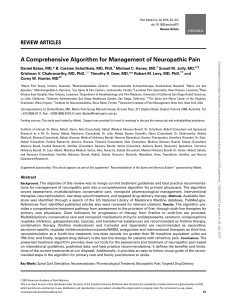
Support Care Cancer DOI 10.1007/s00520-015-3060-7 ORIGINAL ARTICLE Evaluation of the treatment of chronic chemotherapy-induced peripheral neuropathy using long-wave diathermy and interferential currents: a randomized controlled trial Katarina Lindblad 1 & Leif Bergkvist 2 & Ann-Christin Johansson 3 Received: 2 September 2015 / Accepted: 14 December 2015 # Springer-Verlag Berlin Heidelberg 2015 Abstract Purpose The purpose was to investigate the effects of longwave diathermy in combination with interferential currents (interferential therapy and long-wave diathermy at high power (ITH)) in comparison with long-wave diathermy at a power below the active treatment dose (long-wave diathermy at low power (LDL), control group) on sensory and motor symptoms in patients with chronic chemotherapy-induced peripheral neuropathy (CIPN) in the lower extremities. Methods Sixty-seven patients with chronic CIPN were randomized to 12 weeks of either ITH or LDL. Follow-up assessments were performed after the treatment period and at 37 weeks after randomization. The primary outcome was pain (Numeric Rating Scale (NRS)), and the secondary outcomes were discomfort, nerve symptoms, subjective measurement of dizziness (Dizziness Handicap Inventory), and balance. Differences within and between groups were analyzed. Results Pain intensity decreased significantly only in the LDL group directly after the treatment period from NRS median 25 to median 12.5 (P = 0.017). At the 37-week follow-up, no changes were detected, irrespective of group (NRS 13 vs. 20, P = 0.885). Discomfort decreased significantly in both groups at both 12 and 37 weeks after the baseline (P < 0.05). Balance disability showed significant declines in both groups at 12 and 37 weeks (P = 0.001/0.025 in the ITH group vs P = 0.001/<0.001 in the LDL group). Balance ability (tightened Romberg test) increased significantly at both 12 and 37 weeks in both groups (P = 0.004/<0.040 in the ITH group) but did not improve in the LDL group at any of the follow-up time points (P = 0.203 vs P = 0.383). The onelegged stance test was unchanged in the ITH group after 12 weeks but improved 37 weeks after baseline (P = 0.03). No significant changes were observed in the LDL group at any of the follow-up time points. Conclusion This study provides no support for the use of a combination of long-wave diathermy and ITH as a treatment option for patients with chronic CIPN. However, the chronic CIPN symptoms decreased with time irrespective of the treatment. Keywords Physical therapy . Electrotherapy . Diathermy . Interferential current . Cancer Introduction * Katarina Lindblad [email protected] 1 Department of Surgery, Västmanland County Hospital, 721 89 Västerås, Sweden 2 Department of Surgery, Centre for Clinical Research, Uppsala University, Västmanland County Hospital, 721 89 Västerås, Sweden 3 Department of Physiotherapy, School of Health, Care and Social Welfare, Centre for Clinical Research, Mälardalen University, Västmanland County Hospital, Box 883, 721 89 Västerås, Sweden The use of chemotherapy has led to prolonged remission and survival in numerous human cancer diseases. The progress and development of chemotherapeutic agents has, however, come at the cost of toxicity, which may lead to long-lasting negative side effects. The nervous system, both centrally and peripherally, has turned out to be especially sensitive to these agents. Chemotherapy-induced peripheral neuropathy (CIPN) is common and includes sensory deficit, pain, loss of motor functions, and impaired proprioception, which in turn may affect balance and fine motor skills [1, 2]. It is mainly localized to Support Care Cancer the peripheral parts of the extremities and may be transient or permanent [3] and thus affecting the quality of life and functional capacity of the patients [4]. CIPN is a common, potentially severe, and often doselimiting side effect of exposure to numerous classes of antineoplastic agents, including platins, taxanes, vinca alkaloids, bortezomib, and thalidomide [5]. The incidence of CIPN varies according to the agents used but increases when patients receive a mixture of several chemotherapeutic agents and when they have concurrent comorbidities with the neuropathies, e.g., diabetes [2, 6]. Currently, no evidence-based treatment is available