- Ninguna Categoria
Informations Kit Test Bilirubine Directe | RAL
Anuncio
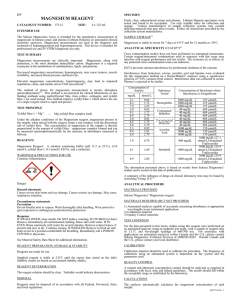
BILIRRUBINA DIRECTA Método colorimétrico Fabricante: RAL TECNICA PARA EL LABORATORIO, S.A. Av. Mare de Déu de Montserrat 51 08970 Sant Joan Despí (Barcelona) IVD PARA USO DIAGNÓSTICO IN VITRO CONSERVAR A 2 - 8º C LEER LAS INSTRUCCIONES ANTES DEL USO REF Referencias: GN 95125: GN 95126: MUESTRA: Suero o plasma heparinizado. Es importante preservar la muestra de la luz. Estabilidad: 6 meses a –20ºC, 7 días a 4-8ºC y 2 días a 20-25ºC. En caso de congelar la muestra, debe realizarse de inmediato. Deben descartarse muestras contaminadas. PROCEDIMIENTO: Existen aplicaciones para los principales sistemas automáticos. Longitud de onda: 546 nm Paso óptico: 1 cm Temperatura: T ambiente (20-25ºC) / 37ºC Reacción: punto final contra blanco de muestra Medida: contra blanco de reactivo Pipetear en cubetas: Cont. Presentaciones: 5 x 20 mL reactivo 1 + 25 mL reactivo 2 5 x 80 mL reactivo 1 + 100 mL reactivo 2 PRINCIPIO DEL METODO: Determinación fotométrica de la concentración de Bilirrubina Directa en suero o plasma por reacción con dicloroanilina diazotada (DCA), que forma un compuesto coloreado en medio ácido. SIGNIFICACIÓN CLINICA: La Bilirrubina es un producto de la descomposición de la hemoglobina. Libre, la Bilirrubina no conjugada es extremadamente apolar y casi insoluble en agua, de modo que forma un complejo con la albúmina para el transporte en la sangre desde el bazo hasta el hígado. En el hígado, la Bilirrubina se conjuga con ácido glucoronico y el resultado es un compuesto hidrosoluble que se excreta a través de los conductos biliares. La Hiperbilirrubinemia puede ser causada por un incremento de la producción de la bilirrubina debido a hemólisis (ictericia pre-hepática), por daños en el parénquima del hígado (ictericia intra-hepática), o por oclusión de los conductos biliares (ictericia post-hepática). La Hiperbilirrubinemia crónica y congénita (predominantemente no conjugada) se conoce como síndrome de Gilbert y es poco frecuente en la población. Se observan altos niveles de Bilirrubina Total en el 60-70% de neonatos debido a un incremento en la hemólisis de eritrocitos tras el parto y por un retraso en la función de los enzimas que degradan la bilirrubina. Los métodos comunes para determinar Bilirrubina detectan la Bilirrubina total o la Bilirrubina directa. Las determinaciones de Bilirrubina directa miden principalmente la Bilirrubina soluble en agua, conjugada. La Bilirrubina no conjugada puede ser estimada como la diferencia entre la Bilirrubina total y la Bilirrubina directa. Blanco Muestra/Calibrador Muestra/Calibrador 100 µL Agua destilada 100 µL Reactivo 1 1000 µL 1000 µL Mezclar, incubar 3 minutos, leer la absorbancia A1 y añadir: Reactivo 2 250 µL 250 µL Mezclar, incubar exactamente durante 5 minutos y leer la absorbancia A2. ∆A = [A2-A1] muestra/cal – [A2-A1] blanco CALCULO: Con calibrador: Conc. Bilirr = ∆A muestra / ∆A calibrador x Conc. Calibrador. CALIBRADORES Y CONTROLES: Se recomienda el uso del multicalibrador Biocal (GN 90999) para calibrar la técnica. Se recomienda el uso de los controles Gernorm (GN 90998) y Gerpath (GN 90997) para controlar a dos niveles