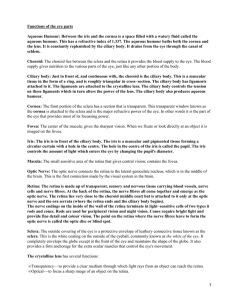
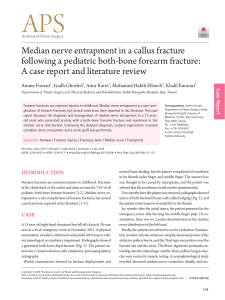
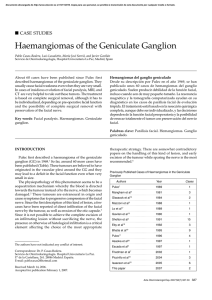
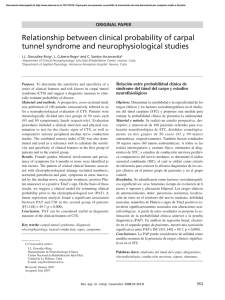
PROCEDURE 41 Nerve Transfers for Shoulder and Elbow Restoration After Upper Trunk Brachial Plexus Injuries Christopher J. Dy and Scott W. Wolfe PART 1: Double Nerve Transfer to Restore Elbow Flexion INDICATIONS •Injury to the upper trunk of the brachial plexus or musculocutaneous nerve (MCN) with resultant loss of elbow flexion •Inadequate recovery of elbow flexion following a minimum of 3 months observation with serial physical examinations and electromyograms (EMG) •Intact (at least M4, but ideally M5 strength with normal or near-normal EMG characteristics) strength of donor muscles (flexor carpi radialis [FCR]/pronator and flexor carpi ulnaris [FCU]/flexor digitorum profundus) (Schreiber et al., 2013) •Both the biceps and brachialis are targeted for reinnervation to maximize recovery of elbow flexion. EXAMINATION/IMAGING •Manual muscle testing of elbow flexion, forearm supination, wrist flexion, and extrinsic finger flexion •Normal or near-normal manual muscle strength of forearm pronation, wrist flexion, and digital and thumb flexion •EMG of the biceps and brachialis showing signs of recent denervation (insertional activity, fibrillations, sharp waves), absence of nascent motor unit potentials, and discreet or absent motor unit potentials (Schreiber et al., 2013) •EMG of the FCU, flexor carpi radialis, and flexor digitorum superficialis to ensure absence of denervation changes and normal/minimally decreased motor unit recruitment •In the context of brachial plexus injuries, computed tomography (CT) myelogram can be used to evaluate for pseudomeningoceles that would indicate preganglionic root avulsion injuries. Magnetic resonance imaging (MRI) of the brachial plexus can also be used to better characterize the anatomic aspects of injury, although it may not ultimately change the management plan. SURGICAL ANATOMY INDICATIONS PITFALLS •Lack of healthy donor nerves •Irreversible denervation atrophy of the biceps and brachialis muscles •Lack of familiarity with brachial plexus anatomy and variations •Lack of experience with microsurgical technique for internal neurolysis and nerve coaptation INDICATIONS CONTROVERSIES •Delay of greater than 1 year from injury •Distal avulsion of the biceps OR brachialis nerve fascicles from the muscle belly (not an absolute contraindication, but this has implications for prognosis—less robust muscle recovery is expected if direct muscle neurotization is performed) TREATMENT OPTIONS •Other potential donor nerves used to restore elbow flexion include intercostal nerves to the musculocutaneous nerve, spinal accessory nerve (with an intercalary graft), medial pectoral nerve, and thoracodorsal nerve •Nerve grafting (typically with sural nerve autograft) from an intact spinal nerve root or the upper trunk to the anterior division of the upper trunk, lateral cord, or musculocutaneous nerve •Free functioning gracilis neurovascular muscle transfer for chronic injuries •The MCN (C5/C6/C7) is the continuation of the lateral cord of the brachial plexus. After originating deep to the pectoralis minor, it innervates and pierces the coracobrachialis typically 7–8 cm distal to the acromion and passes between the biceps and brachialis muscles in the brachium. •The first motor branch (to the biceps) is 12–13 cm from the acromion. This branch typically bifurcates to innervate the long and short heads of the biceps. Alternatively, two or three separate branches to the heads of the biceps may arise from the MCN. A more distal fascicle to the biceps common belly is sometimes also present (Fig. 41.1). •The second motor branch (to the brachialis) is typically 5 cm distal to the biceps motor branch. There is usually a transversely oriented vascular pedicle to the biceps muscle at the bifurcation point of the brachialis nerve branch from the MCN (Fig. 41.2). •The preferred donor fascicle from the ulnar nerve contains fibers that primarily innervate the FCU. At this level of the brachium, no fascicle of the ulnar nerve is specific to a single muscle. Topographically, this fascicle is usually along the anterolateral quadrant of the ulnar nerve. We use a handheld nerve stimulator to confirm isolation 403 Descargado para Alexis Studer de Oya ([email protected]) en Mutua de Accidentes de Trabajo y Enfermedades Profecionales de la Seguridad Social de ClinicalKey.es por Elsevier en marzo 31, 2019. Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2019. Elsevier Inc. Todos los derechos reservados. 404 PROCEDURE 41 Nerve Transfers for Shoulder and Elbow Restoration After Upper Trunk Brachial Plexus Injuries Anterior Vascular pedicle Proximal Biceps Musculocutaneous nerve Brachialis Median nerve Ulnar nerve Ulnar nerve Lateral * Posterior * Posterior Anterior Median nerve Lateral Anterior Medial Medial FIG. 41.2 FIG. 41.1 POSITIONING PEARLS •If performing nerve transfers for the deltoid and supraspinatus during the same operative session, both surgeries can be performed in a semi-lateral position (on a beanbag) for staged access to the anterior brachium and posterior shoulder. STEP 1 PEARLS •Palpating the musculocutaneous nerve deep to the biceps (“rolling it” along the humerus) can be helpful to localize the initial intramuscular approach. It is also helpful to trace the musculocutaneous nerve from distal to proximal. It is important to stay within the proximal third of the brachium when starting this retrograde dissection, as the branch point for the biceps fascicle is typically halfway between the acromion and medial epicondyle and is at risk in a retrograde dissection. •The transversely oriented vascular pedicle from the brachial artery to the biceps muscle can be a helpful landmark to identify the brachialis fascicle from the musculocutaneous nerve (Fig. 41.3). •Longitudinally oriented epineural vessels can be helpful landmarks to identify intraneural cleavage planes when performing internal neurolysis. FIG. 41.3 of this fascicle. One or two fascicles can be used, but never more than 20% of the cross-sectional area of the ulnar nerve can be used. •The preferred donor fascicle from the median nerve is from the FCR and/or the pronator. Topographically, this fascicle is usually along the anteromedial quadrant of the median nerve. We use a handheld nerve stimulator to confirm isolation of this fascicle. •There are an average of 1826 and 1840 axons in the biceps and brachialis branches of the MCN, respectively. Within the brachium, there are an average of 1318 axons per fascicle in the ulnar nerve and 1860 axons per fascicle in the median nerve (Schreiber, 2015). POSITIONING •Supine positioning with a hand table extension •General anesthesia without long-acting muscle paralysis (due to the use of a handheld nerve stimulator during case) •The arm is abducted and the shoulder is externally rotated to provide access to the medial brachium. Descargado para Alexis Studer de Oya ([email protected]) en Mutua de Accidentes de Trabajo y Enfermedades Profecionales de la Seguridad Social de ClinicalKey.es por Elsevier en marzo 31, 2019. Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2019. Elsevier Inc. Todos los derechos reservados. PROCEDURE 41 Nerve Transfers for Shoulder and Elbow Restoration After Upper Trunk Brachial Plexus Injuries PROCEDURE Step 1: Exposure of the Musculocutaneous Nerve •Longitudinal incision along the medial midbrachial sulcus, beginning at the distal insertion of the pectoralis major (see Fig. 41.2). • Branches of the medial brachial cutaneous and medial antebrachial cutaneous nerves are identified, isolated, and protected. •The fascial plane between the biceps and brachialis muscles is developed, exposing the MCN. •The MCN is externally neurolysed, inspecting for the (more proximal) branches to the biceps and the (more distal) branch to the brachialis. All nerve branches are traced distally to visualize entrance to their respective muscle bellies, ensuring that reinnervation will not target the sensory component of the MCN (lateral antebrachial cutaneous nerve). Absence of function in these target fascicles is confirmed with the handheld nerve stimulator. •The target nerve branches are then internally neurolysed to ensure that a tensionfree coaptation can be achieved. In our experience, the biceps fascicle(s) can be internally neurolysed approximately 5 cm, and the brachialis fascicle can be internally neurolysed up to 9 cm as needed for appropriate swing distance. Excessive internal neurolysis is not recommended, as it increases the distance and time to reinnervation. Step 2: Exposure of the Donor Nerves •The median nerve is immediately deep to the anterior brachial fascia along the medial aspect of the biceps and is the most anterior major peripheral nerve in the brachium. After isolating it from the brachial artery and vein, external neurolysis of the median nerve is performed. It is recommended that both median and ulnar nerves are identified and stimulated prior to assigning targets and donors. Once the proximal-to-distal location of the biceps and brachialis fascicles is known, the level of intraneural dissection of the median nerve can be selected. Topographically, the donor fascicles to the FCR/pronator/FDS are typically on the anteromedial aspect of the nerve. Because anatomic variation and fascicular interconnection are expected, a handheld nerve stimulator is used to confirm a strong and redundant fascicle. Using loupe magnification or a floor-mounted operating microscope, microsurgical technique is used to isolate the desired donor fascicle from the remainder of the median nerve (see Fig. 41.1). •Within the middle third of the brachium, the ulnar nerve is identified as a medial and posterior structure posterior to the medial intermuscular septum. It must be stimulated to confirm its identity. It is externally neurolysed, and the level of intraneural dissection is selected based on location of the recipient nerve branch. Topographically, the donor fascicle that predominantly innervates the FCU is typically on the anterolateral aspect of the nerve. Because anatomic variation and fascicular interconnection are expected, a handheld nerve stimulator is used to confirm the location of the fascicle. Using loupe magnification or a floor-mounted operating microscope, microsurgical technique is used to isolate the FCU fascicle from the remainder of the ulnar nerve (see Fig. 41.1). Step 3: Microsurgical Nerve Coaptation •The recipient fascicles to the biceps and brachialis are sharply transected proximally at a level that allows tension-free coaptation to the donor ulnar and median fascicles (Fig. 41.4). •Microsurgical technique is used to perform a tension-free nerve coaptation without fascicular extrusion/eversion or excessive compression of the nerve ends. We prefer the use of 9-0 OR 10-0 nylon suture (2–3 sutures per coaptation), followed by the application of fibrin glue (Fig. 41.5). •The nerve coaptation is inspected in end-range positions of shoulder and elbow motion to note whether additional dissection of the donor or recipient nerve is necessary or whether limitations in postoperative rehabilitation will be needed. •Hemostasis is obtained, and a drain is placed away from the nerve coaptation sites. We do not routinely reapproximate the deep fascia. A routine, layered wound closure is performed. 405 STEP 1 PITFALLS •Poor initial selection of the plane for dissection between the biceps and brachialis •Not visually confirming the insertion of the target fascicles into the muscle bellies •Surgical techniques that traumatize the target fascicles •Inexperience with microsurgical dissection technique •Targeting the lateral antebrachial cutaneous nerve component of the musculocutaneous nerve STEP 1 CONTROVERSIES •Given its anteromedial location, the surgeon may find it easier to expose the median nerve before dissecting the musculocutaneous nerve. •If an avulsion injury of the distal nerve stump from the muscle belly is encountered, direct muscle neurotization (implantation of the donor fascicles directly into the muscle belly) can be used to reinnervate the target muscle. •If biceps or brachialis fascicles stimulate briskly with 0.5 mA with a handheld nerve stimulator, consider changing to a single fascicle transfer (instead of a double fascicular transfer). STEP 2 PEARLS •Following internal neurolysis and proximal division of the target fascicles to the biceps and brachialis, the surgeon can reflect these fascicles to the median and