- Ninguna Categoria
Informe sobre procedimiento de terapia fotodinámica en
Anuncio
Informes valorativos 2001 e r v i c i o e v a l u a c i ó n Terapia fotodinámica en oftalmología Degeneración macular asociada a la edad e c n o l o g í a s GENERALITAT VALENCIANA febrero 2001 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 I.- PREÁMBULO Y PLANTEAMIENTO SEGUIDO..............................................1 II.- EXTRACTO DE LA INFORMACIÓN RECOPILADA.......................................3 II.I.- DATOS MANEJADOS ..........................................................................3 II.II.- EVIDENCIAS Y CONCLUSIONES .......................................................7 III.- RECOMENDACIONES Y SUGERENCIAS....................................................10 APÉNDICES .......................................................................................................................13 APÉNDICE A Criterios de indicación, Criterios de no indicación ..........................................13 APÉNDICE B Procedimientos e instrumentación, Modo de administración y reintervención.................................................................................................14 APÉNDICE C Guía de conocimientos clínicos......................................................................15 APÉNDICE D Datos a recoger y documentar (susceptibles de mecanizar y tratar)..............16 APÉNDICES E prevalencias poblacionales referidas o estimadas a partir de datos de los estudios de prevalencia/incidencia poblacional seleccionados.................17 APÉNDICE F escenarios de costes previsto ........................................................................19 ANEXOS .......................................................................................................................20 1.- febrero 2001. ANEXO DOCUMENTAL DE EXPLOTACIÓN DE DATOS DE CONCIERTOS ............................................................................................................... 21 2.- febrero 2001. ANEXO DOCUMENTAL DE LA BÚSQUEDA BIBLIOGRÁFICA EN LA CDR (en sus bases de datos DARE, NHS EED y HTA)........................................... 29 3.- febrero 2001. ANEXO DOCUMENTAL DE LA BÚSQUEDA BIBLIOGRÁFICA EN MEDLINE A TRAVÉS DE LA NATIONAL LIBRARY OF MEDICINE (bajo criterios: “photodynamic therapy degeneration macular”) ............................................................ 31 4.- febrero 2001. ANEXO DOCUMENTAL DE LA BÚSQUEDA BIBLIOGRÁFICA EN MEDLINE A TRAVÉS DE LA NATIONAL LIBRARY OF MEDICINE (bajo criterios: “prevalence blindness older” or “epidemiology maculopathy” or “prevalence aged macular”) ........................................................................................................................ 36 5.- marzo 2000. SMM-REPORT NR.3/2000 THE NORWEGIAN CENTRE FOR HEALTH TECHNOLOGY ASSESSMENT Photodynamic therapy for age-related macular degeneration..................................................................................................... 57 6.- 1.994: GUIDE CANADIEN DE MEDICINE CLINIQUE ET PRÉVENTIVE. Dépistage de la deficience visuelle chez les personnes âgées ..................................... 68 7.- enero 2000. NATIONAL HORIZON SCANNING CENTRE. Photodynamic therapy for age-related macular degeneration. ........................................................................... 83 8.- Issue 1, 2001. Oxford. THE COCHRANE LIBRARY (COCHRANE REVIEW). Photodynamic therapy for neovascular age-related macular degeneration................... 90 9.- enero 2001. Irveng Arons in OCULAR SURGERY NEWS. Visudyne looks promising for treating wet AMD .................................................................................... 108 10.- febrero 2001: Información registrada en la FDA sobre el verteporfin .......................... 113 11.- febrero 2001: Información registrada en la EMEA sobre el verteporfin ....................... 126 INDICE INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 INFORME VALORATIVO A DEMANDA I.- PREAMBULO Y PLANTEAMIENTO SEGUIDO En fecha 12-II-2001 se recibe en estas dependencias solicitud de informe valorativo relativo a la aplicación de la técnica de terapia fotodinámica que se viene realizando por el servicio de oftalmología del hospital Universitario La Fe y de manera derivada en centros asistenciales privados. Ya en el seno del grupo de trabajo de “Organización de la Investigación médico-clínica: Usos Tutelados”, y por parte del Dr. José Luis Rey (jefe del Área de asistencia sanitaria), se comentaron las dudas que para el servicio de Conciertos se planteaban, acerca de la efectividad y eficacia de la citada técnica. A pesar de que este tipo de teapia se utiliza en otros campos especializados (dermatología y oncología) y dado lo requerido en la solicitud, nos ceñiremos en el presente informe a la utilización de la citada técnica en el campo oftalmológico. En concreto se analizarán las indicaciones dirigidas a la resolución de problemas visuales derivados de la degeneración macular asociada a la edad [DMAE (acrónimo en español), ARM, ARMD (acrónimos en inglés), DMLA (acrónimo en francés)]. La solicitud de informe valorativo recibida abarca un amplio campo prospectivo (utilidad, nivel de adecuación, guía de uso, optimización de recursos, previsión de demanda y análisis de escenarios, entre otros). Por ello se ha recurrido para la elaboración de este trabajo, a diversos servicios y organismos que pudieran aportarnos datos o informaciones relevantes para el tema y los campos a evaluar. Así pues y por dicho motivo se ha recabado información de diversos servicios de la Conselleria de Sanidad, en un intento de recopilar toda aquella pertinente para el tema de análisis. Así pues mencionaremos ahora las peticiones de datos efectuadas a los servicios de Epidemiología, de Conciertos, de Actividad Asistencial y de Prestación Farmaceútica. Tras la recepción de lo solicitado, (cuando ésto se ha producido) se ha procedido en este Servicio de Evaluación de Tecnologías al cotejo y análisis de los datos, y al extracto y confección de indicadores ajustados a las necesidades que el informe requería. Pá gina 1 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Así mismo se ha procedido a solicitar información en el propio hospital Universitario La Fe. Pareció prudente sin embargo, prescindir de recabar datos de otros servicios asistenciales públicos o privados de la Comunidad Valenciana ralacionados con esta técnica, dado que este informe no es sino un primer intento de acercamiento sistemático al tema. Por ello se consideró que debiera huirse de alentar espectativas innecesarias en esta fase evaluativa inicial. También se ha recogido información de las diversas agencias de evaluación de tecnologías tanto nacionales (autonómicas y española), como de las extranjeras. Igualmente se han sondeado bases de datos del campo asistencial especializado oftalmológico, así como aquellas obrantes y accesibles divulgadas por las sociedades científicas y profesionales en relación con el campo de análisis. Del mismo modo se ha reclutado información relevante de institutos y centros oftalmológicos nacionales y extranjeros con competencia en el tema abordado. Pá gina 2 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad II.