plasma creatinine Target plasma phosphorus Dogs Cats Dogs and cats IRIS stage mg/dL mol/L mg/dL mol/L mg/dL mmol/L 1 2 3 4 <1.4 1.4–2.0 2.1–5.0 >5.0 <125 125–179 180–439 >440 <1.6 1.6–2.8 2.9–5.0 >5.0 <140 140–249 250–439 >440 N/A 2.5–4.5 2.5–5.0 2.5–6.0 N/A 0.81–1.45 0.81–1.61 0.81–1.94 of phosphate ions by decreasing the slope of the relationship between plasma phosphate concentration and urinary phosphate ion excretion (see Figure 1). An increase in plasma inorganic phosphorus concentration stimulates PTH secretion directly and indirectly (see Figure 2), and PTH subsequently inhibits phosphate ion reabsorption in the proximal tubules, acting to increase fractional excretion of phosphate by the kidney. However, PTH is principally a hormone regulating plasma ionized calcium concentration, and as such, it also acts to increase calcium and phosphate ion efflux from bone and stimulates calcitriol production by the kidney (which increases calcium and phosphorus absorption from the small intestine). This serves overall to increase ionized calcium concentrations and decrease phosphorus concentrations, but the limitation in the mechanism is that phosphorus can only be excreted via the kidney. In CKD, if GFR continues to decline and dietary phosphorus intake remains stable, phosphorus retention will ultimately occur, leading to whole body overload with phosphorus, hyperphosphatemia, and increased plasma PTH concentrations. Chronic elevation of PTH leads to demineralization of bone. Additionally, phosphorus deposition occurs in soft tissues and mineralization ensues, a phenomenon which is thought to contribute to progressive kidney injury (ie, when the kidneys become mineralized) and to the extra-renal (particularly cardiovascular) effects of SRHP. Originally described in the early 1970s, this description of the pathophysiology of SRHP is known as the “trade-off hypothesis,”14 where the “trade-off” for the increased fractional excretion of phosphorus by each remaining nephron, is the chronic elevation in PTH (see Figure 2). Over the past 40 years this hypothesis has been greatly expanded, although many aspects of phosphorus sensing and homeostasis still remain unclear. Current Published Human Research Information and Data Phosphatonins The presence of hormones primarily involved in phosphorus regulation was first proposed in the 1990s 124 Figure 1: Renal function curves for phosphorus excretion. In the normal situation, phosphate ions appear in the urine once plasma phosphate exceeds 3.1 mg/dL (1 mmol/L) as this exceeds the reabsorptive transport maximum for phosphorus. The slope of the curve is dependent on GFR although its position is shifted to the left by increases in PTH and FGF-23, both of which reduce the transport maximum for phosphate ion absorption in the proximal tubule and increase phosphate ion excretion at a given plasma phosphorus concentration. At stable GFR, for a given dietary phosphorus intake, the daily excretion of phosphorus in the urine will match phosphorus intake (dietary intake minus fecal losses) and the plasma phosphorus concentration at which this occurs will be influenced by the prevailing PTH and FGF-23 concentrations. In CKD, as GFR falls the gradient of this renal excretion curve becomes less steep and plasma phosphate concentration for a given dietary intake will increase despite increases in plasma PTH and FGF-23. GFR, glomerular filtration rate; PTH, parathyroid hormone; FGF-23, fibroblast growth factor-23; CKD, chronic kidney disease. following investigations of human patients and animal models with conditions characterized by severe derangements in phosphorus homeostasis. A number of phosphatonins have now been identified: FGF-23, secreted frizzled-related protein 4, matrix extracellular phosphoglycoprotein, and FGF-7;15, 16 however, FGF-23 remains the most thoroughly studied of these hormones. FGF-23 is secreted primarily by osteocytes17 and osteoblasts18 in response to increased plasma phosphorus or calcitriol concentrations.19 To bind to its receptor, FGFR1c, FGF-23 requires a co-factor, Klotho, which exists in both membrane bound and circulating forms. This heterodimeric receptor, Klotho-FGFR1c, appears to C Veterinary Emergency and Critical Care Society 2013, doi: 10.1111/vec.12032 Role of phosphorus in the pathophysiology of CKD Figure 2: Schematic presenting the traditional and recently updated views of the “trade-off” hypothesis. In the traditional hypothesis, the reduction in GFR leads to reduced phosphate ion clearance in the kidney and therefore to an increase in plasma phosphorus concentration. Increasing plasma phosphorus stimulates PTH secretion directly, and indirectly via inhibition of calcitriol production in the kidney and by reducing plasma ionized calcium concentration via the law of mass action. The “trade-off” for an increase in phosphate ion excretion is an increase in plasma PTH concentration leading to a number of deleterious effects. In the updated hypothesis, the decrease in phosphate ion clearance stimulates FGF-23 secretion, which increases the FE of phosphate ions and inhibits calcitriol production in the kidney in early CKD. This maintains plasma phosphorus concentration within normal limits. In late-stage CKD, the kidney is unable to increase the FE of phosphate ions any further due to low nephron mass, and hyperphosphatemia develops. The increased plasma phosphorus, reduced calcitriol, and reduced ionized calcium all drive the increase in PTH concentration and the clinical manifestations of SRHP develop. GFR, glomerular filtration rate; PTH, parathyroid hormone; CKD, chronic kidney disease; FE, fractional excretion; SRHP, secondary renal hyperparathyroidism; FGF-23, fibroblast growth factor-23. be predominantly expressed in the kidney, parathyroid, and pituitary glands,20 however, Klotho gene expression has also been detected in the choroid plexus21 and sinoatrial node.22 In the kidney, FGF-23 acts to regulate phosphorus and calcitriol homeostasis through regulation of the sodium-phosphorus type II co-transporters (NaPi-IIa and NaPi-IIc)15 and the vitamin D synthesis enzyme (25-hydroxyvitamin D-1␣-hydroxylase).20 In the parathyroid gland, it acts to decrease PTH production and secretion.23 FGF-23 is a