Fracturas de Astrágalo: Anatomía, Mecanismos y Tratamiento
Anuncio

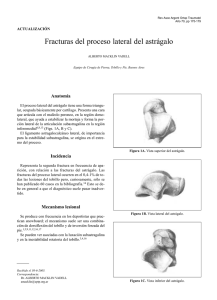
Hospital Universitario Dr. José Eleuterio González Fracturas de Astrágalo Asesor – Dr. Ángel Arnaud Dr. Abiel Eugenio Garza Borjón RIV TyO Introducción • “Articulación universal del pie” • 1% de todas las fracturas (Alta energía) – Accidente vehicular – Caídas de altura • Segundo hueso en fracturarse por incidencia (+ Calcáneo) Introducción • Astrágalo proviene de la palabra – Francesa “Talo” – Tobillo – Latín “Taxillus” – Dado – Griego “Astragalus” – Dado Introducción • Descritas desde 1608 – Fabricius de Hilden - Talectomía • 1818 (James Syme) – Tratamiento de fracturas Amputación distal a rodilla (Mortalidad de 25%) • 1952 (Coltart) – Descripción de 228 casos acumulados por la 2da Guerra Mundial • 1970 (Hawkins) – Describe clasificación pronóstica para necrosis avascular Anatomía Esquelética • Articulaciones (Movilidad de retro-pie y medio-pie): – Sub-astragalina – Tarsal transversa – Tobillo • 2/3 cubierto por cartílago articular (5 carillas articulares) – Fracturas desplazadas = Sub/luxación 13.1.1 Talus (Figures 13.6–13.7, 13.17 Anatomía Esquelética The talus is called the astragalus in other anim situated between the tibia and fibula superiorly to this bone. It rests atop the calcaneus and arti lower member of the talocrural joint. Talar va a. The head is the rounded, convex, distal art of the navicular. • No inserciones tendinosas medial malleolar articular surface body b. The body is the squarish bulk of the bone neck c. The trochlea isneck the saddle-shaped articula and medial malleolar surfaces (or facets respectively. d. The neck connects the head of the talus to lar facets on the neck, formed by contact w head strong dorsiflexion of the foot at the ankle squatting facets. lateral malleolar articular surface body • Transfiere el peso del pie a la tibia y peroné. medial subtalar facet posterior subtalar facet lateral process Figure 13.7 Right talus. Left: medial view; right: lateral view. Dorsal is up. Natural size. • Se divide en 3 partes y 2 procesos: e. surface of the talar body. It is so named because it transmits the tendon of this muscle, a calf muscle that plantarflexes the foot and hallux. f. The subtalar (or calcaneal) facets on the inferior aspect of the talus are usually three in number and variable in shape. trochlea 1. The anterior subtalar (or calcaneal) facet is the most anterior facet on the plantar (inferior) surface of the talus, often somewhat continuous with the articular surface of posterior process the talar head. 2. The medial subtalar (or calcaneal) facet is highly variable, sometimes separated from — but often merging to a greater or lesser extent with — the anteriorgroove subtalar for flexor hallucis longus facet (see Figure 3.1 for examples). 3. The posterior subtalar (or calcaneal) facet is the largest facet on the plantar surface anterior fa neck medial malleolar vertical groove on the posterior The groove for flexor hallucis longus is the short, nearly surface – Cuerpo, Cuello y Cabeza – Lateral y posterior face head superior articular surface lateral malleolar surface lateral process posterior subtalar facet ne Anatomía Esquelética Cabeza del Astrágalo • “Acetabulum Pedis” – Porción distal del astrágalo que hace “nido” a la articulación • Formado por – Superficie intermedia y anterior del calcáneo – Superficie articular del escafoides – Unidas por los ligamentos inferior y superomedial calcaneo-escafoideos SK: Anatomy of the foot and ankle, Philadelphia, 19 Anatomía Esquelética Cabeza del Astrágalo • Se mantiene en posición en “plano axial”: – Lateral – Ligamento bifurcado calcáneoescafoideo – Medial – Tibial posterior y ligamento “Spring o CalcáneoEscafoideo” A C B Figure 39-4 The talocalcaneal angle demonstrates deviation of the talus on the calcaneus, not only fro declination angle of the talar neck but also from the articulation. a keystone. This unique shape provides maximal congruence in the articular joint when the talu dorsiflexed position. The inferior surface of the talar body consis facies articularis calcanea posterior tali.134 This surface is quadrilateral and is concave in the long flat transversely. It articulates with the posterior the calcaneus (Fig. 39-4). 2104 Anatomía Esquelética Cabeza del Astrágalo • Porción anteroinferior medial es cuadrilateral u oval – Se articula con faceta anterior del calcáneo. Anatomía Esquelética Cuello del Astrágalo • Cuenta con 4 superficies: – Superior, lateral, medial e inferior. • No cubierto por superficie articular • Cuello angulado – 24º medial (10-44º) – 5-50º plantar – Parte más vulnerable a fracturarse Anatomía Esquelética Cuello del Astrágalo • Superior – Limitado por: • Domo del astrágalo (Posterior) • Cabeza del astrágalo (Anterior) – Cápsula Tibioastragalina se inserta en superficie superior • Aledaño a inserción capsular de articulación astrágalo-escafoidea. 13.1.1 Talus (Figures 13.6–13.7, 13.17) Anatomía Esquelética Cuello del Astrágalo The talus is called the astragalus in other animals. It is the second largest of the tarsals and is situated between the tibia and fibula superiorly and the calcaneus inferiorly. No muscles attach to this bone. It rests atop the calcaneus and articulates distally with the navicular. It forms the lower member of the talocrural joint. Talar variation is illustrated in Figure 3.1 of Chapter 3. a. The head is the rounded, convex, distal articular surface of the talus. It fits into the hollow of the navicular. b. The body is the squarish bulk of the bone posterior to the talar neck. c. The trochlea is the saddle-shaped articular surface of the body. Its sides are the lateral and medial malleolar surfaces (or facets), which articulate with the fibula and tibia, respectively. d. The neck connects the head of the talus to the body. Occasionally there are small articular facets on the neck, formed by contact with the anterior surface of the distal tibia during strong dorsiflexion of the foot at the ankle (or talocrural) joint. These facets are called squatting facets. • Inferior – Forma el techo del seno del tarso, canal del tarso. – Punto de inserción del ligamento: facet for the navicular head • Astrágalo-calcáneo medial (Estabilizador de malleolar surface articulación subastragalina) head anterior subtalar facet neck superior articular surface neck medial subtalar facet lateral malleolar surface lateral process sulcus tali trochlea posterior subtalar facet posterior process groove for flexor hallucis longus groove for flexor hallucis longus Figure 13.6 Right talus. Left: dorsal (or superior) view; right: plantar (or inferior) view. Distal is up. Natural size. Anatomía Esquelética Cuello del Astrágalo • Lateral – Forma cóncava – Inserción del aspecto medial del retínaculo extensor inferior • Medial – Forma convexa – Inserción de ligamentos astrágalo-escafoideos L M Dorsal metatarsal ligaments Lateral talocalcaneal ligament Dorsal c u n e o c u b o i d ligament Long plantar ligament Cuboid bone Fibularis (peroneus) longus Dorsal calcaneocuboid ligament Fibularis (peroneus) brevis Right foot: medial view Posterior tibiotalar part Medial (deltoid) ligament of ankle ) Medial talocalcaneal ligament Tibiocalcaneal part Tibionavicular part Anterior tibiotalar part Posterior process of talus Dorsal talonavicular ligament Posterior talocalcaneal igament Navicular bone Dorsal cuneonavicular ligaments Medial cuneiform bone Calcaneal (Achilles) tendon (cut) Dorsal intercuneiform ligament Dorsal tarsometatarsal ligaments u ... 