la técnica. CARACTERÍSTICAS DEL METODO: Rango de medida: Pueden determinarse concentraciones de bilirrubina entre 0.1 y 10 mg/dL. Si los valores exceden el límite máximo, debe diluirse la muestra en solución salina (1+1) y multiplicar el resultado obtenido por 2. Especificidad / Interferencias: REACTIVOS: Se encuentran listos para el uso. No se han observado interferencias por ácido ascórbico hasta 30 mg/dL, lipemia hasta 1000 mg/dL triglicéridos. Se presentan interferencias por hemoglobina a concentraciones superiores a 50 mg/dL. Reactivo 1: EDTA-Na2 NaCl: Acido Sulfámico: 0.1 mmol/L 150 mmol/L 100 mmol/L Reactivo 2: Sal 2,4-Diclorofenil-diazonio HCl EDTA-Na2 0.5 mmol/L 900 mmol/L 0.13 mmol/L Sensibilidad / Límite de detección: El límite inferior de detección es 0.1 mg/dL. Precisión intra ensayo (n=20, a 37ºC): Muestra 1 (mg/dL): media: 0.36, SD: 0.01, CV: 3.34% Muestra 2 (mg/dL): media: 0.76, SD: 0.01, CV: 1.46% Muestra 3 (mg/dL): media: 2.07, SD: 0.03, CV: 1.30% CONSERVACIÓN: Los reactivos son estables hasta fecha de caducidad si se mantienen a 2-8ºC, protegidos de contaminaciones. No debe congelarse. El reactivo 2 se debe proteger de la luz. Precisión inter ensayo (n=20, a 37ºC): PRECAUCIONES EN EL MANEJO: Reactivos 1 y 2 (S24/25): Evitar el contacto de reactivos con ojos y piel. Deben tomarse las precauciones necesarias en el uso de reactivos de laboratorio clínico. Deben seguirse las disposiciones locales para la gestión de residuos. Comparación con otros métodos: Muestra 1 (mg/dL): media: 0.35, SD: 0.01, CV: 3.34% Muestra 2 (mg/dL): media: 0.75, SD: 0.01, CV: 1.00% Muestra 3 (mg/dL): media: 2.13, SD: 0.02, CV: 0.71% Se han analizado 85 muestras utilizando el reactivo de Gernon (y) y otro de un fabricante de la competencia (x). Correlación: r= 0.995. Relación: y = 0.95x + 0.04 mg/dL RANGO DE VALORES Adultos y niños ≤ 0.2 mg/dL (≤ 3.4 µmol/L) Cada laboratorio debe establecer su propio rango de referencia. BIBLIOGRAFÍA: Thomas L. Clinical Laboratory Diagnostics. Verlagsgesellschaft; 1998. p. 192-202 1sted. Frankfurt: TH-Books IU/GN/95125/R0/0309 Tel: (+34) 93 480 80 47 Fax: (+34) 93 373 00 92 e-mail: [email protected] web: www.ral-sa.com BILIRUBIN DIRECT Colorimetric Method Manufacturer: RAL TECNICA PARA EL LABORATORIO, S.A. Av. Mare de Déu de Montserrat 51 08970 Sant Joan Despí (Barcelona) - Spain IVD FOR IN VITRO DIAGNOSTIC USE PROCEDURE: Application sheets for automated systems are available on request. Wavelength: 546 nm Optical path: 1 cm Temperature: R.T. (20-25ºC) / 37ºC Reaction: end point against sample blank Measurement: against reagent blank STORE AT 2 - 8º C READ INSTRUCTIONS REF Reference: GN 95125: GN 95126: SPECIMEN: Serum or heparin plasma. It is important to store the sample protected from light. Stability: 6 months at -20ºC, 7 days at 4-8ºC and 2 days at 20-25ºC. In case of sample freezing, do it immediately. Freeze only once. Discard contaminated specimens. Cont. Pipette into cuvettes: Package: 5 x 20 mL reagent 1 + 25 mL reagent 2 5 x 80 mL reagent 1 + 100 mL reagent 2 PRINCIPLE: Direct bilirubin in presence of diazotized 2,4-dichloroaniline forms a red colored azocompound in acidic solution. SUMMARY: Bilirubin is a breakdown product of haemoglobin. Free, unconjugated