AB ABCD BCD EA D EARL ARLY LE LY LEAR EARNING RNING G
Anuncio

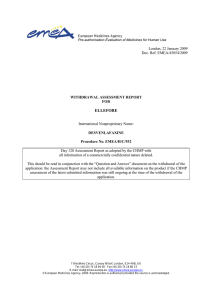
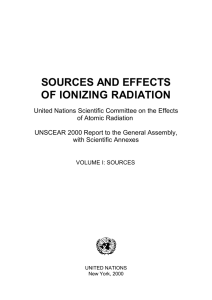
ABCD D EARL LY LEAR RNING AB BCD EA ARLY LE EARNING G APPLIICATION PACK KET Thhank you fo or your inteerest in ou ur Early Learning Proogram. Attaached is ouur applicatiion with thee necessary y forms needed to staart your chiild’s enrolllment. Pleaase take a few minuttes to fill ouut the inform mation below so we can c help you with thee enrollmeent processs. Today’s Date: D Name of child nt: Applican Child’s date of o Birth Parrent/Guardiaan Name Address Phone # OF FFICE USE ONLY Casseworker folllow-up: 1st contact: date:_ ____________ ___ (wiithin 2wks from m app pick-up)) (REMIND PARENT TO T COMPLE ETE DENTA AL/MAKE A APPOINTM MENT) __ ___________ __________ ___________ ___________ _______________________________________ __ ___________ __________ ___________ ___________ ________________________________________ No longer interestted application incomp plete /waiting oon documentattion Application su ubmitted C Continue follow w-up Apppt made 2nd contact: date: ____________ _ ___ (if aapplicable, with hin 2 wks of 1st contact) __________ ___________ __________ ______________________ ______________________ ________ ___ ___ __________ ___________ __________ ______________________ ______________________ ________ No long ger interested applicatiion incompletee /waiting on doocumentation pplication subm mitted Continue ffollow-up Ap Appt maade ABCD D EARL LY LEAR RNING Deear Parent or Guardian,, ABCD Inc. Thank you so mucch your inteerest in the programs ooffered at A I hhave encloseed the requiired applicaation packett for you to complete. I have also included a flyer that proovides you with w inform mation abou ut our Early Learning pprograms annd their locations. Pleaase bring thee following items when n you return n the appliccation: Birth verifiication (Birrth certificatte, Passportt, Hospital C Certificate, etc..) Social Secu urity Numb bers for the family Child’s Me edical Insurrance Card Guardiansh hip documeents (If appllicable) Parent or Guardian’s G proof p of inccome Most recen nt monthly pay p stubs State Budg get form (for one month h of incomee) Child’s Phy ysical, Imm munization and a Dental form (or prroof of denttal appointm ment) Two emerg gency namees and telep phone numb ber pleted packeet to our Earrly Learninng Departmeent at ABC CD Inc. 10700 Park Yoou can returrn the comp Avve or to the site of yourr choice. Fo or more info ormation caall ABCD aat 366-8241 Ext 221 Thhank you dre / encargaado: Esttimado Pad Muchaas gracias po or su interés en los pro ogramas ofrrecidos por ABCD Inc. Adjunto enccontraran lo os formularrios requerid dos para qu ue usted pueeda complettar su aplicaación. Se inncluye adeemás folleto os que conttienen inforrmación aceerca de los pprogramas dde cuidado de niños y las loccalizacioness de los missmos. Los siguientes do ocumentos son requeriidos para pooder processar la apllicación de su niño(a): Verificació ón de nacim miento (Certtificado de nacimiento, n , pasaporte,, certificadoo de hospitaal, etc…) Los número de Seguro o Social de la familia Tarjeta del seguro médico del niñ ño Prueba de Ingreso I Eco onómico (P Padre o Encaargado) Deben ser talonarios t de d pagos reccientes o caarta oficial ddel estado Prueba de custodia c Examen fís sico compleeto (debe in ncluir las vaacunas) Examen de ental (o prueeba de cita con dentista) Dos nombr res de emerrgencia y nú úmero de teeléfono d esttos formulaarios a ABC CD Inc. 10770 Park Avee o algún dee los otros ccentros. Ussted puede devolver Parra más información llaame a ABCD D al teléfon no 366-824 1 Ext 221 Muucha Graciaas ABCD D EARL