1st metatarsal bone Tuberosity ii i ^ J j , •; ^y^i Tibialis anterior tendon Tibialis posterior tendon „ Short plantar ligament Plantar calcaneonavicular (spring) ligament Sustentaculum tali ^ L o n g plantar ligament Anatomía Esquelética Cuerpo del Astrágalo • Vista coronal – Polea • Vista axial – “Piedra Angular” – Anterior “+ ancha” • Dividido en 5 superficies – – – – – Lateral Medial Superior Inferior Posterior. Anatomía Esquelética Cuerpo del Astrágalo • Superficie Lateral consiste de: – Superficie articular larga – Fascia Maleolaris Lateralis • Articula con peroné distal – Proceso lateral • Componente no articular donde se inserta: – Lig. Astrágalo-calcaneo lateral – Ligamento anterior y posterior Astrágalo-peroneo Right foot: lateral view Fibula Anterior and Posterior tibiofibular ligaments Superior fibular (peroneal) etinaculum i Posterior talofibular ligament ) Component s of lateral Calcaneofibular ligament > (collateral) ligament Anterior talofibular ligament \ of ankle Interosseous talocalcaneal ligament Dorsal talonavicular ligament Calcaneonavicular ligament ( caneocuboid ligament J __ Blfurcate h ^ament Dorsal cuboideonavicular ligament Dorsal cuneonavicular ligaments Dorsal intercuneiform ligaments Dorsal tarsometatarsal ligament alcaneal (Achilles) endon (cut) nferior ibular peroneal) retinaculum Dorsal metatarsal ligaments Lateral talocalcaneal ligament Long plantar ligament Fibularis (peroneus) longus Dorsal c u n e o c u b o i d ligament Cuboid bone Dorsal calcaneocuboid ligament Anatomía Esquelética Cuerpo del Astrágalo • Superficie medial cuenta con 2 áreas: – Superior • Ocupada por faceta articular – Fascia malleolaris medialis • “Cola” – Inserción de lig. deltoideo. – Inferior • No articular • Mitad anterior con forámenes vasculares. respectively. d. The neck connects the head of the talus to the body. Occasionally there are small articular facets on the neck, formed by contact with the anterior surface of the distal tibia during strong dorsiflexion of the foot at the ankle (or talocrural) joint. These facets are called squatting facets. Anatomía Esquelética Cuerpo del Astrágalo • Superficie Inferior facet for the navicular head anterior subtalar – Facies articularis neck facet calcanea posterior superior neck articular surface medial tali. malleolar lateral malleolar surface head medial subtalar facet surface lateral process • Superficie cuadrilateral trochlea y cóncava en el eje posterior subtalar facet largo posterior process groove for sulcus tali groove for flexor halluciscon longus faceta flexor hallucis longus • Se articula posterior calcáneo. Figure 13.6 Right talus. Left: dorsaldel (or superior) view; right: plantar (or inferior) view. Distal is up. Natural size. respectively. Anatomía Esquelética Cuerpo del Astrágalo • Superficie posterior consiste de Tubérculos d. The neck connects the head of lar facets on the neck, formed b strong dorsiflexion of the foot squatting facets. head neck • Postero-lateral (+ Prominente) • Postero-medial – Flanquean el tendón flexor largo del 1er ortejo. superior articular surface medial malleolar surface lateral malleo surface lateral proce trochlea posterior su facet • PL también llamado Proceso de Stieda o Os Trígono (3-8% de los pacientes) posterior process groove for flexor hallucis longus Figure 13.6 Right talus. Left: dorsal (or superior) view; right: plantar (or infer 276 CHAPTER 13 Foot: Tarsals, Metatarsals, and Phalanges Anatomía Vascular • Estudiada a detalle por la incidencia de NAV después de las fracturas y luxaciones • Irrigación extra-ósea e intra-ósea extensa • Al no haber inserciones musculares hay pocas áreas de ingreso vascular Anatomía Vascular Irrigación Arterial Extra-ósea • Ramas de: – Tibial posterior(+ Aporte) – Pedia dorsal / tibial anterior – Arterias peroneas • Crean anastomosis que rodean al astrágalo en su región no cartilaginosa. Anatomía Vascular Irrigación Arterial Extra-ósea • Tibial Posterior (2 ramas) – Rama Deltoidea – Plexo vascular Anatomía Vascular Irrigación Arterial Extra-ósea • Tibial Posterior (2 ramas) – Rama Deltoidea • Pasa entre las porciones: – Astrágalo-tibial – Astrágalo-calcáneo del ligamento deltoideo. • Irriga la región medial del cuerpo del astrágalo Anatomía Vascular Irrigación Arterial Extra-ósea • Tibial Posterior (2 ramas) – Plexo vascular • Se forma por anastomosis de: – Arteria calcanea (T. Posterior) – Arteria peronea • Se encuentra sobre el tubérculo medial del astrágalo Anatomía Vascular Irrigación Arterial Extra-ósea Interosseous Muscles and Deep Arteries of Foot • Tibial Anterior (Pedia Dorsal) Dorsal view Fibularis (peroneus) longus tendon (cut) • Provee irrigación a través de 2 grupos de vasos. Fibularis (peroneus) brevis tendon (cut) Cuboid bone Lateral tarsal artery Tuberosity of 5th metatarsal bone – Ramas tarsales media / Ramas de la Arteria Maleolar anteromedial Fibularis (peroneus) tertius tendon (cut) Posterior perforating branches (from deep plantar arterial arch) Dorsal metatarsal arteries Extensor digitorum longus tendons (cu Navicular bone Dorsalis pedis artery Medial tarsal artery Lateral ) Intermediate / Cuneiform bones Medial ) Dorsal tarsometatarsal ligaments Dorsal metatarsal ligaments artery Deep plantar artery passes to contribute to deep plantar arch interosseous muscles Metatarsal bones Extensor expansions • Superficie superior del cuello del astrágalo Anterior perforating branches (from plantar metatarsal arteries) Extensor hallucis longus tendon (cut) Extensor digitorum brevis and extensor hallucis brevis tendons (cut) Dorsal digital arteries – Rama Maleolar anterolateral Plantar view • Anastomosa con arterias perforantes de la peronea = Arteria del seno tarsal. Proper plantar digital arteries C o m m o n plantar digital arteries Lumbrical muscles (cut) Deep transverse metatarsal ligament and plantar ligaments (plates) Interosseous muscles Plantar Dorsal A b d u c t o r digiti minimi muscles Plantar metatarsal arteries Flexor digiti minimi brevis muscle Deep plantar arch Lateral plantar artery (cut) Tuberosity of 5th metatarsal bone Flexor hallucis longus tendon (cut) Anterior perforating branches (to dorsal metatarsal arteries) Sesamoid bones Insertion of adductor hallucis and lateral head of flexor hallucis brevis muscles (cut) Insertion of abductor hallucis and medial head of flexor hallucis brevis muscles (cut) Medial origin of flexor hallucis brevis muscle (cut) Deep plantar artery (from dorsalis pedis artery) Posterior perforating branches (to dorsal metatarsal arteries) Plantar metatarsal ligaments (between bases of metatarsal bones) Medial cuneiform bone Anatomía Vascular Irrigación Arterial Extra-ósea • Arteria Peronea • Irrigación a través de 2 fuentes. – Plexo vascular por ramas anastomosadas: • A. Peronea + A. Calcanea (T. Posterior) • Ubicadas en tubérculo posterior de astrágalo – Arteria del seno tarsal • Ramas perforantes de la peronea se anastomosan con otras. Anatomía Vascular Irrigación Arterial Extra-ósea • Arteria del Seno Tarsal – Formada por anastomosis de varias arterias de la región