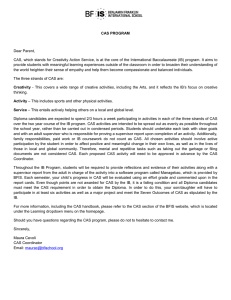
Genetic and Diagnostic Marker Research in Childhood Apraxia of Speech Lawrence D. Shriberg Waisman Center University of Wisconsin-Madison Program Committee Session: Link Between Theory and Practice American Speech-Language-Hearing Association National Convention, San Diego, CA November 18, 2011 Acknowledgments Waisman Center Phonology Project University of Wisconsin-Madison Collaborators Marios Fourakis Jane McSweeny Leonard Abbeduto Kathy Jakielski Sheryl Hall Alison Scheer-Cohen Kirrie Ballard Barbara Lewis Heather Karlsson Sonja Tatro Adriane Baylis Christopher Moore Joan Kwiatkowski Christie Tilkens Stephen Camarata Rhea Paul Heather Lohmeier David Wilson Thomas Campbell Nancy Potter Kathy Chapman Sharynne McCleod Biostatistics and Genomics Peter Flipsen, Jr. Angela Morgan Roger Brown Gordana Raca Morton Gernsbacher Edythe Strand David Dimmock Gregory Rice Hill Goldsmith Bruce Tomblin Craig Jackson Shelley Smith Jordan Green Erin Wilson Jennifer Laffin Elizabeth Worthey This research is supported by the National Institute on Deafness and Other Communication Disorders [DC00496], an American Recovery and Reinvestment Act Supplement Grant, and a core grant to the Waisman Center from the National Institute of Child Health and Development [HD03352]. Topics I. Speech Sound Disorders (SSD) A. Multicausal Perspective B. Genetic Findings in Speech Delay II. Childhood Apraxia of Speech (CAS) A. Neurogenetic Perspective B. Genetic Findings C. Diagnostic Findings Diagnosis: Childhood Apraxia of Speech Topics I. Speech Sound Disorders (SSD) A. Multicausal Perspective B. Genetic Findings in Speech Delay II. Childhood Apraxia of Speech (CAS) A. Neurogenetic Perspective B. Genetic Findings C. Diagnostic Findings Speech Disorders Classification System (SDCS) Genetic and Environmental Risk and Protective Factors I. Etiological Processes (Distal Causes) Neurodevelopmental Substrates II. Speech Processes (Proximal Causes) Encoding/Memory *Transcoding **Execution (Representational) (Planning/Programming) (Neuromotor) III. Clinical Typology Speech Errors (SE) Speech Delay (SD) Speech DelayGenetic (SD-GEN) **Motor Speech (SE-/r/) *Motor Speech DisorderApraxia Of Speech (MSD-AOS) (MSD-DYS) Motor Speech DisorderNot Otherwise Specified (MSD-NOS) -- -- -- -- ------ -- -- -- -- ------ -- -- -- -- ------ -- -- -- -- ------ -- -- -- -- ------ -- -- -- -- ------ -- -- -- -- ------ -- -- -- -- ------ -- -- -- -- ------ -- -- -- -- ------ Speech DelayDevelopmental Psychosocial Involvement (SD-DPI) Speech Errors /s/ Speech Errors /r/ (SE-/s/) --- --- --- --- --- -- -- -- -- ------ --- --- --- --- --- -- -- -- -- ------ Speech DelayOtits Media With Effusion (SD-OME) Motor Speech Disorder (MSD) DisorderDysarthria IV. Diagnostic Markers --- --- --- --- --- V. Phenotypes --- --- --- --- --- Topics I. Speech Sound Disorders (SSD) A. Multicausal Perspective B. Genetic Findings in Speech Delay II. Childhood Apraxia of Speech (CAS) A. Neurogenetic Perspective B. Genetic Findings C. Diagnostic Findings Regions of Interest and Candidate Genes for Speech Delaya Chromosome Candidate Gene Group 1 1p34-36 DYX8 Pennington 3 3p12-q13 ROBO1 (DYX5) Lewis 6 6p22-p21 DCDC2, KIAA0319 Pennington; Rice 15q21 DYX1C1 (EKN1) Pennington 15 aBased ROI on genetic research in verbal trait disorders (speech, language, reading) Recent Genetic Findings for Speech Sound Disorders (SSD)a,b Chromosome Gene 3 ROBO2 11 BDNF 15 DYX1C1 a Endophenotype c Nonsense Multisyllabic Words Words X X Phenotype SSD X X X X X Lewis et al. (2011) Speech Sound Disorders (SSD) includes Speech Delay (SD) and possible