LY LEAR RNING EA ARLY LEAR RNING APPL LICATION Applic cant/Child Informatio on Child’s/A Applicant’s Na ame: First: Addresss: House/ A Apartment # & Street Nam me: City: Mid ddle: Lasst: Gender: Sttate: Te elephone: Pho one #1: Language(s)): Phone #2: Eng glish Speakin ng Ability: Male:___ ____ Female:_ _____ Primary: Veryy Well:___ Well::___ Not Well:__ __ Not at all:___ _ Date of Birth: Mode off Transportatio on: Walk:__ ___ Se econdary: Own car:____ Zip Code: Frie end’s/Family m member car/rride:____ P Public:____ Servicess Needed: Full Day/ D Full Yea ar:______ Parrt Day/ Part Year:______ Y H Home Base:_ ______ Transitioning from EHS/DC:___ ____ Family y/Household Informa ation Mother o of child: Live es with child: yes____ no o____ Father o of child: Live es with child: yes____ no o____ Guardian’s name: Rellationship to cchild: Names o of other childrren in the houssehold Age Relationship R to o ch hild/applicant Other ad dult members in the househo old (over 18yyrs of age) A Age Relationship to child/a applicant I certify tthat the inform mation provided in this app plication is accurate and tru uthful to the b best of my knowledge Parent/G Guardian Sign nature: I would llike refer an eligible e family to your progrram: Name: Phone#: Confiden ntiality Statem ment: All inforrmation share ed with Early Learning L Stafff will be kept strictly confid dential unlesss its release is s authorizzed in writing. These forms s will be mainttained in locke ed files. For offfice use on nly Date recceived: Staff Signature: S Ap pril 2016 ABCD D EARL LY LEAR RNING APLIC CACIÓN DE D EARLY Y LEARNING Inform macion d el solicittante / ni no Nombre del solicitantte/ niño : Nombre: Medio: M Direcció ón: Casa / a apartamento # & nombre de la calle: Ciudad: Estado: Te eléfono: Te eléfono # 1: Fecha de nacimiento: Género: Macho:___ ____ Ap pellido: Idioma (s): Hembra: ______ Primaria: Secu undaria: Código posta al: T Teléfono # 2: Cap pacidad de ha ablar Ingles: Muyy bien:____ Bien n:____ Regular:_ ____ No sabes:_ ____ Modo de e transporte: caminar:____ _ coche propio:____ amigo / familia mie embros coche/paseo:____ _ público:_____ Servicios necesarios: Todo día a / todo año:_ ____ Día parrte / parte año o:____ Programa de Hom e Base;_____ _ Pasando de e EHS/DC:__ _____ Inform macion d e la fami lia/hogarr Madre d de niño: Vive con niños: ssí no ____ Padre de e niño: Vive con niños: ssí no ____ Nombre del encargad do: Rellación al niño: Nombres de otros niñ ños en el hogarr Edad Rellación con el niño (solicitante) adultos Otross miembros a en ell hogar (máss de 18 años de edad) E Edad Relacción con el niñ ño (solicitante) Certifico o que la inform mación proveíída en esta aplicación es correcta c y verrdadera de accuerdo a mi m mejor conocim miento Firma de el padre/enca argado: Quiero rreferir a otra familia f a su prrograma: Nom mbre: Teléfono #: Declaracción de confid dencialidad: Toda T informac ción compartiida será manttenida estricta amente confid dencial a men nos que usted lo autorices por escrito. Esto os formularios s serán mante eniendo bajo llave. Para uso de officina so lamente: Date recceived: Staff Signature: S Ap pril 2016 State of Connecticut Department of Education Early Childhood Health Assessment Record (For children ages birth – 5) To Parent or Guardian: In order to provide the best experience, early childhood providers must understand your child’s health needs. This form requests information from you (Part I) which will be helpful to the health care provider when he or she completes the health evaluation (Part II). State law requires complete primary immunizations and a health assessment by a physician, an advanced practice registered nurse, a physician assistant, or