Journal http://jcn.sagepub.com/
of Child Neurology
Progressive Myelopathy Mimicking Subacute Combined Degeneration After Intrathecal
Chemotherapy
Youbin Yi, Hyung Jin Kang, Hee Young Shin and Keewon Kim
J Child Neurol published online 20 March 2014
DOI: 10.1177/0883073814527157
The online version of this article can be found at:
http://jcn.sagepub.com/content/early/2014/03/20/0883073814527157
Published by:
http://www.sagepublications.com
Additional services and information for Journal of Child Neurology can be found at:
Email Alerts: http://jcn.sagepub.com/cgi/alerts
Subscriptions: http://jcn.sagepub.com/subscriptions
Reprints: http://www.sagepub.com/journalsReprints.nav
Permissions: http://www.sagepub.com/journalsPermissions.nav
>> OnlineFirst Version of Record - Mar 20, 2014
What is This?
Downloaded from jcn.sagepub.com at UNIV OF ILLINOIS URBANA on August 22, 2014
Brief Communication
Progressive Myelopathy Mimicking
Subacute Combined Degeneration
After Intrathecal Chemotherapy
Journal of Child Neurology
1-4
ª The Author(s) 2014
Reprints and permission:
sagepub.com/journalsPermissions.nav
DOI: 10.1177/0883073814527157
jcn.sagepub.com
Youbin Yi, MD, MS1, Hyung Jin Kang, MD, PhD2,
Hee Young Shin, MD, PhD2, and Keewon Kim, MD, MS1,3
Abstract
Intrathecal chemotherapy including methotrexate is well documented for neurotoxicity of diverse clinical manifestation. Acute or
chronic leukoencephalopathy is the most common type of methotrexate-induced neurotoxicity, and subacute myelopathy is rare.
Although its pathogenesis is not fully understood, it is postulated that direct damage of methotrexate to the central nervous
system plays a major part and elevated levels of homocysteine and its excitatory amino acid neurotransmitter metabolites (homocysteic acid and cysteine sulfinic acid) could mediate, in part, MTX-associated neurotoxicity. On the while, subacute combined
degeneration is a progressive degeneration of the dorsal and lateral columns of the spinal cord, mostly due to vitamin B12
deficiency. The authors report a case of a 15-year-old boy with Burkitt leukemia who developed progressive myelopathy after
intrathecal triple therapy (methotrexate, cytarabine, and hydrocortisone) whose clinical and radiologic features were compatible
with subacute combined degeneration. The pathogenic mechanism could be explained by biochemical alteration by methotrexate
and a possible treatment strategy was discussed.
Keywords
intrathecal, methotrexate, subacute combined degeneration
Received October 12, 2013. Received revised December 13, 2013. Accepted for publication February 13, 2014.
Intrathecal triple therapy, which is composed of methotrexate,
cytarabine, and hydrocortisone, is widely used in children for
the treatment of malignancies involving the central nervous
system. It is also well known to be related to various degrees
of transient and permanent neurotoxicity.1 Acute or
chronic leukoencephalopathy is the most common type of
methotrexate-induced neurotoxicity, and subacute myelopathy is rare.
Subacute combined degeneration, on the other hand, is a
progressive disease that shows characteristic ataxic features
with diminished sense of pressure, vibration, and touch. It
usually occurs due to a deficiency of vitamin B12, but also that
of copper.2,3 To the authors’ knowledge, chemotherapyinduced neurotoxicity whose magnetic resonance image (MRI)
findings mimic subacute combined degeneration is rare and
there have been no such reports in pediatric patients.
Here we report a case of intrathecal triple therapy–induced
progressive myelopathy in a child with Burkitt leukemia
whose magnetic resonance image showed findings resembling
subacute combined degeneration. We have also reviewed
the literature for suggested pathogeneses and discussions of
possible treatments.
Case Report
A 15-year-old boy was diagnosed with Burkitt leukemia with
central nervous system involvement in May 2011. The initial
white blood cell count was 11 900/mL. He underwent multiple
courses of systemic chemotherapy, with a session of 70 mg of
intrathecal cytarabine and 35 mg of hydrocortisone followed by
a total of 8 rounds of intrathecal triple therapy of 15 mg of
methotrexate, 30 mg of cytarabine, and 15 mg of hydrocortisone. The systemic chemotherapy he received comprised
1
Department of Rehabilitation Medicine, Seoul National University Hospital,
Seoul, Republic of Korea
2
Department of Pediatrics, Cancer Research Institute, Seoul National
University College of Medicine, Seoul, Republic of Korea
3
Department of Biomedical Engineering, Seoul National University College of
Medicine, Seoul, Republic of Korea
Corresponding Author:
Keewon Kim, MD, MS, Department of Rehabilitation Medicine, Seoul National
University College of Medicine, Seoul National University Hospital, 101
Daehak-ro, Jongro-gu, Seoul, 110-744, South Korea.