- REF.: ACEMSA/SET/AC/ac febrero-2001 EXTRACTO DE LA INFORMACIÓN RECOPILADA (En este apartado se reseñarán diversos datos considerados como elocuentes y representativos de la información global contenida en todo el informe. Se ha pretendido que de la lectura de este cuerpo del informe, se puedan obtener elementos de juicio claros para las decisiones a acometer. En el material anexado a este informe, se reflejan diversas explotaciones, análisis y referencias de forma más exhaustiva a lo sintetizado en este apartado). II.I.- 1.- DATOS MANEJADOS En contacto con el servicio de conciertos, se constata la presentación de un total de 190 casos propuestos para la realización de la técnica reseñada. Diversas características de los casos para los que se dispone información en el mencionado servicio, pueden observarse en la siguiente tabla. Lo presentado en los anexos, permite un más amplio y exhaustivo conocimiento de las solicitudes de terapia fotodinámica que han sido registradas hasta la fecha en el servicio de conciertos. DATOS EXISTENTES EN CONCIERTOS SOBRE: SOLICITUDES DE TERAPIA FOTODINÁMICA: AÑO Y MES DE ESTIMACIÓN POR CONCIERTOS % por AÑO – MES DE ESTIMACIÓN Recuento ACEPTA CONCIERTOS SI NO 2000-01 2000-02 2000-03 2000-04 2000-05 2000-06 2000-07 2000-08 2000-09 2000-10 2000-11 2000-12 2001-01 2001-02 TOTAL 10 10 16 13 10 10 13 13 3 1 2 1 7 1 110 1 1 3 10 7 18 25 11 1 1 1 1 80 TOTAL 10 11 17 16 20 17 31 38 14 2 3 2 7 2 190 ACEPTA CONCIERTOS SI NO 100.0% 90.9% 94.1% 81.3% 50.0% 58.8% 41.9% 34.2% 21.4% 50.0% 66.7% 50.0% 100.0% 50.0% 57.9% 9.1% 5.9% 18.8% 50.0% 41.2% 58.1% 65.8% 78.6% 50.0% 33.3% 50.0% 50.0% 42.1% TOTAL 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% % por MES ESTIMACION ACEPTA CONCIERTOS SI NO 9.1% 9.1% 14.5% 11.8% 9.1% 9.1% 11.8% 11.8% 2.7% .9% 1.8% 0.9% 6.4% 0.9% 100.0% 1.3% 1.3% 3.8% 12.5% 8.8% 22.5% 31.3% 13.8% 1.3% 1.3% 1.3% 1.3% 100.0% TOTAL POR MES 5.3% 5.8% 8.9% 8.4% 10.5% 8.9% 16.3% 20.0% 7.4% 1.1% 1.6% 1.1% 3.7% 1.1% 100.0% Pá gina 3 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad 2.- Puestos en REF.: ACEMSA/SET/AC/ac febrero-2001 contacto con el hospital Universitario La Fe se obtuvieron informaciones relativas al número de pacientes tratados, técnica de abordaje y resultados obtenidos hasta la fecha. Durante los meses de enero y febrero del año 2001, 54 pacientes han sido analizados en el citado hospital ante propuestas de aplicación de Terapia Fotodinámica. La aplicación de la técnica parece adaptarse en líneas generales a lo estipulado en la autorización vigente para el Verteporfin ®, en USA, Unión Europea y Suiza. No obstante, el protocolo de aceptación de técnica empleado en la Fe se ha ampliado así mismo para la miopia degenerativa (actualmente y todavía en fase de estudio –ensayo VIP multicéntrico). 3.- Mediante contacto con los servicios de Epidemiología, de Análisis de la Actividad asistencial y con el de Protocolarización, Alternativas Asistenciales y Evaluación Económica se pretendía recoger información relativa al alcance de la patología oftalmológica intervenible con la técnica citada, de aquella otra cercana a la misma y de los costes imputables a dicha actividad asistencial. De ninguno de los servicios se nos refiere información específica de la patología a estudio. Únicamente se toman en consideración datos relativos a incidencia atendida o prevalencia poblacional para patologías cercanas o “competidoras asistenciales” de la analizada. Ésta información se ha tenido Pá gina 4 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 en cuenta de cara a proyectar escenarios y calibrar mejor las estimaciones y recomendaciones que posteriormente se presentan. 4.- En la misma fecha del recibo de la solicitud, se procede a realizar búsquedas dirigidas en diversas bases de datos de evaluación de tecnologías y científicas a las que desde este servicio se tiene acceso pleno o parcial: INAHTA, ISTAH, AEETSA, CDR-NHS, MEDLINE, COCHRANE LIBRARY. En dichos procesos indagatorios, se han empleado métodos de sondeo aproximativos recursivo-selectivos al tema buscado. Los criterios últimos de búsqueda, se expresan en las diversas tablas que se adjuntan en el informe. Así mismo en información anexada se presentan los artículos o resúmenes de las referencias más relevantes y que dan soporte a las recomendaciones que se plantean en el informe. 5.- Mediante las búsquedas dirigidas empleadas, se han localizado una serie de análisis evaluativos efectuados por diversas agencias de evaluación nacionales y extranjeras. La existencia y posibilidad de acceso a revisiones sistemáticas, metaanálisis y diversos ensayos clínicos controlados han permitido aumentar la base científica en la que se apoyan los elementos de juicio, así como las recomendaciones y sugerencias que se plantean. 6.- Tras los procesos de búsqueda dirigida, las referencias halladas de forma inmediata han sufrido un cotejo selectivo previo a su análisis y consideración definitiva. En dicho sentido los criterios ponderados de selección empleados han sido: 1.- Relevancia de la información aportada para la indagación 2.- Robustez del diseño y método científico empleado 3.- Entornos socioeconómicos comparables o análogos a nuestro entorno 4.- Información accesible Las referencias han sido analizadas en su versión íntegra siempre que ha sido posible acceder a ellas, no desdeñándose aquella que sólo ha podido ser accesible en su formato resumido. Pá gina 5 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad 7.- REF.: ACEMSA/SET/AC/ac febrero-2001 En una segunda etapa se han sondeado como registros específicos, (aparte de las bases antes descritas), las de la FDA americana y la EMEA europea, dado que la técnica a analizar precisa de la utilización de productos farmacológicos de reciente incorporación al mercado farmacológico. En dicho sentido y como ya ha sido reseñado, también se ha solicitado la información obrante en diversos servicios dependientes de la D.G. para la Prestación Farmaceútica, en búsqueda de información respecto a la adquisición, uso, conservación y reacciones adversas a los fármacos involucrados en la técnica analizada. Desde esa dirección, no se nos ha comunicado hasta la fecha reacciones al producto. No obstante hay una prolija descripción de las mismas en referencias procedentes de la FDA o EMEA, así como en otras de las fuentes manejadas. Pá gina 6 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Tras la lectura, extracto y análisis de la profusa información final seleccionada, se pueden avanzar ciertas conclusiones: II.II.