for acute or chronic CIPN. A variety of different drugs or drug combinations have been clinically tested, but the value of these treatments remains uncertain [7]. Although some promising results have been reported regarding the effects of nutraceuticals in the prevention or treatment of CIPN (magnesium, calcium, vitamins E and B6, glutamine, glutathione, N-acetyl cysteine, omega-3 fatty acids, acetyl-L-carnitine, and alpha lipoic acid), additional research is needed to evaluate the effect of these treatments [8]. Many patients with chronic CIPN are referred to physical therapy, which is based more on clinical experience and tradition than on scientific evidence. Acupuncture and electrical sensory stimulation have also been evaluated, but only in studies with small samples and without convincing treatment effects [9, 10]. In a nonrandomized study without a control group performed by Smith et al., sensory electrical stimulation was tested [11]. The intensity of the treatment was gradually increased over 10 days. A 20 % reduction of pain was detected in 15 out of the 16 participating patients. However, the pain gradually returned to pretreatment levels 1 or 2 months after the treatment period. Another nonrandomized study that used Scrambler therapy, which minimizes pain signals via cutaneous nerve block, reported reduced pain and an increase in the quality of life of participants [12]. Significant changes in pain from the baseline were observed at 14, 30, 60, and 90 days after the baseline measures and treatment. Likewise, Pachman et al. showed decreased pain, tingling, and numbness after ten daily treatment sessions of Scrambler therapy on patients with chronic CIPN [13]. Our clinical experience indicates that treatment with long-wave diathermy may decrease chronic CIPN symptoms, as pain is assumed to be reduced by electromagnetic radiation, which increases circulation and heat according to the capacitor method [14]. Interferential therapy is an electrophysical method that is based on the application of an electric field in the painful area via four electrodes or vacuum cups that are placed on the skin. Increased blood circulation and pain relief are supposed to be achieved [15]. Interferential therapy uses two different intermediate frequencies (1001–10,000 Hz) of alternating currents in the painful area. The two medium-frequency currents come together, thereby creating a stream with a lower frequency (1– 1000 Hz) or beats per second (bps). The treatment effect corresponds to the gate control theory: the inhibition of pain signals in small-diameter fibers by activity in large-diameter Aβ fibers by spinal neurons [16]. Some studies have reported the reduction of pain by interferential currents after pain was experimentally induced or induced by cold in otherwise pain-free volunteers compared with a control or placebo [17–19]. However, research on the effect of electrical inhibition on chronic CIPN is limited, even if this approach is used in clinical practice for reducing chronic CIPN. The aim of this study was to investigate the effects of combination therapy with long-wave diathermy at high-power and interferential currents compared with long-wave diathermy at low power (control group) on sensory and motor symptoms in patients with chronic CIPN in the feet and lower legs. Sensory and motor symptoms were defined as pain, discomfort, numbness, and balance impairment. Method Study design This was a randomized controlled trial with assessment performed before randomization and 12 and 37 weeks after the baseline measurements. The study protocol was registered in Clinical Trials Gov, reference number NCT02088996. Study population The participants had chronic CIPN symptoms after chemotherapy treatment, as assessed by their responsible physician. The patients were recruited consecutively from the Västmanland County Hospital, Västerås, Sweden, from January 2010 to February 2014; they were all referred to the physical therapy department by the consulting physician. The inclusion criteria were as follows: patients aged over 18 years who received chemotherapy and had documented side effects, such as numbness, tingling, pain, or a swelling sensation in the feet/lower legs. The exclusion criteria were pregnancy, thrombosis, thrombophlebitis in the feet or lower legs, muscle cramps, acute bleeding