a legally qualified practitioner of medicine, an advanced practice registered nurse or a physician assistant stationed at any military base prior to entering an early childhood program in Connecticut. Please print Birth Date (mm/dd/yyyy) ❑ Male ❑ Female Parent/Guardian Name (Last, First, Middle) Home Phone Cell Phone Early Childhood Program (Name and Phone Number) Race/Ethnicity Primary Health Care Provider: ❑ American Indian/Alaskan Native ❑ Hispanic/Latino ❑ Black, not of Hispanic origin ❑ Asian/Pacific Islander ❑ White, not of Hispanic origin ❑ Other Child’s Name (Last, First, Middle) Address (Street, Town and ZIP code) Name of Dentist: Health Insurance Company/Number* or Medicaid/Number* Does your child have health insurance? Y Does your child have dental insurance? Y Does your child have HUSKY insurance? Y N N N If your child does not have health insurance, call 1-877-CT-HUSKY * If applicable Part I — To be completed by parent/guardian. Please answer these health history questions about your child before the physical examination. Please circle Y if “yes” or N if “no.” Explain all “yes” answers in the space provided below. Any health concerns Y N Allergies to food, bee stings, insects Allergies to medication Any other allergies Any daily/ongoing medications Any problems with vision Uses contacts or glasses Any hearing concerns Y Y Y Y Y Y Y N N N N N N N Frequent ear infections Any speech issues Any problems with teeth Y Y Y N N N Has your child had a dental examination in the last 6 months Y N Very high or low activity level Weight concerns Y Y N N Problems breathing or coughing Y N Y Y Y Y Y N N N N N Developmental — Any concern about your child’s: 1. Physical development Y N 5. Ability to communicate needs 6. Interaction with others 2. Movement from one place to another Y N 7. Behavior 3. Social development Y N 8. Ability to understand 4. Emotional development Y N 9. Ability to use their hands Asthma treatment Seizure Diabetes Any heart problems Emergency room visits Any major illness or injury Any operations/surgeries Lead concerns/poisoning Sleeping concerns High blood pressure Eating concerns Toileting concerns Y Y Y Y Y Y Y Y Y Y Y Y N N N N N N N N N N N N Birth to 3 services Preschool Special Education Y Y N N Explain all “yes” answers or provide any additional information: Have you talked with your child’s primary health care provider about any of the above concerns? Y N Please list any medications your child will need to take during program hours: All medications taken in child care programs require a separate Medication Authorization Form signed by an authorized prescriber and parent/guardian. I give my consent for my child’s health care provider and early childhood provider or health/nurse consultant/coordinator to discuss the information on this form for confidential use in meeting my child’s health and educational needs in the early childhood program. ED 191 REV. 8/2011 Signature of Parent/Guardian C.G.S. Section 10-16q, 10-206, 19a.79(a), 19a-87b(c); P.H. Code Section 19a-79-5a(a)(2), 19a-87b-10b(2) Date ED 191 REV. 8/2011 Part II — Medical Evaluation Health Care Provider must complete and sign the medical evaluation, physical examination and immunization record. Child’s Name Birth Date ❑ I have reviewed the health history information provided in Part I of this form Date of Exam (mm/dd/yyyy) (mm/dd/yyyy) Physical Exam Note: *Mandated Screening/Test to be completed by provider. *HT in/cm % *Weight lbs. oz / % BMI / % *HC in/cm % *Blood Pressure (Birth – 24 months) / (Annually at 3 – 5 years) Screenings *Vision Screening *Hearing Screening *Anemia: at 9 to 12 months and 2 years ❑ EPSDT Subjective Screen Completed (Birth to 3 yrs) ❑ EPSDT Annually at 3 yrs (Early and Periodic Screening, Diagnosis and Treatment) ❑ EPSDT Subjective Screen Completed (Birth to 4 yrs) ❑ EPSDT Annually at 4 yrs (Early and Periodic Screening, Diagnosis and Treatment) *Hgb/Hct: Type: Type: Right Left With glasses 20/ 20/ Without glasses 20/ 20/ Test done: ❑ No Left ❑ Pass ❑ Pass ❑ Fail ❑ Fail ❑ Yes *Dental Concerns ❑ Yes Date: ❑ Referral made to: Results: ❑ No ❑ Yes Has this child received dental care in the last 6 months? ❑ No ❑ Yes Treatment: *Developmental Assessment: (Birth – 5 years) ❑ No *Lead: at 1 and 2 years; if no result screen between 25 – 72 months ❑ No ❑ Referral made to: ❑ No *Date Lead poisoning (≥ 10ug/dL) ❑ Unable to assess ❑ Unable to assess ❑ Referral made to: *TB: High-risk group? Right ❑ Yes ❑ Yes *Result/Level: *Date Other: Type: Results: *IMMUNIZATIONS ❑ Up to Date or ❑ Catch-up Schedule: MUST HAVE IMMUNIZATION RECORD ATTACHED *Chronic Disease Assessment: Asthma ❑ No ❑ Yes: ❑ Intermittent ❑ Mild Persistent ❑ Moderate Persistent If yes, please provide a copy of an Asthma Action Plan ❑ Rescue medication required in child care setting: ❑ No ❑ Yes Allergies ❑ No ❑ Yes: ❑ No ❑ Yes Epi Pen required: History/risk of Anaphylaxis: ❑ No ❑ Yes: ❑ Food ❑ Insects ❑ Latex ❑ Medication ❑ Unknown source If yes, please provide a copy of the Emergency Allergy Plan Diabetes Seizures ❑ No ❑ No ❑ Yes: ❑ Yes: ❑ Type I Type: ❑ Type II ❑ Severe Persistent ❑ Exercise induced Other Chronic Disease: ❑ This child has the following problems which may adversely affect his or her educational experience: ❑ Vision ❑ Auditory ❑ Speech/Language ❑ Physical ❑ Emotional/Social ❑ Behavior ❑ This child has a developmental delay/disability that may require intervention at the program. ❑ This child has a special health care need which may require intervention at the program, e.g., special diet, long-term/ongoing/daily/emergency medication, history of contagious disease. Specify: ❑ No ❑ Yes This child has a medical or emotional illness/disorder that now poses a risk to other children or affects his/her ability to participate safely in the program. ❑ No ❑ Yes Based on this comprehensive history and physical examination, this child has maintained his/her level of wellness. ❑ No ❑ Yes This child may fully participate in the program. ❑ No ❑ Yes This child may fully participate in the program with the following restrictions/adaptation: (Specify reason and restriction.) ❑ No ❑ Yes Is this the child’s medical home? ❑ I would like to discuss information in this report with the early childhood provider and/or nurse/health consultant/coordinator. Signature of health care provider MD / DO / APRN / PA Date Signed Printed/Stamped Provider Name and Phone Number Child’s Name: Birth Date: REV. 8/2011 Immunization Record To the Health Care Provider: Please complete and initial below. Vaccine (Month/Day/Year) Dose 1 Dose 2 Dose 3 Dose 4 Dose 5 DTP/DTaP/DT IPV/OPV MMR Measles Mumps Rubella Hib Hepatitis A Hepatitis B Varicella PCV* vaccine Rotavirus MCV** Flu Other Dose 6 *Pneumococcal conjugate vaccine **Meningococcal conjugate vaccine Disease history for varicella (chickenpox) (Date) Exemption: (Confirmed by) Religious Medical: Permanent †Temporary †Recertify Date †Recertify Date †Recertify Date Date Immunization Requirements for Connecticut Day Care, Family Day Care and Group Day Care Homes Vaccines Under 2 By 3 By 5 By 7 By 16 16–18 By 19 2-3 years of age 3-5 years of age months of age months of age months of age months of age months of age months of age months of age (24-35 mos.) (36-59 mos.) DTP/DTaP/ DT None 1 dose 2 doses 3 doses 3 doses 3 doses 4 doses 4 doses 4 doses Polio None 1 dose 2 doses 2 doses 2 doses 2 doses 3 doses 3 doses 3 doses MMR None None None None Hep B None 1 