lateral: • A. Antero lateral maleolar (T. Anterior) • A. Proximal/distal lateral tarsal • Arteria peronea – Principal aportador a estructuras intra-senosas y del astrágalo. Anatomía Vascular Irrigación Arterial Extra-Ósea • Arteria del canal Tarsal – Nace de la tibial posterior – 1 cm proximal al origen de las arterias plantares medial y lateral – Pasa en la mitad posterior más cerca del astrágalo que el Anatomía Vascular Irrigación Arterial Extra-Ósea • Arteria del canal Tarsal – Se anastomosa • Seno tarsal para formar la arteria del “tarsal sling” • Da ramas que pasan por la parte inferior del cuello Anatomía Vascular Irrigación Arterial Intra-Ósea • Cabeza del Astrágalo – Dos fuentes • Ramas de Tibial anterior (Pedia dorsal) – Mitad supero-medial • Tarsal Sling – – Mitad latero-inferior Anatomía Vascular Irrigación Arterial Intra-Ósea • Cuerpo del Astrágalo – Aporte mediante vasos perforantes de las 5 superficies – 2/3 laterales del cuerpo - Arteria del canal tarsal • Aporte a 4 de las 5 ramas principales del cuerpo Anatomía Vascular Irrigación Arterial Intra-Ósea • Cuerpo del Astrágalo – Tercio medial • Arteria Deltoidea – Tubérculo Posterior • Ramas pequeñas de la anastomosis posterior de: – Arteria peronea – Ramas de tibial posterior. Fracturas de Cabeza de Astrágalo Incidencia • < 10% de las fracturas del astrágalo involucran la cabeza. • Se presentan con lesiones asociadas en: – Cuello – Cuerpo – Luxación-fractura de complejo de Mecanismo de lesión • Resultado de caídas o accidentes vehiculares • Tipos de fractura – Compresión • Impacto en eje longitudinal del pie en flexión plantar – Cizallamiento • Causado por inversión • Escafoides separa porción de la cabeza del astrágalo Evaluación Clínica • Historia de flexión plantar al momento del traumatismo • Dolor en la región dorsal de la articulación astrágalo-escafoidea • Dolor a la movilización de articulación medio tarsal Evaluación Radiográfica • AP, Lateral, Oblicuas del pie • Delinear margen de cabeza y cuello (AP y Lateral) • Duda - TAC Tratamiento • No desplazadas – Yeso sin apoyo por 4 semanas – Apoyo progresivo hasta que haya consolidación y alivio del dolor Tratamiento • Desplazada – Reducción abierta y fijación interna – Meta de restaurar • Superficie articular – Art. Astrágalo escafoidea – Art. Astrágalo calcaneo • Longitud de columna medial y lateral Tratamiento • Desplazada – Fragmentos • Pequeños – retirarlos por posibilidad de bloquear articulación astrágaloescafoidea • Grandes que causen acortamiento de columna medial – Fij. Externo + Tornillos Headless/Clavos (4-6 semanas) – Conminución importante • Artrodesis astrágaloescafoidea vs Triple Artrodesis Fracturas de Cuello del Astrágalo Fracturas de Cuello del Astrágalo • 50% de las fracturas en astrágalo • 20-30% son fracturas expuestas • Alto porcentaje de fracturas se relacionan a lesiones en: – Pie, Tobillo y Columna Fracturas de Cuello del Astrágalo • Complicaciones principales son: – – – – – – Necrosis avascular No-unión Mal-unión Infección Artritis Pérdida de hueso Anatomía Cuello • Porción mas débil del astrágalo – Porosidad por vasculatura • Única porción extraarticular • Orientación: – Sagital (Caudal) – Axial (Medial – 24º) Mecanismo de Lesión • Hiper-dorsiflexión del pie – Cuello impacta a la tibia • Aplastamiento – Calcáneo y tibia (Sin movilidad de astrágalo) – Alta energía • Lesión de ligamentos interóseos (Desplazamiento anterior/medial/lateral del calcáneo) • Supinación forzada del pie – Asociada a fx maleolar Clasificación • Coltart (1952 – 2da Guerra Mundial) – Fracturas • Avulsiones, Compresión – Fracturas/Luxaciones • Fracturas del cuello/Luxación sub-astragalina • Fracturas del cuello/Luxación posterior cuerpo • Fracturas del cuerpo/Luxación Sub-astragalina – Luxaciones Clasificación Hawkins • Simple, Útil, Valor pronóstico – Fracturas de cuello (Imagen RX al momento de lesión) • Inicialmente idea: – Fracturas cuello --Osteonecrosis – Fracturas del cuerpo --Artritis Postraumatica • Estudios recientes: – Tasas similares de Necrosis avascular y artritis postraumática en ambas fracturas graphs.131 In type I injuries, onl sources of blood supply to Clasificación Hawkins • Tipo 1 – No desplazadas – Relación preservada con articulación subastragalina. A B C D – Fractura acaba en el aspecto inferior del cuello – Solo 1 de las 3 fuentes de irrigación afectada • Vasos dorsolaterales del cuello y que van hacia proximal Clasificación Hawkins • Tipo 2 – Fracturas desplazadas del cuello + Subluxación o luxación de articulación subastragalina – Luxación puede ser: • Medial (Inversión) “+” • Lateral (Eversión) – Relación entre cuerpo y tobillo preservada Clasificación Hawkins • Tipo 2 – Relación entre cabeza y escafoides y faceta anterior preservada – Al menos 2 de 3 fuentes de irrigación afectadas Clasificación Hawkins • Tipo 3 – Fractura vertical desplazada del cuello – Luxación del Cuerpo de tobillo y articulación subastragalina – Cuerpo astragalino extruido hacia posterior y medial. – Localizado entre superficie posterior de la tibia y el tendón de Aquiles. Clasificación Hawkins • Tipo 3 – Cabeza mantiene relación con escafoides – Paquete neurovascular tibial en riesgo con tensión de piel sobre hueso luxado – >50% son expuestas (Postero-medial) – 3 fuentes de irrigación afectadas Clasificación Hawkins • Tipo 4 Fractura del cuello + Luxación del cuerpo (Tobillo y Subastragalina) + Luxación de Cabeza (Astrágalo-escafoideo) – Lesión vascular al cuerpo, cabeza y cuello Evaluación Clínica Fractures and Fracture-Dislocations of the Talus ■ Chapter 39 Inferior surface • Adultos jóvenes Tarsal Superior surface Head sinus 112 + 28 140 Lateral • Hombres 3:1 process Skin necrosis Tarsal sinus 61 Tarsal canal 22 + 33 Lateral process 55 Astragalus dislocated • Lesiones asociadas Neck fractures – SME Body fractures 39-9 Talar neck and talar body fractures can be • Figure Maléolo medial accurately distinguished by evaluating the position from the fracture lumbar line exits the talus at the level of the • which Columna subtalar joint. Numbers indicate number of cases with each pattern. (From Inokuchi S, Ogawa K, Usami N: Classification of fractures of the talus: clear differentiation between neck and body fractures. Foot Ankle Int 17:748-750, 1996.) attempts to differentiate vertical fractures of the talar neck Figure 39-10 Displacement of the talus against the skin causes pressure necrosis, which can lead to development of an open fracture. These bony protrusions must be evaluated and treated immediately. (From McKeever FM: Treatment of complications of fractures and dislocations of the talus. Clin Orthop Relat Res 30:45-52, 1963.) that neck and body fractures could be distinguished more clearly by evaluating the fracture line on the inferior surface of the talus. The inferior fracture line consistently propagated either in front of or behind the lateral process of the talus. Fractures in front of the lateral process entered the sinus tarsi and thus were extraarticular talar neck frac- the ankle is distorted, with the rapid onset of swelling preventing palpation of the displaced talar body.11,101 In these injuries, the pressure and tension from the displaced bones beneath the unyielding anterior skin are accompanied by extensive hemorrhagic infiltration of the tissues and venous thrombosis of