disorders, dementia, type 1 diabetes mellitus, open sores on the feet or lower legs, peripheral sensory neuropathies caused by factors other than chemotherapy, and ongoing chemotherapy with drugs known to cause chronic CIPN. An independent physical therapist interviewed potential participants to check for eligibility. Patients who met the study criteria were informed about the study and asked to participate in it. Support Care Cancer The patients who gave their approval for participation were randomized into one of the two study groups: & & Interferential therapy and long-wave diathermy at high power (ITH) Long-wave diathermy at low power (LDL) The patients were informed that they would be randomized into one of the groups: ITH or LDL. The LDL treatment was chosen as a placebo. Sixty-seven participants entered the trial; 59 were followed up after 12 weeks and 50 patients were followed up after 37 weeks (Fig. 1). There were no significant differences between groups before treatment (at the baseline) (Table 1). Treatment Both groups were treated by a physical therapist once a week for 12 weeks. Treatment manuals were prepared beforehand, and treatments were administered according to these manuals. Treatment was considered complete in both groups if it had been administered at least nine of the 12 planned occasions (75 %). distally and dorsally on the patient’s leg. An electrode gel was applied to the sole of the patient’s foot. Treatment was delivered via application of circular motions and light pressure of the active electrode to the sole of the foot for 6 min (Fig. 2). The treatment manual is available [20]. Interferential therapy was performed on the lower legs with the patient placed in a supine position. Treatment was administered using an Electro Stimulation Device ES 520 & Vacuum Unit for 15 min/lower leg. Four vacuum electrodes were placed on the lower leg, with a channel intersecting the other. The electrodes were placed medially and laterally (Fig. 3). Wet electrode sponges were placed in the vacuum electrodes. A frequency of 0–100 Hz was used, which provides both sensory and motor nerve stimulation. When the stimulation began, the patients were asked to indicate when the stimulation felt strong but did not hurt. The treatment manual is available [21]. The long-wave diathermy at low power group (control group) The control group was treated with only LDL in the low-effect range, which was applied to the soles of the feet using a Skanlab 25 Body Wave® apparatus for 6 min. This low effect was not expected to have any therapeutic effect. The treatment manual is available [20]. The interferential therapy and long-wave diathermy at high power group Measurements This treatment group received ITH. Long-wave diathermy was administered at the soles of the feet using a Skanlab 25 Body Wave® apparatus. A ground electrode rod was placed All measurements were performed on both groups at the baseline and at 12 and 37 weeks after the baseline by an independent physical therapist who was not involved in the treatment. Fig. 1 Flowchart Assessed for eligibility (n = 73) Excluded (n = 2) declined participation (n = 1) Randomized (n = 70) Interferential therapy and long-wave diathermy at high power (n = 34) Did not meet the inclusion criteria (n = 3) Long-wave diathermy at low power (n = 33) Withdrew from planned treatment/died (n=3) Withdrew from planned treatment/died (n=5) Follow-up 12 weeks after treatment (n = 29) Withdrew from planned follow-up (n=3 ) or died (n=2) Follow-up 12 weeks after treatment (n = 30) Withdrew from planned follow-up (n=4 ) Follow-up 37 weeks after treatment (n=24 ) Follow-up 37 weeks after treatment (n=26 ) Support Care Cancer Table 1 Baseline demographics, including name, age, sex, diagnosis, and information of chemotherapy ITH group n = 34 LDL group n = 33 Sex, women/men 17/17 17/16 Age, mean (SD) (years) 62.77 (±12.1) 65.26 (±9.0) Diagnosis, frequency Uterine cancer 2 1 Pancreatic cancer Gastric cancer 0 1 1 0 Cervix cancer 2 1 Lymphoma Colon cancer 0 17 4 12 Ovarian cancer Breast cancer 2 1 2 1 Basalioma 1 0 Rectal cancer Small-bowel cancer 7 1 10 1 25 4 23 5 1 1 3 0 3 1 0 1 11 (12.0) 12 (9.3) 11 (6.5) 11 (3.9) Chemotherapeutic agent, frequency Oxaliplatin Taxanes (paclitaxel, docetaxel, paclitaxel/carboplatin) Vincristine Capecitabine Cisplatin Vinblastine Months between completed