low molecular weight protein that has been hypothesized to be excreted by the kidney and is therefore likely to accumulate in CKD due to reduced renal clearance.24 FGF-23 in serum from CKD patients is predominantly that of the full-length molecular weight, termed intact FGF-23, rather than FGF-23 fragments24 and it has been well documented that circulating intact FGF-23 increases with declining renal C Veterinary Emergency and Critical Care Society 2013, doi: 10.1111/vec.12032 function in people.24–27 The correlation of serum FGF23 concentration and GFR suggests that reduced GFR in CKD is an important determinant of circulating FGF-23 concentration,28 but serum FGF-23 is also affected by additional factors. In a number of studies involving people and rodents, FGF-23 concentrations increased during dietary phosphorus loading and decreased with dietary phosphorus restriction.29–31 Although the role of FGF-23 has yet to be thoroughly explored in companion animals, it is appropriate to update the working hypothesis for the pathophysiology of hyperphosphatemia in CKD based on the observations in the human literature. An updated “trade-off” hypothesis still begins with phosphorus retention developing as GFR starts to decline in the failing kidney, but it is necessary to consider the mechanisms involved in early CKD and latestage CKD separately. In early CKD, the increase in 125 R. F. Geddes et al. phosphorus will drive an increase in FGF-23 concentration (via a currently unknown sensor), which has a number of effects. First, there will be inhibition of the sodium-phosphorus co-transporters in the kidney which will act to increase fractional excretion of phosphorus in the remaining nephrons. Second, inhibition of 1␣hydroxlyase, by increased phosphorus and FGF-23, will result in lower concentrations of calcitriol, thereby decreasing phosphorus absorption from the GI tract. Third, FGF-23 will cause direct inhibition of PTH secretion via activation of Klotho-FGFR1c in the parathyroid gland cells. The inhibition of PTH will prevent the drive to increase ionized calcium concentration that also results in a concurrent increase in phosphorus concentration when calcium and phosphorus are released from bone in response to PTH. In patients with early CKD this increase in FGF-23, and consequent increase in urinary phosphate ion excretion, will therefore be enough to restore phosphorus homeostasis and prevent the development of SRHP (see Figure 2). In support of this theory, it has been observed that in human patients with CKD, a rise in FGF-23 concentrations and fall in calcitriol concentrations precedes the development of overt hyperphosphatemia.26 In more severe CKD, there will be 3 main reasons that FGF-23 will continue to increase. First, as GFR decreases, intact FGF-23 will also increase because it is freely filtered at the glomerulus. Second, once GFR drops to below a critical rate (which has shown to be 30 mL/min/1.73 m2 in human patients), plasma phosphate concentrations start to increase28, 32 and will stimulate FGF-23 secretion. Third, end organ resistance to FGF-23 will develop as a result of reduced expression of FGFR1 and Klotho mRNA, leading to downregulation of the Klotho-FGFR1 receptors and resulting in FGF-23 losing its direct inhibition of PTH.23, 33 At this point FGF-23 might be considered a uremic toxin, because it will continue to decrease calcitriol concentrations without hypophosphatemic action. Reduced calcitriol will both reduce inhibition of PTH secretion in the parathyroid gland and indirectly increase PTH secretion via reduced GI uptake of ionized calcium leading to reduced plasma ionized calcium. Low plasma ionized calcium concentration then becomes a major driving force for a rise in PTH, and additionally, hyperphosphatemia will stimulate PTH secretion directly.34, 35 The development of overt hyperphosphatemia will only occur late in the progression of SRHP in this model because PTH and FGF-23 are both phosphaturic, and the fractional excretion of phosphorus is at its highest in patients with both high FGF-23 and high PTH.36 Therefore, the increases in both of these hormones will compensate for the reduction in nephron mass until GFR falls below 30 mL/min/1.73 m2 , at which stage plasma phos126 phate concentrations have been shown to increase.28, 32 In end-stage CKD there is loss of all feedback on PTH through downregulation of not only FGFR1-Klotho, but also the vitamin D receptor and the calcium sensing receptor in the parathyroid glands,23 resulting in hyperphosphatemia and calcitriol deficiency despite vastly increased plasma concentrations of FGF-23 and PTH (see Figure 2). FGF-23 has been shown to predict the progression of CKD in human patients.27 This is potentially a very important finding, since increased plasma FGF-23 concentration (defined as FGF-23 > 50 pg/mL) in human CKD patients is up to 6 times more prevalent in the mild stages of CKD than increased plasma PTH concentrations (defined as PTH > 40 ng/L).36 FGF-23 concentrations are also independently and directly associated with mortality rate in patients starting hemodialysis for CKD, with a strong concentration-dependent relationship.37 At present, it is unclear whether FGF-23 is a uremic toxin, or whether it could be a surrogate marker for other causes of uremic toxicity in these patients. Answering this question may clarify whether increased FGF-23 concentrations should be a target of treatment or just used as a marker of disease severity. Current Published Veterinary Information The prevalence of hyperphosphatemia and SRHP in CKD Hyperphosphatemia and SRHP are highly prevalent in both feline and canine CKD patients. Barber and Elliott identified an overall prevalence of hyperparathyroidism of 84% in cats with CKD.5 The 80 cats with naturally occurring CKD (plasma creatinine [Cr] >177 mol/L [>2.0 mg/dL]) included in this study were categorized subjectively into 3 groups; “compensated” for cats with no clinical signs (mean Cr 229 mol/L [2.6 mg/dL]), “uremic” for cats with historical and physical examination findings compatible with the uremic syndrome (mean Cr 316 mol/L [3.6 mg/dL]), and “end-stage” (mean Cr 909 mol/L [10.3 mg/dL]). Hyperparathyroidism was the most common abnormality