Bon Jovi Roulette Letra En Español -- Info!
Anuncio

\
,,,,.,, ,"'- {'
Child and Adult Care Food Program, Child Enrollment Form, Agreement#4-07-39-428
Sponsoring Organization
Lehigh Valley Children's Centers
Center/Home:
Address
1501 Lehigh Street, Suite 208
Address
-.,- __
--'Allentown PA 18103
1-800-258-3737, or 610-820-5333
_
_
CHILD AND ADULT CARE FOOD PROGRAM
I INFANT ENROLLMENT FORM
This enrollment supplem9nt must be; completed for all infants in care at the time of enrollment to determine
responsibility for providing infant formula as part of the phild and Adult Care Food Program (CACFP). Please have
the parent sign and date tW0 forms. Send one to your sponsoring organization and keep the other as part of the
infant's enrollment file.'
I
I
Directions:
I
Infant Name:
I
I
Date of Birthi
Home/Center Site:
I
Home/Center will offer the following iron-fbrtified formula:
PARENT CHOICE: (Please check one)
I
The Center/Home will furnish infant's'formula,
-The Parent will furnish the iffant's forrulalbreast
Indicate Type of Formula or BreaSJMilk
I
_
milk.
'
I
IF THE ABOVE TYPE OF IRON FORMU A DOES NOT MEET CACFP REQUIREMENTS, PLEASE A IT ACH A COpy OF
THE PHYSICIAN'S ME ICAL STATEMENT RECOMMENDING THIS TYPE OF FORMULA
Are there any special circumstances or. conditions indicated by the infant's physician?
I
As the parent of the above-named
notice.
child, I untlerstand that I may change my decision regarding furnishing infant formula with proper
Parent's Signature
Date
Signature of Center Director/Home
Provider
Date
CHILD CARE REPRESENTATIVE USE ONLY:
Name of Representotive¥Signature
The effective date can be made retroactive
The U.S. Department
natianalorigin,
orientation,
program
Date
back to the first day the c~ild participates
oj Agriculture
prahibits
discrimf,·nation against its customers,
age, disability, sex, gender identity,
or al/ or part of an individual's
in the CACFPas long as
it
occurs in the same month this form is received.
employees,
and applicants for employment
on the bases of race, color,
ligian, reprisal, and where applicable, political beliefs, marital status, familial ar parental status, sexual
income is erived from any public assistance
pragram,
or protected
genetic information
in emptoyment
or
activity conducted
or funded
by the Department.
If yau wish ta file a Civil Rights program
complaint
(No al/ prohibited
of discrimination,
l]!Jl2JL!www.ascr.usdSHlQy!coITJRlaintfilingcust.htl.
containing
ar in any
\
al/ of the information
requested
in the for
bases will apply to 01/programs
complete
and/or employment
the USDA Program Discrimination
Camplaint Farm, faund anline at
or at any USDA office, or call (866) 632-9992 ta request the form.
. Send your completed
activities.)
Yau may alsa write a letter
complaint form ar letter ta us by mail at U.S. Department
of Agriculture,
Director, Office of
Adjudication,
Individuals
1400 Independence
Avenue,
S. W., Wasqington,
D.C. 20250-9410, by fax (202) 690-7442 or email ate!:[email protected]{.
who are deaf, hard of hearing or have spepch disabilities may contact USDA through the Federal Relay Service at (800)877-8339; or (800) 845-
6136 (Spanish).
USDA-is an equal opportunity
provider and employer.
·r ~~,-~
,.j
,-%
.;!i
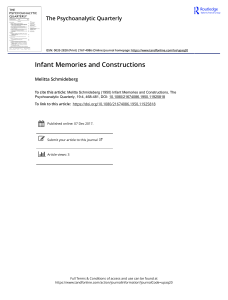
Child and Adult Care Food Program Child Enrollment Form
""j•.-J
:;.