the skin.101 This can result in an area of skin necrosis over the protruding bone • Dolor, edema importante en pie • Cuerpo se palpa baseddel on the astrágalo fracture line at the superior surface of the talus caused considerable confusion in making the correct superficialmente diagnosis. In evaluating 215 fractures, they recognized Evaluación Clínica • Infiltración hemorrágica – Se promueve a la trombosis venosa de la piel con necrosis de piel sobre hueso (Urgencia - reducción) • Luxación del cuerpo posterior – Tensa capsula posterior, tendones y paquete neurovascular – Exploración – Dedos flexionados, movilidad produce dolor Evaluación Radiológica • AP, Lateral, Mortaja y Oblicuas de Tobillo y Pie • Valorar lesiones asociadas: – – – – Maléolo medial Calcáneo Escafoides Cuboides Evaluación Radiológica • Desplazamiento puede ocurrir en 2 planos: – Desplazamiento Dorsal-plantar (Rx lateral) – Desplazamiento en varo (Menos apreciada) – Vista de Canale para evaluar el cuello Part X ■ Trauma 75° 15° A B Figure 39-11 A, The Canale view, as described by Canale and Kelly, is obtained by everting and plantar flexing the foot in relation to the x-ray beam. B, The resultant image should move the calcaneus out from underneath the talus to allow an unobstructed view of the talar neck. (From Banerjee R, Nickisch F, Easley M, DiGiovanni C: Foot injuries. In Browner B, Jupiter J, Levine A, Trafton, editors: Skeletal trauma, ed 4, Philadelphia, 2009, Saunders.) the talus within the ankle mortise. The lateral radiograph stability, and minimization of complications, such as Evaluación Radiológica • TAC – Indicado para delinear la fractura y desplazamiento. (1-2mm) • RM – No recomendado en agudo – Sub-agudo • Útil para evaluar lesiones ligamentarias, osteocondrales – Útil para lesiones tipo 1 (no desplazadas) confundidas con esguinces Tratamiento • Metas – Reducción anatómica – Preservación de la movilidad – Estabilidad articular – Minimizar complicaciones • Infección, no-unión, malunión, artrosis postraumática, Necrosis avascular Tratamiento • Fracturas Tipo 1 – Conservador – Osteonecrosis de 0% (0 – 13%??) – Presencia de trazo de fractura incita a buscar el desplazamiento para la clasificación, tratamiento y pronostico. (TAC) Tratamiento • Fracturas Tipo 1 – Inmovilizar sin apoyo por 6-8 semanas con yeso (Bota chica) • “Walker” sin apoyo pero con movilidad le sigue por 4 semanas • Apoyo temprano promueve el desplazamiento de la fractura Tratamiento • Fracturas Tipo II – Conservador • Reducción anatómica confirmada por TAC (Cerrada) – 49% Requieren de reducción abierta Tratamiento • Fracturas Tipo II – Conservador • Bota con flexión plantar + Inversión/Eversión (6 semanas) • Mal posición causa deformidad, limitación en rangos de movilidad en subastragalina. Tratamiento • Tipo II – Quirúrgico • Dificultad en reducción cerrada • No relación: – Tiempo en iniciar cirugía con el desarrollo de necrosis avascular • Necrosis Avascular /Tasa de Unión afectada por: – – – – Desplazamiento Conminución Lesión de tejidos blandos Calidad de reducción Fractures and Fracture-Disl Lateral approach Posterior tibial tendon Medial approach Anterior tibial tendon Figure 39-17 Surgical approaches to the talus. (From Sangeorzan BJ: Foot and ankle joint. In Hansen ST Jr, Swiontkowski MF, editors: Orthopaedic trauma protocols, New York, 1993, Raven, p 352.) After open red placed as describe the talar neck m fragment plates provide no biome they may offer su control anatomic Corticocancellous imal tibia or the i tutes may also be comminution. No studies hav tage of using stain ture fixation. Som and Thordarson e allow subsequent implications of th POSTOPERATIVE Most authors agre fixation, the patie early motion of minimum of 10 to menced until clin Fractures and Fracture-Dislocations of the Talus ■ Chapter 39 Tratamiento fractures will be best treated with surgical reduction and mechanical advantage than anteriorly placed screws, fixation. Historically, despite a lack of sufficient evidence, which passed eccentrically through the dorsal part of the urgent treatment of displaced talar neck fractures was talar head and neck, oblique to the plane of fracture advocated as a method for reducing the risk of AVN. (Fig. 39-14). However, more recent studies suggest no relationship The advantages of placing screws from an anterior between the timing of surgery and the subsequent develdirection include the option to perform direct visualiza7,90,160 Instead, the displacement of the opment of AVN. tion of the fracture and avoidance of minor blood vessels fracture, fracture comminution, soft tissue injury (open entering posteriorly. After reduction, internal fixation is fractures), and quality of surgical reduction impact the accomplished with two titanium 3.5-mm small-fragment development of AVN, union rates, and overall result. cortical screws inserted from the talar neck into the Fractures that are relatively nondisplaced and with body.136 The cortical screws, whenever possible, should be inserted as lag screws by overdrilling the near fragment to absent or minimal comminution may be treated with provide maximum stability. It is usually possible to insert fluoroscopically guided closed reduction and minimally the two screws near the osteocartilaginous junction of the invasive or percutaneous screw fixation. Closed reduction head, either both on the medial side or one on the medial is performed as described above and stabilized with perand one on the lateral side (Fig. 39-15A). These screws are cutaneously placed K-wires. Careful fluoroscopic imaging best placed in parallel so that the fragments can compress. is used to ensure anatomic reduction. Internal fixation is If the neck is comminuted, screws might have to be placed then typically performed with screws placed across the in a nonparallel alignment to function as position screws fracture site. to maintain alignment. Lagging the fracture together Screws may be placed from an anterior to posterior under such circumstances would lead to shortening of the direction through small incisions, or alternatively, through neck, which would result in subtalar subluxation and all a posterior approach. Although Kirschner wires were used Figure 39-14 The difference between posterior and the problems associated with a malreduction.136 in many earlier studies, Kirschner wires alone should not anterior It is oftenAtdifficult placetoan times, it isto necessary insert one or more screws be used for fixation becausescrew they do insertion. not provide sufficient 153 mechanically tested variousto the through the cartilaginous covering of the head at the stability. Swanson et al screw anterior perpendicular fracture line. (From fixation devices in vitro and found that fixation with talonavicular joint. If the screw is inserted through the Swanson TV, Bray TJ, provided HolmesbyGB cartilage, Jr: Fractures of head the should talar be recessed below screws provided superior strength to that the screw Kirschner wires. The calculated theoretic maximum shear the level the cartilage 39-15B neck. A mechanical study of fixation. J of Bone Joint (Fig. Surg Am and C).54,136 Grob et al54 showed how the screws should be countersunk and force across the talar neck during active motion was 1129 74:544-551, 1992.) positioned relative to the fracture