of calciumphosphorus (Ca-P) homeostasis, with plasma PTH concentrations increased in 47% of the compensated cases, 87% of the uremic cases, and 100% of the end-stage cases. Hyperphosphatemiaa was present in 20% of the compensated cases, 49% of the uremic cases, and 100% of the end-stage cases. SRHP was present in 13% of cases which had normal ionized calcium and plasma phosphorus concentrations. Calcitriol concentrations were assayed in 31 cases and 11 of these (including 8/10 [80%] in the end-stage group) were below the reference interval. Similar findings have been published for cases of canine CKD. Cortedellas and colleagues published a C Veterinary Emergency and Critical Care Society 2013, doi: 10.1111/vec.12032 Role of phosphorus in the pathophysiology of CKD study of 54 dogs with CKD, diagnosed based on persistent proteinuria (urine protein:creatinine ratio ≥0.5) or azotemia (Cr ≥ 125 mol/L [1.4 mg/dL]) with a concurrent urine specific gravity <1.025, and classified the cases according to the IRIS staging system.6 Again, hyperparathyroidism was the most common abnormality of Ca-P homeostasis, occurring in 75.9% of cases overall and increasing in prevalence with IRIS stage: 36.4% of stage 1, 50% of stage 2, 96% of stage 3, and 100% of stage 4 cases. Hyperphosphatemiab was documented in 68.5% of dogs, again increasing in prevalence with increasing IRIS stage: 18% of stage 1, 40% of stage 2, 92% of stage 3, and 100% of stage 4. Calcitriol concentrations were below the reference range in 10 cases, 5/25 (20%) in stage 3 and 5/8 (62.5%) in stage 4. For both species therefore, SRHP and hyperphosphatemia are common and occur with increasing prevalence as kidney function declines. It has been demonstrated that in all but IRIS stage 4 in dogs6 and end-stage CKD in cats,5 SRHP is more prevalent than hyperphosphatemia in both species. This suggests that the increase in PTH concentration precedes the development of hyperphosphatemia, as would be expected from the updated trade-off hypothesis in which overt hyperphosphatemia is the last derangement of Ca-P homeostasis to occur. In support of this, a prospective longitudinal study of nonazotemic cats by Finch et al38 demonstrated that plasma PTH concentrations are significantly increased in cats that develop azotemia within 12 months, when compared to cats which remain nonazotemic over the same time period. In that study, cats were classified into 3 groups based on their kidney function at the study end point (12 months): group 1: Cr ≤ 140 mol/L (≤1.6 mg/dL), group 2: Cr > 140 mol/L (>1.6 mg/dL) but did not meet the criteria for group 3, and group 3: persistent Cr ≥ 177 mol/L (≥2.0 mg/dL) with concurrent urine specific gravity <1.035 when available. In group 3, 32% had increased plasma PTH concentrations at entry to the study (ie, before they became azotemic), despite none of the cats being hyperphosphatemic. Ca-P product also increased significantly over the 12-month study period in these cats. In agreement with previous studies, at the 12-month time point, a greater proportion of the azotaemic cats (30 cats in IRIS stage 2 and 1 cat in IRIS stage 4) had SRHP (48%) than were hyperphosphatemic (16%).38 Data presented in abstract form from studies involving cats with naturally occurring CKD and appropriately age-matched controls has shown plasma concentrations of FGF-23 in cats with CKD increases with IRIS stage, inversely correlating with GFR. In addition to plasma creatinine, plasma phosphate has been shown to be an C Veterinary Emergency and Critical Care Society 2013, doi: 10.1111/vec.12032 independent predictor of plasma FGF-23 concentration in cats with CKD. Clinical consequences of hyperphosphatemia and SRHP in cats and dogs Hyperphosphatemia in CKD is associated with decreased survival and significant morbidity. In dogs with experimentally induced CKD, hyperphosphatemia has been associated with a more rapid progression of CKD and with decreased survival.10, 11 Hyperphosphatemia is also associated with shorter survival times in cats with naturally occurring CKD.7, 39 Additionally, plasma phosphorus has recently been documented to be an independent predictor for progression of feline CKD; an increase of 0.32 mmol/L (1 mg/dL) in plasma inorganic phosphorus was independently associated with a 41% increase in the risk of progression (where progression was defined as an increase in plasma Cr of ≥25%).40 Clinical manifestations of SRHP include soft tissue mineralization (see Figure 3) and renal osteodystrophy. Cats with CKD can develop pathological fractures, loose teeth, and “rubber jaw” syndrome as a consequence of bone demineralization.41 It has been suggested that soft tissue calcification may be a more common manifestation of feline SRHP than bone demineralization,42 although in one study of 74 cats with CKD, 9.8% had generalized osteoporosis, 7.3% had nephrocalcinosis, and 9.5% had soft tissue mineralization.3 Soft tissue structures that have shown mineralization in feline CKD cases include the kidneys, thoracic and abdominal aorta, the gastric wall, and pulmonary arteries and capillaries (see Figure 3).43, 44 Metastatic calcifications have been documented in cases of feline and canine CKD in the paws, which can cause lameness,43–46 and have been suggested to occur when the serum Ca-P product is >70 mg2 /dL2 and PTH is concurrently increased.45 Evidence in support of the IRIS targets for plasma phosphorus A group of veterinary nephrologists established guidelines for plasma phosphorus concentrations in 2006, to fit in with the IRIS classification of canine and feline CKD. Extrapolating from the Kidney Disease Outcomes Quality Initiative recommendations for human CKD patients and their own clinical experience, control of plasma phosphorus concentration to well within the laboratory reference interval was considered to be an important goal in the management of CKD cases. It was recommended that diets with phosphorus restriction ± intestinal phosphorus-binding agents should be used to achieve the targets as shown in Table 1. There is a substantial evidence basis from experimental model and 127 R. F. Geddes et al. Figure 3: Soft tissue calcification affecting the kidneys and gastric wall, with some mestastatic calcification