Orange County School of the Arts FREE/REDUCED
Anuncio

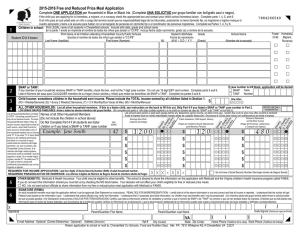
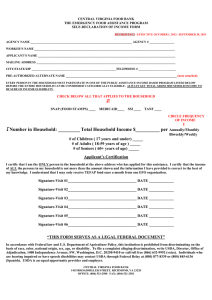
Orange County School of the Arts FREE/REDUCED-PRICE LUNCH PROGRAM / INCOME ELIGIBILITY GUIDELINES July 1, 2016 – June 30, 2017 Household Size Year Month Twice Per Month Every Two Weeks Week 1 $21,978 $1,832 $916 $846 $423 2 29,637 2,470 1,235 1,140 570 3 37,296 3,108 1,554 1,435 718 4 44,955 3,747 1,874 1,730 865 5 52,614 4,385 2,193 2,024 1,012 6 60,273 5,023 2,512 2,319 1,160 7 67,951 5,663 2,832 2,614 1,307 8 75,647 6,304 3,152 2,910 1,455 642 321 296 148 For each additional family member, add: + 7,696 FAQs for OCSA’s Free/Reduced Lunch Program (FRLP) How do I apply? If you qualify, based on your annual income and household size as listed above, please print and complete an OCSA FRLP application. To download an application, visit www.ocsarts.net/ApplyFRLP. Please complete ONLY ONE APPLICATION PER HOUSEHOLD. We cannot approve incomplete applications. Please be sure to carefully complete all required information and sign the form to avoid delays in approval. Please return the completed application to: OCSA Business Office Becky. Parsons 1010 N. Main St. Santa Ana, CA 92701 Return the completed application to the address above or by fax to 714-664-0463, or by email to [email protected] . If your household currently receives FDPIR benefits, CalFresh, or CalWORKs your child may automatically qualify for benefits; however, you MUST still return the form indicating that you are participating in these programs. Who can get free or reduced price lunch? Children in households getting CalFresh, CalWORKS, or FDPIR and most foster children (under the legal responsibility of a welfare agency or court) can get free lunch regardless of income. Also, if your household income is within the limits on the Income Eligibility Guidelines, your children can receive free or reduced priced lunch. Homeless, runaway, and migrant children may qualify for lunch benefits, check with the school liaison for these circumstances. Children in households participating in WIC may be eligible for lunch benefits. Children do not have to be a U.S. citizen to qualify for lunch benefits. Are there any other items that may be free/discounted because my family is eligible for this program? Yes, all OCSA students in a qualified family can receive free/discounted pricing on several school related items. For more information see the FRLP Fee Schedule listed at www.ocsarts.net/FRLP. Can my child choose any food item from the menu? No. All students that qualify for FRLP will receive a free “Daily Special” meal from our cafeteria which includes an entrée, whole fruit and milk or water. All a la cart menu items including breakfast items will be at their own cost. Visit www.ocsarts.net/FRLPmenu for more information. Will the information I submit on my application be checked? Yes. You may be asked to submit proof of the information you provide at any time during the school year. You must include income of all people living in your household, related or not (such as grandparents, cousins or friends). If you are a single parent residing at your parent’s home, you must include their income on the application. Who will know if my child is on this program? All applications and records concerning FRLP shall be confidential, and shall not be open to examination for any purpose not directly connected with the administration of this program. Those accessing FRLP information could include Administrators of OCSA programs, such as the OCSA Food Service program, After-School Student Program, School Registration, Locker Rentals, Parking Permits, AP Testing, Collage Transcripts, and Student Services, for which your family may qualify for free/reduced pricing. If I don’t qualify now, may I apply again later? Yes. You may apply at any time during the school year if your household size goes up or income goes down. What if I disagree with the decision about my FRLP application? You may ask for an explanation by calling or writing Becky Parsons at [email protected] or 714-560-0900, ext. 5535. California Department of Education, May 2016 School Year 2016-2017 Orange County School of the Arts Application for Free and Reduced-Price Meals Complete one application per household. Read the instructions included with Application on how to apply. Please print and use a pen. This institution is an equal opportunity provider. California Education Code Section 49557(a): “Applications for free and reduced-price meals may be submitted at any time during a school day. Children participating in the federal National School Lunch Program will not be overtly identified by the use of special tokens, special tickets, special serving lines, separate entrances, separate