dose 2 doses 2 doses HIB None 1 dose 2 doses Varicella None None None None None None Pneumococcal Conjugate None 1 dose 2 doses 3 doses 1 dose after 1st birthday 1 dose after 1st birthday 1 dose after 1st birthday Hepatitis A None None None None 1 dose after 1st birthday5 1 dose after 1st birthday5 1 dose after 1st birthday5 Influenza None None 1 or 2 doses 1 or 2 doses 1 or 2 doses6 1 or 2 doses6 1 or 2 doses6 1 dose after 1st 1 dose after 1st 1 dose after 1st 1 dose after 1st 1 dose after 1st birthday1 birthday1 birthday1 birthday1 birthday1 2 doses 2 doses 3 doses 3 doses 3 doses 2 or 3 doses 1 booster dose 1 booster dose 1 booster dose 1 booster dose 1 booster dose depending on after 1st after 1st after 1st after 1st after 1st vaccine given3 birthday4 birthday4 birthday4 birthday4 birthday4 Vaccine (PCV) 1 dose after 1 dose after 1 dose after 1st birthday or 1st birthday or 1st birthday prior history of prior history of or prior history disease1,2 disease1,2 of disease1,2 1 dose after 1st birthday 1 dose after 1st birthday 2 doses given 2 doses given 6 months apart5 6 months apart5 1 or 2 doses6 1 or 2 doses6 1. Laboratory confirmed immunity also acceptable 2. Physician diagnosis of disease 3. A complete primary series is 2 doses of PRP-OMP (PedvaxHIB) or 3 doses of HbOC (ActHib or Pentacel) 4. As a final booster dose if the child completed the primary series before age 12 months. Children who receive the first dose of Hib on or after 12 months of age and before 15 months of age are required to have 2 doses. Children who received the first dose of Hib vaccine on or after 15 months of age are required to have only one dose 5. Hepatitis A is required for all children born after January 1, 2009 6. Two doses in the same flu season are required for children who have not previously received an influenza vaccination, with a single dose required during subsequent seasons Initial/Signature of health care provider MD / DO / APRN / PA Date Signed Printed/Stamped Provider Name and Phone Number ABCD D EARL LY LEAR RNING nt, Deear Paren Taake the Dental Exaam Form to the Deentist. It iss very im mportant thhat your cchild haas a dental exam beefore he/sshe is enrrolled in th the Child Care Proogram at A ABCD Incc. Yoour child’’s doctor cannot co omplete this t form. If you do not have a dentist leet us know w. We wiill help yoou to locaate a denttist. p , Esstimados padres Toomar estaa forma dee Examen n Dental al a Dentistta. Es muuy importaante que ssu hijo tennga un ex xamen den ntal antess de que él é o ella eestá inscriito en el pprograma en AB BCD Inc.. Ell pediatra no puedee complettar este fo ormularioo. Si usted no tiene un dentista nos n dejó saber. s Tee ayudarem mos a loccalizar a uun deentista. D ABCD EARL LY LEAR RNING Den ntal Form F Name of o the Child d : _______ __________ ________________________ Date of Birth: _______ __________ ________________________ ___________ ________________________ Date of Dentist Viisit: ______ REAS SON FOR D DENTAL V VISIT UPPER C B E F G H I LINGUAL L A LEFT D J 14 3 30 T 19 K LINGUAL L S M R Q N P O LO OWER RIGHT 1 □ ORAL E EXAMINAT TION 2 □ PREVE ENTIVE CA ARE □ □ □ C Cleaning F Flouride Ap pplication S Sealant Application 3 □ TREATMMENT □ Exxtraction □ Reestorationn □ Puulp Therappy w –up or work w is needed please provide appointme ent date: If Follow Date: __________ _ ___________ _________ d for Follow-up needed □ Cleaningg □ XX-rays □ Treatmeent DENTIS ST NAME & SIGNATU URE & DAT TE Revised January 2016 a b d c The mission of ABCD’s Early Learning Division is to empower families so that they may overcome the impact of poverty and improve the quality of life for all family members. To that end, ABCD is committed to a comprehensive