line. Failure to bury the N. This exceeded the strength provided by Kirschner wires head sufficiently will result in altered talonavicular and anteriorly inserted screws but not the strength promotion and subsequent arthritis. Rarely, the fracture vided by screws placed posteriorly. In addition, because pattern is so oblique that the only location for the screw the posteriorly inserted screws were placed across the is in the medial talar head, requiring partial removal of central portion of the talar neck and perpendicular to the medial navicular.25 The surgeon should take great care the plane of fracture, they theoretically had 101 a better Part X ■ Trauma • Tipo II – Quirúrgico • Desplazamientos menos marcados – 2 tornillos percutáneos (media rosca) de anterior a posterior • Fuerza de cizallamiento del cuello es de 1129 N, – No tolerados por clavos 0.62 o tornillos vía posterior Ad close neal to til is ob there Penn over redu Be cate o for e inclu the s posit joint In compromise of the skin about the ankle, and prompt radio reduction is needed. Any skin slough that leads to wound infection places the underlying structures at risk casts for deep infection.24,66,101 accep has b NONOPERATIVE TREATMENT well Sa An immediate closed reduction should be performed in misa the emergency department by manipulating the foot into sensi full plantar flexion, thereby bringing the head in line with ditio the body.5,35,116 The goal of reduction at this point is to diminish the risk of soft tissue compromise. Reduction of with the subtalar joint is then obtained by manipulating the acter A heel into either inversion B C or eversion, depending on stage Figure 39-15 Internal fixation of the talus with screws placed anterior to posterior. Screws may be parallel or, especially with whether the subtalar component of the dislocation is of th comminution of the talar neck (A), may be crossed. When screws must be inserted through the talar head, countersinking is 116 MF, editors: Orthopaedic trauma critical (B and C). (A, From Sangeorzan BJ: Foot and ankle joint. In Hansen ST Jr, Swiontkowski and Dunn medial or lateral (see Fig 39-13D). Pennal comp protocols, New York, 1993, Raven, p 351. B and C, From Brunner CF, Weber BG: Special techniques in internal fixation, Berlin, 1982, Springer-Verlag.) et al35 cautioned against repeated forceful attempts at Meas closed reduction. If closed reduction is unsuccessful, conta 2115 open reduction is required. rior If an anatomic closed reduction is obtained and conbut m firmed with a CT scan, definitive closed treatment may be conc attempted. However, an exact reduction of both the talar the n neck fracture and the subtalar dislocation is required. The joint Tratamiento • Fracturas Tipo II – Manejo postoperatorio con movilidad de tobillo y sub-astragalina sin apoyo. (10 - 12 semanas) – Apoyo hasta que haya datos radiográficos y clínicos de Complicaciones • Fracturas tipo II – Más común Necrosis avascular (0-50%) y Artrosis Subastragalina/Tobillo (90%) – Conminución = Peor Pronostico a motor vehicle accident, including this open type III talar (B). The talar body assumed a typical posteromedial location ach, and the patient underwent open reduction and G Tratamiento Fractures • Tipo III – Cuerpo ubicado – 50% son expuestas, resto con piel a tensión (necrosis) A Fractures and Fracture-Dislocations of the Talu A B C • Posterior y medial entre fibras del ligamento deltoideo D E F Figure 39-19 A 20-year-old female sustained multiple fractures neck fracture as seen in the lateral radiograph (A) and photograp (C and D). The body was reduced through an extensile medial ap B through two incisions (E-G). internal fixation on the overlying skin, which can result in necrosis unless prompt reduction is instituted. Tratamiento • Tipo III – Conservador – Poco alentador por: • Difícil reducción (falta de soporte ligamentario) – No evidencia que apoye tratarlo de manera conservador Tratamiento Part X ■ Trauma • Tipo III – Quirúrgico – Abordaje medial • Reducción (Maléolo fx) Figure 39-20 Osteotomy of the medial • Maléolo íntegro malleolus for treatment of fractures and Chevron Line of osteotomy Deltoid ligament dislocations of the talar body. – Osteotomía (Chevron) – Posterior a reducción se fija de If the body of the talus is trapped behind the medial la misma manera malleolus and no space seems to exist for the body, disquetraction lasis required. tipoA femoral II distractor can be placed on the medial side with one Schanz screw in the tibia and one in the os calcis. This opens up the space between the tibia and the os calcis much more efficiently than manual traction and greatly eases the manipulative reduction of 136 AUTHORS’ PREFERRED METHOD OF TREATMENT The authors recommend urgent attempted reduction of these fractures in the emergency department. If the fracture can be reduced by closed means, urgent operative treatment is not required. If closed reduction cannot be achieved, the authors recommend urgent operative treatment to relieve pressure on the skin and neurovascular Tratamiento • Postoperatorio – Unión ósea en 5-8 meses • NAV 75-100% • No unión 30% • Mal unión 30% – Artrosis Pos traumática • 70% Tobillo • 30% Sub-astragalina – Intervenciones subsecuentes Tratamiento • Tipo IV – Expuestas – Riesgo de: • Necrosis de cabeza y cuerpo • Infección – 71% de falla en procedimiento quirúrgicos • Artrosis – Grob, Kleiger, Boyd, Knight, Pnnal, Canale, Kelly, Szyszkowitz • Fusión sub-talar primaria Luxación Total del Astrágalo of injury is forced supination or pronation, usually they manifest wit coupled with plantar flexion, causing a medial or lateral lateral coupled with plantar flexion, causing a medial or lateral lateralside sideseconda second often referred to asdislocation, a pantalar dislocation. The with mechanism When these injuries areagainst closed, with no subtalar combined a force strong enough talus thethe sofs subtalar dislocation, combined with a force strong enough talus against 14,74,88,125 of injurytoisdislocate forced supination or pronation, usually they manifest with tense anterior skin, u ated with fractures thethe ankle (Fig. 39-24). ated with fractureo to dislocate ankle (Fig. 39-24).14,74,88,125 coupled with plantar flexion, causing a medial or lateral subtalar dislocation, combined with a force strong enough to dislocate the ankle (Fig. 39-24).14,74,88,125 lateral side secondary to the pressure of t talus against the soft tissue envelope.24 Ma ated with fractures of at least some portio Luxación Total de Astrágalo • También conocida como: – Luxación pantalar A • Afección completa de articulaciones: – Tobillo – Sub-astragalina – Astrágaloescafoidea B1 B1B1 AA Luxación Total de Astrágalo • Rara – Cerradas • Tensión en piel – Abiertas • Variante de expulsión completa del cuerpo sin fracturas asociadas • Mecanismo – Supinación/ Pronación forzada + Flexión plantar Luxación Total de Astrágalo • Acompañadas de Fx maleolares • Dilema – ¿Reimplantación, Fusión, Talectomía? Reimplantación • Diferentes autores: – Sneed, Coltart, Mindell, Pennal, Ritsema, Hiraizumi, Marsh, Burston, Brewster, Maffulli, Palomo-Traver. – Resultados variables – Reimplantar si hay tejido blando adherido al astrágalo. Resección y Fusión • Stimpson, Detenbeck, Kelly, Jaffe, Hiraizumi • Resección en casos de: – Contaminación – Separación completa de tejidos blandos + • Realizar Fusión tibiacalcanea. • 89% osteomielitis Luxación Sub-total del Astrágalo (Subastragalina o Peri-Astragalina) Fr ac tu re s A Fi ta gur lo e na 3 vic 9-2 ul 6 ar an A, L d a su ter bt al al ar rad jo iog in ts. rap C, h o an Luxación Sub-total del Astrágalo (Subastragalina o Peri-Astragalina) Fractures and Fracture-Disloc • Alta y baja energía (Basquetbol) Fr ac tu r A Fi ta gur Fractures and Fracture-Dislocations of the Talus ■ Chapter 39 lo e na 3 vic 9-2 ul 6 ar A B C a n A, L d at su erFigure 39-26 A, Lateral radiograph of a closed peritalar dislocation. B, Postreduction l bt al and subtalar joints. C, Postreduction computed tomography scan that show al talonavicular ar rad i jo og in ts. rap C, h o Po f a str cl ed os B uc ed Fi t p io fra gur A n erit co al ct e 3 m ar ur pu d es 9-2 te islo of 7 d t B fra to cBati he o A C d m on c y t in tu o al . Btype I: coronal (A) and sagittal (B). C, S Figure 39-27 Body fractures of the talus.gShear ar fra B C talar body. D, Crush fractureraof , Ptalar body. (Copyright Jesse C. DeLee arA juri res, fractures of the bo ctu phthe t e os icu s, fra dy re y poFigure C tr s s u 39-26 A, Lateral radiograph of a closed peritalar dislocation. B, Postreduction lateral demonstrating reduction of c . l c ste ar su tu D, of antheedu m talonavicular and subtalar joints. C, Postreduction computed tomography scan that shows a small fracture of the talar neck. t r all es Cr th th cti b en rio io • Dirección del pie y calcáneo ---Medial • Cabeza astragalina --- Dorsolateral Luxación Sub-total del Astrágalo (Subastragalina o Peri-Astragalina) • Reducción cerrada + Bota sin apoyo (4-6 Semanas) Fractures and Fractu A Fi ta gur lo e na 3 vic 9-2 ul 6 ar an A, L d a su ter bt al al ar rad jo iog in ts. rap C, h o Po f a str cl ed os B uc e d tio pe n r A co ital m a • Alta energía (47%) – Reducción abierta x obstrucción de tejidos blandos) Fi fra gur A ct e 3 u B Fracturas del Cuerpo del Astrágalo Introducción • Son 13-20% de las fracturas astragalinas • Se acompañan de – Fracturas del cuello o maléolos – Luxación – Expuestas • Lesión intra-articulares verdaderas – Incongruencia art. Astragalo-tibial (Bloqueo en dorsi-flexión) Mecanismo de Lesión • Compresión axial con alta energía (Caídas de altura o Accidentes vehiculares) • Lesión articular Tibio-Astragalina + Sub-Astragalina – Peor pronóstico – 38 - 50% Necrosis Avascular – 65 - 100% Artritis Posttraumática Clasificación • Se dividen en: – Fracturas por cizallamiento • I – Trazo coronal o sagital – IA - ID • II – Trazo horizontal – IIA – No desplazadas – IIB – Desplazadas (>3mm) – Fracturas “Crush” Tratamiento • Objetivo – Restaurar congruencia articular – Prevenir infección – Necrosis avascular • Conservador – Fracturas no desplazadas – Bota corta sin apoyo por 6-8 semanas Type IA Tratamiento Quirúrgico Type IB A • Restaurar articulaciones (T-A y S-A) para movilización temprana Type IC Type ID Figure 39-28 Shearing injuries to the talar body. This classification is for coronal and sagittal fractures only. (Copyright Jesse C. DeLee, MD.) • Fijación temprana no influye en resultado Nonoperative Treatment Nonoperative treatment is reserved for nondisplaced fractures of the talar body.13,116 These patients are treated with a below-knee non–weight-bearing cast for 6 to 8 weeks or until there are clinical and radiographic signs of fracture healing. For fractures with dislocation of the talar body (Fig. 39-29), an attempt at closed reduction is made in the emergency department, but failure to achieve closed reduction requires urgent open reduction to relieve soft tissue and neurovascular compromise. B • Trazo simple (1 abordaje) • Trazo complejo (2 abordajes) Surgical Treatment The majority of talar body fractures are displaced and will require operative treatment to restore anatomic congruity at the tibiotalar and subtalar joints and to allow early mobilization of the joints (Figs. 39-29 to 39-33).* Open talar body fractures are treated with appropriate antibiotics and surgical debridement before fixation. The surgical approach is carefully planned based on C Figure 39-29 A, Lateral radiograph depicting a portion of the talar dome rotated and facing anteriorly. B, Anteroposterior view showing the sagittal fracture line through the talar dome. C, Postoperative lateral view with lateral-to-medial screw and bioabsorbable fixation reducing the sagittal body fracture. The anteromedial and anterolateral approaches can be planned to incorporate fractures or osteotomies of the Tratamiento Quirúrgico • Alta conminución sin posibilidad de reconstrucción – Astragalectomía / Fusión Tibio-Calcanea • Post-Operatorio – Férula por 2 semanas – No apoyo por 8-12 semanas – Insistir en rangos de movilidad Part X ■ Trauma A B D G C E H F I Figure 39-31 Open talar body fracture dislocation with associated pilon and medial malleolar fractures in a 33-year-old female nurse. A, Transverse medial open wound. Lateral (B) and anteroposterior (AP) (C) views of the fracture. D, Provisionally reduced talus with a malreduced pilon fracture. E, Accurate pilon reduction after working through the talus fracture. AP (F) and lateral (G) postoperative views depicting fracture reduction of the talus, pilon, and medial malleolus. AP (H) and lateral (I) views 9 months after surgery, showing increased talar dome density. Patient remains fully ambulatory without aids but still experiences pain with daily use. arthritis is an expected result in displaced talar body fractures despite accurate reduction with stable fixation. Authors’ Preferred Method of Treatment will often require a concomitant medial or lateral malleolar osteotomy as described above. A distractor is almost always used to improve visualization. After exposure of the fracture, fragments are manipulated with K-wires as joysticks. Anatomic reduction is provision- concomitant fracture of the anterior colliculus of the medial malleolus was reduced through a separate anteromedial incision and stabilized with a single 2.7-mm lag screw (D). A D B E C F G Figure 39-33 A 37-year-old male jumped off a roof, sustaining bilateral talar body fractures. Injury radiographs (A) and computed tomography scan (B) demonstrate a talar body fracture with displacement and depression of the articular surface. The fracture was exposed through a fibular osteotomy. After exposure of the distal fibula, the anterior tibiofibular ligament (C, indicated by the elevator) was divided. An oblique osteotomy of the tibula was performed above the level of the plafond (D), to allow external rotation of the distal fibula and exposure of the fracture. A distractor was applied from the tibia to the talar neck to further improve exposure (E). The talar body was anatomically reduced and stabilized with 2.0-mm screws, and the fibular osteotomy was reduced and fixed (F and G). The syndesmotic ligaments were repaired and the syndesmosis was stabilized with a tricortical 3.5-mm screw. Postoperatively, the patient is immobilized in a short leg splint for 2 weeks to allow wound healing. Patients posttraumatic arthritis of the subtalar joint, the ankle joint, or both. Complicaciones Asociadas • Necrosis de piel • Osteomielitis • Necrosis avascular del astrágalo (8 semanas inicia) – Signo Hawkins) • Retraso