dining areas, or by any other means.” STEP 1 – STUDENT INFORMATION Children in Foster Care and children who meet the definition of Homeless, Migrant, or Runaway are eligible for free meals. Attach another sheet of paper for additional names. Enter the name of EACH STUDENT who will attend school Check the applicable box if the student is Enter school name and grade level Enter student’s birth date (First, Middle Initial, Last) foster, homeless, migrant, or runaway. Foster Child Homeless Migrant Runaway EXAMPLE: Joseph P Adams Lincoln Elementary 1st 12-15-2010 STEP 2 – ASSISTANCE PROGRAMS: CalFresh, CalWORKs, or FDPIR Do ANY household members (including yourself) currently participate in one of the following assistance programs? If NO, skip STEP 2 and complete STEP 3. Select Program Type: If YES, do not complete STEP 3. Check the applicable program box, enter one case number, and then go to STEP 4. CalFresh CalWORKs FDPIR Enter Case Number: A. STUDENT INCOME: Sometimes students in the household earn income. Please include the TOTAL income earned by Total Student Income How Often all students listed in STEP 1 here. Report total income in whole dollars earned before taxes and deductions. $ Enter the appropriate pay period: W = Weekly, 2W = Bi-Weekly, 2M = Twice a Month, M = Monthly, Y = Yearly B. ALL OTHER HOUSEHOLD MEMBERS (including yourself): List ALL household members not listed in STEP 1 even if they do not receive income. For each household member, report the TOTAL income for each source in whole dollars only. If they do not receive income from any source, write “0”. If you enter “0” or leave any fields blank, you are certifying (promising) that there is no income to report. Report all income earned before taxes and deductions. Enter the appropriate pay period in the “How Often” column: W = Weekly, 2W = Bi-Weekly, 2M = Twice a Month, M = Monthly, Y = Yearly Enter the name of ALL OTHER Household Members How Public Assistance/SSI/ How Pensions/Retirement/ How Earnings from Work (First and Last) Often Child Support/Alimony Often All Other Income Often $ $ $ $ $ $ $ $ $ $ $ $ Enter the last four digits of Social Security number (SSN) from the Primary Wage Earner or Other Adult Household Member DO NOT COMPLETE. SCHOOL USE ONLY Annual Income Conversion: Weekly x52, Bi-Weekly x26, Twice a Month x24, Monthly x12 How Often? Weekly Bi-Weekly Twice a Month Monthly Yearly Total Household Income Total Household Size Categorical Eligibility Status: Free Verified as: Homeless Determining Official’s Signature: Reduced-price Migrant Paid (Denied) Runaway Error Prone Date: Confirming Official’s Signature: Date: Verifying Official’s Signature: Date: STEP 4 – CONTACT INFORMATION & ADULT SIGNATURE STEP 3 – REPORT INCOME FOR ALL HOUSEHOLD MEMBERS (Skip this step if you answered ‘Yes’ to STEP 2) Total Household Members (Children and Adults) Certification: “I certify (promise) that all information on this application is true and that all income is reported. I understand that this information is given in connection with the receipt of federal funds, and that school officials may verify (check) the information. I am aware that if I purposely give false information, my children may lose meal benefits, and I may be prosecuted under applicable state and federal laws.” Signature of adult completing this form: Print Name: Today’s Date: Phone Number: Address: City: State: Zip: E-mail: Check the box if NO SSN OPTIONAL – CHILDREN’S ETHNIC AND RACIAL IDENTITIES We are required to ask for information about your children’s race and ethnicity. This information is important and helps to make sure we are fully serving our community. Responding to this section is optional and does not affect your children’s eligibility for free or reduced-price meals. Ethnicity (check one): Hispanic or Latino Not Hispanic or Latino Race (check one or more): American Indian or Alaskan Native Native Hawaiian or other Pacific Islander Asian Black or African American White 2016-2017 Orange County School of the Arts licitud de comidas gratis o a precio reducido Llene una solicitud por hogar. California Department of Education, June 2016 Artículo 49557(a) del Código de Educación de California: “Las solicitudes de comidas gratis o a precio reducido se pueden presentar en cualquier momento durante un día de clase. A los menores que participen en el Programa Nacional de Almuerzos Escolares (federal National School Lunch Program) no se les identificará abiertamente con el uso de fichas, boletos o filas para servir especiales; entradas o comedores separados; ni por ningún otro medio”. Anote TODOS los miembros del hogar que son bebés, niños o estudiantes hasta el grado 12 (si necesita más espacio para más nombres, adjunte otra hoja de papel) ¿Estudiante? Sí No Inicial