ulnar nerves to determine the appropriate location for donor fascicle dissection. •Always divide the donor nerve distal to the reflected recipient fascicle with enough length for a tension-free nerve coaptation. •Move the elbow through a full range of motion (ROM) to ensure absence of tension at the nerve coaptation site. STEP 2 PITFALLS •Absolute confidence in the selection of donor fascicles is imperative. •Lack of robust response to a handheld nerve stimulator indicates that either the inappropriate fascicle has been selected or the planned donor nerve may have been injured. STEP 2 CONTROVERSIES •Based on our experience, the most common pairing in the double nerve transfer is FCR to the biceps and FCU to the brachialis. This is based on convenient anatomic matching during dissection. Using the alternative pairing is unlikely to have any negative effects with regard to reinnervation or cortical re-education and sometimes provides a better fascicular match or technically easier coaptation. Descargado para Alexis Studer de Oya ([email protected]) en Mutua de Accidentes de Trabajo y Enfermedades Profecionales de la Seguridad Social de ClinicalKey.es por Elsevier en marzo 31, 2019. Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2019. Elsevier Inc. Todos los derechos reservados. 406 PROCEDURE 41 Nerve Transfers for Shoulder and Elbow Restoration After Upper Trunk Brachial Plexus Injuries STEP 3 PEARLS Vascular pedicle •Tension-free nerve coaptation is an absolute necessity. •Passing the brachialis fascicle deep to the median nerve (and resting along the brachialis muscle belly) can be helpful to decrease the length of neural regeneration. Anterior Proximal Musculocutaneous nerve STEP 3 PITFALLS •Prior to division, both the donor and recipient nerves should be maximally mobilized to allow tension-free coaptation. Additional excursion can be gained after the nerves have been divided, but it is slightly more challenging. •Any tension on the nerve coaptation increases the risk of coaptation rupture and increases the likelihood of fibrosis that will impede neural regeneration. •Excessive compression at the nerve coaptation (and the resultant fascicular extrusion or invagination) substantially decreases the chances of successful neural regeneration and robust functional recovery. Median nerve Branch to FCU Branch to FCR transferred to transferred to branch to brachialis branch to biceps Ulnar nerve FIG. 41.4 STEP 3 INSTRUMENTATION/ IMPLANTATION •We use a floor-mounted microscope and microsurgical instruments for nerve coaptation. STEP 3 CONTROVERSIES •If only a single donor fascicle is available, we typically will target the biceps branch to obtain both active elbow flexion and supination. •There is variation in surgeon preference for nerve coaptation technique. Some surgeons prefer to use fibrin glue to minimize sutures, while others prefer the use of conduits or connectors (particularly in the setting of a size mismatch). •While not used in our practices, xenograft or synthetic materials to wrap the nerve ends following coaptation have been described. We prefer not to use these materials due to concern for additional fibrosis and potential ischemia. POSTOPERATIVE PEARLS •We begin discussing cortical reeducation with patients before surgery and emphasize the importance of beginning to couple the paired actions on the contralateral side. POSTOPERATIVE PITFALLS •A disengaged patient who does not invest adequate time and effort for postoperative therapy will not achieve strong elbow flexion (M4), although he or she may have a satisfactory outcome. FIG. 41.5 POSTOPERATIVE CARE AND EXPECTED OUTCOMES •The postoperative drain is typically removed within the first 48 hours of surgery if there are no signs of hematoma. •If the pectoralis major has not been detached (and later repaired) for exposure, a simple shoulder sling is used for the first 3–4 weeks for initial immobilization of the shoulder and elbow. Active and gentle passive shoulder and gentle passive elbow motion is started after 4 weeks. •Once initial signs of muscle reinnervation are present, motor retraining begins. Mirror training and coupled exercises are a helpful adjunct. •We expect to see signs of muscle contraction on EMG by 10–12 weeks; clinical evidence of elbow flexor contraction within 24 weeks; and antigravity elbow flexion by 9–12 months (Bhandari and Deb, 2015). •M4 or M4+ elbow flexion is expected in the majority of patients (>80%) (Liverneaux et al., 2006; Mackinnon et al., 2005). EVIDENCE Bhandari PS, Deb P. Management of isolated musculocutaneous injury: comparing double fascicular nerve transfer with conventional nerve grafting. J Hand Surg Am. 2015;40(10):2003–6. Liverneaux PA, Diaz LC, Beaulieu JY, Durand S, Oberlin C. Preliminary results of double nerve transfer to restore elbow flexion in upper type brachial plexus palsies. Plast Reconstr Surg. 2006;117(3):915–9. Mackinnon SE, Novak CB, Myckatyn TM, Tung TH. Results of reinnervation of the biceps and brachialis muscles with a double fascicular transfer for elbow flexion. J Hand Surg Am. 2005;30(5):978–85. Schreiber JJ, Byun DJ, Khair MM, Rosenblatt L, Lee SK, Wolfe SW. Optimal axon counts for brachial plexus nerve transfers to restore elbow flexion. Plast Reconstr Surg. 2015;135(1):135e-41e. Schreiber JJ, Feinberg JH, Byun DJ, Lee SK, Wolfe SW. Preoperative donor nerve electromyography as a predictor of nerve transfer outcomes. J Hand Surg Am. 2014;39(1):42–9. Descargado para Alexis Studer de Oya ([email protected]) en Mutua de Accidentes de Trabajo y Enfermedades Profecionales de la Seguridad Social de ClinicalKey.es por Elsevier en marzo 31, 2019. Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2019. Elsevier Inc. Todos los derechos reservados. PROCEDURE 41 Nerve Transfers for Shoulder and Elbow Restoration After Upper Trunk Brachial Plexus Injuries PART 2: Posterior Nerve Transfers to Restore Shoulder Function After Brachial Plexus Injury INDICATIONS •Injury to the upper (± middle) trunk of the brachial plexus, suprascapular nerve, and/ or axillary nerve. •Inadequate recovery of shoulder external rotation and/or abduction strength following a period of observation and serial physical examinations and electromyograms (EMG). •Glenohumeral subluxation related to weakness/atony of the rotator cuff and deltoid. •Intact (at least M4, but ideally M5 strength with normal EMG characteristics) strength of potential donor muscles (upper, middle, and lower heads of trapezius; medial, long, and lateral heads of triceps). •Ideally, both the suprascapular nerve and axillary nerve are targeted for reinnervation to maximize recovery of shoulder stabilization and function (Cardenas-Mejia et al., 2008; Garg et al., 2011). •If possible, nerve transfers are selected and performed in a manner that allows direct end-to-end coaptation (which avoids the use of an intercalary nerve graft; Merrell et al., 2001). EXAMINATION/IMAGING •Manual muscle testing of shoulder shrug, external rotation in adducted and abducted position, shoulder extension, and shoulder abduction during internal rotation. • Evaluation for dysesthesias, numbness, or allodynia over the lateral cutaneous branch of the axillary nerve (to assist with injury localization). •Evaluation of scapular position and rhythm, noting whether winging is present. •Evaluation of glenohumeral stability. •EMG of the supraspinatus, infraspinatus, teres minor, and all heads of deltoid showing signs of recent denervation (insertional activity, fibrillations, sharp waves) and discrete or absent motor unit potentials. Nerve conduction studies (particularly, compound motor action potentials) may be helpful in identifying whether a focal point of compression (suprascapular notch or spinoglenoid notch for the suprascapular nerve; quadrangular space for the axillary nerve) is present in the recovering nerve palsy. •EMG of the upper, middle, and lower heads of trapezius; medial, long, and lateral heads of triceps to ensure normal or near normal motor unit recruitment (Schreiber et al., 2013). •Computed tomography (CT) myelogram can be used to evaluate for pseudomeningoceles indicating preganglionic root avulsion injuries. MRI of the brachial plexus can also be used to better localize the site of injury, particularly if a segmental/extended level injury (e.g., root and cord level injuries to the C5 nerve) is suspected. 407 INDICATIONS PITFALLS •Lack of healthy donor nerves •Irreversible denervation atrophy of the supraspinatus, infraspinatus, and deltoid •Discontinuity of the rotator cuff musculotendinous unit •Capsular stiffness and limited passive shoulder range of motion (ROM) •Scapulothoracic instability/weakness or serratus palsy limits the functional gains from restoration of shoulder abduction and external rotation •Poorer functional outcomes have been demonstrated in older patients and those with longer times from injury-to-surgery •Lack of familiarity with brachial plexus anatomy and variations •Lack of familiarity with microsurgical technique for intraneural dissection and nerve coaptation INDICATIONS CONTROVERSIES •Partially recovering nerve injury in which muscle contraction occurs but strength is inadequate. •Secondary nerve compression at suprascapular notch or spinoglenoid notch for the suprascapular nerve; quadrangular space for the axillary nerve. Decompression at known areas of potential compression may be helpful when preoperative imaging or fracture variants suggest secondary entrapment or when nascent motor unit potentials are present but clinical recovery is insufficient. •In the setting of a partially recovering nerve injury, reverse end-to-side nerve transfer may accelerate functional recovery. However, this indication is not widely supported and is not firmly substantiated by laboratory or clinical research. •Ipsilateral lower third trapezius tendon transfer is increasingly recognized as a reliable option to restore shoulder function. Use of the spinal accessory nerve for nerve transfer precludes the use of this procedure. •The spinal accessory nerve is a powerful neurotizer. Consequently, the brachial plexus surgeon may choose to leave this donor nerve intact in case additional surgery (such as a free functioning muscle transfer) is needed in the future. SURGICAL ANATOMY • The spinal accessory nerve enters the posterior cervical triangle posterior to the proximal apex of the sternocleidomastoid, usually 8–9 cm proximal to the clavicle. It obliquely courses through the posterior cervical triangle along the anterior surface of the splenius cervicalis and levator scapulae, heading toward the insertion of the upper trapezius on the clavicle. During this course, it provides 2–3 branches to the upper trapezius in the supraclavicular fossa. The spinal accessory nerve then continues along the undersurface of the trapezius muscle, 2 cm inferior to the superior edge of the muscle. Distal to the clavicle, it continues deep to the trapezius muscle along the medial border of the scapula, giving terminal muscle branches to the middle and lower trapezius (Fig. 41.6). •The upper trunk trifurcates into the suprascapular nerve, posterior division of the upper trunk, and anterior division of the upper trunk (lateral to medial). The suprascapular nerve’s course is oblique (proximal-medial to distal-lateral) and follows the Descargado para Alexis Studer de Oya ([email protected]) en Mutua de Accidentes de Trabajo y Enfermedades Profecionales de la Seguridad Social de ClinicalKey.es por Elsevier en marzo 31, 2019. Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2019. Elsevier Inc. Todos los derechos reservados. 408 PROCEDURE 41 Nerve Transfers for Shoulder and Elbow Restoration After Upper Trunk Brachial Plexus Injuries TREATMENT OPTIONS •In this chapter, we describe the use of a posterior approach to perform these nerve transfers (spinal accessory to suprascapular nerve; triceps branch to anterior branch of the axillary nerve). Both these transfers can be performed from an anterior approach during supraclavicular and infraclavicular exposure of the brachial plexus. •Other potential donor nerves used to transfer to the suprascapular nerve include cervical motor branches and the phrenic nerve, both of which require an intercalary nerve graft. •Other potential donor nerves used to transfer to the axillary nerve include medial pectoral nerve, thoracodorsal nerve, and intercostal nerves. •Nerve grafting from an intact spinal nerve root or the upper trunk to the suprascapular nerve, posterior division of the upper trunk or axillary nerve. •Ipsilateral lower third trapezius