en la unión (No evidencia de unión x 6 meses) • No-Unión (2.5%) • Mala-Unión (Mala reducción- Deformidad en Varo) • Artritis Post-traumática de tobillo y Subastragalina Fracturas del Proceso Posterior lar facets on the neck, formed by cont strong dorsiflexion of the foot at the a squatting facets. Anatomía head Proceso Posterior • Compuesto de tubérculos: an neck – Postero-lateral (+ Prominente, No-articular) superior articular surface medial malleolar surface lateral malleolar surface lateral process – Postero-medial trochlea posterior subtalar facet posterior process • Separados por surco del tendón flexor largo del 1er ortejo groove for flexor hallucis longus Figure 13.6 Right talus. Left: dorsal (or superior) view; right: plantar (or inferior) view 276 CHAPTER 13 Foot: Tarsals, Metatarsals, and Phalanges Anatomía • Estructuras con inserción en tubérculo Posterolateral: – Ligamento Astrágaloperoneo Posterior – Componente astragalino del ligamento PeroneoAstrágalo-Calcáneo Radiologic E, Clinical photograph shows Evaluation fracture of the posterior process (arrow) with injury of the posterior facet of the talus. Anatomía Os Trigonum D C E • Hueso accesorio asociado al tubérculo Posterolateral Figure 39-37 Posterior process fracture (arrows). Anteroposterior (A) and lateral (B) radiographs, and coronal (C) and transverse (D) computed tomography scans, demonstrate true extent of injury into the subtalar joint. E, Clinical photograph shows fracture of the posterior process (arrow) with injury of the posterior facet of the talus. • Presente en 50% de los pies os trigo num th A lateral radiographic view of the ankle best demonstrat fracture the lateral tubercle of the posterior process of th netium talus and the os trigonum. To differentiate from of the normal smooth-surfaced os trigonum, the surgeon shou the fibr remember that in an acute fracture of the posterior tal process, the fracture surfaces should be rough and irreg lar (Fig. 39-41). Because the os trigonum is reported to be unilateral more than two thirds of cases, however, compariso radiographs may not be of value.100 Paulos et al115 sugge the use of a special 30-degree subtalar oblique view help distinguish between an acute fracture and an trigonum. They found that a posterior process fracture generally larger and extends farther into the body of th talus. Bone scans can be used to distinguish among a norm os trigonum, a traumatic separation of a normal os trig num through its fibrous attachment to the talus, and fractured posterior process of the talus.115 A positive tec netium bone scan is present in all patients with fractu of the posterior process and in those with disruption the fibrous attachment of the os trigonum to the talu A B Figure 39-38 Os trigonum varies greatly in size. A, Small oval structure w more of the subtalar joint. (Copyright Jesse C. DeLee, MD.) • Varía en tamaño y puede estar fusionado al astrágalo/calcáneo – Proceso trigonal A B • Cuenta con 3 superficies: Figure 39-38 Os trigonum varies greatly in size. A, Small oval structure with smooth surfaces. B, Large structure involving more of the subtalar joint. (Copyright Jesse C. DeLee, MD.) – Anterior, Inferior y 213 Fracturas del Tubérculo Postero-Lateral Mecanismo de Lesión • Flexión plantar forzada del pie (+ Común) – Vista en bailarinas de Ballet y Soccer • Dorsi-flexión excesiva del tobillo – Tensión del ligamento astrágalo-peroneo Avulsión Fracturas del Tubérculo Postero-Lateral Evaluación Clínica • Dolor y edema en región posterior del tobillo – Incrementadas al correr, brincar, bajar escaleras, hacer sentadilla. • Dolor al movilizar tendón flexor del 1er Ortejo (Surco Adyacente) Fracturas del Tubérculo Postero-Lateral • Palpación – Dolor anterior al tendón de Aquiles y Posterior al Astrágalo – Crepitación al realizar flexión plantar • Conjunto de estos hallazgos = Síndrome del Os Trigonum Fracturas del Tubérculo Postero-Lateral • Diagnostico diferencial – Fractura del proceso lateral – Fractura del Os trigonum fusionado – Ruptura de la Sincondrosis del Os trigonum con el cuerpo Fracturas del Tubérculo Postero-Lateral Evaluación Radiológica • Radiografía lateral – Demuestra tubérculo lateral de proceso posterior del astrágalo y Os Trigonum • Radiografía con 30º de oblicuidad Sub-astragalina – Fractura aguda vs Os Trigonum • TAC – Información adicional A A B D B B Clinically, tenderne tendon and posterior t heard or felt with plant be seen with motion o of the flexor hallucis lo to the injured lateral tu D This syndrome of c 15,66, trigonum syndrome. Fractures and Fracture-Dislocations of the T diagnosis, however, n lateral process, fracture of the synchoa Clinically,ruption tenderness is present body. tendon and talar posterior to the talus, an C E plantar flexion of t heard or felt with seen process with fracture motion(arrows). of the great t Figure 39-37 be Posterior Radiologic Evaluat Anteroposteriorof(A) andflexor lateralhallucis (B) radiographs, andtendon coronal the longus (C) and transverse (D) computed tomography scans, to the injured tubercle of thev A lateral lateral demonstrate true extent of injury into the radiographic subtalar joint. Thisshows syndrome findin E, Clinical photograph fracture ofof theclinical posterior processo the lateral tubercle 15,66,95,167 (arrow) with injury of the posterior of the talus. trigonum syndrome. talusfacetand the The os mo tri diagnosis, however, necessarily inc normal smooth-surface lateral process, fracture that of a in fused remember an ao ruption of the synchondrosis of th Tratamiento • Fracturas agudas = Conservador – Bota corta de yeso con pie en 15º de equino (4-6 semanas) • Evidencia radiográfica de unión = Rehabilitación • Si continua dolor 6 meses posterior (2/3 de Px) = Escisión quirúrgica Fracturas de Tubérculo PosteroMedial • Poco comunes • También llamadas de Cedell (Dorsi-flexión + Pronación) • Masa dolorosa, firme detrás del maléolo medial con perdida del contorno posteromedial. Fracturas de Tubérculo PosteroMedial • Radiografía – Fragmento de tamaño variable situado medial y dorsal al astrágalo • Tratamiento – Conservador vs Escisión del fragmento Fracturas del Proceso Lateral Incidencia • Mal diagnosticadas como esguinces de tobillo • Son el 24% de las fracturas del cuerpo del astrágalo 13.1.1 Talus (Figures 13.6–13.7, 13.17 Anatomía The talus is called the astragalus in other anim situated between the tibia and fibula superiorly to this bone. It rests atop the calcaneus and arti lower member of the talocrural joint. Talar va a. The head is the rounded, convex, distal art of the navicular. • Comprende la región más lateral del cuerpo del astrágalo b. The body is the squarish bulk of the bone c. The trochlea is the saddle-shaped articula and medial malleolar surfaces (or facets respectively. d. The neck connects the head of the talus to lar facets on the neck, formed by contact w strong dorsiflexion of the foot at the ankle squatting facets. face head • Forma: – La pared posterior del seno del tarso – La esquina anterolateral de la faceta posterior del astrágalo anterior fa neck superior articular surface medial malleolar surface lateral malleolar surface lateral process trochlea posterior subtalar facet posterior process groove for flexor hallucis longus ne Anatomía • Involucran 2 articulaciones – Astrágalo-peronea – Calcáneo-astragalina (Posterior) • Inserciones – Ligamento AstrágaloCalcaneo lateral – Ligamento Astrágaloperoneo anterior – Ligamento Astrágaloperoneo posterior Mecanismo de Lesión • Carga axial + Dorsiflexión + Eversión/Rotación Externa • “Snowboarder Fracture” Evaluación Clínica • Síntomas parecidos a un esguince de tobillo • Dolor en cara lateral de tobillo distal al maléolo lateral • Luxación de tendones peroneos se ha descrito, se deben explorar Part PartX X■■Trauma Trauma Evaluación Radiográfica • Radiografías – AP, Lateral y Mortaja – Brodén (AP con tobillo neutral y pierna con rotación interna 20º ) • TAC AA BB Figure 39-46 A A27-year-old 27-year-oldmale malepresented presented with with late late 39-46 – Ayuda aFigure clarificar and coronal computed tomography scan (B) demonstra tamaño,and coronal computed tomography scan (B) demonstra reduction and internal fixation through a lateral appro reduction desplazamiento y and internal fixation through a lateral appro 2.0-mm screws(D). (D). 