bilirubin is extremely apolar and nearly insoluble in water, thus forming a complex with albumin for the transport in the blood from the spleen to the liver. In the liver, bilirubin is conjugated with glucoronic acid and the resulting water is excreted via the bile ducts. Hyperbilirubinemia can be caused by increased bilirubin production due to hemolysis (pre-hepatic jaundice), by parenchymal damages of the liver (intrahepatic jaundice) or by occlusion of bile ducts (post-hepatic jaundice). A chronic congenital (predominantly unconjugated) hyperbilirubinemia called Gilbert’s syndrome is quite frequent in the population. High levels of total bilirubin are observed in 60-70% of neonates due to an increased postpartal breakdown of erythrocytes and because of delayed function of enzymes for bilirubin degradation. Common bilirubin methods detect either total bilirubin or direct bilirubin. Determinations of direct bilirubin measure mainly conjugated, water soluble bilirubin. Unconjugated bilirubin can therefore be estimated as the difference between total bilirubin and direct bilirubin. Blank Sample/Calibrator Sample/Calibrator 100 µL Distilled water 100 µL Reagent 1 1000 µL 1000 µL Mix, incubate for 3 minutes, read the absorbance A1 and add: Reagent 2 250 µL 250 µL Mix, incubate for exactly 5 minutes and read the absorbance A2. ∆A = [A2-A1] sample/calibrator – [A2-A1] blank CALCULATION: With calibrator: Bilir Conc = ∆A sample / ∆A calibrator x Conc. Calibrator. CALIBRATORS AND CONTROLS: It is recommended to use the multicalibrator Biocal (GN 90999) to calibrate the method. It is recommended the use of the controls Gernorm (GN 90998) and Gerpath (GN 90997) to control at two levels the method. PERFORMANCE CHARACTERISTICS: Measuring range: REAGENTS: Reagents are ready to use. The test has been developed to determine bilirubin concentrations within a measuring range from 0.1 – 10 mg/dL. When exceed this range, samples should be diluted 1+1 with NaCl solution (9 g/L) and the result multiplied by 2. Reagent 1: EDTA-Na2 NaCl: Sulfamic acid: 0.1 mmol/L 150 mmol/L 100 mmol/L Reagent 2: 2,4-Dichlorophenil-diazonium salt HCl EDTA-Na2 0.5 mmol/L 900 mmol/L 0.13 mmol/L STORAGE: The reagents are stable up to the end of the indicated month of expiry, if stored at 2-8ºC and contamination is avoided. Do not freeze the reagents. Reagent 2 must be protected from light. WARNING AND PRECAUTIONS: Reagents 1 and 2 (S24/25): Avoid contact with skin and eyes. Refer to the safety data sheets and take the necessary precautions for the use of laboratory reagents. Refer to local legal requirements for waste management. Specificity / Interferences: No interference was observed by ascorbic acid up to 30 mg/dL and lipemia up to 1.000 mg/dL triglycerides. Interference by haemoglobin occurs starting at haemoglobin concentrations of 50 mg/dL. Sensitivity / Limit of detection: The lower limit of detection is 0.1 mg/dL. Precision intra-assay (n=20, at 37ºC): Sample 1 (mg/dL): mean: 0.36, SD: 0.01, CV: 3.34% Sample 2 (mg/dL): mean: 0.76, SD: 0.01, CV: 1.46% Sample 3 (mg/dL): mean: 2.07, SD: 0.03, CV: 1.30% Precision inter-assay (n=20, at 37ºC): Sample 1 (mg/dL): mean: 0.35, SD: 0.01, CV: 3.34% Sample 2 (mg/dL): mean: 