~:
.,;',
Sponsoring Organization Lehigh Valley Children's Centers
Address
1501 Lehigh Street, Suite 208 AllentownPA 18103
-
Home Provider:
Telephone
r
Address:
I
I
I
Home
ENROLLMENT
Address
I
Parent/Guardian:
Agreement #300-39-428--0
1-800-258-3737,or610-820-5333
Work:
WITHDRAWAL
DATE-
DATE-
TIMES CHILD NORMALLY ATTENDS DURING WEEK
DAY OF WEEK IN
FULL NAME OF ENROLLED
(Include
TIME IN
ATTENDANCE
CHILD
Birth Date/Age)
Please Cheyk (v"")
,
TIME CHILDATIENDS SCHOOL
I
A
M
P
TIME
M
MONDAY
A
M
P
TIME
M
:
I
THURSDAY
I
FRIDAY
:
:
I
Optional:
Relationship
Will
to provider:
additional
- yes,
School
meals
specrrv-
please
0
D Asian
I
Day care
be provided
District
0
--
u::,naCK
Elementary~
Yes
SUPPER
:
EVENING
SNACK
--
D Native Hawaiian or Other Pacific Islander
DOwn
o No
o Foster
u::,upp
Middle
School
High School
_
-
,
I
ENROLLMENT
PM SNACK
:
DIWhite
o Nephew/Niece
Grandchild
-,Luncn
,
LUNCH
D Not Hispanic or Latino
not in session?
i
u sreakrast
-
me meal:
C
school
AM SNACK
:
:
0 I'\merican Indian or Alaska Native
child
when
:
:
:
i? Hispahic or Latino
Mark one ethnic and racial identities
Optional:
Mark one more racial identities:
DBlack or African American
BREAKFAST
:
I
SUNDAY
RETURNS
TO
CENTER
:
:
:
SATURDAY
GENDER D F D M
LEAVES
CENTER
:
TUESDAY
AGE
Please Check
:
WEDNESDAY
BIRTH DATE
MEALS RECEIVED (v"")
TIMES VARY Please (v') if necessary
DAYS VARY
NAME (First Child)
TIMEOUT
WITHDRAJvAL
DATE:
DATE:
TIMES CHILD NORMALLY ATTENDS DURING WEEK
DAY OF WEEK IN
TIME IN
FULL NAME OF ENROlLED
ATTENDANCE
CHILD
Please Check (v"")
(Include
TIME CHILDATIENDS SCHOOL
A
M
DAYS VARY
TUESDAY
:
WEDNESDA'
THURSDAY
Will
additional
If yes, please
School
meals
specify
District
0
the meal:
LEAVES
CENTER
RETURNS
TO
CENTER
:
:
:
AM SNACK
:
:
:
:
LUNCH
:
:
:
:
PM SNACK
FRIDAY
:
:
:
:
SUPPER
SATURDAY
:
:
:
:
EVENING
SUNDAY
:
:
:
o Hisp~nic or Latino
0 Asian
when
0
TIME
BREAKFAST
Day care
be provided
P
M
:
Mark one ethnic and racial identities
to provider:
A
M
child
[]
school
Breakfast
o Not Hispanic or Latino
o White o Native Hawaiian
C American Indian or Alaska Native
o Nephew/Niece
Grandchild
s not in session?
[]Lunch
0
DSnack
Elementary
Middle
Yes
DOwn
or Other Pacific Islander
o Foster
DNa
DSupper
School
High School
I
Signature:
Signature:
Date:
Date:
JI1
I
p
pprop
g
V)
Please Check
:
Optional:
Mark one more racial identities:
DBlack or African American
Relationship
TIME
:
GENDER 0 F D M
Optional:
p
M
MONDAY
BIRTH DATE
AGE
MEALS RECEIVED
TIMES VARY Please (v') if necessary
Birth Date/Age)
NAME (First Child)
TIMEOUT
/
SNACK