chemotherapy and randomization, means (SD) Number of chemotherapy cycles, means (SD) Pain intensity and discomfort Numeric Rating Scale (NRS) was used for measuring the intensity of pain. This is a reliable instrument that has been validated for patients with cancer [22, 23]. Patients rated their pain from 0 to 100, with 0 reflecting no pain and 100 reflecting the worst possible pain. Discomfort was defined as an uncomfortable feeling of not knowing where the feet are in relation to the room; this was also assessed using an NRS in which 0 represented no discomfort and 100 represented the worst possible discomfort. For the analysis of the nerve symptoms, the depictions of legs with drawn symptoms were divided into ten zones, four on the feet and six on the legs, by using a transparent template with all ten zones marked out. The mean number of zones marked with symptoms of numbness was then calculated for each patient based on the sum of zones for both legs (Fig. 4). This method was created by the researchers and has not been tested for reliability and validity. Balance disability/ability testing Three tests were undertaken: 1. Measurement of a subjective experience of balance via the Dizziness Handicap Inventory, for the assessment of patients’ experience of their balance [26]. The questionnaire contains 25 items and has good reliability in vestibular disorders/disabilities [27]. In this study, the form was abbreviated and contained only 15 questions: 10 questions that were constructed for vertigo symptoms were omitted, as they were considered inappropriate for this patient group. 2. Tightened Romberg test (tandem standing with the hands crossed and touching the shoulders, maximum 60 s) [28, 29]. 3. One-legged stance test (standing on one leg with the hands crossed and touching the shoulders, maximum 30 s) [28]. The tests (1 and 2) have good validity and reliability when applied to healthy elderly females. In the tightened Romberg test and one-legged stance test, the patient was allowed three attempts of each test, and the best result was recorded. The tests were performed with closed eyes. The timer was stopped when the patient moved the feet/arm position and/or looked when the eyes should be closed. The means of both legs regarding both the tightened Romberg test and the one-legged stance test were calculated for each patient, and this value was used for all descriptions and analyses. Other measures Baseline demographics, including name, age, sex, diagnosis, and chemotherapeutic agent, were also recorded. Data analyses Nerve symptoms The definition of nerve symptoms included sensations of pins and needles, tingling, and paresthesias. Patients were asked to draw the occurrence of any of the nerve symptoms of their legs and feet on a sketch, which was based on a pain-drawing sketch [24, 25]. As there are few available studies in this field, we performed a post hoc power analysis based on data from the first 26 patients included in the study. We estimated that the clinically significant difference in pain intensity between the treatment groups was 17 (SD, 22) units of the NRS, with a power of 80 % and an alpha of 0.05. Support Care Cancer Fig. 2 The Skanlab 25 Body Wave® device positioned to treat chronic CIPN This estimation required 31 participants in each group. Regarding the Dizziness Handicap Inventory, we estimated that a clinically significant difference between groups corresponded to a difference of 6 units (SD, 7), which required 28 patients in each group, with a power of 80 % and an alpha of 0.05. Based on our experience from the first 26 patients included in the study, the dropout rate was 15 %; thus, we decided to include 70 patients in the current study. Comparisons between groups were performed according to the intention to treat principle, using the Mann–Whitney U test for ordinal data and the chi-squared test for nominal data, Fig. 3 The Electro Stimulation Device ES 520 & Vacuum Unit device positioned to treat chronic CIPN and differences within groups were analyzed using the Wilcoxon test. Differences regarding the mean of zones with numbness before and after treatment were calculated for each patient and compared between groups using the chisquared test. Because not all patients had pain at the baseline, we performed an adjustment for pain at the baseline using linear regression