evident in the abdominal vasculature, due to SRHP in a cat. Radiograph taken postmortem. SRHP, secondary renal hyperparathyroidism. veterinary patient studies to support these guidelines, as discussed below. The use of phosphorus restriction in the control of SRHP was initially investigated in the early 1970s. Using canine remnant kidney models, with a staged approach to reduce GFR 4 times throughout the course of the experiments, Slatopolsky et al clearly demonstrated that PTH concentrations increased with every reduction in GFR when the dogs were fed a normal diet, but PTH did not increase at all when the dogs were fed a severely phosphorus-restricted diet.47 In a follow-on study they demonstrated that a “proportional reduction” of dietary phosphorus in parallel with the reduction in GFR also prevented any increase in plasma PTH concentrations.48 It was concluded from these studies that phosphorus restriction should be the mainstay in control of SRHP.49 Only one experimental study has been published in cats where the effect of phosphorus intake on progressive renal injury in a renal mass reduction model has been studied.50 It compared the effect of feeding a normal phosphorus diet (NPD; 1.56% phosphorus on a dry matter [DM] basis) and a restricted phosphorus diet (RPD; 0.42% phosphorus DM) to cats following a 4/6 nephrectomy and concluded that neither diet caused a significant change in renal function over 343 days. After 8 weeks on the diets, the restricted phosphorus group had a mean plasma phosphorus concentration of approximately 1.6 mmol/L (approximately 5 mg/dL) compared to approximately 2.2 mmol/L (approximately 6.8 mg/dL) in the normal phosphorus group.e After 28 weeks, the mean plasma phosphorus concentrations were approximately 1.3 mmol/L (approximately 4.0 mg/dL) and approximately 2.3 mmol/L (approximately 7.0 mg/dL) for the 128 restricted phosphorus and normal phosphorus groups, respectively. Additionally, they reported that the NPD induced marked mineralization, fibrosis, and mononuclear cell infiltration in the remnant kidneys, whereas the cats fed the phosphorus-restricted diet had much milder histological changes. This study refers to the NPD as being equivalent to the phosphorus content of a commercial canned cat food; however, it should be noted that the current recommendation by the American Association of Food Control Officials for phosphorus intake in an adult cat at maintenance is 1.25 g/1000 kcal metabolizable energy (ME), equivalent to 0.5% phosphorus on a DM basis (assuming a dietary energy density of 4000 kcal ME/kg).51 Additionally, the authors of this study stated the recommended dietary phosphorus intake for adult cats at the time of publication to be 0.8% dry weight. Therefore, the NPD in this study greatly exceeded recommended phosphorus food content. Overall, this study suggests that reducing phosphorus intake and maintaining a plasma phosphorus concentration of between 1.29 and 1.61 mmol/L (4.0 and 5.0 mg/dL) is protective of remaining functioning renal tissue in this surgical reduction model of renal failure, which is close to the IRIS targets (<1.45 or 1.61 mmol/L [<4.5 or 5.0 mg/dL]) for stages 2 and 3 CKD. The effect of dietary phosphorus restriction and protein content on progressive deterioration of renal function has also been studied in a remnant kidney (15/16 surgical nephrectomy) model in dogs,10 by using 4 diets (group 1: low phosphorus (Pi), low protein (Pr); group 2: high Pi, low Pr; group 3: low Pi, high Pr; group 4: high Pi, high Pr). This study demonstrated that the amount of phosphorus fed influenced survival, with 15/24 dogs fed the low phosphorus diet (groups 1 and 3) surviving the 24 months of the study and only 8/24 dogs fed the high phosphorus diet (groups 2 and 4) surviving. The level of protein fed did not affect survival. GFR remained stable for longer in the dogs fed the low phosphorus diets (groups 1 and 3; 12.7 ± 2.0 mo) when compared with those animals receiving high phosphorus diets (groups 2 and 4; 7.5 ± 2.0 mo). There was no significant effect of diet on renal morphology or mineral content in the remnant kidney as assessed at the end of the 24-month study or earlier if the dogs died or were euthanized due to uremia. The authors of that study concluded that dietary phosphorus content was more important than dietary protein content for preventing adverse responses to reduction in renal mass and that the survival benefit from phosphorus restriction may be due to extra-renal effects, since the low phosphorus diets (0.4% Pi on a DM basis) were inadequately phosphorus restricted to prevent renal mineralization. At the 4-month time point, the mean plasma phosphorus concentrations were 1.62 mmol/L C Veterinary Emergency and Critical Care Society 2013, doi: 10.1111/vec.12032 Role of phosphorus in the pathophysiology of CKD (5.03 mg/dL) for group 1, 2.61 mmol/L (8.08 mg/dL) for group 2, 2.10 mmol/L (6.51 mg/dL) for group 3, and 2.62 mmol/L (8.11 mg/dL) for group 4. The results could be interpreted to mean that the 4-month plasma phosphorus concentration of between 1.62 mmol/L and 2.1 mmol/L (5.03 and 6.51 mg/dL) is not optimal to protect against soft tissue mineralization. Thus, these data are compatible with the IRIS recommendations to maintain plasma phosphorus at <1.45 mmol/L (<4.5 mg/dL) for stage 2 and <1.61 mmol/L (<5.0 mg/dL) for stage 3. Studies of feeding protein- and phosphorus-restricted diets to cats with naturally occurring CKD have shown that these diets can reduce plasma urea and phosphorus concentrations, which is associated with a reduction in the risk of a uremic crisis developing and death due to renal causes.52 One study demonstrated a significant reduction in plasma PTH concentrations by 105–147 days in cats with CKD eating a commercially produced renal diet (see Figure 4).53 No significant change was demonstrated in PTH concentrations in a control group (fed the maintenance diet preferred by their owners) over the same time period (see Figure 4). Plasma phosphorus concentrations decreased significantly in the renal diet group at the earlier time point of 28–49 days, and remained significantly reduced at 105–147 days when compared to baseline (see Figure 5). The reduction in plasma