Hipertensión Arterial Sistémica: Definición, Fisiopatología y Tratamiento
Anuncio

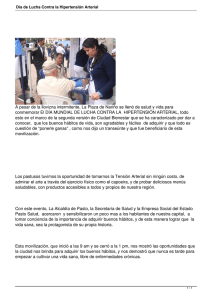
HIPERTENSIÓN ARTERIAL SISTÉMICA Dr. ALFREDO GONZALES SAAVEDRA DEFINICIÓN HIPERTENSIÓN ARTERIAL SISTÉMICA ENFERMEDAD Crónica Controlable Multifactorial caracterizada por aumento SOSTENIDO de Presión arterial sistólica (PS) por arriba de 120 mm Hg y/o Presión arterial diastólica (PD) igual o mayor a 80 mmHg. James PA, Oparil S, Carter BL, et al. Evidence based-guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; DOI:10.1001/jama.2013.284427. HIPERTENSIÓN ARTERIAL TRASCENDENCIA HIPERTENSIÓN ARTERIAL TRASCENDENCIA Principio de PASCAL PRESIÓN Ley de LAPLACE YOUNG NO ☺ T P ¿Es lo mismo que TENSIÓN ARTERIAL? Magnitud física que mide la fuerza por unidad de superficie Fuerza ejercida por la sangre en una superficie determinada de la pared interna (endotelio) del vasos sanguíneo por el que circula dicha sangre. cuantificamos T Presión RELATIVA (MANOMÉTRICA) PRESIÓN Y TENSIÓN SON VARIABLES DIRECTAMENTE PROPORCIONALES… pero NO son lo mismo. Presión ABSOLUTA Es la presión manométrica MÁS la presión atmosférica NO MODIFICABLES MODIFICABLES Carga genética Edad Raza (etnia) Estilo de vida Alimentación Actividad Física Tabaquismo Alcoholismo Estrés emocional TÉCNICA MÉTODOS Directo DETERMINADA POR FACTORES Indirecto Si la PRESIÓN AUMENTE entonces LA TENSIÓN AUMENTA PALPO AUSCULTATORIA Principio de BERNOULLI INVASIVO NO INVASIVO Mediante catéter intravascular Mediante un esfigmomanómetro Número de REYNOLDS Si el RADIO del vaso AUMENTA entonces LA TENSIÓN AUMENTA CLASIFICACIONES RECORDAR LOS ANEURISMAS NOM MENOS MAS Utilizado JNC-VIII HIPERTENSIÓN ARTERIAL FISIOPATOLOGÍA Fauci AS , Kasper DL, Branwald E. Harrison Principios de Medicina Interna, 17a edición Capitulo 241. FISIOPATOLOGÍA: SRAA PERFUSIÓN RENAL Riñón Hígado Angiotensinógeno RENINA PRESIÓN ARTERIAL Pulmón ECA Angiotensina II PRESIÓN ARTERIAL Resistencia vascular Volumen extracelular ANGIOTENSINA Células endoteliales Receptores AT Músculo liso vascular VASOCONSTRICCIÓN H 20 Capa glomerular GLÁNDULA SUPRARRENAL ALDOSTERONA Reabsorción de Na Nefrona De la Serna F. Novedades en el sistema renina-angiotensina Insuficiencia cardiaca Vol. 9 - Nº 1 (2014): 16-24 HIPERTENSIÓN ARTERIAL FISIOPATOLOGÍA: SRAA CARDIACO El angiotensinógeno y la renina provienen tanto de la producción local como de la circulación sistémica. La enzima convertidora de angiotensina (ECA) se expresa tanto en los miocitos cardíacos como en los fibroblastos. La síntesis de angiotensina II tiene lugar en el espacio intersticial y en el intracelular. La síntesis extracelular depende generalmente de la pro-renina y de la ECA. En miocitos cardíacos, la síntesis intracelular puede ocurrir en el citoplasma, mediada por renina y quimasa. La vía de síntesis dependiente de quimasa es la predominante en condiciones de hiperglucemia y resulta en un incremento muy importante de la concentración de angiotensina II intracelular, sin afectar a la concentración intersticial. De la Serna F. Novedades en el sistema renina-angiotensina Insuficiencia cardiaca Vol. 9 - Nº 1 (2014): 16-24 HIPERTENSIÓN ARTERIAL FISIOPATOLOGÍA: SRAA CARDIACO Los miocitos cardíacos y los fibroblastos responden a condiciones de hiperglucemia mediante la activación del SRA local. Las acciones de la angiotensina II intracelular no son bloqueadas por los antagonistas de los receptores de angiotensina (BRA), que solo serían eficaces para la angiotensina II extracelular producida por los fibroblastos cardíacos, mientras que los inhibidores de la ECA bloquearían la síntesis de angiotensina II de los fibroblastos. La angiotensina II intracelular en los miocitos cardíacos podría no ser susceptible de ninguno de estos agentes, sugiriendo sólo una parcial eficacia de los fármacos en condiciones de hiperglucemia. Un inhibidor de la renina podría tener mejores resultados terapéuticos en condiciones donde se activara el SRA intracelular. De la Serna F. Novedades en el sistema renina-angiotensina Insuficiencia cardiaca Vol. 9 - Nº 1 (2014): 16-24 Singh M, et al. Hypertension and Hypertensive Heart Disease: Pathogenesis and Clinical Physiology of Hypertension Cardiol Clin 28 (2010) 545–559. HIPERTENSIÓN ARTERIAL CLASIFICACIÓN ETIOLOGÍA HIPERTENSIÓN ARTERIAL SISTÉMICA ESENCIAL O PRIMARIA 90-95% SECUNDARIA 5-10% ESTABLE URGENCIA HIPERTENSIVA CRISIS HIPERTENSIVA EMERGENCIA HIPERTENSIVA Fauci AS , Kasper DL, Branwald E. Harrison Principios de Medicina Interna, 17a edición Capitulo 241. PRESIÓN ARTERIAL CUANTIFICACIÓN Ogedegbe G, et al. Hypertension and Hypertensive Heart Disease: Principles and Techniques of Blood Pressure Measurement Cardiol Clin 28 (2010) 545–559. Tratamiento TRATAMIENTO NO