- 1.- EVIDENCIAS Y CONCLUSIONES La relativamente reciente finalización del ensayo clínico controlado a doble ciego para el uso del Verteporfin® (Visudyne) en fase II y posterior fase III (TAP 1 y 2, VIP 1 y 2 en proceso), y los datos aportados por el mismo, han servido como elemento de juicio científico para la autorización de dicho producto y unas indicaciones precisas para la realización de la Terapia Fotodinámica en el caso de la degeneración macular asociada a la edad para su forma exudativa con degeneración neovascular retrofoveal visible (presentación clásica). Dichas autorizaciones se realizaron en abril del 2000 en USA y en junio del 2000 para los países de la Unión Europea. Actualmente no se han obtenido evidencias formales que permitan la autorización para la miopía degenerativa, para la DMAE no exudativa, ni para la DMAE exudativa no visible. 2.- Para los casos en los que existe degeneración neovascular con característica geográfica extrafoveal, la técnica de la fotocoagulación con láser es la de elección. No así en los casos en donde se invade francamente mácula y fóvea. En estos casos, la nueva técnica pudiera presentar una cierta ventaja comparativa ante los malos resultados obtenida con la anterior, a pesar de que el estudio TAP no contemplaba dicha comparación. 3.- Las diversas evaluaciones realizadas por las agencias coinciden en no recomendar la terapia fotodinámica en lesiones cuasi-asintomáticas y/o muy incipientes, en las no visibles y la desaconsejan en las variantes secas, constituyendo estas últimas casi el 90% de las degeneraciones maculares asociadas a la edad. 4.- La técnica empleada es meramente protectora de la mala evolución pronóstica, no abordando en absoluto las causas y factores desencadenantes de la degeneración macular. La terapia fotodinámica en la DMAE, como técnica estabilizadora que trata de ser, y para el tipo de pacientes indicado en el es- Pá gina 7 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 tudio TAP (base de la autorización), ostenta una eficacia comparativa menor del 28%. De los datos manejados en el propio estudio TAP se desprende un NNT=6’7 para todos los individuos tratados (se necesitan tratar 6’7 pacientes para que uno muestre el efecto mejorador). El NNT obtenido en el ensayo TAP es de 2, si en el análisis únicamente se consideran a los pacientes que cumplen las condiciones extrictas (DMAE, clásica con vasos visibles retrofoveales: presentación clásica). A parte del ensayo TAP, la aplicación de la técnica sobre el terreno, hace augurar a algunos expertos una efectividad inferior al 20%. Existen ahora mismo en marcha estudios y ensayos clínicos controlados que investigan la acción de ciertas substancias de la dieta o fármacos inhibidores de la neovascularización, que inhibirían o protegerían de la aparición de esta degeneración desencadenante de la enfermedad clínica. Ninguno de los finalizados hasta ahora, ha obtenido resultados concluyentes. 5.- En línea con las recomendaciones efectuadas por el gobierno canadiense en su guía: “Déspistage de la déficience visuelle chez les personnes âgées”, así como otros informes realizados en países nórdicos, en donde se analizan las oportunidades de priorizar actividades eficaces sobre catarata, glaucoma y degeneración macular asociada a la edad, sería preciso analizar con rigor, elementos tales como coste-utilidad, coste-efectividad, seguridad, NNT efectivo, así como medidas de impacto asistencial y social derivadas de la ponderación de unas alternativas de forma prioritaria sobre otras. Máxime en escenarios con recursos limitados y para los que se comparte (y compite) en recursos destinados a la asistencia de otras patologías oculares en población mayor (glaucoma, catarata, retinopatía diabética. Esta última se presenta en el 15.7% de los casos de diabetes según datos de la Red centinela sanitaria de la Comunidad Valenciana). 6.- La prevalencia de esta enfermedad, el aumento de longevidad en los paises de nuestro entorno socioeconómico, el mal pronostico visual para estos pacientes, el aparente casi nulo riesgo vital de la técnica y la presión del propio mercado sanitario, aventuran una rapidísma expansión de la citada técnica, como de hecho ya se está produciendo. Pá gina 8 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad 7.- REF.: ACEMSA/SET/AC/ac febrero-2001 El bajo coste relativo de amortización de los equipos/intervención (que se sitúa en una posición de gran ventaja sobre otras técnicas novedosas y de auge en el campo oftalmológico, y por tanto con una posibilidad de rendimiento económico por intervención mayor que otras técnicas), y el carácter de ser la única indicación viable para cierto grupo de pacientes (así considerado por los especialistas), abunda todavía más en la generación de una floreciente oferta de este tipo de intervención en el mercado sanitario. Estos hechos posiblemente presionen alentando prescripciones de dicha técnica para gradientes de degeneración macular más amplios que el actualmente indicado. 8.- Por último se hace preciso indicar que las empresas que comercializan o comercializarán los productos farmaceuticos involucrados en la técnica [Verteporfin ® de Ciba-visión-Novartis (ya autorizado), SnET2 de Miravant and Pharmacia & Upjohn (finalizando estudio), Optrin de Pharmacyclics (en estudio)], completarán probablemente estudios con potenciado poder estadístico (grandes muestras), que atestigüen mejoras comparativas en el límite, para fases de la DMAE incipientes. Bajo esta suposición, y dado el alto coste de los tratamientos y las altas prevalencias de las fases incipientes, podemos asistir a un componente de gasto importante para años venideros en los servicios sanitarios, como ya auguran diversos especialistas acerca de dicho fenómeno en el Medicare estadounidense. Pá gina 9 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad III.- REF.: ACEMSA/SET/AC/ac febrero-2001 RECOMENDACIONES Y SUGERENCIAS A la luz de los datos barajados en el informe y sus anexos, se plantean una serie de ejes de actuación en la actuación de diversos servicios competentes para cada una de las materias a abordar: 1.- Parece necesaria la planificación con el máximo rigor (6 meses – 12 meses) de una serie de líneas o medidas a poner en práctica de forma escalonada. Para la elaboración de las mismas y su puesta en marcha, parece necesario el consurso y asesoramiento de oftalmólogos o bien de institutos oftalmológicos con capacidad de ajustar de forma precisa y científica las diversas circunstancias inherentes a la propia técnica. A falta de lo anterior y como planteamientos operativos previos, parece conveniente lo siguiente: 1.1.