PTH concentrations in this study was associated with a decrease in plasma phosphorus concentrations but no change in plasma total calcium or calcitriol concentrations. In dogs with experimentally induced renal failure it has also been shown that a reduction in dietary phosphorus decreases plasma PTH concentrations without changes in plasma ionized calcium or calcitriol concentrations.54 Additionally, in a case report by Jackson and Barber in 1998,45 feeding a protein- and phosphorus-restricted diet exclusively resulted in resolution of metastatic calcification in the paws of a cat with stage 3 CKD by day 105. This was accompanied by a reduction in the Ca-P product to <70 mg2 /dL2 , and a reduction in plasma phosphorus concentration from 2.2 mmol/L (6.8 mg/dL) to 1.5 mmol/L (4.7 mg/dL), which is within the target plasma phosphorus concentration for IRIS stage 3. Survival time of dogs was examined by Jacob et al in 2002.55 This randomized, double-blinded, controlled clinical trial was performed in 38 dogs with naturally occurring CKD in IRIS stage 3 or 4, and examined the effect of feeding a renal food (RF) compared with a standardized maintenance food (MF). The dogs were managed in an identical manner with respect to other treatment interventions. The median survival time for the RF dogs was 594 days, significantly longer than the median survival time of 188 days in the MF group. The onset of a uremic crisis was significantly delayed in the RF group; median C Veterinary Emergency and Critical Care Society 2013, doi: 10.1111/vec.12032 Figure 4: Effect of feeding a commercially produced renal diet to cats with naturally occurring chronic kidney disease (IRIS stages 2 and 3) on plasma PTH concentration. Data are mean values from 14 cats (squares) that were fed a renal care diet and 8 cats (circles) maintained on maintenance diets. Error bars represent 1 SD of the mean. Differences compared to the value on day 0 by a paired t-test are illustrated, significance was taken to be P ≤ 0.017 following Bonferroni correction (∗no significant difference between the 2 groups at Day 0). IRIS, International Renal Interest Society; PTH, parathyroid hormone; SD, standard deviation; NS, not significant. Reproduced with permission from John Wiley and Sons Ltd. From Barber PJ, et al. Effect of dietary phosphate restriction on renal secondary hyperparathyroidism in the cat. J Small Anim Pract 1999;40:62–70. time to a uremic crisis was 615 days in the RF group and 252 days in the MF group. Additionally, renal function (defined as the reciprocal of serum creatinine concentration) was documented to decline more slowly in the RF group over 24 months. However, when the mean overall plasma phosphorus concentrations were compared between the groups, no significant difference was detected. Overall, this study demonstrated that feeding a renal diet significantly increases survival time and slows renal function decline in dogs with stage 3 or 4 CKD. Effect of renal diet on survival time has also been examined in cats, retrospectively56 and prospectively.52, 57 Ross et al, conducted a double-blinded, randomized, controlled clinical trial of cats with naturally occurring stage 2 or 3 CKD, to investigate the effect of feeding a renal diet compared to a feline adult maintenance diet.52 In this study of 45 cats, the cats were managed in an identical manner except for the diet they were randomly assigned to. Over a 2-year period, the group fed the renal diet was found to have significantly lower urea and phosphate concentrations but no significant difference in creatinine or PTH concentrations when compared to the maintenance diet group. The renal diet group had significantly fewer uremic episodes (0%) than the maintenance diet group (26%) and had significantly fewer 129 R. F. Geddes et al. Figure 5: Effect of feeding a commercially produced renal diet to cats with naturally occurring chronic kidney disease (IRIS stages 2 and 3) on plasma phosphate concentration. Data are mean values from 14 cats (squares) that were fed a renal diet and 8 cats (circles) maintained on maintenance diets. Error bars represent 1 SD of the mean. Differences compared to the value on day 0 by a paired t-test are illustrated, significance was taken to be P ≤ 0.017 following Bonferroni correction (∗no significant difference between the 2 groups at Day 0). IRIS, International Renal Interest Society; SD, standard deviation; NS, not significant. Reproduced with permission from John Wiley and Sons Ltd. From Barber PJ, et al. Effect of dietary phosphate restriction on renal secondary hyperparathyroidism in the cat. J Small Anim Pract 1999;40:62–70. renal-related deaths (0% versus 21.7%) during the 2-year study period. A study by Elliott et al also investigated the effects of feeding a protein- and phosphorus-restricted diet to cats with stable naturally occurring CKD.57 All owners were offered the protein-/phosphorus-restricted diet for their cats and the control group (NPD group) was formed using cats that demonstrated poor compliance eating the diet (cats which ate <50% of total intake as the renal diet), or whose owners declined the diet. Although not a double-blinded, placebo-controlled study, the 2 groups were matched for physical, hematological, and biochemical parameters at the beginning of the study. The RPD group was monitored closely to attempt to maintain PTH concentrations within the normal range using the diet ± a phosphorus binder but otherwise the 2 groups were treated equally. The results indicated a significantly longer median survival time in the RPD group of 633 days compared to 264 days for the NPD group. Furthermore, the RPD group had significant decreases in their urea concentrations and had lower plasma phosphorus concentrations than the NPD group. Plasma PTH concentrations significantly increased in the NPD group and decreased in 69% of the RPD group by the mid-survival time point, although the decrease in plasma PTH when 130 Figure 6: The relationship between the survival time and mean plasma phosphorus concentration achieved in the first half of the patients survival period. Data reanalyzed from Elliott (2000). Reproduced with permission from Elliott J and Elliott D. Dietary therapy for feline chronic