0.75, SD: 0.01, CV: 1.00% Sample 3 (mg/dL): mean: 2.13, SD: 0.02, CV: 0.71% Method comparison: A comparison of Bilirubin Direct of Gernon (y) with a commercially available test (x) using 85 samples gave following results: Y = 0.95x + 0.04 mg/dL r = 0.995 REFERENCE RANGE Adults and children ≤ 0.2 mg/dL (≤ 3.4 µmol/L) Each laboratory should establish its own reference range. LITERATURE: Thomas L. Clinical Laboratory Diagnostics. Verlagsgesellschaft; 1998. p. 192-202 1sted. Frankfurt: TH-Books IU/GN/95125/R0/0309/EA Tel: (+34) 93 480 80 47 Fax: (+34) 93 373 00 92 e-mail: [email protected] web: www.ral-sa.com BILIRUBINE DIRECTE Méthode Colorimétrique Fabricant: RAL TECNICA PARA EL LABORATORIO, S.A. Av. Mare de Déu de Montserrat 51 08970 Sant Joan Despí (Barcelone) - Espagne IVD POUR LE DIAGNOSTIC IN VITRO MODE OPÉRATOIRE: Des notices d’application adaptées aux systèmes automatisés sont disponibles sur demande. Longueur d’onde: 546 nm Trajet optique: 1 cm Température: T ambiante (20-25ºC) / 37ºC Réaction: Point final contre le blanc échantillon Mesure: Contre le blanc réactif CONSERVER À 2 - 8º C LIRE LES NOTICES REF SPÉCIMEN: Sérum, plasma recueilli sur héparine. Il est très important de conserver le spécimen à l’abri de la lumière. Stabilité: 6 mois à -20ºC, 7 jours à 4-8ºC et 2 jours à 20-25ºC. S’il faut congeler le spécimen, il faut le faire immédiatement. Congélation unique. Eliminer les échantillons contaminés. Cont. Pipetter dans des cuvettes: Référence: GN 95125: GN 95126: Emballage: 5 x 20 mL réactif 1 + 25 mL réactif 2 5 x 80 mL réactif 1 + 100 mL réactif 2 PRINCIPE: La bilirubine directe forme avec la 2,4-dichloroaniline diazotée, en milieu acide, un azocomposé coloré en rouge. INTÉRÊT CLINIQUE: La bilirubine est un produit de dégradation de l’hémoglobine. La bilirubine libre, non conjuguée, est fortement non polaire et pratiquement insoluble dans l’eau; c’est pourquoi elle forme un complexe avec l’albumine pour passer dans le sang de la rate vers le foie. Dans le foie, la bilirubine se conjugue avec l’acide glucuronique et le conjugué résultant, soluble dans l’eau, est excrété par les voies biliaires. L’hyperbilirubinémie peut avoir pour origine une production accrue de bilirubine à la suite d’une hémolyse (ictère pré-hépatique), des lésions du parenchyme hépatique (ictère hépatique) ou une occlusion des voles biliaires (ictère post-hépatique). Le syndrome de Gilbert est une hyperbilirubinémie essentiellement non conjuguée) congénitale chronique, d’apparition fréquente dans la population. Des valeurs élevées de bilirubine peuvent être observées chez 60 à 70 % des nouveau-nés en raison d’une lyse post-natale accrue des érythrocytes et d’un retard de fonctionnement des enzymes de dégradation de la bilirubine. Les méthodes d’analyse pour la détermination de la bilirubine mesurent, soit la bilirubine totale, soit la bilirubine directe; dans le cas de la bilirubine directe, c’est essentiellement la bilirubine conjuguée, soluble dans l’eau, qui est mesuré. Le taux de bilirubine non conjuguée peut alors être estimé par différence entre la bilirubine totale et la bilirubine directe. Blanc Échantillon/Calibrant Échantillon/Calibrant 100 µL Eau distillée 100 µL Réactif 1 1000 µL 1000 µL