- Generación de normativa clara respecto a la prescripción de la terapia, criterios de intervención y flujos procedimentales de la citada técnica (Una serie de propuestas preliminares se ofrecen en páginas subsiguientes: apéndices A y B). 1.2.- Guía clínica de actuación e indicaciones para los pacientes con DMAE franca. (Una serie de propuestas preliminares se ofrecen en páginas subsiguientes: apéndice C). 1.3.- Adecuación de un subsistema informativo para la captación de información asistencial de este tipo de patología. Conveniencia de generar un registro específico para esta enfermedad, ligado o no a registro poblacional de ceguera. (Una serie de propuestas preliminares se ofrecen en páginas subsiguientes: apéndice D). 1.4.- Pautas de anotación y registro específicas para la terapia fotodinámica (a modo de registro de intervención específica documentada). (Una serie de propuestas preliminares se ofrecen en páginas subsiguientes: apéndice D). Pá gina 10 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad 1.5.- REF.: ACEMSA/SET/AC/ac febrero-2001 Estudio poblacional transversal sobre deficit visual y ceguera en personas de más de 50 años, con evaluación específica para este tipo de degeneración asociada a la edad. (Una estimación proyectada se ofrece en las tablas subsiguientes: apéndice E). 2.- Autorización de la técnica citada por parte del servicio competente y establecimiento de los criterios de adquisición y registro del aparataje (en el sector público) de forma reglada y centralizada. La homologación formal de centros (referenciales o no), para la ejecución de esta técnica es una línea que debiera valorarse e impulsarse en su caso. 3.- Estudio de alternativas y costes de asunción en el sector público de esta intervención para estadíos categóricamente planteados. Esto implicaría la planificación del número de unidades a georeferenciar para la Comunidad (una por provincia, una central...) y adecuar recursos para las mismas de forma que la repercusión de esta alternativa no lastrase la actividad que ya se realiza en dichos servicios de oftalmología (retinopatía diabética, cataratas ...). (La opción de asumir de forma reglada este tipo de intervención en el sector público posibilitaría que mediante negociación global con la/s empresa/s proveedoras del fármaco se pudiera optimizar en grado sumo la adquisición o cesión del aparataje. A su vez, la compra centralizada del fármaco para uso hospitalario podría permitir una rebaja substancial en el precio unitario). 4.- Estudio de la alternativas de asunción mediante externalización (concertada o no) y estimación de costes. En este caso sería preciso el mejor aquilatamiento de los precios, estableciéndolos bien por sesión o bien por proceso global. (Una estimación de escenarios se ofrece en las tablas subs¡guientes: apéndice F). 5.- En cualquiera de los escenarios de asunción de esta terapia con cargo al erario público, habría que sopesar y estimar mecanismos que solventasen la posible llegada de pacientes de otros servicios autonómicos de salud o del INSALUD en caso de que la terapia (bien con proveedor público o privado) sólo fuera asumida en la Comunidad Valenciana. Por otro lado no se tiene Pá gina 11 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 hasta la fecha información de reintegros o sentencias judiciales que dicten la asunción del coste de este tratamiento por las arcas públicas (única terapia considerada viable por los oftalmólogos para cierto tipo de pacientes). La posibilidad en un futuro próximo de este tipo de circunstancias, sin duda debería ser tenida en cuenta de cara a los análisis económicos que convendría realizar. Valencia 1 de marzo del año 2001 Servicio de Evaluación de Tecnologías Pá gina 12 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 APÉNDICE A Criterios de indicación La terapia de la DMAE mediante terapia fotodinámica con Verteporfin podrá indicarse a criterio del especialista oftalmólogo bajo las siguientes condiciones: - El diagnóstico de DMAE con NVC (neovascularización coroidal) retrofoveolar predominantemente visible (50%) debe haberse establecido de forma clara. - Se trata de una forma exudativa con lesión retrofoveolar en la que más del 50% esté constituida por nuevos vasos visibles, demostrado por angiografía de fluorescencia (completada en caso de necesidad con la angiografía con verde de indocianina) (un cliché de angiografía debe poder ser consultado). - Debe respetarse un intervalo de noventa días entre dos sesiones de tratamiento. Criterios de no indicación Las formas predominantemente visibles son las menos frecuentes de las DMAE exudativas retrofoveolares. La terapia de la DMAE mediante terapia fotodinámica con Verteporfin® no está indicada en el tratamiento: - de las NVC ocultas; - de la DMAE con NVC visibles respetando la mácula (extra o yuxta foveolares) susceptibles de un tratamiento por fotocoagulación láser convencional; - de las NVC secundarias a una fuerte miopía para las cuales el beneficio terapéutico de Verteporfin® está todavía en evaluación Otras indicaciones sólo deberían establecerse en el marco de ensayos clínicos, debidamente protocolorizados y autorizados. Para étos es preciso asegurar las condiciones metodológicas, éticas y legales para su puesta en marcha. Pá gina 13 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 APÉNDICE B Procedimientos e instrumentación Para esta terapia, el oftalmólogo debe de haber realizado los siguientes exámenes en los 7 días anteriores: - medida de la agudeza visual, completada eventualmente con la medida de sensibilidad a los contrastes - angiografía con fluoresceína, comportando clichés a 1, 2, 5 y 10 minutos, eventualmente completada con angiografía con verde de indocianina - fotografía del fondo de ojo (equipo con agrandamiento recomendado de 2,4-2,6). La mayor dimensión de la lesión coroidiana se estimará sobre angiografía y la fotografía del fondo de ojo. Equipo necesario: • angiografo de fluoresceína y si es necesario la posibilidad de realizar una angiografía con verde de indocianina • jeringa eléctrica • láser diodo (longitud de onda: 689 nm), Las contraindicaciones y reservas respecto a la manipulación, reconstitución del Verteprofin, protección a la luz, tiempo de activación, área de incidencia y actuación lumínica, y protecciones lumínicas postintervención en tiempo y forma, deben ser respetadas. El riesgo de interacción con medicamentos u otros agentes fotosensibilizantes debe ser investigado. Modo de administración y reintervención El tratamiento comprende dos etapas: 1. Perfusión intravenosa de Verteporfin® durante 10 minutos con una dosis de 6mg/m2 de superficie corporal, diluido en 30 ml. de solución glucosada. 