analyses. In these analyses, the dependent variables were pain intensity at 12 and 37 weeks, and pain at the baseline and group was independent variables. Support Care Cancer Thirty-seven weeks after the baseline, the medians for pain had decreased to 12.5 in the ITH group, but increased to 20 in the LDL group; however, none of these changes was significant (P = 0.173 in the ITH group and 0.146 in the LDL group) (Table 2). Discomfort decreased significantly in both groups at both 12 and 37 weeks after the baseline (P < 0.05) (Table 2). Nerve symptoms All patients reported numbness prior to treatment. The median number of affected zones in the ITH group was 5.5 at the baseline, and it significantly decreased to four zones 12 weeks after the baseline (P = 0.003). Similarly, the number of numbness zones decreased in the LDL group from five to four (P = 0.002). Both of these improvements remained after 37 weeks (Table 2). Balance disability/ability Fig. 4 Sketch of numbness Significance was set at P ≤ 0.05. Collected data were processed using the Statistical Packages for the Social Sciences (SPSS), version 22. The study was approved by the Research Committee of Uppsala University, no. 2010/364, 2011-02-28. Results Comparison of differences between groups Changes in outcome variables were not significantly different between the two groups at any of the follow-up time points (Table 2). After an adjustment for baseline values of the primary outcome, variable pain intensity, the analyses showed that baseline pain values had no significant effect on the results (slope coefficient, −0.242; P = 0.957 (pain intensity at 12 weeks) and slope coefficient, 2.873; P = 0.613 (pain intensity at 37 weeks)). Both the ITH group and the LDL group showed significant declines in balance disability between before and after the test. The median value of the DHI decreased from 14 at the baseline to 8 after 12 and 37 weeks in the ITH group (P = 0.001 and 0.025, respectively). The corresponding values in the LDL group were 14 at the baseline, with a decrease to 9 (P = 0.001) 12 weeks after the baseline and 10 (P < 0.001) 37 weeks after the baseline. In the tightened Romberg test, the mean value at the baseline for both the right and left legs in both groups was 9 s. In the ITH group, there was a significant (P = 0.004) improvement at 12 weeks after the baseline, to 11 s, and a further significant (P = 0.040) improvement to 13 s at 37 weeks after the baseline. Balance did not improve in the LDL group at any of the follow-up time points (P = 0.203, 12 weeks after the baseline and P = 0.383, 37 weeks after the baseline). The results of the one-legged stance test were unchanged in the ITH group 12 weeks after the baseline but improved significantly from 5 to 7 s 37 weeks after the baseline (P = 0.03). No significant change in the one-legged stance test was observed in the LDL group at any of the follow-up time points (Table 2). Comparison within groups Pain intensity and discomfort Discussion Pain intensity was 30 (median) in the ITH group at the baseline and 25 in the LDL group; nine patients in the ITH group and 13 patients in the LDL group rated pain as 0 at the baseline. Twelve weeks after the baseline, pain had decreased to 20 in the ITH group and to 12.5 in the LDL group. The results of these analyses were significant only in the LDL group (P = 0.55 in the ITH group and 0.017 in the LDL group). The aim of this study was to compare the effect of combination therapy (long-wave diathermy at high-power and interferential currents) with LDL (control group) for sensory and motor symptoms in patients with chronic CIPN in the feet and lower legs. Our results showed some improvement in both treatment groups over time, although no significant differences were detected between groups. The chronic Support Care Cancer Table 2 Medians, means, and dispersion values at the baseline and at 12 and 37 weeks Baseline Pain intensity (NRS 0–100), median (q1–q3) Numbness zone frequency (0–10), median (min–max) Discomfort (NRS 0–100), median (q1–q3) DHI (0–60), median (q1–q3) Tightened Romberg test, eyes closed, both legs (0–60 s), mean (SD) One-legged stance, eyes closed, both legs (0–30 s), mean (SD) After 12 weeks After 37 weeks ITH LDL ITH LDL P valuea ITH LDL P value 30 (0–50) 25 (0–58) 20 (0–40) 13* (0–43) 0.804 13 (0–47) 20 (0–40) 0.885 6 (1–10) 5 (2–10) 4** (0–8) 4** (2–8) 0.938 4*** (0–7) 4*** (0–7) 0.828 60 (34–80) 70 (35–80) 40*** (23–53) 53** (30–70) 0.503 38* (20–54) 50* (30–75) 0.816 14 (8–34) 9 (12.2) 14 (11–22) 9 (10.8) 8*** (1–20) 11* (11.1) 9*** (4–16) 12 (15.4) 0.489 0.241 8* (4–22) 13* (15.9) 10*** (6–16) 8 (6.09) 0.922 0.297 5 (5.2) 4 (4.2) 5 (4.7) 4 (2.7) 0.994 7* (6.6) 5 (83.5) 0.784 ITH interferential therapy and long-wave diathermy at high power, LDL long-wave diathermy at low power a The P values represent the comparison of differences in changes within each group from the baseline to 12 and 37 weeks after the baseline, respectively *P ≤ 0.05, **P ≤ 0.01, ***P ≤ 0.001 CIPN symptoms decreased with time irrespective of treatment which might be an effect of the natural history of chronic CIPN. According to Pachman and coworkers, the CIPN symptoms decrease with time, but for some patients, the symptoms are persistent [30]. It cannot be ruled out that the improvement that the patient experienced was an effect of the natural course. These results are in contrast with the clinical impression of the treatment response reported for selected patients. However, these were probably influenced by the fact that the symptoms are troublesome and influence daily life and that the patients value and appreciate every effort made to decrease their symptoms. This highlights the need for randomized studies aimed at evaluating treatment effects over time to disentangle the true treatment effects from the natural course of the disease. We cannot be absolutely sure that the treatment that was administered to the control group was without effect; however, this treatment was far below the intensity that is believed to have a therapeutic effect. If we had left the control group without any treatment at all, the difference in the attention provided to the groups would have represented a problematic bias. The possible placebo effect from receiving treatment was assumed to be equal in both groups since both groups got similar treatment attention. In this study, we chose to administer a combination of treatments to the treatment group, i.e., interferential currents and long-wave diathermy at high power, because the idea was that both methods, given at the recommended treatment dosage, stimulate the nerves and complement each other. The theoretical background for our treatment was based on the gate control theory [31]. Acupuncture is, at least in part, a parallel treatment mechanism that has also been evaluated on this patient group by Rostock et al. [32]. Their study included four relatively small treatment groups (14–17 participants), and in agreement with our results, these researchers did not find any significant differences between treatments. In the study reported by Coyne et al. [12], the effect of Scrambler therapy was evaluated in patients with chronic CIPN. Those authors showed that the pain was significantly reduced after 10, 30, 60, and 90 days. The same pattern was seen in the nonrandomized study on chronic CIPN patients by Pachman et al.; these authors, however, demanded placebo-controlled studies [13]. In a study performed by Smith et al. [11], the pain reoccurred in most of the patients 1 to 2 months after the administration of treatment with electrostimulation. However, none of these studies included a control group, which renders it difficult to draw any conclusions regarding the treatment. In our study, the LDL group exhibited significantly reduced pain at 12 weeks; however, at 37 weeks, the pain had reoccurred, which was similar to the pattern reported by Smith et al. The present study had some strength in that the physical therapist that performed all the measurements and tests was independent. Further, the study comprised follow-up sessions, both directly after the treatment and a long-term follow-up. The study also had some limitations. First, 25 % of the 67 patients who received treatment were not followed up. This can be explained by the vulnerability of this patient group and the generally weak health condition of several patients. Unfortunately, ten patients died during the follow-up period (Fig. 1). Second, we could not report the patients’ chemotherapy dosages; unfortunately, doses are written on separate dose Support Care Cancer charts for logistic reasons and kept in a separate department in our hospital. Presentation