program consisting of: Family & Child Services for all family members ABCD / INNER CITY CHILDREN’S CENTER 1070 Park Ave Bridgeport, CT LUCILLE E. JOHNSON CENTER 816 Fairfield Ave Bridgeport, CT 203-366-8241-X 273 203-331-4541 ABCD at HOLY NAME OF JESUS CENTER 1950 Barnum Ave Stratford, CT ABCD at GEORGE E. PIPKIN CENTER 52 George Pipkins Way Bridgeport, CT 203-385-1127 203-576-9960 x 231 TRUMBULL GARDENS CENTER 715 Trumbull Ave Bridgeport, CT CESAR BATALLA CTR 927 Grand Street Bridgeport, CT 203-336-2153 203-371-5117 Inclusive of parents in the implementation & development of programs and policies BULLS HEAD HOLLOW HEADSTART 108 Sanford Ave Bridgeport, CT CHARLES B TISDALE CENTER 1795 Stratford Ave Bridgeport, CT Advocacy and support for families and children 203-338-9640 203-330-0166 An enhanced collaboration between and among family & child services agencies to improve the knowledge and responsiveness of these agencies to the needs of children and their families The fulfillment of this mission will create a collaborative consisting of parent, agency, and community of opportunity for all families and their children. JAMIE A. HULLEY CTR 460 Lafayette St Bridgeport, CT WEST END CENTER 361 Bird Street Bridgeport, CT 203-367-6801 203-335-0553 TENDER LOVING CARE: THERAPEUTIC PROGRAM (TLCC) ABCD 1070 Park Ave Bridgeport, CT FULL & PART YEAR TRUMBULL / MONROE REGIONAL HEAD START 240 Middlebrooks Ave Trumbull, CT 203-366-8241 x 244 203-452-4423 PART DAY/PART YEAR: BULLARDS HAVEN 500 Palisade Ave Bridgeport, CT PART DAY/PART YEAR: ABCD at STRATFORD SOUTHEND COMMUNITY CTR 19 Bates Street Stratford, CT 203-377-4721 203-579-6333 x 6611 ACTION FOR BRIDGEPORT COMMUNITY DEVELOPMENT 1070 PARK AVE BRIDGEPORT, CT www.abcd.org The first five years of childhood are the most important in development and learning. Our educational curriculum is designed to help children reach their fullest potential. At ABCD we have set the standard for the highest quality of preschool programs in the Greater Bridgeport area. Our programs feature fun, age-appropriate lessons and activities which help develop the whole child: physically, intellectually, emotionally and socially. Each child is encouraged to explore and discover at his or her own pace. Not only do we provide services for the children, we also help families with their needs. Our social service team is ready to assist families with referrals to community agencies or other ABCD programs. Most families qualify for our sliding scale fee or free programs. Our curriculum has been developed in accordance with CT Department of Education Early Learning standards as well as the Head Start’s Creative Curriculum program with the goal of School Readiness. In addition our Early Head Start Home Based program option supports children and their families through home visits and group socialization experiences. ABCD welcomes all children. We greatly appreciate the cultures of all our families and staff and provide a multicultural environment. We assist in providing translation services. Our qualified staff are also trained for children with disabilities. With on-site support from mental health, education and disabilities specialists all children are assured to receive the required services. Assistance with referrals for children are also available. We provide free nutritional meals daily. The meals are planned by the staff nutritionist with the parents, staff, and the caterer. We also have health professionals on staff who assist with children’s health concerns at the centers. We have an open door policy and parents are always welcome. Parents have the opportunity to volunteer in their child’s classroom and also become active members of many different parent groups.