2.0-mm screws conminución B withhigh-energy high-energyinjuries injuriesororthose those managed managed non non with C D 118,159 Nonunion,while whilerare rareafter afterORIF, ORIF, is is freq freq tively. 118,159 Nonunion, tively. percent of patien lateral process talus fractures for approximately 3.5 years. ondary operative Figure 39-44 90% Anteroposterior view of the ankle with The authors reported excellent and good clinical legan internally 20 degrees suggests a large impingement. Ap results and average rotated American Orthopaedic Foot and fractu the lateral process (arrow). (Copyright Jesse DeLee, M unable return Ankle Society (AOFAS) Hindfoot Score of 93 out ofC.to 100. activity. The best result scores, hindfoot motion, and least pain were noted in patients with large fracture fragments (type Results are affe I) that were anatomically reduced and rigidly Fifty sis fixed. and by the dev percent of patients treated nonoperatively fragment. required secSubtalar • Hawkins (3 Tipos) Figure 39-44 Anteroposterior view of the ankle with the ondary operative debridement because of talus nonunion or occ fractures leg internally rotated 20 degrees suggests a large fracture of – Tipo I impingement. Approximately 20% of patients were the lateral process (arrow). (Copyright Jesse C. DeLee, MD.) patients and is m • Fractura simple, fragmento unable to return to their preinjury level of athletic grande activity. ResultsFigure are affected the presenceofoflateral subtalar arthro39-45byClassification process talus frac sis and byA,the development of nonunion of the fracture Baker JF, Liu DF, Stephens MM: The management and – Tipo II fragment. 2010. Subtalar arthrosis associated with lateral process oposterior view of the ankle with the • Conminuta que involucra talus fractures occurs in approximately 15% to 25% of 20 degrees suggests a large fracture of superficie articular y and is more frequently seen in those patients rrow). (Copyright Jesse C. DeLee, MD.) patients Clasificación proceso lateral – Tipo III 39-45 Figure Classification of lateral process talus fractures as described by Hawkins Baker JF, Liu Stephens MM: The management and outcome of lateral process ta •A,Fractura enDF, “Chip” •2010. Porción antero-inferior (solo afecta articulación sub-astragalina) fication of lateral process talus fractures as described by Hawkins. (Modified with permission from Perera ephens MM: The management and outcome of lateral process talus fractures. Foot Ankle Surg 16:15-20, Tratamiento • Basado en: – Tamaño del fragmento (Grande – RA + Fijación) – Conminución (Escisión) – Desplazamiento • Fragmentos pequeños / mínimamente desplazados – Bota de yeso sin apoyo x 4-6 semanas Procedimientos de Salvamento Secuelas • Tres problemas: Dome DomeDome collapse collapse collapse A A A B B B – Perdida ósea • Colapso y deformidad • Traumática, sepsis o necrosis avascular Figure 39-49 The patient had a comminuted Figure 39-49 Thehad patient had a comminuted Figure 39-49 The patient a comminuted fracture that was treated a in closed talar fracture was a closed talartalar fracture that was that treated intreated a in closed manner with strict non–weight bearing. manner with strict non–weight bearing. manner with strict non–weight bearing. A, Approximately 5 months after injury, the the A, Approximately 5after months after injury, A, Approximately 5 months injury, the patient developed and radiographs patient developed and radiographs patient developed pain,pain, andpain, radiographs revealed avascular necrosis and collapse revealed avascular necrosis and collapse revealed avascular necrosis and collapse (arrows), despite non–weight bearing. (arrows), despite non–weight bearing. (arrows), despite non–weight bearing. B, Magnetic resonance image reveals totaltotal B, Magnetic resonance image reveals B, Magnetic resonance image reveals total involvement of talus. the C, Talectomy involvement of talus. the talus. C, Talectomy involvement of the C, Talectomy was was was performed, verifying destruction of talus. the performed, verifying destruction of talus. the talus. performed, verifying destruction of the D, Radiographs 1 year later. E, Clinical D, Radiographs 1 year later. E, Clinical D, Radiographs 1 year later. E, Clinical examination 1 year later. Patient has returned examination 1 year later. Patient has returned examination 1 year later. Patient has returned to work as a as mechanical engineer. to awork a mechanical engineer. to work as mechanical engineer. – Mal unión (Mala reducción) – Artritis severa de articulaciones aledañas al astrágalo C C C E D E E D D Artrodesis • Identificar articulaciones afectadas (Deformidad) – Tobillo – Sub-astragalina – Astrágalo-escafoidea • A valorar – Infección ¿? – Piel en buenas condiciones – Procedimiento brindara extremidad funcional Artrodesis de Tobillo • Se recomienda uso de tornillos con combinación de placas. • NO se recomienda uso de clavo retrogrado – Involucra articulación sub-astragalina Astragalectomía • Traumática o electiva (+ Artrodesis de Blair 1608) • Subtotal – Ausencia de domo o cuerpo • Total – Astrágalo entero removido Astragalectomía • Blair – 71% Buenos Resultados – 43% No-Unión – 28% Pseudoartrosis – Colapso a largo plazo + modificación de calzado – Procedimiento de salvamento, no de primera opción Reemplazo Prostético Astragalino • Información limitada • Harnroongroj et al – 16 pacientes tratados – Seguimiento a los 9.5 años – Resultados satisfactorios Fusión Tibio-Calcanea • Utilizado cuando las lesiones afectan articulación subastragalina. • Se puede realizar con: – – – – – Tornillos (6.5), Placas Clavo intramedular, Fijación externa Injertos vascularizados de perone. • Poco dolor pero funcionalidad limitada. Placas de Fusión • Placas anteriores (Sanders et al) – 100% tasa de fusión con osteotomías y resección cartilaginosa – Poca satisfacción por rigidez y limitación de actividades – Promedio de 3 hospitalizaciones para procedimientos (20-107 días intrahospitalarios) – Gastos de aproximadamente $62,174 dlls por paciente – ¿Procedimiento de Salvamento vs Amputación? Otras opciones • Fijación Externa – Resultados variables • Estabilización con clavo intramedular – Clavo retrogrado supracondileo femoral. – Únicamente rimado sin resección de cartílago lleva a no-unión