motor speech disorders c X = Significant p value b Summary of Molecular Genetic Findings in Speech Sound Disorders To date, Regions of Interest (ROIs) and/or candidate genes for Speech Sound Disorders have been reported for 5 of the 22 autosomes: 1, 3, 6, 11,15. Two of the five genes have been associated with a binary phenotype (Speech Sound Disorders) that includes both Speech Delay and possibly motor speech disorder. Topics I. Speech Sound Disorders (SSD) A. Multicausal Perspective B. Genetic Findings in Speech Delay II. Childhood Apraxia of Speech (CAS) A. Neurogenetic Perspective B. Genetic Findings C. Diagnostic Findings Complex Neurodevelopmental Disorders Reporting ‘Significant’ Speech Delay/CAS Autism Chromosome Translocations Down syndrome (Trisomy 21) Rolandic Epilepsy Fragile X syndrome (FMR1) Joubert syndrome (CEP290; AHI1) Galactosemia Rett syndrome (MeCP2) Russell-Silver syndrome (FOXP2) Velocardiofacial syndrome (22q11.2 deletion) Topics I. Speech Sound Disorders (SSD) A. Multicausal Perspective B. Genetic Findings II. Childhood Apraxia of Speech (CAS) A. Neurogenetic Perspective B. Genetic Findings C. Diagnostic Findings III. Collaborative Genetics Research The Iconic Pedigree FOXP2: KE Family Studiesa Genotype: Half the family members in each generation have a point mutation in FOXP2 (7q31) Biomarker: None to date Endophenotype: Affected members had low scores on a nonword repetition task Phenotype: Affected members received services for a severe speech sound disorder consistent with CAS Affected members had low scores on a task assessing oral motor movements Other: a Many affected members had low verbal and performance IQs, language impairments, other involvements Over two decades of continuous research. Detailed summaries of findings available in many sources. FOXP2 and CAS in Four Other Families MacDermot et al. (2005) reported that of 49 probands in Europe, Australia, or the United States with reported apraxia of speech who were screened for FOXP2 mutations, 1 proband (i.e., approximately 2% attributable risk), his affected sister and their mother had a heterozygous nonsense mutation in FOXP2. The 4-year-old boy had a developmental delay in speech, language, and social skills. He communicated mainly using single words and was unable to repeat multisyllabic words. His 20-month-old sister had a history of motor and oropharyngeal dyspraxia, was unable to speak any words, could not identify objects, and had poor vocalization. His mother reported a history of speech delay in childhood and showed severe problems in communication, with poor speech clarity and simple grammatical constructions. FOXP2 and CAS in Four Other Families Zeesman et al. (2006) reported a 5-year-old girl with an interstitial deletion of paternally-derived chromosome 7q31.2-q32.2 encompassing the FOXP2 gene. This girl has a severe communication disorder with evidence of oromotor dyspraxia and mild developmental delay. She was unable to cough, sneeze, or laugh spontaneously. This child also has dysmorphic features, including microcephaly, brachycephaly, small nose, long philtrum, and down-turned corners of the mouth. These features are similar to those for the child described in Sarda et al. (1988) and the child “CS” reported in Lai et al. (2000) who had a translocation disrupting FOXP2. FOXP2 and CAS in Four Other Families Shriberg et al. (2006) reported a de novo balanced 7;13 translocation in a 50-year old mother and her 19-year-old daughter Mother and daughter have been treated for apraxia of speech since early childhood Mother and daughter have a broad range of mild cognitive impairments