Email: [email protected]
Downloaded from jcn.sagepub.com at UNIV OF ILLINOIS URBANA on August 22, 2014
2
Journal of Child Neurology
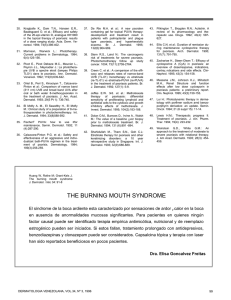
Figure 1. Magnetic resonance images (MRIs) on T1- (A, C) and T2-weighted images (B, D) show diffuse high signal intensities along the whole
spinal cord. T2-weighted axial images at C2 (E), T4 (F), and T10 (G) levels respectively show high signal intensities on the dorsal columns, which
resemble typical findings of subacute combined degeneration.
1 cycle of cyclophosphamide, vincristine, and prednisolone;
2 cycles of cyclophosphamide, vincristine, prednisolone, doxorubicin, and methotrexate; and 1 cycle of etoposide with
high-dose cytarabine. In addition, he underwent 2 sessions
of high-dose systemic methotrexate of 14 g.
Five months from the onset of the disease, after the 8th
round of intrathecal chemotherapy, a second isolated central
nervous system relapse was proven by positive cerebrospinal
fluid cytology. Another round of intrathecal triple therapy was
instilled, and the cerebrospinal fluid cytology converted to negative. Two more rounds of intrathecal triple therapy followed.
Between the 10th and 11th round of intrathecal chemotherapy,
he started to feel difficulty urinating. He subsequently developed gait ataxia and bilateral lower extremity weakness. His
proprioception and sense of light touch were decreased in the
bilateral lower extremities. Cerebellar function tests were
normal. Nine days after the symptom onset, the 11th intrathecal
triple therapy was administered. After that, magnetic resonance
imaging revealed diffuse high signal intensities along the
dorsal columns of the whole spinal cord on T2-weighted
images, which resembled typical findings of subacute combined degeneration (Figure 1). Because his serum vitamin
B12 was normal (3354 ng/L) and serum copper was decreased
(524 mg/L), copper (II) sulfate pentahydrate 4 mL was given over
15 minutes intravenously based on the suspicion that reduced
copper level might have induced his neurologic condition.
In spite of copper supplementation, his symptoms worsened.
On the 7th day of copper supplementation, the 27th day from
the symptom onset, bilateral facial palsy and decreased facial
sensation developed. Nerve conduction studies revealed bilateral
Downloaded from jcn.sagepub.com at UNIV OF ILLINOIS URBANA on August 22, 2014
Yi et al
3
facial neuropathy and there were no responses on the bilateral
blink reflex test. Magnetic resonance image revealed bilateral
symmetric enhancement of the facial nerve, which was compatible with chemotherapy-induced cranial neuropathy. His
hypesthesia and weakness progressed to the upper extremities
by 15 days after the start of the copper supplementation and he
became unable to walk in the following 15 days. Nerve conduction studies showed combined peripheral lesions of generalized sensorimotor peripheral neuropathy.
Fifty-nine days after the onset of the urinary and gait disturbance, left third cranial nerve palsy and dysphagia developed.
He also complained of mild dyspnea, but his chest radiographs
showed no specific lung lesions. Follow-up magnetic resonance images on the 61st day from the symptom onset showed
an increased extent of the high signal intensities to the bilateral
lateral columns of the thoracic spinal cord on T2-weighted imaging. Two days after the onset of dyspnea, he was transferred to
the intensive care unit because of respiratory failure induced by
pneumonia. He expired because of respiratory failure 9 months
after the onset of the leukemia.
Discussion
We documented a case of progressive myelopathy that exhibited the typical radiologic characteristics of subacute combined
degeneration. The patient was diagnosed as Burkitt leukemia
and treated with several rounds of intrathecal triple therapy and
systemic chemotherapy. Because the magnetic resonance
images resemble subacute combined degeneration with T2
high signal intensities in the dorsal and lateral columns of the
spinal cord, laboratory tests for vitamin B12 and copper were
performed. The serum level of vitamin B12 was normal and that
of copper was only mildly decreased. Copper administration
was carried out, but it did not help prevent progression of his
neurologic symptoms. His neurologic symptoms deteriorated
over time. After 11 rounds of intrathecal triple therapy, on the
224th day from the first intrathecal triple therapy administration and the 84th day from the last one, the patient expired not
from malignancy but from respiratory failure, supposedly
associated with neurologic deterioration.
Methotrexate is a folate analogue that is used in the treatment of various malignant diseases including acute lymphoblastic leukemia. It certainly plays a critical role in treating
those threatening diseases but also increases the risk of neurotoxicity, which might be transient but might also be irreversible
and severe enough to even cause death.4 Subacute combined
degeneration, on the other hand, refers to the progressive
degeneration of the posterior and lateral columns of the spinal
cord, and it can also involve the brain and peripheral nervous
system.5 The direct cause of subacute combined degeneration
is defective transmethylation of myelin6 caused by dysfunction
of the methyl-transfer pathway. In other words, vitamin B12
deficiency, the main cause of subacute combined degeneration,
causes lack of methionine and, in turn, S-adenosylmethionine,
a universal methyl-group donor in the brain.7 Methotrexate and
methotrexate polyglutamates are known to inhibit the enzyme
dihydrofolate reductase and thymidylate synthase.8,9 This leads
to a deficiency of 5-methyltetrahydrofolate, which is a donor of
the methyl group for producing methionine and, in turn, S-adenosylmethionine, as in subacute combined degeneration.