tendon transfer. •Contralateral lower third trapezius tendon transfer. •Pedicled latissimus or pectoralis major tendon transfers. •Glenohumeral arthrodesis. omohyoid muscle to the suprascapular notch, passing deep to the superior transverse (suprascapular) ligament. After providing a branch to the supraspinatus and a branch to the glenohumeral joint, it travels within the spinoglenoid notch to supply the infraspinatus (see Fig. 41.6). •After it exits the triangular interval, the first branch of the radial nerve is to the long head of the triceps (along the caudal border of the teres major tendon). The long head branch has a diameter of 2 mm and length of 30 mm. The next branch is typically to the upper-medial head of the triceps, running longitudinally and parallel to the course of the radial nerve proper. This upper-medial head branch has a diameter of 1.6 mm and length of 65 mm (Bertelli, 2007; see Fig. 41.6). •The cutaneous branch of the axillary nerve pierces the deep fascia 9 cm (6–11 cm) inferior to the posterolateral corner of acromion. This nerve can be traced proximally to identify the posterior division of the axillary nerve. The anterior and posterior divisions of the axillary nerve arise within the quadrangular space, but they can originate slightly proximal or distal to the quadrangular space. The teres minor and posterior deltoid branches are easily identified from the posterior division of the axillary nerve. The anterior division branch of the axillary nerve was originally targeted for this nerve Trapezius Spinal accessory nerve Branch of axillary nerve to teres minor Axillary nerve Supraspinatus Suprascapular nerve Acromion Branch of axillary nerve to posterior head of deltoid Axillary nerve Branch of axillary nerve to anterior head of deltoid Branch of axillary nerve to middle head of deltoid Cutaneous branch of axillary nerve Deltoid Lateral head triceps Nerve to medial head triceps Infraspinatus Teres minor Teres major Long head triceps Nerve to lateral head Nerve to long head FIG. 41.6 Descargado para Alexis Studer de Oya ([email protected]) en Mutua de Accidentes de Trabajo y Enfermedades Profecionales de la Seguridad Social de ClinicalKey.es por Elsevier en marzo 31, 2019. Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2019. Elsevier Inc. Todos los derechos reservados. PROCEDURE 41 Nerve Transfers for Shoulder and Elbow Restoration After Upper Trunk Brachial Plexus Injuries transfer to maximize motor recovery of the anterior and middle heads of the deltoid. However, many surgeons prefer to transfer to the entire axillary nerve or to both the anterior division and the teres minor branch to restore both abduction and external rotation (Khair et al., 2016; see Fig. 41.6). •At the levels accessed for the posterior nerve transfer, the axonal counts for the spinal accessory nerve and the suprascapular nerve are 1300–1600 and 3500, respectively. The axon counts for the branches to the long and medial heads of the triceps are 2302 and 2198, respectively. The axon count in the anterior branch of the axillary nerve is 4052 (Khair et al., 2016). POSITIONING •Prone positioning with the ipsilateral shoulder and arm included in sterile field •General anesthesia without long-acting muscle paralysis (due to the use of a handheld nerve stimulator during case) •The arm is rested on a sterile Mayo stand in an adducted position or flexed at the elbow over a padded bolster. PORTALS/EXPOSURES •The scapular spine, medial scapular border, posterolateral corner of the acromion, and vertebral midline are used as surface anatomy landmarks. The distal spinal accessory nerve courses just midline to the medial border of the scapula, approximately 40% of the distance between the thoracic spine and the posterolateral corner of the acromion. The suprascapular notch is present at approximately half the distance between the medial border of the scapula and the posterolateral corner of the acromion (Fig. 41.7). •A 7–8-cm transverse incision is made 2–3 cm cephalad to the scapular spine, allowing exposure of both these landmarks (Fig. 41.8). •A longitudinal incision from the soft spot of the quadrangular space and along the midline of the posterior proximal brachium is utilized for exposure of the quadrangular space and triangular interval. 409 POSITIONING PEARLS •A sterile bump/support is placed under the anterolateral acromion. •Bony landmarks are palpated and marked with indelible ink prior to sterile prep and draping. •Dilute epinephrine solution (1:200,000) is infiltrated into the planned skin incisions prior to the sterile prep and draping. •The sterile prep and draping includes the vertebral midline and posterior aspect of the neck. POSITIONING CONTROVERSIES •Semilateral decubitus positioning on a beanbag can be used for the posterior approach to the axillary nerve. This is particularly useful if additional nerve transfers to address elbow flexion and/or serratus anterior palsy are planned, but this may make the posterior approach to the suprascapular and spinal accessory nerves more challenging. PROCEDURE Step 1: Exposure of the Suprascapular Nerve •A transverse skin incision just cephalad to the superior border of the scapula is created. The upper trapezius fibers are split in line with the skin incision to expose the fascia of the supraspinatus muscle and the superior border of the scapula (Fig. 41.9, and see also Fig. 41.8). •As the supraspinatus muscle is typically atrophied, there is no reason to incise its fascia or mobilize it from the suprascapular fossa. •The superior border of the scapula is palpated from medial to lateral toward the base of the coracoid. The suprascapular notch is immediately adjacent to the coracoid base and can be palpated as a depression in the superior border of the scapula. The suprascapular ligament spans the notch. FIG. 41.8 FIG. 41.7 FIG. 41.9 Descargado para Alexis Studer de Oya ([email protected]) en Mutua de Accidentes de Trabajo y Enfermedades Profecionales de la Seguridad Social de ClinicalKey.es por Elsevier en marzo 31, 2019. Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2019. Elsevier Inc. Todos los derechos reservados. 