kidney disease. In: Pascale P, Biourge V, Elliott D. eds. Encyclopedia of feline clinical nutrition. Ainargues, France: Aniwa SAS Ltd; 2008:411–45. compared to baseline did not reach statistical significance. Overall, this study clearly demonstrated that cats which ate a diet specially formulated for CKD had significantly longer survival times than cats that were not willing to eat a renal diet. Unpublished data from the same study showed that 55%, 90%, and 100% of cats presenting in stage 2, 3, and 4 CKD, respectively, had plasma phosphorus concentrations above 1.45 mmol/L (4.5 mg/dL) at diagnosis. The relationship between the mean plasma phosphorus concentrations for the first half of their survival period and survival times for the cats in this study is shown in Figure 6. Additionally, reanalysis of the data from this study demonstrated that if the average plasma phosphorus concentration was maintained at below 1.45 mmol/L (4.5 mg/dL) for the first half of their survival time (this was achieved in 18 of the 50 cats) their median survival time was 799 (interquartile range 569–1,383) days whereas for cats where the average plasma phosphorus concentration exceeded 1.45 mmol/L (4.5 mg/dL) the median survival time was 283 (interquartile range 193–503) days. Although this study was not designed to determine the effect of achieving a particular plasma phosphate target by restricting phosphate intake, these data are supportive of the target guidelines for plasma phosphorus concentration in CKD. To date, no studies have been published examining the effect of dietary phosphorus restriction on plasma FGF-23 concentrations in companion animal species. However, in the recently published abstract examining C Veterinary Emergency and Critical Care Society 2013, doi: 10.1111/vec.12032 Role of phosphorus in the pathophysiology of CKD FGF-23 in a cross-section of nonazotemic and azotemic IRIS stage 2–4 cats, plasma FGF-23 concentrations were found to be significantly higher in stage 2 and 3 cats with plasma phosphorus concentrations above the maximum IRIS targets for those stages (>1.45 mmol/L [>4.5 mg/dL] for stage 2 and >1.61 mmol/L [>5mg/dL] for stage 3).d The evidence from the veterinary literature indirectly suggests that maintaining plasma phosphorus concentrations below the IRIS targets for each stage of CKD improves survival, can prevent or reverse SRHP and can resolve clinical manifestations of hyperphosphatemia in companion animals. It is widely accepted that intestinal phosphorus-binding agents are useful in reducing plasma phosphorus concentrations for CKD patients.58, 59 However, there have been no controlled clinical studies examining the effect of using phosphate binders on the progression of naturally occurring CKD or on survival time of dogs and cats with CKD. One study has demonstrated that for cats with a model of CKD equivalent to IRIS stages 1 and 2, addition of a chitosan and calcium carbonate phosphorus binder to a feline maintenance diet can reduce serum phosphorus concentration to below the IRIS target of 1.45 mmol/L (4.5 mg/dL) after 6 months.60 Another preliminary study has shown that lanthanum carbonate octahydrate can significantly reduce apparent digestive phosphorus availability and increase fecal excretion of phosphorus in normophosphatemic cats with a model of CKD.f Within the scope of this review, it is not possible to discuss the evidence for other aspects of CKD management, but this is covered in detail elsewhere.61, 62 Application to Veterinary Emergency and Critical Care Progression of CKD to end-stage frequently occurs, but the time frame is extremely variable and is difficult to predict.39 Many cases remain relatively stable for long periods of time and then suffer a sudden decline in kidney function, which is likely to be a result of a trigger factor resulting in an acute-on-chronic presentation, although in many cases the trigger cannot be identified.9 Companion animals presenting with a uremic crisis must be evaluated carefully to ensure accurate diagnosis of acute kidney injury or an acute-on-chronic episode for a patient with CKD. Hyperphosphatemia can be present in both of these scenarios as any cause of decreased GFR will cause a reduction in urinary phosphate ion excretion leading to an increase in plasma phosphorus. The IRIS staging system and plasma phosphorus targets should only be applied following assessment of fasting plasma creatinine concentrations in a stable patient.63 Therefore, they cannot be used appropriately during evaluation of C Veterinary Emergency and Critical Care Society 2013, doi: 10.1111/vec.12032 the emergency patient. Once a diagnosis of a primary intrinsic renal cause of azotemia has been established the differentiation between acute kidney injury and an acutely decompensated case of CKD must be established. This is important because unless a specific factor is causing acute decompensation in the CKD patient, which is then identified and treated aggressively, the prognosis for advanced CKD is poor. Conclusions and Recommendations for Future Studies There is strong evidence from the veterinary literature for feeding a renal diet to cats and dogs with CKD,61, 62 and this should therefore be considered to be the mainstay of management in these cases. The current general consensus of opinion is to start dietary modification once stable azotemia is demonstrated.63 Additionally, phosphorus binders should be used when necessary to achieve plasma phosphorus concentrations within the IRIS recommendations for each stage of CKD, as maintaining plasma phosphorus concentrations within these targets has been demonstrated to improve survival and prevent or resolve the clinical manifestations of hyperphosphatemia and SRHP in companion animals. Due to the prevalence of hyperparathyroidism being higher than that of hyperphosphatemia at each stage of CKD in both dogs6 and cats,5 it has been recommended that plasma PTH should be measured when plasma phosphorus is within the IRIS targets in order to establish if phosphorus restriction is appropriate.59 FGF-23 is now considered to be a key regulator of plasma phosphate concentrations and to be involved in the development of SRHP in people. However, research is only just beginning