Actas Urológicas Españolas
Anuncio

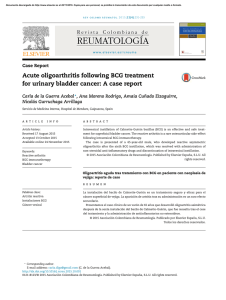
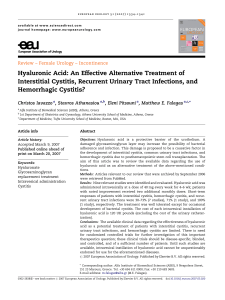
Documento descargado de http://www.elsevier.es el 18/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. Actas Urol Esp. 2012;36(10):624---625 Actas Urológicas Españolas www.elsevier.es/actasuro LETTERS TO THE EDITOR Evaluating the role of computerized tomography triphasic urography in patients with painless hematuria: A practical view夽 Evaluar el papel de la urografía por tomografía computarizada trifásica en pacientes con hematuria sin dolor: una visión práctica Dear Sir, Computed tomography triphasic urography (CTU) is a relatively new diagnostic imaging examination providing comprehensive anatomical and clinical evaluation of the upper and lower urinary tract. As CTU has become more widely available, CTU began to replace other imaging techniques, especially intravenous urography and ultrasonography in investigating painless hematuria.1,2 We assessed our experience regarding the use of CTU as first line imaging modality in patients with painless hematuria who attended one stop hematuria clinic for flexible cystoscopy. A total of 50 patients presented to our institution with painless hematuria over a two-year period were included. Mean age was 63.5 years. Male to female ratio was 3:1. CTU, flexible cystoscopy findings and risk factors were all documented for each patient. Overall abnormal findings of CTU were 66% (33/48). 23 patients developed macroscopic hematuria (Fig. 1). 12 patients were cigarette smokers. Malignant causes were 3 renal cell carcinomas and 3 bladder transitional cell carcinomas (TCC) (12%). Cystoscopy findings of bladder tumors corresponded to their CTU results. Benign causes were 14 renal cysts, consisting of 12 simple and 2 complex (Bosniak II), 3 calculi (1 kidney and 2 ureteric), 1 renal infarction, 4 bladder wall thickening and 1 benign adrenal adenoma. Malrotated and horseshoe kidney were also diagnosed on CTU. All the bladder tumors that were seen on flexible cystoscopy had been imaged on CTU. 夽 Please cite this article: Raheem OA, et al. Evaluar el papel de la urografía por tomografía computarizada trifásica en pacientes con hematuria sin dolor: una visión práctica. Actas Urol Esp. 2012;36:624---5. Figure 1 Results of computed tomography triphasic urography (CTU). (A) Phase without contrast: the primary interpolar tumor is not clearly visible. (B) Nephrographic phase: a solid lesion (arrowhead) shows uptake in the interpolar region of the right kidney. (C) Excretory phase: right calyces, pelvis, and proximal ureter without evidence of hydronephrosis. CTU can image kidneys, ureters and bladder in one investigation with a greater sensitivity for identifying the cause of hematuria. This systematic study showed an incidence of urological malignancy of 12% and overall abnormal findings of 66%. Where available, it is recommended to use CTU as first-line investigation in hematuria patients, replacing ultrasonography and intravenous urography, particularly in high-risk patients. Adding to this, CTU serves as a critical adjuvant to cystoscopy in evaluating patients with hematuria and excluding bladder carcinoma. 2173-5786/$ – see front matter © 2012 AEU. Published by Elsevier España, S.L. All rights reserved. Documento descargado de http://www.elsevier.es el 18/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. LETTERS TO THE EDITOR References 1. Van Der Molen AJ, Cowan NC, Mueller-Lisse UG, Nolte-Ernsting CC, Takahashi S, Cohan RH, CT Urography Working Group of the European Society of Urogenital Radiology (ESUR). CT urography: definition, indications and techniques. A guideline for clinical practice. Eur Radiol. 2008;18:4---17. 