FARMACOLÓGICO ABORDAJE TRATAMIENTO FARMACOLOGICO Si se excluye a los afroamericanos, en la poblacion general, incluyendo a los diabeticos, el tratamiento inicial debe incluir uno de los siguientes fármacos: Diurético tipo tiazida Bloquedor de los canales de calcio Inhibidor de la enzima convertidora de angiotensina Antagonista del receptor de angiotensina II James PA, Oparil S, Carter BL, et al. Evidence based-guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; DOI:10.1001/jama.2013.284427. JNC-8 RECOMENDACION #6 Las 4 clases de fármacos recomendados tienen efectos comparables sobre la mortalidad global y los eventos cardiovasculares, cerebrovasculares y renales Tiazidas ˃ EFECTIVIDAD IECA ˃ MEJORÍA EN FALLA CARDIACA BCC JNC-8 RECOMENDACION #6 NO se recomiendan como fármacos de primeral línea Beta bloqueadores Alfa antagonistas • Mayor asociación a muerte por causas cardiovasculares, infarto de miocardio o EVC, en comparación con un ARA • Principalmente por aumento en el EVC • Peores resultados cerebrovasculares, de insuficiencia cardiaca y eventos cardiovasculares combinados en comparación con un diurético. James PA, Oparil S, Carter BL, et al. Evidence based-guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; DOI:10.1001/jama.2013.284427. JNC-8 RECOMENDACION #6 NO se recomiendan como fármacos de primeral línea Diuréticos de asa • Furosemida Antagonistas del receptor de aldosterona • Espironolactona Bloqueadores adrenérgicos duales • Carvedilol Agonistas adrenergicos centrales α-2 • Clonidina Vasodilatadores directos • Hidralazina JNC-8 RECOMENDACION #7 En la poblacion de pacientes afroamericanos el tratamiento antihipertensivo inicial debe incluir un bloqueador de los canales de calcio o diuretico tipo tiazida B SIN diabetes C CON diabetes James PA, Oparil S, Carter BL, et al. Evidence based-guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; DOI:10.1001/jama.2013.284427. JNC-8 RECOMENDACION #8 En la población de 18 años o mas con enfermedad renal crónica e hipertensión, el tratamiento antihipertensivo inicial (o agregado) debe incluir un IECA o un ARA para mejorar los eventos renales. B Esto se aplica a todos los pacientes con enfermedad renal crónica e hipertensión, independientemente del grupo étnico o de la presencia de diabetes James PA, Oparil S, Carter BL, et al. Evidence based-guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; DOI:10.1001/jama.2013.284427. JNC-8 RECOMENDACION #9 El principal objetivo del tratamiento es alcanzar y mantener la presion arterial meta. Si esta no se alcanza en un mes de tratamiento, aumente la dosis de la droga inicial o agregue una segunda droga de las clases mencionadas en la recomendacion 6. El medico debe continuar ajustando el tratamiento hasta que se alcanza la presion arterial meta. Si esta no se alcanza aun, agregue y titule una tercera droga de la lista. No use un IECA y un ARA juntos. James PA, Oparil S, Carter BL, et al. Evidence based-guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; DOI:10.1001/jama.2013.284427. JNC-8 SELECCIÓN DEL FÁRMACO James PA, Oparil S, Carter BL, et al. Evidence based-guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; DOI:10.1001/jama.2013.284427. James PA, Oparil S, Carter BL, et al. Evidence based-guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; DOI:10.1001/jama.2013.284427. James PA, Oparil S, Carter BL, et al. Evidence based-guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; DOI:10.1001/jama.2013.284427. FÁRMACOS SELECCIÓN DEL INDICADO Ogedegbe G, et al. Hypertension and Hypertensive Heart Disease: Principles and Techniques of Blood Pressure Measurement Cardiol Clin 28 (2010) 545–559 FÁRMACOS SELECCIÓN DEL INDICADO COMBINACIONES Verde continuo: preferido Verde discontinuo: útil con limitaciones Negro: posible, menor evidencia Rojo: no recomendable. Prieto MA. Guías en el manejo de hipertensión. Semergen. 2014;40(Supl 4):2-10. Diuretics Low-dose thiazide diuretics may be used alone or in combination with other antihypertensive drugs. Thiazides inhibit the Na+/Cl– pump in the distal convoluted tubule and hence increase sodium excretion. In the long term, they also may act as vasodilators. Thiazides are safe, efficacious, inexpensive, and reduce clinical events. They provide additive blood pressure–lowering effects when combined with beta blockers, angiotensin-converting enzyme inhibitors (ACEIs), or angiotensin receptor blockers (ARBs). In contrast, addition of a diuretic to a calcium channel blocker is less effective. Usual doses of hydrochlorothiazide range from 6.25 to 50 mg/d. Owing to an increased incidence of metabolic side effects (hypokalemia, insulin resistance, increased cholesterol), higher doses generally are not recommended.