to be published on the role of FGF23 in companion animals with CKD. Further studies are required to establish the role of this hormone in Ca-P homeostasis and whether FGF-23 is a marker or mediator of SRHP. Footnotes a b c d e f Hyperphosphatemia was defined in this study as a plasma phosphorus concentration above the reference range (>1.87 mmol/L [>5.8 mg/dL]). Hyperphosphatemia was defined in this study as plasma phosphorus >1.78mmol/L (>5.5mg/dL). Finch NC, Geddes, RF,Syme, H, Elliott, J. FGF-23—mediator of renal secondary hyperparathyroidism or a marker of glomerular filtration rate (GFR) in cats? J Vet Intern Med 2011; 25:720 (Abstract). Geddes RF, Finch NC, Syme, H., Elliott, J. Fibroblast growth factor 23 (FGF-23) in feline chronic kidney disease. J Vet Intern Med 2011; 25:720– 721 (Abstract). The results are depicted in a figure in this paper, therefore the results reported here are approximate. Schmidt DH, Spiecker-Hauser U, Murphy M. Efficacy and safety of Lantharenol on phosphorus metabolism in cats with chronic kidney disease. J Vet Intern Med 2008; 22:798 (Abstract). 131 R. F. Geddes et al. References 1. Lulich JP. Feline renal failure: questions, answers, questions. Compend Contin Educ Pract Vet 1992; 14:127–152. 2. Jepson RE, Brodbelt D, Vallance C, et al. Evaluation of predictors of the development of azotemia in cats. J Vet Intern Med 2009; 23:806– 813. 3. DiBartola SP, Rutgers HC, Zack PM, et al. Clinicopathologic findings associated with chronic renal disease in cats: 74 cases (1973–1984). J Am Vet Med Assoc 1987; 190:1196–1202. 4. Macdougall DF, Cook T, Steward AP, et al. Canine chronic renal disease: prevalence and types of glomerulonephritis in the dog. Kidney Int 1986; 29:1144–1151. 5. Barber PJ, Elliott J. Feline chronic renal failure: calcium homeostasis in 80 cases diagnosed between 1992 and 1995. J Small Anim Pract 1998; 39:108–116. 6. Cortadellas O, del Palacio MJF, Talavera J, et al. Calcium and phosphorus homeostasis in dogs with spontaneous chronic kidney disease at different stages of severity. J Vet Intern Med 2010; 24:73–79. 7. Boyd LM, Langston C, Thompson K, et al. Survival in cats with naturally occurring chronic kidney disease (2000–2002). J Vet Intern Med 2008; 22:1111–1117. 8. Kuwahara Y, Ohba Y, Kitoh K, et al. Association of laboratory data and death within one month in cats with chronic renal failure. J Small Anim Pract 2006; 47:446–450. 9. Elliott J, Barber PJ. Feline chronic renal failure: clinical findings in 80 cases diagnosed between 1992 and 1995. J Small Anim Pract 1998; 39:78–85. 10. Finco DR, Brown SA, Crowell WA, et al. Effects of dietary phosphorus and protein in dogs with chronic renal failure. Am J Vet Res 1992; 53:2264–2271. 11. Brown SA, Crowell WA, Barsanti JA, et al. Beneficial effects of dietary mineral restriction in dogs with marked reduction of functional renal mass. J Am Soc Nephrol 1991; 1:1169–1179. 12. de Brito Galvao JF, Nagode LA, Schenck PA, et al. Calcitriol, calcidiol, parathyroid hormone and fibroblast growth factor-23 interactions in chronic kidney disease. J Vet Emerg Crit Care 2013; 23(2):134–162 13. Guyton AC, Hall JE. Textbook of Medical Physiology, 10th ed. Philadelphia: W. B. Saunders; 2000. 14. Bricker NS. On the pathogenesis of the uremic state. An exposition of the “trade-off hypothesis.” N Engl J Med 1972; 286:1093–1099. 15. Marks J, Debnam ES, Unwin RJ. Phosphate homeostasis and the renal-gastrointestinal axis. Am J Physiol Renal Physiol 2010; 299:F285–F296. 16. Kumar R. Phosphate sensing. Curr Opin Nephrol Hypertens 2009; 18:281–284. 17. Pereira RC, Juppner H, Azucena-Serrano CE, et al. Patterns of FGF23, DMP1, and MEPE expression in patients with chronic kidney disease. Bone 2009; 45:1161–1168. 18. Riminucci M, Collins MT, Fedarko NS, et al. FGF-23 in fibrous dysplasia of bone and its relationship to renal phosphate wasting. J Clin Invest 2003; 112:683–692. 19. Saito H, Maeda A, Ohtomo S, et al. Circulating FGF-23 is regulated by 1 alpha,25-dihydroxyvitamin D-3 and phosphorus in vivo. J Biol Chem 2005; 280:2543–2549. 20. Urakawa I, Yamazaki Y, Shimada T, et al. Klotho converts canonical FGF receptor into a specific receptor for FGF23. Nature 2006; 444:770–774. 21. Tsujikawa H, Kurotaki Y, Fujimori T, et al. A gene related to a syndrome resembling human premature aging, functions in a negative regulatory circuit of vitamin D endocrine system. Mol Endocrinol 2003; 17:2393–2403. 22. Takeshita K, Fujimori T, Kurotaki Y, et al. Sinoatrial node dysfunction and early unexpected death of mice with a defect of klotho gene expression. Circulation 2004; 109:1776–1782. 23. Galitzer H, Ben-Dov IZ, Silver J, et al. Parathyroid cell resistance to fibroblast growth factor 23 in secondary hyperparathyroidism of chronic kidney disease. Kidney Int 2010; 77:211–218. 24. Larsson T, Nisbeth U, Ljunggren O, et al. Circulating concentration of FGF-23 increases as renal function declines in patients with 132 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. chronic kidney disease, but does not change in response to variation in phosphate intake in healthy volunteers. Kidney Int 2003; 64:2272–2279. Shigematsu T, Kazama JJ, Yamashita T, et al. Possible involvement of circulating fibroblast growth factor 23 in the development of secondary hyperparathyroidism associated with renal insufficiency. Am J Kidney Dis 2004; 44:250–256. Gutierrez O, Isakova T, Rhee E, et al. Fibroblast growth factor23 mitigates hyperphosphatemia but accentuates calcitriol deficiency in chronic kidney disease. J Am Soc Nephrol 2005; 16: 2205–2215. Fliser D, Kollerits B, Neyer U, et al. Fibroblast growth factor 23 (FGF23) predicts progression of chronic kidney disease: the Mild to Moderate Kidney Disease (MMKD) Study. J Am Soc Nephrol 2007; 18:2600–2608. Filler G, Liu D, Huang SH, et al. Impaired GFR is the most important determinant for FGF-23 increase in chronic kidney disease. Clin Biochem 2011; 44:435–437. Perwad F, Azam N, Zhang MY, et al. Dietary and serum phosphorus regulate fibroblast growth factor 23 expression and 1,25-dihydroxy vitamin D metabolism in mice. Endocrinology 2005; 146:5358–5364. Ferrari SL, Bonjour JP, Rizzoli R. Fibroblast growth factor-23 relationship to dietary phosphate and renal phosphate handling