2. Activación de Verteporfin® por la luz 15 minutos después del inicio de la perfusión por medio de una luz roja no térmica (longitud de onda: 689 nm), proporcionada por un laser diodo con ayuda de una fibra óptica, de una lámpara de hendidura y de una lentilla de contacto apropiada. Para la intensidad luminosa recomendada (600 mW/cm2), son necesarios 83 segundos para proporcionar la dosis luminosa requerida de 50 julios/cm2. Los pacientes deben ser reevaluados cada tres meses. En caso de recidiva, el tratamiento por Verteporfin® puede ser administrado hasta cuatro veces por año. Pá gina 14 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 APÉNDICE C Guía de conocimientos clínicos La indicación de la terapia fotodinámica es muy precisa en la DMAE: los pacientes que presentan una neovascularización coroidiana retrofoveolar predominantemente visible. En esta indicación, la eficacia de Verteporfin® sólo ha sido demostrada en los pacientes en los que la agudeza visual estaba comprendida entre 1/10 y 5/10. Los pacientes deben ser reevaluados cada tres meses en caso de recidiva, el tratamiento por Verteporfin® debe ser administrado un máximo de cuatro veces por año. El Verteporfin® es un derivado de una benzoporfirina (BDP-MA) cuyas propiedades fotosensibilizantes son utilizadas para limitar la pérdida de la agudeza visual ligada a la degeneración macular asociada a la edad (DMAE) en su forma exudativa, en los pacientes que presentan una neovascularización coroidiana retrofoveolar predominantemente visible (50% de nuevos vasos bien delimitados en la angiografía con fluoresceina). Esta forma de DMAE es una patología con mal pronóstico que conduce en un breve plazo a un déficit visual mayor. La fototerapia dinámica con Verteporfin® es una alternativa terapéutica cuyo interés reside en que respeta el tejido retiniano macular. La prescripción debe ser únicamente realizada por especialistas en oftalmología. El coste particularmente elevado de Verteporfin® y el riesgo de una utilización para indicaciones no validadas o justificadas, teniendo en cuenta otras alternativas terapéuticas, hacen que la utilización del mismo en la terapia fotodinámica sea sometido al mayor control posible y a asegurar la idoneidad de los casos a ser tratados y que por tanto puedan beneficiarse del citado tratamiento. Contraindicaciones del Verteporfin: - pacientes afectos de porfiria; pacientes que presenten una insuficiencia hepática grave; hipersensibilidad al verteporfin o a alguno de sus excipientes Reservas y precauciones de empleo: - en ausencia de estudios apropiados, Verteporfin® debe ser utilizado con precaución en los pacientes afectos de insuficiencia hepática moderada o de obstrucción de las vías biliares - no se dispone de ninguna experiencia clínica en los pacientes que sufren de insuficiencia cardíaca no controlada (clases III y IV) ni en los afectos de HTA no controlada - en ausencia de datos clínicos y farmacológicos, conviene ser prudente al considerar un tratamiento con Verteporfin® bajo anestesia general - Verteporfin® no ha sido estudiado en la mujer embarazada o mujer que amamante Después de tratamiento por Verteporfin®, los pacientes pueden desarrollar molestias visuales como visión anormal, disminución de la agudeza visual, alteración del campo visual. Mientras persistan las molestias los pacientes a los que su agudeza visual les permite habitualmente conducir, no deben hacerlo ni utilizar máquinas. Pá gina 15 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 APÉNDICE D Datos a recoger y documentar (susceptibles de mecanizar y tratar) La unidad de registro será el paciente afecto de la DMAE detectado en los servicios de oftalmología. Para cada paciente registrado se anexarán los datos referentes a las valoraciones periódicas efectuadas, así como de las intervenciones oftalmológicas realizadas, indicando para cada uno de los datos la fecha de acopio real de la información. Una serie de datos socio-epidemiológicos deberán consignarse para cada paciente. A fin de permitir el seguimiento de la adecuación de este tipo de intervenciones y del resultado en el grupo de pacientes intervenidos, diversos datos deben ser recogidos en cada sesión valorativa o terapeútica en la historia clínica del paciente y tenidas a disposición de agentes evaluadores de la Conselleria de Sanidad: - afectación uni o bilateral - agudeza visual precisa del ojo (o de los dos ojos) afectados - naturaleza y extensión de las lesiones por imagen angiográfica (un cliché de angiografía debe poder ser consultado) - datos relativos a la intervención (fecha, hora y minutos de la inyección de la droga, activación del verteporfin mediante láser, tiempo de iluminación y campo) - datos del seguimiento oftalmológico del paciente Pá gina 16 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 APÉNDICE E (1) prevalencias poblacionales referidas o estimadas a partir de datos de los estudios de prevalencia/incidencia poblacional seleccionados (datos referidos salvo otra indicación expresa en porcentaje poblacional para las cohortes de edad analizadas) (agosto 2000: 2000) Australia >40 años (pob. n=5147 Victoria, examen oftalm.) (sept 1999: 1993-1995) Wisconsin 48-72 años (pob. n=11532 North Carolina, examen oftalm. graduac. Wisconsin) (sept 1999: 4 años) VECAT study 55 a 80 años (Cas-control n=1204, examen oftalm., Int.Clasif. ARM-AMD) (jun 1999) NHNES-III USA >40 años (pob. n=8270 USA, examen oftalm.) (jun 1999) Baltimore >70 años (pob n=5308 Baltimore, exam. oftalm.) (agosto 2000) Blue Mountain Eye Study (pob n=3654 Australia examen oftalm) 50-59 años (uni-bilateral) alteraciones Degenerac. maculares maculopatía macular tempranas asociada a ligada a la la edad drusas edad (>65 µm ) exudativa) 15’1 0’39 DMAE en ciegos DMAE en ciegos o con daños visuales severos 5’6 32 9’4 15 2’1 0’4 - 2’7 (agosto 2000) Blue Mountain Eye Study (pob n=3654 Australia examen oftalm) 60 – 69 años (uni-bilateral) 0’8 - 6’2 (agosto 2000) Blue Mountain Eye Study (pob n=3654 Australia examen oftalm) 70 – 79 años (uni-bilateral) 4’1 - 15’37 (agosto 2000) Blue Mountain Eye Study (pob n=3654 Australia examen oftalm) >80 años (uni-bilateral) 20’1 - 39’9 (feb 2000: final 1998) Israel >18 años (registro nacional de ceguera n=15.937) 0’36 (ciegos) (jun 2000) Salisbury 65-84 años (pob Medicare, n=2520, examen oftalm) (may 2000: 3 meses) Serv. Oftalmología Orleans (Francia) (pob asistida, n=1172, examen oftalm)<60 años (may 2000: 3 meses) Serv. Oftalmología Orleans (Francia) (pob asistida, n=1172, examen oftalm) 60-79 años (may 2000: 3 meses) Serv. Oftalmología Orleans (Francia) (pob asistida, n=1172, examen oftalm) >80 años (jun 1998) Irlanda >16 años (registro nacional de ceguera, n=5002) (agosto 1998:seguim 10 años) Depart. Oftalm. Pensilvamia >43 años (seguim cohorte, n=?, examen oftalm.) (may 1998) North London (pob médica, n=1547, Londres, examen oftal.) >65 años (may 1998) Rotterdam Study (pob, n=6775, examen oftalm.) >85 años (nov 1996) Baltimore >40 años (pob, n=5308, examen oftalm.) (abril 1995) Finlandia >70 años (pob, n=500 hab Oulu, examen oftalm.) 