410 PROCEDURE 41 Nerve Transfers for Shoulder and Elbow Restoration After Upper Trunk Brachial Plexus Injuries STEP 1 PEARLS •Absolute hemostasis and a headlamp are necessary for exposure. •It may be easier to identify the spinal accessory nerve before the suprascapular nerve. In either case, proceed cautiously near the medial border of the scapula and use a handheld nerve stimulator to assist with identification of the spinal accessory nerve. STEP 1 PITFALLS •Avoid making the skin incision directly over the scapular spine or mobilizing the supraspinatus muscle, as notch exposure becomes difficult and may lead to injury of the suprascapular nerve. •Inadequate visualization can lead to damage to the suprascapular artery or veins, bleeding that is difficult to control, and potential thermal injury to the suprascapular nerve. •Improper surgical technique can traumatize the target fascicles. STEP 2 PEARLS •The spinal accessory nerve is typically accompanied by vasa nervorum. We have found it helpful to use a surgical ligaclip when dividing the nerve distally. The nerve end is then re-cut using a scalpel prior to microsurgical coaptation. FIG. 41.10 •Blunt dissection using a Kittner/peanut sponge over the suprascapular notch assists in exposing the suprascapular ligament. Care must be taken when bluntly dissecting to expose and protect the suprascapular vessels during this maneuver. They may be ligated with silk sutures as needed during the exposure. Rarely, the supraspinatus branch from the suprascapular nerve may overlay the suprascapular ligament. Often, the suprascapular nerve is not visualized until the suprascapular ligament is divided (Fig. 41.10). •Following exposure of the suprascapular ligament, a right-angled (Mixter) clamp is inserted beneath the ligament and gently swept to clear adhesions. A vessel loop may be passed as necessary. The suprascapular ligament is divided under direct visualization using a long-handled scalpel. •The suprascapular nerve is mobilized under loupe magnification back to the level of the clavicle and its origin from the upper trunk to allow maximal excursion for nerve coaptation. If there is suspicion for a secondary point of compression at the spinoglenoid notch, the nerve may be traced distally and decompressed. Step 2: Exposure of the Spinal Accessory Nerve STEP 2 PITFALLS •Lack of robust response to a handheld nerve stimulator indicates that either the inappropriate fascicle has been selected or the planned donor nerve may have been injured. STEP 3 PEARLS •Prone or lateral decubitus positioning over a bolster is optimal. •Deep cerebellar retractors between the posterior deltoid and lateral head of the triceps are helpful for exposure. •Early identifying and tracing of the cutaneous branch facilitates dissection of the axillary nerve. •A headlight is critical in facilitating deep dissection. •If nascent motor unit potentials are present in the teres minor and posterior deltoid, a single transfer to the anterior division of the axillary nerve should be performed. STEP 3 PITFALLS •Inadequate knowledge of the anatomy of the axillary nerve •Careful dissection about the posterior humeral circumflex vessels is required to avoid vascular injury, difficulty with hemostasis, and nerve injury. •At the level of the superior border of the scapula and near its medial edge, the trapezius is gently spread in line with its fibers until the nerve is identified running along its anterior face. Meticulous hemostasis, loupe magnification, and use of a handheld nerve stimulator are essential. The course of the spinal accessory nerve is dissected parallel to the scapular border within its protective fat. The nerve is traced until its branching points to generate sufficient length for transfer (Fig. 41.11). •Following exposure of both donor and recipient nerves, the suprascapular nerve is divided first to identify the necessary length of the donor. The spinal accessory nerve is dissected proximally and distally to maximize excursion and then is divided sufficiently distal to enable tension-free coaptation to the suprascapular nerve (Fig. 41.12). Step 3: Exposure of the Axillary Nerve •We first describe exposure of the axillary nerve, but some surgeons may prefer to expose the radial nerve first. •A 15–20-cm posterior midline incision is made from the posterior “soft spot” over the quadrangular space to the mid-humerus. The fat is divided with electrocautery down to the fascia of the lateral and long heads of the triceps. Proximally, blunt dissection is performed along the posterior deltoid fascia to identify the cutaneous branch of the axillary nerve approximately 8–9 cm distal/interior to the posterolateral corner of the acromion. This cutaneous branch is looped and traced proximally to the axillary nerve in the quadrangular space. •The fascial plane between the posterior head of the deltoid and the lateral head of the triceps is bluntly developed to expose the quadrangular space, and hemostasis is critical to avoid damage to the branches of the axillary nerve. •Deep in the quadrangular space and posteromedially, the teres minor branch exits as the first branch from the posterior division of the axillary nerve. The posterior division of the axillary nerve then divides into the branch to the posterior deltoid and the Descargado para Alexis Studer de Oya ([email protected]) en Mutua de Accidentes de Trabajo y Enfermedades Profecionales de la Seguridad Social de ClinicalKey.es por Elsevier en marzo 31, 2019. Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2019. Elsevier Inc. Todos los derechos reservados. PROCEDURE 41 Nerve Transfers for Shoulder and Elbow Restoration After Upper Trunk Brachial Plexus Injuries 411 STEP 3 CONTROVERSIES FIG. 41.11 FIG. 41.12 •We do not routinely target the posterior branch of the axillary nerve, as shoulder extension is not a high-priority function. We do, however, target the nerve to teres minor, since transfer of the suprascapular nerve is generally inadequate to restore strong external rotation. Double nerve transfers for shoulder function have been demonstrated to provide superior clinical outcomes (Bertelli and Ghizoni, 2010; Khair et al., 2016; Merrell et al., 2001). •We do not perform sensory nerve transfers to reinnervate the skin supplied by the cutaneous branch of the axillary nerve. STEP 4 PEARLS cutaneous branch. A loop may be placed around the posterior axillary division. The lateral tendinous