in healthy young men. J Clin Endocrinol Metab 2005; 90:1519–1524. Burnett SM, Gunawardene SC, Bringhurst FR, et al. Regulation of C-terminal and intact FGF-23 by dietary phosphate in men and women. J Bone Miner Res 2006; 21:1187–1196. Westerberg PA, Linde T, Wikstrom B, et al. Regulation of fibroblast growth factor-23 in chronic kidney disease. Nephrol Dial Transplant 2007; 22:3202–3207. Canalejo R, Canalejo A, Martinez-Moreno JM, et al. FGF23 fails to inhibit uremic parathyroid glands. J Am Soc Nephrol 2010; 21:1125– 1135. Nielsen PK, Feldt-Rasmussen U, Olgaard K. A direct effect in vitro of phosphate on PTH release from bovine parathyroid tissue slices but not from dispersed parathyroid cells. Nephrol Dial Transplant 1996; 11:1762–1768. Almaden Y, Hernandez A, Torregrosa V, et al. High phosphate level directly stimulates parathyroid hormone secretion and synthesis by human parathyroid tissue in vitro. J Am Soc Nephrol 1998; 9:1845– 1852. Evenepoel P, Meijers B, Viaene L, et al. Fibroblast growth factor23 in early chronic kidney disease: additional support in favor of a phosphate-centric paradigm for the pathogenesis of secondary hyperparathyroidism. Clin J Am Soc Nephrol 2010; 5: 1268–1276. Gutierrez OM, Mannstadt M, Isakova T, et al. Fibroblast growth factor 23 and mortality among patients undergoing hemodialysis. N Engl J Med 2008; 359:584–592. Finch NC, Syme H, Elliott J. Parathyroid hormone (PTH) concentrations in cats prior to the development of azotemia compared to cats remaining non-azotemic. J Am Vet Med Assoc; 2012; 241:1326–1335. King JN, Tasker S, Gunn-Moore DA, et al. Prognostic factors in cats with chronic kidney disease. J Vet Intern Med 2007; 21:906–916. Chakrabarti S, Syme HM, Elliott J. Clinicopathological variables predicting progression of azotemia in cats with chronic kidney disease. J Vet Intern Med 2012; 26:275–281. Yaphe W, Forrester SD. Renal secondary hyperparathyroidism— pathophysiology, diagnosis, and treatment. Compend Contin Educ Pract Vet 1994; 16:173–181. Barber P. Diagnosis and management of chronic renal failure in the cat. In Practice 2003; 25:306–313. Bertazzolo W, Toscani L, Calcaterra S, et al. Clinicopathological findings in five cats with paw calcification. J Feline Med Surg 2003; 5:11–17. Barber PJ. Parathyroid Gland Function in the Ageing Cat. London: University of London; 1998. Jackson HA. Resolution of metastatic calcification in the paws of a cat with successful dietary management of renal hyperparathyroidism. J Small Anim Pract 1998; 39:495–497. C Veterinary Emergency and Critical Care Society 2013, doi: 10.1111/vec.12032 Role of phosphorus in the pathophysiology of CKD 46. Kowalewich NJ, Hawkins EC. Calcinosis circumscripta involving the metatarsal region in a dog with chronic renal failure. Can Vet J 1992; 33:465–466. 47. Slatopolsky E, Caglar S, Pennell JP, et al. On the pathogenesis of hyperparathyroidism in chronic experimental renal insufficiency in the dog. J Clin Invest 1971; 50:492–499. 48. Slatopolsky E, Caglar S, Gradowska L, et al. On the prevention of secondary hyperparathyroidism in experimental chronic renal disease using “proportional reduction” of dietary phosphorus intake. Kidney Int 1972; 2:147–151. 49. Slatopolsky E, Bricker NS. The role of phosphorus restriction in the prevention of secondary hyperparathyroidism in chronic renal disease. Kidney Int 1973; 4:141–145. 50. Ross LA. Effect of dietary phosphorus restriction on the kidneys of cats with reduced renal mass. Am J Vet Res 1982; 43:1023–1026. 51. AAFCO. 2011, Official Publication. Atlanta: AAFCO Inc; 2011. 52. Ross SJ, Osborne CA, Kirk CA, et al. Clinical evaluation of dietary modification for treatment of spontaneous chronic kidney disease in cats. J Am Vet Med Assoc 2006; 229:949–957. 53. Barber PJ, Rawlings JM, Markwell PJ, et al. Effect of dietary phosphate restriction on renal secondary hyperparathyroidism in the cat. J Small Anim Pract 1999; 40:62–70. 54. Lopez-Hilker S, Dusso AS, Rapp NS, et al. Phosphorus restriction reverses hyperparathyroidism in uremia independent of changes in calcium and calcitriol. Am J Physiol 1990; 259:F432–F437. 55. Jacob F, Polzin DJ, Osborne CA, et al. Clinical evaluation of dietary modification for treatment of spontaneous chronic renal failure in dogs. J Am Vet Med Assoc 2002; 220:1163–1170. C Veterinary Emergency and Critical Care Society 2013, doi: 10.1111/vec.12032 56. Plantinga EA, Everts H, Kastelein AM, et al. Retrospective study of the survival of cats with acquired chronic renal insufficiency offered different commercial diets. Vet Rec 2005; 157: 185–187. 57. Elliott J, Rawlings JM, Markwell PJ, et al. Survival of cats with naturally occurring chronic renal failure: effect of dietary management. J Small Anim Pract 2000; 41:235–242. 58. Nagode LA. Nephrocalcinosis caused by hyperparathyroidism in progression of renal failure: treatment with calcitriol. Semin Vet Med Surg (Small Anim) 1992; 7:202–220. 59. Vétoquinol. Phosphatemia management in the treatment of chronic kidney disease, a Roundtable Discussion. Vétoquinol Academia, 2006. Available at: http://www.vetoquinol.ca/documents/ Quoi%20de%20neuf/Articles/Round%20table%20discussion.pdf. Accessed February 2013. 60. Brown SA, Rickertsen M, Sheldon S. Effects of an intestinal phosphorus binder on serum phosphorus and parathyroid hormone concentration in cats with reduced renal function. Int J Appl Res Vet M 2008; 6:155–160. 61. Roudebush P. Therapies for feline chronic kidney disease. What is the evidence? J Fel Med Surg 2009; 11:195–210. 62. Roudebush P, Polzin DJ, Adams LG, et al. An evidence-based review of therapies for canine chronic kidney disease. J Small Anim Pract 2010; 51:244–252. 63. Elliott J, Elliott D. Dietary therapy for feline chronic kidney disease. In: Pibot P, Biourge V, Elliott D. eds. Encyclopedia of Feline Clnical Nutrition. Ainargues, France: Aniwa SAS Ltd; 2008, pp. 411–445. 133
 0
0
Anuncio
Documentos relacionados



Descargar
Anuncio
Añadir este documento a la recogida (s)
Puede agregar este documento a su colección de estudio (s)
Iniciar sesión Disponible sólo para usuarios autorizadosAñadir a este documento guardado
Puede agregar este documento a su lista guardada
Iniciar sesión Disponible sólo para usuarios autorizados