12 1’2 (con daños severos) 0’48 (daños severos) 2’32 (daños seeros) 5’84 (daños severos) 40 16 2’54 (con cegurera) 8 10’8 14’2 41 4’7 Pá gina 17 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 APÉNDICE E (2) prevalencias poblacionales referidas o estimadas a partir de datos de los estudios de prevalencia/incidencia poblacional seleccionados (datos referidos salvo otra indicación expresa en porcentaje poblacional para las cohortes de edad analizadas) (enero 2000) National Horizon Scanning Centre >75 años alteraciones maculaDegeneración macures tempranas lar asociada a la edad maculopatía ligada a drusas (>65 ) (DMAE exudativa) la edad 30 3 (proyecto de revisión sistemática.) 0’21 con pérdida (febrero 2000) Norwegian Centre for Health Technology Assessment >45 años (evaluación de la terapia fotodinámica: diciembre 1999 – febrero 2000) (proyección de datos del Beaver, Dam Eye Study) 20 1’2 a PDT: 0’48 (febrero 2000) Norwegian Centre for Health Technology Assessment (evaluación de la terapia fotodinámica: diciembre 1999 – febrero 2000) (proyección de datos del Beaver, Dam Eye Study) 43-54 años 0’1 (febrero 2000) Norwegian Centre for Health Technology Assessment >45 años (evaluación de la terapia fotodinámica: diciembre 1999 – febrero 2000) (proyección de datos del Beaver, Dam Eye Study) >75 años 7’5 (febrero 2000) Norwegian Centre for Health Technology Assessment >45 años (evaluación de la terapia fotodinámica: diciembre 1999 – febrero 2000) (proyección de datos del Beaver, Dam Eye Study) >85 20 (enero 1994) Dépistage de la déficience visuelle chez les personnes âgéesCanadá 55 años, (revisión sistemática y recomendaciones, 1 Ministre des Approvisionnements et Services Canada: Guide Canadien de Medicine clinique et préventive, 1994 >80 años 15 Ministre des Approvisionnements et Services Canada: Guide Canadien de Medicine clinique et préventive, 1994 64 años 35 Ministre des Approvisionnements et Services Canada: Guide Canadien de Medicine clinique et préventive, 1994 85 años 50 ESTIMACIONES PARA LA COMUNIDAD VALENCIANA PROYECTANDO ESTUDIOS RECIENTES SOBRE LA DMAE (los datos contenidos en el cuadro se refieren a número de personas) Población susceptible de intervención de más de 45 años tras examen oftalmológico Demanda expresada (no alentada) por importante pérdida visual (pacientes de más de 45 años) Población susceptible de intervención de más de 70 años tras examen oftalmológico Demenda expresada (no alentada) por importante pérdida visual (pacientes de más de 70 años) Prevalencia estimada máxima actual Incidencia estimada 8.000 pacientes 2.000 /pacientes-año 1.250 - 3.000 pacientes 400 – 1.000 /pacientes-año 4.000 pacientes 1.500 /pacientes-año 600 – 1.250 pacientes 350 – 650 /pacientes-año Pá gina 18 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 APÉNDICE F ESTIMACIÓN DE COSTES DE LOS PRODUCTOS, PROCEDIMIENTOS Y EQUIPOS INVOLUCRADOS EN LA TÉCNICA A PESETAS CONSTANTES (2001) SEGÚN LOS ESTUDIOS REFERENCIADOS BASE DEL ESTUDIO PARA LA PROYECCIÓN (Los datos se expresan en pesetas) Dosis de verteporfín Equipo láser (amortización ± 25 sesiones) REINO UNIDO NORUEGA USA 195.000 5.500.000 263.000 2.000.000 (adaptación cabezal) 262.000 Angiógrafo 7.800.000 (compartido) Otros equipos 1.500.000 (compartido) 260.000 195.000 Sesión láser Estancia y personal Sesión excepto fármaco 61.380 (reembolso Medicare) Factura actual por sesión ESTIMACIÓN VALENCIA 175.000 6.000.000 8.000.000 (5’5 M revelado diferido; 14’5 M digital) 1.000.000 (compartido) 230.000 70.000 Posibilidad de ajustar a 1.000.000 para 4 sesiones 300.000 ESCENARIOS DE COSTES PREVISTOS PARA LA ASUNCIÓN DE LA PREVALENCIA EXISTENTE Y POSTERIOR INCIDENCIA AL RITMO PREVISTO ESTIMACIÓN CON FACTURACIÓN ACTUAL (300.000 pts por sesión) COSTE ESTIMADO DE TRATAMIENTOS EN MILLONES DE PESETAS (DMAE uniocular o bilateral en la misma sesión) población diana potencial de más de 45 años Demanda expresada (no alentada) para más de 45 años población diana potencial de más de 75 años Demanda expresada (no alentada) para más de 75 años Coste primer año Coste segundo año 9.600 4.800 14.400 1.500 - 3.600 750 - 1.800 2.250 - 5.400 4.800 2.400 7.200 720 - 1.500 360 - 750 1.080 - 2.250 Coste primer año Coste segundo año 8.000 4.000 12.000 1.250 – 3.000 625 – 1.500 1.875 – 4.500 4.000 2.000 6.000 600 – 1.250 300 -625 900 – 1.875 Facturación total ESTIMACIÓN CON FACTURACIÓN AJUSTADA COSTE ESTIMADO DE TRATAMIENTOS EN MILLONES DE PESETAS (DMAE uniocular o bilateral en la misma sesión) población diana potencial de más de 45 años Demanda expresada (no alentada) para más de 45 años población diana potencial de más de 75 años Demanda expresada (no alentada) para más de 75 años Facturación total Pá gina 19 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 ANEXOS Relación de anexos: 1.- febrero 2001. ANEXO DOCUMENTAL DE EXPLOTACIÓN DE DATOS DE CONCIERTOS ........................................................ 21 2.- febrero 2001. ANEXO DOCUMENTAL DE LA BÚSQUEDA BIBLIOGRÁFICA EN LA CDR (en sus bases de datos DARE, NHS EED y HTA) ................................................................... 29 3.- febrero 2001. ANEXO DOCUMENTAL DE LA BÚSQUEDA BIBLIOGRÁFICA EN MEDLINE A TRAVÉS DE LA NATIONAL LIBRARY OF MEDICINE (bajo criterios: “photodynamic therapy degeneration macular”) ..................................................... 31 4.- febrero 2001. ANEXO DOCUMENTAL DE LA BÚSQUEDA BIBLIOGRÁFICA EN MEDLINE A TRAVÉS DE LA NATIONAL LIBRARY OF MEDICINE (bajo criterios: “prevalence blindness older” or “epidemiology maculopathy” or “prevalence aged macular”) ............................................................................ 36 5.- marzo 2000. SMM-REPORT NR.3/2000 THE NORWEGIAN CENTRE FOR HEALTH TECHNOLOGY ASSESSMENT Photodynamic therapy for age-related macular degeneration.................. 57 6.- 1.994: GUIDE CANADIEN DE MEDICINE CLINIQUE ET PRÉVENTIVE. Dépistage de la deficience visuelle chez les personnes âgées ....................................................................... 68 7.- enero 2000. NATIONAL HORIZON SCANNING CENTRE. Photodynamic therapy for age-related macular degeneration. ............. 83 8.- Issue 1, 2001. Oxford. THE COCHRANE LIBRARY (COCHRANE REVIEW). Photodynamic therapy for neovascular age-related macular degeneration. ........................................................... 90 9.- enero 2001. Irveng Arons in OCULAR SURGERY NEWS. Visudyne looks promising for treating wet AMD ..............................108 10.- Información registrada en la FDA sobre el verteporfin ...............113 11.