of dosage might, however, have added valuable information. Third, the sketches used for describing the nerve symptoms have not been psychometrically evaluated. This method was developed by our research group, as we did not find any established method in Swedish for describing the distribution of chronic CIPN symptoms. Similarly, the validity of the Dizziness Handicap Inventory can be questioned, because several items were omitted and it had not been psychometrically tested on this patient group. Generally, it is difficult to find sensible and clinical applicable measurement methods for the nerve symptoms and functional limitations of these patients. The FACT/GOG-NTX which has the advantage of being validated in Swedish could have been considered [33], but many items in this questionnaire do not capture entities which correspond to our aim. In general, there is a need for valid and reliable measurement methods in Swedish, for capturing the functional limitations of patients with chronic CIPN symptoms. As pain intensity was the primary outcome variable, the study sample was underpowered in relation to pain. According to our power calculation, we expected a difference of pain reduction of 17 points. This can be questioned, since according to Farrar et al. [34], a clinically significant pain reduction of at least 30 % is regarded as relevant. If we had chosen this benchmark, the study sample could have been reduced. By including 67 patients, we increased power in relation to the second outcome variable Dizziness Handicap Inventory. The measurement of pain intensity does not seem to be the ultimate method for capturing the symptoms of these patients. The less specific concept of Bdiscomfort^ might better describe the chronic CIPN symptoms. In conclusion, this study showed some improvement in chronic CIPN symptoms 3 and 6 months after treatment by chemotherapy. However, this improvement occurred irrespective of treatment by ITH. Considering costs and required treatment time in relation to treatment outcome, we cannot recommend long-wave diathermy in combination with interferential currents as a treatment option in clinical practice for patients with chronic CIPN. References Acknowledgments The study was supported by research grants from the Västmanland County Hospital, Västerås, Sweden. We are grateful for the support provided by physical therapists Jenny Ulmestedt and Karin Tissier Knutsgård, for helping with the assessment and evaluation of the patients. We also acknowledge Berit Werner-Erichsen, Head of Physical Therapy, Surgical Department, Västmanland County Hospital, Västerås, who gave permission for performing the study. 16. 18. Compliance with ethical standards 19. Conflict of interest The authors declare no conflicts of interest. 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 17. Grisold W, Cavaletti G, Windebank AJ (2012) Peripheral neuropathies from chemotherapeutics and targeted agents: diagnosis, treatment, and prevention. Neuro Oncol 14(4):iv45–iv54 Visovsky C, Collins M, Abbott L, Aschenbrenner J, Hart C (2007) Putting evidence into practice: evidence-based interventions for chemotherapy-induced peripheral neuropathy. Clin J Oncol Nurs 11:901–913 Cavaletti G, Alberti P, Frigeni B, Piatti M, Susani E (2011) Chemotherapy-induced neuropathy. Curr Treat Options Neurol 13:180–190 Rao RD, Flynn PJ, Sloan JA, Wong GY, Novotny P, Johnson DB, et al. (2008) Efficacy of lamotrigine in the management of chemotherapy-induced peripheral neuropathy. Cancer 112:2802– 2808 Ferrier J, Pereira V, Busserolles J, Authier N, Balayssac D (2013) Emerging trends in understanding chemotherapy-induced peripheral neuropathy. Curr Pain Headache Rep 17:364 Stillman M, Cata JP (2006) Management of chemotherapy-induced peripheral neuropathy. Curr Pain Headache Rep 10:279–287 Wolf S, Barton D, Kottschade L, Grothey A, Loprinzi C (2008) Chemotherapy-induced peripheral neuropathy: prevention and treatment strategies. Eur J Cancer 44:1507–1515 Schloss JM, Colosimo M, Airey C, Masci PP, Linnane AW, Vitetta L (2013) Nutraceuticals and chemotherapy induced peripheral neuropathy (CHRONIC CIPN): a systematic review. Clin Nutr 32(6): 888–893. doi:10.1016/j.clnu.2013.04.007 Donald GK, Tobin I, Stringer J (2011) Evaluation of acupuncture in the management of chemotherapy-induced peripheral neuropathy. Acupunct Med 