and severe speech and language deficits similar to those reported for affected members of the KE family Mother and daughter have speech profiles consistent with both apraxia and spastic dysarthria. FOXP2 and CAS in Four Other Families Rice et al. (in press) report a de novo deletion of FOXP2 in a 24-year-old mother and her 4-year-old son. Mother and son treated for apraxia of speech since early childhood Mother and son have cognitive impairments and severe speech and language deficits similar to those reported for affected members of the KE family and to those reported for a mother and daughter with a de novo balanced 7;13 translocation affecting FOXP2 (Shriberg et al., 2006) Mother’s speech profile is consistent with both apraxia and spastic dysarthria; son severe apraxia Son does not cough or laugh spontaneously Genetic Research in CAS FOXP2 Studies reporting Speech Delay (Zhao et al., 2010) Studies of downstream genes (Roll et al., 2010) Studies with animal models (birds, mammals) FOXP1 Carr et al. (2010); Hamdan et al. (2010) Horn et al. (2010); Pariani (2009) FOXG1 Brunetti-Pierri et al. (2011) ELP4 Pal et al. (2010) RAI1 Kogan et al. (2009) Some recent literature reviews: Bishop (2009); Fisher & Scharff (2009); Grigorenko (2009); Ramus & Fisher (2009); Vernes & Fisher (2009); Lewis (2010); Newbury & Monaco (2010); Newbury, Fisher, & Monaco (2010); Shriberg (2010) Topics I. Speech Sound Disorders (SSD) A. Multicausal Perspective B. Genetic Findings in Speech Delay II. Childhood Apraxia of Speech (CAS) A. Neurogenetic Perspective B. Genetic Findings C. Diagnostic Findings Design Research in Speech Sound Disorders Speech Sound Disorders (SSD) Clinical Typology: Speech DelayGenetic (SD-GEN) Speech Processes: Diagnostic Markers: Speech Delay (SD) Speech DelayOtits Media With Effusion (SD-OME) Speech DelayDevelopmental Psychosocial Involvement (SD-DPI) Speech Errors (SE) Speech Errors /s/ Speech Errors /r/ (SE-/s/) (SE-/r/) Motor Speech Disorder (MSD) Motor Speech Disorder ApraxiaOf Speech (MSD-AOS) Motor Speech DisorderDysarthria (MSD-DYS) Encoding/Memory Transcoding Execution (Representational) (Planning/Programming) (Neuromotor) Motor Speech DisorderNot Otherwise Specified (MSD-NOS) Current Diagnostic Markers and Classification Criteria for CASa “For a judgment of the presence of CAS, the child had to exhibit vowel distortions and at least 3 of the following 10 characteristics in at least 3 of the tasks: difficulty achieving initial articulatory configurations or transitionary movement gestures equal stress or lexical stress errors distorted substitutions syllable segregation groping intrusive schwa voicing errors slow rate slow DDK increased difficulty with multisyllabic words” a Shriberg, L.D., Potter, N.L., & Strand, E.A (2011). Speech Disorders Classification System (SDCS) Candidate Diagnostic Markers for Eight Subtypes of SSDa Componentsb Organized Ten Linguistic Domains Analytics (TLDA) Competence, Precision, Stability Analytics (CPSA) Operationalized Madison Speech Assessment Protocol (MSAP) Procedures for transcription, prosody-voice analyses, and acoustic analyses Standardized Reference Database (200 typical speakers, 3 to 80 years old) a Candidate markers selected from pediatric and adult literature in speech sound disorders of known and unknown origin. b All components processed in the PEPPER software environment. Ten Linguistic Domains Analytic (TLDA) for Speech Sound Disorders (SSD) TLDA Speech Delay SD-GEN SD-OME Segmental 1. Vowels 2. Consonants 3. Vowels and Consonants Suprasegmental Prosody 4. Phrasing 5. Rate 6. Stress Voice 7. Loudness 8. Pitch 9. Laryngeal