- Información registrada en la EMEA sobre el verteporfin .............126 Pá gina 20 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 ANEXO 1 Pá gina 21 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 ANEXO DOCUMENTAL DE EXPLOTACIÓN DE DATOS DE CONCIERTOS CENTRO ORIGEN DE PROPUESTA H. LA RIBERA H. GENERAL DE VALENCI H. ARNAU DE VILANOVA H. GENERAL DE ELDA H. FRANCESC DE BORJA H. LLUIS ALCANYIS H. LA FE H. CLINICO UNIVERSITA C.E. JUAN LLORENS H. GENERAL DE CASTELL H. DE ONTINYENT H. DR. PESET H. SAN JUAN DE ALICAN H. VIRGEN LIRIOS H. DE SAGUNT C.E. MONTEOLIVETE H. DE REQUENA H. MARINA ALTA DE DEN H. DE SAGUNTO H. VALENCIA AL MAR ESCA-VALENCIA AREA 7 H. MARINA BAJA H. GENERAL DE ALICANT Total Frecuencia porcentaje 30 23 23 18 15 12 10 10 7 6 5 5 5 4 3 3 3 2 2 1 1 1 1 15.8 12.1 12.1 9.5 7.9 6.3 5.3 5.3 3.7 3.2 2.6 2.6 2.6 2.1 1.6 1.6 1.6 1.1 1.1 .5 .5 .5 .5 190 100.0 Porcentaje acumulado 15.8 27.9 40.0 49.5 57.4 63.7 68.9 74.2 77.9 81.1 83.7 86.3 88.9 91.1 92.6 94.2 95.8 96.8 97.9 98.4 98.9 99.5 100.0 Pá gina 22 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 CENTRO DESTINO Frecuencia porcentaje CLINICA VIRGEN DEL CONSUELO NO CONSIGNADO INSTITUTO ALIO INSTITUTO OFTALMOLOGICO DE ALICANTE CERE INSTITUTO MICROCIRUGIA OCULAR 137 45 3 72.1 23.7 1.6 Porcentaje acumulado 72.1 95.8 97.4 3 1.6 98.9 1 1 .5 .5 99.5 100.0 Total 190 100.0 ESTIMACION POR CONCIERTOS Porcentaje Frecuencia porcentaje acumulado SI ACEPTADO 110 57.9 57.9 NO ACEPTADO 80 42.1 100.0 Total 190 100.0 AÑO Y MES DE ESTIMACIÓN Frecuencia porcentaje Porcentaje acumulado 2000-01 2000-02 2000-03 2000-04 2000-05 2000-06 2000-07 2000-08 2000-09 2000-10 2000-11 2000-12 2001-01 2001-02 10 11 17 16 20 17 31 38 14 2 3 2 7 2 5.3 5.8 8.9 8.4 10.5 8.9 16.3 20.0 7.4 1.1 1.6 1.1 3.7 1.1 5.3 11.1 20.0 28.4 38.9 47.9 64.2 84.2 91.6 92.6 94.2 95.3 98.9 100.0 Total 190 100.0 MESGRUPO de VII-2000 hasta hoy de inicio 2000 a VI-2000 Total Frecuencia porcentaje 99 91 52.1 47.9 190 100.0 Porcentaje acumulado 52.1 100.0 Pá gina 23 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 24 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 25 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 26 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 ESTIMACION POR CONCIERTOS / tiempo de resolución (tiempo de resolución dicotomizado:: hasta junio-2000, desde julio 2000) MESGRUPO de inicio 2000 a VI-2000 ESTIMACION POR CONCIERTOS NO ACEPTADO SI ACEPTADO Total Recuento % de ESTIMACION POR CONCIERTOS % de MESGRUPO Recuento % de ESTIMACION POR CONCIERTOS % de MESGRUPO Recuento % de ESTIMACION POR CONCIERTOS % de MESGRUPO Total de VII2000 hasta febrero 2001 22 58 80 27.5% 72.5% 100.0% 24.2% 69 58.6% 41 42.1% 110 62.7% 37.3% 100.0% 75.8% 91 41.4% 99 57.9% 190 47.9% 52.1% 100.0% 100.0% 100.0% 100.0% Prueba de chi-cuadrado significativa para p<0’0001 Pá gina 27 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 28 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 ANEXO 2 Pá gina 29 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 ANEXO DOCUMENTAL DE LA BÚSQUEDA BIBLIOGRÁFICA EN LA CDR (en sus bases de datos DARE, NHS EED y HTA) CONSTRUCTO DEL SONDEO: criterios no restrictivos para cualquier campo: “photodynamic Y therapy” RESULTADO: 11 referencias TÍTULO ORIGEN Photodynamic therapy - Summary. Canadian Coordinating Office for Health Technology Assessment (CCOHTA) 1994. Photodynamic therapy for skin and mucosal can- Medicare Services Advisory Committee (MSAC) cer. 1999 (MSAC application 1008: Final Assessment Report): pp.16. Photodynamic therapy in gastroenterology and Comite de Evaluation et de Diffusion des InnovaENT (systematic review, expert panel). tions Technologiques (CEDIT) 1999. Photodynamic therapy for neovascular age- Wormald R, Evans J, Smeeth L. Wormald R, Evrelated macular degeneration. ans J, Smeeth L. Photodynamic therapy for neovascular age-related macular degeneration. (Cochrane Review). In: The Cochrane Library, Issue 4, 2000. Oxford: Update Software.. Multi-drug versus single agent chemotherapy for Huncharek M, Muscat J, Geschwind J F. Anticanhigh grade astrocytoma; results of a metacer Research 1998; 18(6B): 4693-4697. analysis. A systematic review of treatment modalities for Thissen M R, Neumann M H, Schouten L J. Arprimary basal cell carcinomas. chives of Dermatology 1999; 135(10): 1177-1183. Photodynamic therapy for age-related macular Seland JH, Bragadottir R, Hedels C, Syrdalen P, degeneration. Holm S, Kjonniksen I. The Norwegian Centre for Health Technology Assessment (SMM) 2000. (SMM-Report 3/2000). Photofrin(R) and photodynamic therapy of cancer Agence d'Evaluation des Technologies et des - systematic review (project). Modes d'Intervention en Sante (AETMIS). Photodynamic therapy of aged-related nuclear Danish Institute for Health Technology Assessdegeneration (funded by DIHTA) - systematic rement (DIHTA). view (project). Photodynamic therapy (project). Medicare Services Advisory Committee (MSAC). Photodynamic therapy for treatment of ageNational Horizon Scanning Centre (NHSC). related macular degeneration - horizon scanning review (project). En gris: referencias electas Pá gina 30 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 ANEXO 3 Pá gina 31 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 ANEXO DOCUMENTAL DE LA BÚSQUEDA BIBLIOGRÁFICA EN LA NATIONAL LIBRARY OF MEDICINE (a través de NLM el 15-II-2001 bajo criterios: “photodynamic therapy degeneration macular”) CONSTRUCTO DEL SONDEO: (("photochemotherapy"[TÉRMINOS MeSH] O photodynamic therapy[Texto]) Y ("macular degeneration"[TÉRMINOS MeSH] O degeneration macular[Texto])) RESULTADO: 31 referencias TÍTULO DEL ARTÍCULO ORIGEN Extracts from "clinical evidence": age re- Aberdeen Royal Hospilated macular degeneration. tals NHS Trust, Aberdeen. [email protected] AUTORES Arnold JJ; Sarks SH; Photodynamic therapy with verteporfin (Visudyne) for macular degeneration. IDIOMA REFERENCIA DE REVISTA eng BMJ 2000 Sep 23;321(7263):741-4. eng Med Lett Drugs Ther 2000 Sep 4;42(1086):81-2. Update on photodynamic therapy. Wills Eye Hospital, Philadelphia, Pennsylvania 19107, USA. Regillo CD; eng Curr Opin Ophthalmol 2000 Jun;11(3):166-70. Ophthalmology update for the primary practitioner. Part II. Therapeutic management of age-related macular degeneration. William Beaumont Hospital, Royal Oak, Michigan, USA. Sarrafizadeh R; Trese MT; eng Dis Mon 2000 Aug;46(8):533-43. No efficacious treatment for age-related macular degeneration. Department of Ophthalmology, Algemeen Ziekenhuis Sint-Jozef, Turnhout, Belgium. Roodhooft J; eng Bull Soc Belge Ophtalmol 2000;276(8):83-92. Potocky M; Trnavec B; slo Bratisl Lek Listy 2000;101(4):231-3. eng Mayo Clin Health Lett 2000 Feb;18(2):4. [Etiopathogenesis of age-related macular degeneration and present possibilities of treatment] New treatment for macular degeneration being tested. Age-related macular degeneration: update for primary care. Southern California Permanente Medical Group, Baldwin Park, California, USA. Fong