edge of the lateral head of the triceps can be divided to gain more proximal access to the axillary nerve. •The anterior division of the axillary nerve innervates the middle and anterior heads of the deltoid. Using loupe magnification, the anterior division is internally neurolysed from the remainder of the axillary nerve and a vessel loop is placed around it. A nerve stimulator is used to confirm absence of contraction prior to performing the nerve transfer. Step 4: Exposure of the Triceps Branches from the Axillary Nerve •The raphe between the lateral and long heads of the triceps is identified and bluntly separated down to the humerus. Medium or large sharp self-retaining (Weitlaner) retractors are used to help gain exposure. The radial nerve is visualized in the spiral groove and traced proximally to where it passes deep to the tendon of the teres major in the triangular space. The medial head branch of the triceps is deep/anterior to the radial nerve proper along the humerus. •The branches to the long head of the triceps and upper-medial head of the triceps are identified. The long head branch exits from the medial aspect of the nerve deep to the teres major and runs slightly obliquely, entering the long head just distal to the teres major tendon. The upper-medial head branch exits at the level of the latissimus dorsi tendon anteriorly and typically runs in the spiral groove, longitudinal and deep to the radial nerve proper. The lateral head branches run obliquely from the lateral aspect of the radial nerve. •The donor branch is selected based on surgeon preference and excursion of the dissected branch (Khair, 2016). A handheld nerve stimulator is used to confirm health of the donor nerve. Step 5: Microsurgical Nerve Coaptation •The recipient fascicles to the suprascapular nerve and the anterior branch of the axillary nerve are sharply transected proximally at a level that allows tension-free coaptation to the donor spinal accessory nerve and triceps branch, respectively (Fig. 41.13 and see also Fig. 41.12). •Microsurgical technique is used to perform a tension-free nerve coaptation without fascicular extrusion/eversion or excessive compression of the nerve ends. We prefer the use of 9-0 OR 10-0 nylon suture (2–3 sutures per coaptation), followed by application of fibrin glue (Figs. 41.14 and 41.15). •Just prior to performing the coaptation, the aligned nerve ends are observed during end-range positioning of shoulder motion to note whether additional dissection of the donor or recipient nerve is necessary or whether limitations in postoperative rehabilitation are needed. •Hemostasis is obtained and a drain is placed away from the nerve coaptation sites as needed. We do not routinely reapproximate the deep fascia. A routine, layered wound closure is performed. •The deltoid tuberosity can be a useful bony landmark for localizing the radial nerve: at this location, the radial nerve courses obliquely along the spiral groove. It is generally easiest if the radial nerve is traced proximally from this point. •Subtotal division of the teres major tendon and gentle neurolysis of the donor branch from the radial nerve can be used to gain additional donor length, especially for the long head branch, which almost always has sufficient length and girth to coapt to the entire axillary nerve. •It is often easiest to join the long head branch from the triceps directly to the entire axillary nerve. Using all branches to the long head and coapting them to the axillary nerve when cut deep in the quadrangular space provides an excellent size match, double innervation, and adequate length without tension (Bertelli, 2010; Colbert and Mackinnon, 2006). •If multiple branches of the spinal accessory nerve are harvested, they can be coapted with fibrin glue and trimmed into a single cable with a nerve cutting device. •Addition of a sub-branch of one of the other two triceps heads does not weaken the triceps in a clinically apparent way and provides the advantage of additional axonal input (Khair, 2016). •The medial head branch is the longest branch and will always reach the target nerve. •Divide the axillary nerve before dividing the donor nerve to identify appropriate donor length—this can be measured using a vessel loop. STEP 4 PITFALLS •Inadequate preparation or proximal neurolysis of a donor branch leads to insufficient excursion and excessive tension on the nerve coaptation. •Partial C7 injuries can compromise the function and strength of the triceps. Generally, the triceps gains strength with time. Recovery can be tracked with serial EMG’s. •The lateral head of the triceps may receive innervation from C5/C6, so its use as a donor in these injury patterns is cautioned. •If C7 is severely damaged, alternative sources for transfer to the axillary nerve (thoracodorsal, intercostal, or medial pectoral nerves) are considered. Descargado para Alexis Studer de Oya ([email protected]) en Mutua de Accidentes de Trabajo y Enfermedades Profecionales de la Seguridad Social de ClinicalKey.es por Elsevier en marzo 31, 2019. Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2019. Elsevier Inc. Todos los derechos reservados. 412 PROCEDURE 41 Nerve Transfers for Shoulder and Elbow Restoration After Upper Trunk Brachial Plexus Injuries STEP 4 INSTRUMENTATION/ IMPLANTATION •A headlamp facilitates deep dissection •Medium or large sharp self-retaining retractors (Weitlaner) •Cerebellar retractors •Nerve-cutting instrument set STEP 4 CONTROVERSIES •There is no consensus as to which branch of the triceps should be used as a donor for this nerve transfer. The advantage of the long head branch is the higher axon count, while the disadvantages are a slightly shorter excursion and a theoretical loss of a secondary function of the long head (assisting in shoulder adduction/ brachiothoracic pinch). This issue may be more important if the thoracodorsal nerve and medial pectoral nerves are also both injured, which is uncommon in upper trunk injuries. •The advantages of the medial head branch are the greater excursion (6 cm) and the redundancy of innervation to the medial head of the triceps (there is also a lower-medial head branch). The lower axonal counts in the medial head branch can be overcome if multiple branches are harvested for transfer (Khair, 