Quality 10. Resonance Quality SD-DPI Motor Speech Disorders MSD-NOS MSD-AOS MSD-DYS Madison Speech Assessment Protocol: Three Analytic Constructs Competence (Normative; Mastery) Precision Stability (Spatiotemporal Accuracy) (Spatiotemporal Consistency) Speech Disorders Classification System (SDCS) Candidate Diagnostic Markers for Eight Subtypes of SSDa Componentsb Organized Ten Linguistic Domains Analytics (TLDA) Competence, Precision, Stability Analytics (CPSA) Operationalized Madison Speech Assessment Protocol (MSAP) Procedures for transcription, prosody-voice analyses, and acoustic analyses Standardized Reference Database (200 typical speakers, 3 to 80 years old) a Candidate markers selected from pediatric and adult literature in speech sound disorders of known and unknown origin. b All components processed in the PEPPER software environment. Madison Speech Assessment Protocol: Speech, Prosody, and Voice Tasks Four age-based protocols: Preschool, school-aged, adolescent, adult Each protocol includes 15 tasks; about 1 hour to administer Articulation Task DDK Task Challenging Word Tasks (3) Phonation Tasks (2) Challenging Phrase Task Stress Tasks (2) Consonant Task Vowel Tasks (3) Conversational Sample Madison Speech Assessment Protocol: Data Reduction PEPPER Environment Perceptual Narrow phonetic transcription Prosody-Voice Screening Profile Acoustic TF32-Active X Automated; high throughput Speech Disorders Classification System (SDCS) Candidate Diagnostic Markers for Eight Subtypes of SSDa Componentsb Organized Ten Linguistic Domains Analytics (TLDA) Competence, Precision, Stability Analytics (CPSA) Operationalized Madison Speech Assessment Protocol (MSAP) Procedures for transcription, prosody-voice analyses, and acoustic analyses Standardized Reference Database (200 typical speakers, 3 to 80 years old) a Candidate markers selected from pediatric and adult literature in speech sound disorders of known and unknown origin. b All components processed in the PEPPER software environment. Procedures to Code Participants as “Positive” for a Sign Using Reference Databases Z-scores are derived from participants’ raw scores on each continuous Competence, Precision, and Stability index using age-gender subgroups in the reference databases of typically developing speakers. Z-scores > 1.0 in conceptually designated direction meet criterion for ‘Positive’ (i.e., affected). Promising Diagnostic Signs for Motor Speech Disorder – Apraxia of Speech (MSD-AOS)a Segmental Precision Stability Vowels/Diphthongs Reduced Vowel Space Reduced Vowel Substitution Coefficients Increased Distorted Vowel Substitutions Less Precise Diphthongs Less Stable F1 Less Stable Vowel Duration Consonants Increased % of /j/ Deletions in Clusters Less Stable Sibilant Centroids Reduced SRT Transcoding Scores Suprasegmental Phrasing Increased % of Pauses Increased % of Inappropriate Pauses Rate Slower Speaking Rate Slower Articulation Rate Resonance Quality Lowered F2: High Vowels (Nasopharyngeal) a Bolded signs use acoustic methods Less Stable F2: High Vowels (Nasopharyngeal) cr 20 10 0 ss St ab D ur at io n e F1 ac le Sp ab we l St we l Vo Vo ed le uc ss of Participants Positive for Marker 90 Le R ed Le ea Percentage In se ap d pr P e op rc ria en t e t ag Pa e us o f Sl es ow er Ar t ic ul at io n R at Sl e ow er Sp ea ki ng Lo R at we e re d F2 :H ig h Vo we ls In Seven Candidate Diagnostic Markers of Apraxia of Speech 100 AOS (n = 47-53) SD (n = 22-24) 80 70 60 50 40 30 Per Participant Percentage of Positive Signs (7) of AOS Participants with Speech Delay Compared to Participants with Apraxia of Speech Speech Delay (n=22; ages 3-6 yrs) Control Group CAS_Idiopathic (n=26; ages 3-19 yrs) CAS_Neurogenetic (n=20; ages 5-50 yrs) Apraxia of Speech AOS (Neurologic) (n=7; ages 45-84 yrs) Per Participant Percentage of Positive Signs (7) of AOS Participants with Speech Delay Compared to Participants with Apraxia of Speech Speech Delay (n=22; ages 3-6 yrs) Control Group CAS_Idiopathic (n=21; ages 3-19 yrs) CAS_Neurogenetic (n=20; ages 5-50 yrs) Apraxia of Speech AOS (Neurologic) (n=7; ages 45-84 yrs) Per Participant Percentage of Positive Signs (7) of AOS Participants with Speech Delay Compared to Participants with Apraxia of Speech Speech Delay (n=22; ages 3-6 yrs) Control Group CAS_Idiopathic (n=21; ages 3-19 yrs) CAS_Neurogenetic (n=19; ages 5-50 yrs) Apraxia of Speech AOS (Neurologic) (n=7; ages 45-84 yrs) Per Participant Percentage of Positive Signs (7) of AOS Participants with Apraxia of Speech Compared to Participants with Speech Delay 90.5% Sensitivity MSD-NOS? 100.0% Sensitivity 94.7% Sensitivity Sensitivity for Combined AOS groups = 93.6% 77.3% Specificity Speech Delay (n=22; ages 3-6 yrs) Control Group CAS_Idiopathic (n=21; ages 3-19 yrs) CAS_Neurogenetic (n=19; ages 5-50 yrs) Apraxia of Speech AOS (Neurologic) (n=7; ages 45-84 yrs) Our Most Accurate ‘Checklist’ Criterion to Date to Phenotype a Speaker as Positive for Apraxia of Speech Checklist Criterion: Positive (affected) on any 4 or more of 7 signs of apraxia of speech Findings to date for 69 qualified participants: 22 Speech Delay; 47 apraxia of speech Sensitivity Specificity Positive Likelihood Ratio Negative Likelihood Ratio Odds Ratio 93.6% 77.3% 4.1 .08 50.7 Some Information on the Seven Most Discriminative Signs of MSD-AOS to Date Signs assess Vowels, Phrasing, Rate, and Resonance Specificity is the primary challenge because young children with Speech Delay are also less precise and less stable than age-matched typical speakers There currently is no one sign of AOS with sufficient diagnostic accuracy. As database expansions permit, the most discriminative signs of AOS are expected to vary by age, cognitive status, language status, speech severity, and causal context (i.e., idiopathic, neurogenetic, neurologic) Challenges in Diagnostic Assessment of CAS Using the MSAP Validity and reliability require a certain level of knowledge and skills in narrow phonetic transcription, prosody-voice coding, and acoustic analyses Biggest challenge to date is the large amount of missing data on the speech tasks Participants can not or will not do the task Participants can do the task, but they make errors on the non-target elements required for assessment of targets e.g., for formant measures of the vowel in a CVC word e.g., ‘bat’ Design Research in Speech Sound Disorders Speech Sound Disorders (SSD) Clinical Typology: Speech DelayGenetic (SD-GEN) Speech Processes: Diagnostic Markers: Speech Delay (SD) Speech DelayOtits Media With Effusion (SD-OME) Speech DelayDevelopmental Psychosocial Involvement (SD-DPI) Speech Errors (SE) Speech Errors /s/ Speech Errors /r/ (SE-/s/) (SE-/r/) Motor Speech Disorder (MSD) Motor Speech Disorder ApraxiaOf Speech (MSD-AOS) Motor Speech DisorderDysarthria (MSD-DYS) Encoding/Memory Transcoding Execution (Representational) (Planning/Programming) (Neuromotor) Motor Speech DisorderNot Otherwise Specified (MSD-NOS) Thanks . . . http://www.waisman.wisc.edu/phonology/ References Bishop, D. V. M. (2009). Genes, cognition, and communication: insights from neurodevelopmental disorders. The Year in Cognitive Neuroscience: Annals of the New York Academy of Sciences, 1156, 1-18. Brunetti-Pierri, N., Paciorkowski, A. R., Ciccone, R., Della