2. O’Keeffe SA, McNally S, Keogan MT. Investigating painless haematuria. BMJ. 2008;337:a260. Bone metastases in muscle invasive bladder carcinoma: Clinical consideration夽 Metástasis Óseas en el Carcinoma Vesical Músculo Invasivo: Examen Clínico Dear Sir, Metastatic transitional cell carcinoma (mTCC) of the bladder to the bone is uncommon occurrence when compared to the breast and prostate carcinoma.1 This may be due to intrinsic biological properties of tumor cells and/or mechanisms of metastases. Notably, high-grade, muscle-invasive bladder carcinoma metastasizes more commonly to regional lymph nodes, at lower rate to the lungs and liver.2---5 We sought to evaluate and establish the prevalence of bone metastasis of muscle invasive bladder carcinomas in well-defined cohort of bladder carcinoma patients at a single academic institution and commented on their subsequent management over an 8-year period. Between July 2000 and June 2008, 376 cases of TCC of bladder were diagnosed. Of these, 8 patients demonstrated mTCC to bony structures. The male to female ratio was 5---3 and the mean age at the time of diagnosis was 67.7. TCC grade and stage (T, tumor; N, nodes; M, metastasis), interval diagnosis of bone metastasis, bone metastasis site, imaging and treatment were also documented. The prevalence of bone mTCC of bladder was 0.02% (8/376). Pathologically, T2 G2 and T3 G2 were the most common histological category (3/8 in each category) whereas T1b G2 was demonstrated in 2 patients. Spinal and femoral metastases were the most common bone mTCC bladder (5/8 and 2/8 patients, respectively). One patient with mTCC had bony metastasis to the ribs. Isotope bone scan was the imaging modality of choice to establish the bony metastatic lesions. 4 patients required external beam radiotherapy to alleviate symptoms of bony metastatic lesions. 2 patients of femoral metastasis required surgical radical excision and 夽 Please cite this article as: Raheem OA, et al. Metástasis óseas en el carcinoma vesical músculo invasive: examen clínico. Actas Urol Esp. 2012;36:625. 625 O.A. Raheem ∗ , R.G. Casey, E. Elmusharaf, D.J. Galvin, T.E.D. McDermott, R. Grainger , T.H. Lynch Servicio de Urología, St James’s Hospital, Dublin, Ireland Corresponding author. E-mail address: [email protected] (O.A. Raheem). ∗ intramedullary nailing and another 2 patients were treated with systematic chemotherapy. We reported on the prevalence of bone mTCC of bladder and commented on their management. With the advancement of skeletal imaging in the form of isotope nuclear scans, the metastatic trends are thought to be changing. Urologists and clinicians should be vigilant to look for bony lesions in the patients with TCC of the bladder when they present with bony or skeletal-related pain and should be prompted by imaging such as isotope nuclear scan. The answer will only be found in a large randomized study where patient’s survival and oncological outcomes are endpoints. References 1. Taher AN, Kotb MH. Bone metastases in muscle-invasive bladder cancer. Egypt Natl Canc Inst. 2006;18:203---8. 2. Petković M, Muhvić D, Zamolo G, Jonjić N, Mustać E, MrakovćićSutić I, et al. Metatarsal metastasis from transitional cell cancer of the urinary bladder. Coll Antropol. 2004;28:337---41. 3. Chua WC, Martin PA, Kourt G. Orbital metastasis from transitional cell carcinoma of the bladder. Clin Experiment Ophthalmol. 2004;32:447---9. 4. Adriazola Semino M, Ortiz Cabria R, García Cobo E, Tejeda Bañez E, Alonso Villalba A, Romero Rodríguez F. Distal bone metastases of transitional-cell carcinoma of the bladder. Apropos of a case. Arch Esp Urol. 2002;55:69---70. 5. Punyavoravut V, Nelson SD. Diffuse bony metastasis from transitional cell carcinoma of urinary bladder: a case report and review of literature. J Med Assoc Thai. 1999;82:839---43. O.A. Raheem a,∗ , A. Molloy b , R.G. Casey a , T.H. Lynch a a Department of Urology, St James’s Hospital, Dublín, Ireland b Department of Orthopedics, St James’s Hospital, Dublín, Ireland Corresponding author. E-mail address: [email protected] (O.A. Raheem). ∗