29:230–233 Schroeder S, Meyer-Hamme G, Epplee S (2012) Acupuncture for chemotherapy-induced peripheral neuropathy (CHRONIC CIPN): a pilot study using neurography. Acupunct Med 30:4–7 Smith TJ, Coyne PJ, Parker GL, Dodson P, Ramakrishnan V (2010) Pilot trial of a patient-specific cutaneous electrostimulation device (MC5-a calmare(R)) for chemotherapy-induced peripheral neuropathy. J Pain Symptom Manag 40:883–891 Coyne PJ, Wan W, Dodson P, Swainey C, Smith TJ (2013) A trial of scrambler therapy in the treatment of cancer pain syndromes and chronic chemotherapy-induced peripheral neuropathy. J Pain Palliat Care Pharmacother 27:359–364 Pachman DR, Weisbrod BL, Seisler DK, Barton DL, FeeSchroeder KC, Smith TJ, et al. (2015) Pilot evaluation of scrambler therapy for the treatment of chemotherapy-induced peripheral neuropathy. Support Care Cancer 23:943–951 Sluka KA (2009) Transcutaneous electrical nerve stimulation and interferential therapy. In: Sluka KA, Walsh D (eds) Transcutaneous electrical nerve stimulation and interferential therapy. IASP Press, Seattle, pp. 166–190 Interferens - Cefar. http://www.cefar.se/treatments.asp?id=&cat= Interference. Accessed 23/3, 2015 Molin B, Norrbrink C, Lundeberg T, Lund I, Lundeberg S (2010) Om smärta: ett fysiologiskt perspektiv. Studentlitteratur, Lund Johnson MI, Tabasam G (2003) An investigation into the analgesic effects of interferential currents and transcutaneous electrical nerve stimulation on experimentally induced ischemic pain in otherwise pain-free volunteers. Phys Ther 83:208–223 Johnson MI, Wilson H (1997) The analgesic effects of different swing patterns of interferential currents on cold-induced pain. Physiotherapy 83:461–467 Stephenson R, Johnson M (1995) The analgesic effects of interferential therapy on cold-induced pain in healthy subjects: a preliminary report. Physiother Theory Pract 11:89–95 Support Care Cancer 20. 21. 22. 23. 24. 25. 26. 27. Användarhandbok Skanlab 25 Bodywave (2004) http://skanlab.no/ wp-content/uploads/2012/02/Skanlab_Usermanual_Norwegian. pdf. Accessed 23/3, 2015 ITO Physiotherapy & Rehabilitation. Elektrostimuleringsenhet ES520 & Vakuumenhet. Device manual. Print Giorgi F, Cellerino R, Gramazio A, Tummarello D, Menichetti ET, Giordani P, Antognoli S, Carle F, Piga A (1996) Assessing quality of life in patients with cancer: a comparison of a visual-analogue and a categorical model. Am J Clin Oncol 19:394–399 Jensen MP (2003) The validity and reliability of pain measures in adults with cancer. J Pain 4:2–21 Margolis RB, Chibnall JT, Tait RC (1988) Test-retest reliability of the pain drawing instrument. Pain 33:49–51 Ohlund C, Eek C, Palmblad S, Areskoug B, Nachemson A (1996) Quantified pain drawing in subacute low back pain. Validation in a nonselected outpatient industrial sample spine 21:1021–1030 discussion 1031 Jacobson GP, Newman CW (1990) The development of the dizziness handicap inventory. Arch Otolaryngol Head Neck Surg 116: 424–427 Jarlsäter S, Mattsson E (2003) Test of reliability of the dizziness handicap inventory and the activities-specific balance confidence scale for use in Sweden. Adv Physiother 5:137–144 28. Briggs RC, Gossman MR, Birch R, Drews JE, Shaddeau SA (1989) Balance performance among noninstitutionalized elderly women. Phys Ther 69:748–756 29. Steffen T, Seney M (2008) Test-retest reliability and minimal detectable change on balance and ambulation tests, the 36-item shortform health survey, and the unified Parkinson disease rating scale in people with parkinsonism. Phys Ther 88:733–746 30. Pachman DR, Qin R, Seisler DK, Smith EM, Beutler AS, Ta LE, et al. (2015) Clinical course of oxaliplatin-induced neuropathy: results from the randomized phase III trial N08CB (alliance). J Clin Oncol 33:3416–3422 31. Wall PD, Melzack R (1999) Textbook of pain. Churchill Livingstone, Edinburgh 32. Rostock M, Jaroslawski K, Guethlin C, Ludtke R, Schroder S, Bartsch HH (2013) Chemotherapy-induced peripheral neuropathy in cancer patients: a four-arm randomized trial on the effectiveness of electroacupuncture. Evid Based Complement Alternat Med 2013:349653 33. FACT/GOG-NTX (Version 4) [Measurement instrument]. http:// www.facit.org/LiteratureRetrieve.aspx?ID=42406. Accessed 5/11, 2015 34. Farrar JT, Young Jr JP, LaMoreaux L, Werth JL, Poole RM (2001) Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 94:149–158