Therefore, intrathecal methotrexate treatment can induce
demyelination of the central nervous system, which is identical
to that from subacute combined degeneration.
In our patient, however, it has not been proven whether
intrathecal methotrexate was the actual cause of his neurologic
deterioration. Although intravenous replacement of copper did
not ameliorate his condition, nutritional deficiency might have
contributed to it. Paraneoplastic neurologic disorders should be
also ruled out. In this patient, antineuronal antibodies were not
screened because his neurologic symptoms did not follow
typical features of paraneoplastic neurologic disorders.
Nevertheless, it was highly probable, in retrospective speculation, that intrathecal methotrexate was the major cause of his
neurologic deterioration, given that his radiologic findings
were typical of subacute combined degeneration, vitamin B12
level was in normal range, and methotrexate and vitamin B12
share biochemical pathways in transmethylation of myelin.
Importantly, clinicians should consider the possibility of
methotrexate-induced neurotoxicity when they encounter a magnetic resonance image showing subacute combined degeneration
features because these patients may need a different treatment
strategy. Although our case showed a vitamin B12 level in the
normal range and no cobalamin supplementation was administered, recent case reports in adult patients have shown improved
neurologic symptoms after high-dose multiple folate metabolite
substitution, including S-adenosylmethionine and methionine as
well as folate and cobalamin10 in spite of a normal level of
cobalamin. Considering the mechanism of methotrexateinduced neurotoxicity and a previous report of elevated homocysteine in the cerebrospinal fluid of methotrexate-treated pediatric patients,11 a deficiency of S-adenosylmethionine and
methionine is implicated in the occurrence of subacute combined degeneration-mimicking neurotoxicity. Based on what is
known, immediate discontinuation of intrathecal methotrexate
treatment and supplementation of methionine or S-adenosylmethionine would be the best treatment option. However, further
research is required to establish an effective and definite
treatment protocol.
In conclusion, occurrence of typical features of subacute
combined degeneration, clinically and radiologically, after
intrathecal methotrexate treatment is not widely known. This
is the first report of a pediatric case of the condition. It is of
clinical significance for physicians to recognize the possibility
of developing subacute combined degeneration-like neurologic
deficit during intrathecal chemotherapy because changing
chemotherapeutic regimen and supplementing folate metabolites might recover the condition.
Author Contributions
YBY conceptualized and drafted the first manuscript. HJK, HYS, and
KWK reviewed and edited the manuscript. KWK supervised the
study.
Downloaded from jcn.sagepub.com at UNIV OF ILLINOIS URBANA on August 22, 2014
4
Journal of Child Neurology
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to
the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship,
and/or publication of this article.
Ethical Approval
Institutional review board approval and informed consent were
waived per our institutional policy for publishing retrospective case
reports with no patient identifier.
References
1. Reddy AT, Witek K. Neurologic complications of chemotherapy for
children with cancer. Curr Neurol Neurosci Rep. 2003;3:137-142.
2. Winston GP, Jaiser SR. Copper deficiency myelopathy and subacute combined degeneration of the cord—why is the phenotype so
similar? Med Hypotheses. 2008;71:229-236.
3. Ferrara JM, Skeen MB, Edwards NJ, Gray L, Massey EW.
Subacute combined degeneration due to copper deficiency. J
Neuroimaging. 2007;17:375-377.
4. Vezmar S, Becker A, Bode U, Jaehde U. Biochemical and clinical
aspects of methotrexate neurotoxicity. Chemotherapy. 2003;49:
92-104.
5. Russell JSR, Batten F, Collier J. Subacute combined degeneration
of the spinal cord. Brain. 1900;23:39-110.
6. Surtees R. Biochemical pathogenesis of subacute combined
degeneration of the spinal cord and brain. J Inherit Metab Dis.
1993;16:762-770.
7. Cantoni GL. Biological methylation: selected aspects. Annu Rev
Biochem. 1975;44:435-451.
8. Allegra C, Chabner B, Drake J, Lutz R, Rodbard D, Jolivet J.
Enhanced inhibition of thymidylate synthase by methotrexate
polyglutamates. J Biol Chem. 1985;260:9720-9726.
9. McKeever M, Weir D, Molloy A, Scott J. Betaine-homocysteine
methyltransferase: organ distribution in man, pig and rat and
subcellular distribution in the rat. Clin Sci (Lond). 1991;81:551.
10. Ackermann R, Semmler A, Maurer G, et al. Methotrexateinduced myelopathy responsive to substitution of multiple folate
metabolites. J Neurooncol. 2010;97:425-427.
11. Quinn CT, Griener JC, Bottiglieri T, Hyland K, Farrow A,
Kamen BA. Elevation of homocysteine and excitatory amino acid
neurotransmitters in the CSF of children who receive methotrexate for the treatment of cancer. J Clin Oncol. 1997;15:2800-2806.
Downloaded from jcn.sagepub.com at UNIV OF ILLINOIS URBANA on August 22, 2014
 0
0