Mina, E., Bonaglia, M. C., Borgatti, R.,... Stankiewicz, P. (2011). Duplications of FOXG1 in 14q12 are associated with developmental epilepsy, mental retardation and severe speech impairment. European Journal of Human Genetics, 19, 102-107. Carr, C. W., Moreno-De-Luca, D., Parker, C., Zimmerman, H. H., Ledbetter, N., Martin, C. L.,... Abdul-Rahman, O. A. (2010). Chiari I malformation, delayed gross motor skills, severe speech delay, and epileptiform discharges in a child with FOXP1 haplounsifficiency. European Journal of Human Genetics, 18, 1216-1220. Fisher, S. E. & Scharff, C. (2009). FOXP2 as a molecular window into speech and language. Trends in Genetics, 25, 166-177. Grigorenko, E. L. (2009). Speaking genes or genes for speaking? Deciphering the genetics of speech and language. The Journal of Child Psychology and Psychiatry, 50, 116-125. Hamdan, F. F., Daoud, H., Rochefort, D., Piton, A., Gauthier, J., Langlois, M.,...Michaud J. L. (2010). De novo mutations in FOXP1 in cases with intellectual disability, autism, and language impairment. The American Journal of Human Genetics, 87, 671-678. Horn, D., Kapeller, J., Rivera-Brugués, N., Moog, U., Lorenz-Depiereux, B., Eck, S.,...Strom, T. M. (2010). Identification of FOXP1 deletions in three unrelated patients with mental retardation and significant speech and language deficits. Human Mutation, 31, E1851-60. Kogan, J. M., Miller, E., & Ware, S. M. (2009). High resolution SNP based microarray mapping of mosaic supernumerary marker chromosomes 13 and 17: Delineating novel loci for apraxia. American Journal of Medical Genetics Part A, 149A: 887–893. Lai, C. S. L., Fisher, S. E., Hurst, J. A., Levy, E. R., Hodgson, S., Fox, M.,...Monaco, A. P. (2000). The SPCH1 region on human 7q31: Genomic characterization of the critical interval and localization of translocations associated with speech and language disorder. American Journal of Human Genetics, 67, 357–368. Lewis, B. (October, 2010). Genetic and neurological correlates of childhood apraxia of speech. Paper presented for the Childhood Apraxia of Speech Virtual Conference, University of Wisconsin-Eau Claire, Eau Claire, WI. References Lewis, B., Qiu, F., Freebairn, L., Avrich, A., Truitt, B., Raghavendra, R.,...Stein, C. (November, 2011). Candidate genes for Speech Sound Disorders. Poster presented at the Annual Convention of the American Speech-Language-Hearing Association, San Diego, CA. MacDermot, K. D., Bonora, E., Sykes, N., Coupe, A.-M., Lai, C. S. L., Vernes, S. C.,…Fisher, S. E. (2005). Identification of FOXP2 truncation as a novel cause of developmental speech and language deficits. American Journal of Human Genetics, 76, 1074–1080. Newbury, D. F., Fisher, S. E., & Monaco, A. P. (2010). Recent advances in the genetics of language impairment. Genome Medicine, 2, 6-13. Newbury, D. F. & Monaco, A. P. (2010). Genetic advances in the study of speech and language disorders. Neuron, 68, 309-320. Pal, D. K., Li, W., Clarke, T., Lieberman, P., & Strug, L. J. (2010). Pleiotropic effects of the 11p13 locus on developmental dyspraxia and EEG centrotemporal sharp waves. Genes, Brain, and Behavior, 9, 10041012. Pariani, M. J., Spencer, A., Grahan, J. M., & Rimoin, D. L. (2009). A 785 kb deletion of 3p14.1p13, including the FOXP1 gene, associated with speech delay, contractures, hypertonia and blepharophimosis. European Journal of Medical Genetics, 52, 123-127. Ramus, F. & Fisher, S. E. (2009). Genetics of language. In M. S. Gazzaniga (Ed.), The Cognitive Neurosciences IV (pp. 855-872). Cambridge, MA: MIT Press. Rice, G. M., Raca, G., Jakielski, K. J., Laffin, J. L., Iyama-Kurtycz, C. M., Hartley, S. L.,...Shriberg, L. D. (in