2016). FIG. 41.13 FIG. 41.14 Axillary nerve STEP 5 PEARLS •Tension-free nerve coaptation is an absolute necessity. •We prefer reinforcement of the nerve coaptation with fibrin glue. STEP 5 PITFALLS •Prior to division, both the donor and recipient nerves should be maximally mobilized to allow tension-free coaptation. Additional excursion can be gained after the nerves have been divided, but it is more challenging and can be traumatic to the cut nerve end. •Any tension on the nerve coaptation increases the risk of coaptation rupture and increases the likelihood of fibrosis that impedes neural regeneration. •Excessive compression at the nerve coaptation (and the resultant fascicular extrusion or invagination) substantially decreases the chances of successful neural regeneration and robust functional recovery. •Use of a compromised donor from C7 diminishes outcome. •High body mass index (BMI) and advanced age are poor prognosticators for postoperative strength and range of motion (Lee, 2012). •Denervation of serratus anterior (seen in upper trunk extended injury patterns) portends a worse prognosis due to scapular instability. Additional nerve transfers to reinnervate the serratus anterior should be considered. FIG. 41.15 Descargado para Alexis Studer de Oya ([email protected]) en Mutua de Accidentes de Trabajo y Enfermedades Profecionales de la Seguridad Social de ClinicalKey.es por Elsevier en marzo 31, 2019. Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2019. Elsevier Inc. Todos los derechos reservados. PROCEDURE 41 Nerve Transfers for Shoulder and Elbow Restoration After Upper Trunk Brachial Plexus Injuries POSTOPERATIVE CARE AND EXPECTED OUTCOMES •An ace-wrapped shoulder spica soft dressing is used for 48 hours until the drains are removed. •The drain is typically removed within the first 48 hours of surgery if there are no signs of hematoma and there is less than 25 mL of output for two consecutive shifts. •A simple shoulder sling is used for the first 3–4 weeks for initial immobilization of the shoulder and elbow. Active and gentle passive shoulder motion is started after 4 weeks. In this context, there is no advantage to earlier motion unless there is a preexisting capsular contracture or acute trauma to the shoulder capsule. •Once initial signs of muscle reinnervation are present, motor retraining begins. Mirror training and coupled exercises are a helpful adjunct. •Following this set of nerve transfers, at least M3 shoulder abduction and external rotation is expected in 70%–80% of patients, with mean abduction of 110–125 degrees (Bertelli, 2004; Leechavengvong, 2006). •Patients with partial C7 injury have worse outcomes (Bertelli, 2010). EVIDENCE Bertelli JA, Ghizoni MF. Nerve root grafting and distal nerve transfers for C5-C6 brachial plexus injuries. J Hand Surg Am. 2010;35(5):769–75. Bertelli JA, Ghizoni MF. Reconstruction of C5 and C6 brachial plexus avulsion injury by multiple nerve transfers: spinal accessory to suprascapular, ulnar fascicles to biceps branch, and triceps long or lateral head branch to axillary nerve. J Hand Surg Am. 2004;29(1):131–9. Bertelli JA, Santos MA, Kechele PR, Ghizoni MF, Duarte H. Triceps motor nerve branches as a donor or receiver in nerve transfers. Neurosurgery. 2007;61(5 Suppl 2):333–8; discussion 338-9. Cardenas-Mejia A, O’Boyle CP, Chen KT, Chuang DC. Evaluation of single-, double-, and triple-nerve transfers for shoulder abduction in 90 patients with supraclavicular brachial plexus injury. Plast Reconstr Surg. 2008;122(5):1470–8. Colbert SH, Mackinnon S. Posterior approach for double nerve transfer for restoration of shoulder function in upper brachial plexus palsy. Hand (N Y). 2006;1(2):71–7. Garg R, Merrell GA, Hillstrom HJ, Wolfe SW. Comparison of nerve transfers and nerve grafting for traumatic upper plexus palsy: a systematic review and analysis. J Bone Joint Surg Am. 2011;93(9):819– 29. Khair MM, Schreiber JJ, Rosenblatt L, Byun DJ, Lee SK, Wolfe SW. Axon counts yield multiple options for triceps fascicular nerve to axillary nerve transfer. J Hand Surg Am. 2016;41(11):e405–10. Lee JY, Kircher MF, Spinner RJ, Bishop AT, Shin AY. Factors affecting outcome of triceps motor branch transfer for isolated axillary nerve injury. J Hand Surg Am. 2012;37(11):2350–6. Leechavengvongs S, Witoonchart K, Uerpairojkit C, Thuvasethakul P, Malungpaishrope K. Combined nerve transfers for C5 and C6 brachial plexus avulsion injury. J Hand Surg Am. 2006;31(2):183–9. Merrell GA, Barrie KA, Katz DL, Wolfe SW. Results of nerve transfer techniques for restoration of shoulder and elbow function in the context of a meta-analysis of the English literature. J Hand Surg Am. 2001;26(2):303–14. 413 STEP 5 INSTRUMENTATION/ IMPLANTATION •We use a floor-mounted microscope and microsurgical instruments for nerve coaptation. •We use a nerve-cutting instrument to freshen the nerve ends prior to coaptation. STEP 5 CONTROVERSIES •While not used in our practices, xenograft or synthetic materials to wrap the nerve ends following coaptation have been described. We prefer not to use these materials due to concern for additional fibrosis and potential ischemia. POSTOPERATIVE PEARLS •We begin discussing cortical re-education with patients before surgery and emphasize the importance of beginning to couple the paired actions on the contralateral side. •Scapular stabilization is essential to functional success after reinnervation of the rotator cuff and deltoid. This can be accomplished through strengthening of the intact periscapular muscles, preservation of the upper trapezius, or addition of a supplemental nerve transfer (thoracodorsal or intercostal nerves) to target the long thoracic nerve. POSTOPERATIVE PITFALLS •A disengaged patient who does not invest adequate time and effort for postoperative therapy will not achieve strong shoulder function, although he or she may have a satisfactory outcome. •Noncompliance with postoperative restrictions can disrupt the repair, which cannot be diagnosed postoperatively. Descargado para Alexis Studer de Oya ([email protected]) en Mutua de Accidentes de Trabajo y Enfermedades Profecionales de la Seguridad Social de ClinicalKey.es por Elsevier en marzo 31, 2019. Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2019. Elsevier Inc. Todos los derechos reservados.