Maria de la Luz Casas-Perez on behalf of:
Julieta Noguez PhD, Agustín Buendía PhD, David Escárcega PhD, José Martín Molina PhD,
Rogelio Bustamante PhD, Edgar López PhD, María Elena Meneses PhD, Enedina Ortega, PhD, David Escobar PhD
candidate, Leonor Zapata MSc, Abel Barragán PhD, Leo Celi PhD, Eric Winkler, Kenneth Paik
WHO: 2 billion people over 60 years old will inhabit Earth by 2050.
CSIS: share of senior citizens in Latin America will triple by 2050, with Mexico having the most elderly.
2010 census: 7 million of elderly in Mexico, expected to double in the next 15 years.
The elderly population of Mexico:
- Most are women in urban areas.
- Mexico City (11%), Oaxaca (10%) and Veracruz (10%) hold the highest populations.
- 37% lack conditions for self-employment.
- 30% are illiterate.
- 40% are the main providers in their homes.
- 30% have no health insurance or are benefited by health services.
No long terms programs to cater the needs of the older population.
Social development and health sectors are unprepared for demographic change – gathering information
is a pressing necessity.
Define, measure, and evaluate frailty to intervene with early prevention.
Foment prevention, self training, and training of health professionals and health-care givers.
The project stages are:
1) Determine the effectiveness of mobile technology to detect frailty.
2) Design and develop and intervention to achieve successful ageing.
Non-specific state of increasing risk, which reflects multisystem psychological change.
Frailty indexes define deterioration in emotional, cognitive, and functional abilities.
Scores look for potential deficits in individuals, they are multifactorial and dynamic.
Basic index developed by Fried:
Measure signs, symptoms, and abnormalities associated to quality of life.
Two main phenotypes:
- Physical
- Cognitive, Functional, and Social Circumstances
Clinical Frailty Scale:
1--------------------------------------------------------------------------------------------------------------------------7
Very fit
Completely Frail
Variables = no standard operational definition.
Complementary data such as analyzing day-to-day activities improve the models or create new ones.
For this project the extra data came in the form of the clinician’s experience on the field.
Mexican standards differ from international frailty scales if poverty and poor conditions are involved.
Said scales essentials are adjusted to: the conditions of Mexican elders and the specificities of their
quality of life.
Demographical, social, familiar, and individual conditions are included.
Register data as fast as possible with low risk of human errors Send specialized help immediately.
Robust
Pre-frail
Frail
Pre-frail can be helped through:
Nutrition
Exercise
SANA: Electronic medical
records platform
Data
Analytics
Urgent
care?
NO
Regular
checkup
YES
NO
Extraction and sending
data
Patient
Biometric
from first
medical
contact
First phase
Sociodemographic
information
Geriatrician
session
Does he/she
require
follow?
YES
Patient
Biometric
tracking
Second phase
1. Specialized personnel measures using biometric devices. 2. Records information through mobile
devices. 3. Sends the information to the platform’s cloud or servers.
Sana
Platform
Server
(Platform sana)
IOs App
Mobile
devices
and Web
App
Biometric
devices
MS Azure
(Sana platform)
Android
App
Bluetooth or Wi-Fi
Communications
Biomet 1
Scales
sociodemographic
information
Web app
Biomet 2
digital
dynamometer
Tablet
Phablet
Smart Phone
Cell Phone
Biomet 3
Digital
Pulser
Biomet n
Current biometric devices are quick, accurate, and have a low risk of making mistakes.
They can help recognize physical and physiological traits and report them in real time for analysis.
A questionnaire to accompany these measurements will reinforce the results obtained.
Sociodemographic
information
Bio-metric
devices
Technology has brought the measurement of frailty above anything seen before.
The simplest of phones have a wide variety of tools.
More accurate and objective data is readily available.
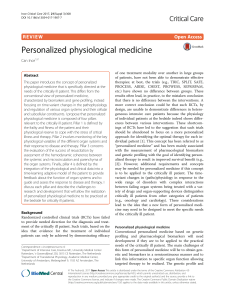
The study of frailty will involve the MIT’s SANA platform, mobile devices equipped with the proper tools,
wearable technology, geriatric information and records, and big data platforms.
All organized by the three tier architecture.
Novelty automatic biometric systems should:
- Improve the accuracy of patient data.
- Prevent human errors.
- Streamline the care of elderly patients.
- Optimize the time specialist geriatricians are available.
- Standardize the processes of care of the elderly.
Software under development to allow mobile devices to:
- Receive signals from biometric devices
- Capture demographic information
- Send information to sound platforms
- Apply data to estimate the urgency of patient care and possible complications
Researchers from Tecnologico de Monterrey and the Massachusetts Institute of Technology wish to
provide health services to senior citizens that are deprived of them.
Seeking to take advantage of technology as:
1. An instrument for health self-promotion.
2. An instrument for health professionals that are trained in prevention to help geriatricians with
their practice.
 0
0