Mélanger, incuber pendant 3 minutes, lire l’absorbance A1 et ajouter: Réactif 2 250 µL 250 µL Mélanger, incuber pendant exactement 5 minutes et lire l’absorbance A2. ∆A = [A2-A1] échantillon/calibrant – [A2-A1] blanc CALCULATION: Avec le calibrant: Bilir Conc = ∆A échantillon / ∆A calibrant x Conc. Calibrant CALIBRANTS ET CONTRÔLES: C’est recommandé d’utiliser le multicalibrant Biocal (GN 90999) pour calibrer la méthode. C’est recommandé d’utiliser les contrôles Gernorm (GN 90998) et le Gerpath (GN 90997) pour contrôler à deux niveaux. PERFORMANCES: Domaine de mesure: Le test a été développé pour la détermination des concentrations de bilirubine dans un domaine de mesure compris entre 1 et 100 mg/L. Au-delà de cet intervalle, diluer l’échantillon 1+1 avec de la solution NaCl (9 g/L) et multiplier le résultat par 2. RÉACTIFS: Réactifs prêts à l’emploi. Réactif 1: EDTA-Na2 NaCl: Acide sulfanilique: 0.1 mmol/L 150 mmol/L 100 mmol/L Réactif 2: 2,4-sel de dichlorophényl-diazonium HCl EDTA-Na2 0.5 mmol/L 900 mmol/L 0.13 mmol/L Spécificité / Interférences: Aucune perturbation n’a été observée par la présence d’acide ascorbique jusqu’à 30 mg/dL and lipémie jusqu’à 1.000 mg/dL de triglicérides. L’hémoglobine interfère à partir de 50 mg/dL. Sensibilité / Limite de détection: La limite de détection analytique est de 0.1 mg/dL. CONSERVATION: Les réactifs sont stables jusqu’à la fin du mois de la date de péremption indiquée, conservés entre 2-8ºC en évitant toute contamination. Ne pas congeler les réactifs. Le réactif 2 doit être protégé de la lumière. Précision intra-série (n=20, à 37ºC): AVERTISSEMENTS ET PRÉCAUTIONS D’EMPLOI: Réactifs 1 et 2 (S24/25): Éviter le contact avec la peau et les yeux. Vous référer aux fiches de sécurité et prendre les précautions nécessaires pour l’utilisation de réactifs de laboratoire. Se référer aux exigences légales nationales pour l’élimination des déchets. Échantillon 1 (mg/dL): moyenne: 0.35, SD: 0.01, CV: 3.34% Échantillon 2 (mg/dL): moyenne: 0.75, SD: 0.01, CV: 1.00% Échantillon 3 (mg/dL): moyenne: 2.13, SD: 0.02, CV: 0.71% Échantillon 1 (mg/dL): moyenne: 0.36, SD: 0.01, CV: 3.34% Échantillon 2 (mg/dL): moyenne: 0.76, SD: 0.01, CV: 1.46% Échantillon 3 (mg/dL): moyenne: 2.07, SD: 0.03, CV: 1.30% Précision inter-série (n=20, à 37ºC): Comparaison de méthodes: Une comparaison entre la Bilirubin Direct de Gernon (y) et une méthode disponible sur le marché (x), réalisée sur 85 échantillons, a donné les résultats suivants: Y = 0.95x + 0.04 mg/dL r = 0.995 VALEURS USUELLES Adultes et enfants ≤ 0.2 mg/dL (≤ 3.4 µmol/L) Chaque laboratoire doit établir son propre range de travail RÉFÉRENCES BIBLIOGRAPHIQUES: Thomas L. Clinical Laboratory Diagnostics. Verlagsgesellschaft; 1998. p. 192-202 1sted. Frankfurt: TH-Books IU/GN/95125/R0/0309/EF Tel: (+34) 93 480 80 47 Fax: (+34) 93 373 00 92 e-mail: [email protected] web: www.ral-sa.com
 0
0
Anuncio
Documentos relacionados

Descargar
Anuncio
Añadir este documento a la recogida (s)
Puede agregar este documento a su colección de estudio (s)
Iniciar sesión Disponible sólo para usuarios autorizadosAñadir a este documento guardado
Puede agregar este documento a su lista guardada
Iniciar sesión Disponible sólo para usuarios autorizados