press). Phenotype of FOXP2 Haploinsufficiency in a Mother and Son. American Journal of Medical Genetics: Part A. Roll, P., Vernes, S. C., Bruneau, N., Cillario, J., Ponsole-Lenfant, M., Massacrier, A.,...Szepetowski, P. (2010). Molecular networks implicated in speech-related disorders: FOXP2 regulates the SRPX2/uPAR complex. Human Molecular Genetics, 19, 4848-4860. Sarda, P., Turleau, C., Cabanis, M. O., Jalaguier, J., de Grouchy, J., & Bonnet, H. (1988). De le tion interstitielle du bras long du chromosome 7 [Interstitial deletion in the long arm of chromosome 7]. Annales de Ge ne tique, 31, 258–261. References Shriberg, L. D. (2010). A neurodevelopmental framework for research in Childhood Apraxia of Speech. In B. Maassen & P. van Lieshout, (Eds.), Speech Motor Control: New Developments in Basic and Applied Research. Oxford: Oxford University Press. Shriberg, L. D., Ballard, K. J., Tomblin, J. B., Duffy, J. R., Odell, K. H., & Williams, C. A. (2006). Speech, prosody, and voice characteristics of a mother and daughter with a 7;13 translocation affecting FOXP2. Journal of Speech, Language, and Hearing Research, 49, 500-525. Shriberg, L. D., Potter, N. L., & Strand, E. A. (2011). Prevalence and phenotype of childhood apraxia of speech in youth with galactosemia. Journal of Speech, Language, and Hearing Research, 54, 487-519. Vernes, S. C. & Fisher, S. E. (2009). Unravelling neurogenetic networks implicated in developmental language disorders. Biochemical Society Transactions, 37, 1263-1269. Zeesman, S., Nowaczyk, M. J. M., Teshima, I., Roberts, W., Ora Cardy, J., Brian, J.,...Scherer, S. W. (2006). Speech and language impairment and oromotor dyspraxia due to deletion of 7q31 that involves FOXP2. American Journal of Human Genetics, 140(A), 509–514. Zhao, Y., Ma, H., Wang, Y., Gao, H., Xi, C., Hua, T.,...Qiu, G. (2010). Association between FOXP2 gene and speech sound disorder in Chinese population. Psychiatry and Clinical Neurosciences, 64, 565-573. Madison Studies of Complex Neurodevelopmental Disorders Neurodevelopmental Disorder Completed Speech Sound Disorders Speech Delay (SD) Speech Errors (SE) Motor Speech Disorders MSD-CAS MSD-DYS MSD-NOS Autism: Verbal Yes Yes No No No Fragile X syndrome Yes Yes No No Yes Galactosemia Yes Yes Yes Yes Yes Joubert syndrome (1) Yes Yes Yes Yes ── Madison Studies of Complex Neurodevelopmental Disorders Neurodevelopmental Disorder In Process Speech Sound Disorders Speech Delay (SD) Speech Errors (SE) Motor Speech Disorders MSD-CAS MSD-DYS MSD-NOS Autism: Low Verbal ── ── ── ── ── Down syndrome ── ── ── ── ── Velocardiofacial syndrome ── ── ── ── ── Joubert syndrome ── ── ── ── ── Rolandic Epilepsy ── ── ── ── ── cr 20 10 0 ss St ab D ur at io n e F1 ac le Sp ab we l St we l Vo Vo ed le uc ss of Participants Positive for Marker 90 Le R ed Le ea Percentage In se ap d pr P e op rc ria en t e t ag Pa e us o f Sl es ow er Ar t ic ul at io n R at Sl e ow er Sp ea ki ng Lo R at we e re d F2 :H ig h Vo we ls In Seven Candidate Diagnostic Markers of Apraxia of Speech 100 AOS (n = 47-53) SD (n = 22-24) 80 70 60 50 40 30 Method Group 4: Neurogenetic and Idiopathic CAS Percentage of Consonants Correct (PCC) Age (yrs) n Neurogenetic Chromosome Region Deletion or Translocation M SD Range % Males M SD 4 13 3 11-16 25.0 76.3 5.0 Copy Number Variation 2 11 5 8-15 100.0 80.6 7.8 FOXP2 4 24 19 4-50 25.0 77.5 23.5 Galactosemia 8 5-16 75.0 68.2 19.4 Joubert Syndrome 1 11 ─ ─ 100.0 70.0 ─ Prader-Willi Syndrome 1 8 ─ ─ 0.0 92.2 ─ Subtotals Idiopathic 9 4 20 13 10 4-50 55.0 74.2 16.5 20 4-19 65.0 72.5 12.1 9 4