Apellido del menor Primer nombre del menor Los menores bajo cuidado adoptivo temporal, y los que cumplen con la definición de sin hogar, inmigrante o se fugó del hogar reúnen los requisitos para recibir comidas gratis. Para obtener más información, lea Cómo solicitar comidas escolares gratis o a precio reducido. PASO 2 ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ Bajo cuidado adoptivo temporal Sin hogar, inmigrante, se fugó del hogar ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ Marque todos los pertinentes PASO 1 Definición de miembro del hogar: “Cualquier persona que viva con usted y comparta los ingresos y gastos, incluso si no es su pariente”. ¿Algún miembro del hogar (incluyéndolo a usted) participa actualmente en uno o más de los siguientes programas de asistencia? Si respondió que SÍ > Marque la casilla del programa pertinente, anote el número de caso y vaya al PASO 4 (No llene el PASO 3) ☐ CalFresh ☐ CalWORKs ☐ FDPIR Número de caso: Si respondió que NO > Llene el PASO 3 PASO 3 Anote sólo un número de caso en este espacio. Declare los ingresos de TODOS los miembros del hogar (sáltese este paso si respondió que ‘Sí’ en el PASO 2) A. Ingresos de los menores ¿Frecuencia? Semanal mente Cada 2 semanas 2 veces al mes Mensualmente $ del hogar anotados en el PASO 1. B. Todos los miembros adultos del hogar (incluyéndolo a usted) Anote todos los miembros del hogar que no anotó en el PASO 1 (incluyéndose a usted mismo) incluso si no reciben ingresos. Para cada miembro que reciba ingresos, declare los ingresos totales de cada fuente en números redondos. Si no reciben ingresos de ninguna fuente, anote ‘0’. Si anota ‘0’ o deja los campos en blanco, está certificando (prometiendo) que no hay ingresos que declarar. Asistencia pública/ manutención de menores/ ¿Frecuencia? Nombre de los miembros adultos del hogar (nombre y Ingresos de trabajo Semanalmente Cada 2 semanas ¿Frecuencia? Semanalmente Cada 2 semanas 2 veces al mes Mensualmente ¿Frecuencia 2 veces por mes Mensualmente pensión alimenticia $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ Total de miembros del hogar (Del PASO 1 y PASO 3) PASO 4 Ingresos totales de los menores En ocasiones, los menores del hogar tienen ingresos. Incluya aquí los ingresos TOTALES que reciben todos los miembros Para obtener más información lea Cómo solicitar comidas escolares gratis o a precio reducido. La sección Fuentes de ingresos de los menores le ayudará a contestar la pregunta Ingresos de los menores. La sección Fuentes de ingresos de los adultos le ayudará con la sección Todos los miembros adultos del hogar. Últimos cuatro dígitos del número de seguro social (SSN) del principal proveedor o de otro miembro adulto del hogar X X X X X Pensiones/jubilación/ todos los demás ingresos Semanalmente Cada 2 semanas 2 veces por mes Mensualmente ☐ Marque la casilla si no tiene SSN Información de contacto y firma del adulto Certificación: “Certifico (prometo) que toda la información en esta solicitud es verdadera y que he declarado todos los ingresos. Entiendo que esta información se proporciona en relación con la recepción de fondos federales y que los funcionarios escolares podrían verificar (revisar) la información. Entiendo que si doy intencionalmente información falsa, mis hijos podrían perder los beneficios alimentarios y yo podría ser enjuiciado bajo las leyes estatales y federales pertinentes”. Dirección OPCIONAL No. de departamento Ciudad Teléfono o correo electrónico Estado Código postal Identidad étnica y racial de los menores Nombre en letra de molde del adulto que llenó este formulario Firma del adulto que llenó este formulario Fecha de hoy Esta institución es un proveedor que ofrece igualdad de oportunidades. Estamos obligados a pedir esta información sobre la raza e identidad étnica de sus hijos. Esta información es importante y nos ayuda a asegurarnos de que estamos sirviendo plenamente a nuestra comunidad. Responder esta sección es opcional y no afecta el cumplimiento de los requisitos de sus hijos para recibir comidas gratis o a precio reducido. Identidad étnica (marque una): ☐Hispano o latino ☐No hispano o latino Raza (marque una o más): ☐ Asiático ☐ Indígena americano o nativo de Alaska ☐Negro o afroestadounidense ☐ Nativo de Hawái u otra isla del Pacífico ☐ Blanco NO LLENE LA SIGUIENTE INFORMACIÓN. ES PARA USO DE LA ESCUELA SOLAMENTE. How often? Total Household Income Weekly Bi-Weekly 2x Month Monthly Yearly Total Household Members Annual Income Conversion Weekly x52 | Bi-Weekly x26 | Twice Per Month x24 | Monthly x12 Determining Official Date Confirming Official Approved as: Verified as: ☐ Free ☐ Reduced-Price ☐ Paid (Denied) Reason: ____________________________ Date ☐ Homeless ☐ Migrant ☐ Runaway Verifying Official ☐ Categorical ☐ Error Prone Date