DS; eng Am Fam Physician 2000 May 15;61(10):3035-42. Photodynamic therapy for neovascular 'Glaxo' Department of age-related macular degeneration. Ophthalmic Epidemiology, Institute of Ophthalmology (UCL) and Moorfields Eye Hospital, City Road, London, UK, EC1V 2PD. Wormald R; Evans J; Smeeth L; eng Cochrane Database Syst Rev 2000;61(2):CD002030. Indocyanine green angiography and retinal University Eye Hospital sensitivity after photodynamic therapy of Luebeck, Medical Unisubfoveal choroidal neovascularization. versity, Luebeck, Germany. SchmidtErfurth U; eng Semin Ophthalmol 1999 Mar;14(1):3544. Department of Clinical Donati G; KaNeurosciences, Uni- petanios AD; versity Hospitals of Pournaras CJ; Geneva, Geneva, Switzerland. eng Semin Ophthalmol 1999 Mar;14(1):210. ger Ophthalmologe 2000 Feb;97(2):154-6. Principles of treatment of choroidal neovascularization with photodynamic therapy in age-related macular degeneration. [Vitreoretinal Update Meeting 1999. Conference of the American Academy of Ophthalmology, Orlando, Florida, 2223/10/1999] UniversitatsAugenklinik, Mainz. Augustin AJ; Pá gina 32 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TÍTULO DEL ARTÍCULO ORIGEN Texaphyrins: new drugs with diverse clini- Department of Chemiscal applications in radiation and photodytry & Biochemistry, namic therapy. University of Texas, Austin 78712, USA. [email protected] REF.: ACEMSA/SET/AC/ac febrero-2001 AUTORES IDIOMA REFERENCIA DE REVISTA Sessler JL; Miller RA; eng Biochem Pharmacol 2000 Apr 1;59(7):733-9. Photodynamic therapy with verteporfin (Visudyne): impact on ophthalmology and visual sciences. Retinal Vascular Center, Wilmer Ophthalmological Institute, Johns Hopkins University School of Medicine, Baltimore, Maryland 21205-2010, USA. Bressler NM; Bressler SB; eng Invest Ophthalmol Vis Sci 2000 Mar;41(3):624-8. Age-related macular degeneration. Department of Ophthalmology, Scheie Eye Institute, University of Pennsylvania Health System, Philadelphia 19104-2689, USA. Fine SL; Berger JW; Maguire MG; Ho AC; eng N Engl J Med 2000 Feb 17;342(7):483-92. [Confocal indocyanine green angiography Augenklinik Universitat Schmidtwith 3-dimensional topography. Results in Lubeck. Erfurth U; choroid neovascularization (CNV)] Noack J; Teschner S; Birngruber R; ger Ophthalmologe 1999 Dec;96(12):797804. Help for macular degeneration. McDonald HR; eng Health News 1999 Dec 15;5(15):1-2. Vision researchers seek to be armed against damaging ARMD. Age-related macular degeneration. Voelker R; eng JAMA 1999 Nov 10;282(18):1711-2. [Present and future treatment of agerelated macular degeneration] Centres Hospitaliers Verougstraete Universitaires BrugC; mann et Saint-Pierre, Bruxelles. fre Bull Soc Belge Ophtalmol 1999;273(18):79-101. Photodynamic therapy: a new approach to the treatment of choroidal neovascularization secondary to age-related macular degeneration. Glaser-Murphy Retina Wu L; Murphy Treatment Center, RP; Chevy Chase, Maryland 20815, USA. eng Curr Opin Ophthalmol 1999 Jun;10(3):217-20. Photodynamic therapy with verteporfin is effective for selected patients with neovascular age-related macular degeneration. Fine SL; eng Arch Ophthalmol 1999 Oct;117(10):1400-2. eng Arch Ophthalmol 1999 Oct;117(10):1329-45. Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin: one-year results of 2 randomized clinical trials--TAP report. Treatment of agerelated macular degeneration with photodynamic therapy Pá gina 33 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TÍTULO DEL ARTÍCULO ORIGEN REF.: ACEMSA/SET/AC/ac febrero-2001 AUTORES IDIOMA REFERENCIA DE REVISTA Photodynamic therapy with verteporfin for choroidal neovascularization caused by age-related macular degeneration: results of retreatments in a phase 1 and 2 study. Retina Department, SchmidtUniversity Eye HospiErfurth U; tal, Lubeck, Germany. Miller JW; Sicuschmidterkenberg M; [email protected] Laqua H; Barluebeck.de bazetto I; Gragoudas ES; Zografos L; Piguet B; Pournaras CJ; Donati G; Lane AM; Birngruber R; van den Berg H; Strong HA; Manjuris U; Gray T; Fsadni M; Bressler NM; eng Arch Ophthalmol 1999 Sep;117(9):1177-87. Photodynamic therapy with verteporfin for choroidal neovascularization caused by age-related macular degeneration: results of a single treatment in a phase 1 and 2 study. Retina Service, MasMiller JW; sachusetts Eye and SchmidtEar Infirmary, Harvard Erfurth U; SicMedical School, Boskenberg M; ton, USA. jwmil- Pournaras CJ; [email protected] Laqua H; Barbazetto I; Zografos L; Piguet B; Donati G; Lane AM; Birngruber R; van den Berg H; Strong A; Manjuris U; Gray T; Fsadni M; Bressler NM; Gragoudas ES; eng Arch Ophthalmol 1999 Sep;117(9):1161-73. SchmidtErfurth U; ger Klin Monatsbl Augenheilkd 1998 Dec;213(6):aA11-5. Department of Clinical Chong NH; BiOphthalmology, Instird AC; tute of Ophthalmology (UCL), Moorfields Eye Hospital, London. eng Br J Ophthalmol 1998 Dec;82(12):1441-3. Age-related macular degeneration: a re- Indiana University Ma- Ciulla TA; Daview of experimental treatments. cular Degeneration Cli- nis RP; Harris nic and Research CenA; ter, Department of Ophthalmology, Indiana University School of Medicine, eng Surv Ophthalmol 1998 SepOct;43(2):134-46. [Photodynamic therapy--a conservative al- Augenklinik, Medizinisternative in treatment of exudative macular che Universitat Lubeck. degeneration] Alternative therapies in exudative age related macular degeneration. [Use of complex compression diagnostic test for defining the indications for surgical treatment of atherosclerotic chorioretinal dystrophy] Basinskii SN; Krasnogorskaia VN; Solomina EV; rus Vestn Oftalmol 1998 JanFeb;114(1):36-8. [New method of atherosclerotic macular dystrophies treatment] Basinskii SN; Krasnogorskaia VN; rus Vestn Oftalmol 1997 NovDec;113(6):17-9. Solberg Y; Belkin M; heb Harefuah 1997 Oct 2;133(7-8):268-72, 335. [Advances in ophthalmological photodynamic therapy] Goldschleger Eye Research Institute, Tel Aviv University. Pá gina 34 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TÍTULO DEL ARTÍCULO ORIGEN Photosensitizers in photodynamic therapy. Quadra Logic Technologies, Inc, Vancouver, British Columbia, Canada. REF.: ACEMSA/SET/AC/ac febrero-2001 AUTORES Levy JG; IDIOMA eng REFERENCIA DE REVISTA Semin Oncol 1994 Dec;21(6 Suppl 15):4-10. Pá gina 35 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 ANEXO 4 Pá gina 36 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 ANEXO DOCUMENTAL DE LA BÚSQUEDA BIBLIOGRÁFICA EN LA NATIONAL LIBRARY OF MEDICINE (a través de NLM el 22-II-2001 bajo criterios: “prevalence blindness older” or “epidemiology maculopathy” or “prevalence aged macular”) CONSTRUCTO DEL SONDEO: CRITERIO A: (((((("epidemiology"[Subheading] OR "prevalence"[MeSH Terms]) OR "epidemiology"[MeSH Terms]) OR "Prevalence"[MeSH Terms]) OR PREVALENCE[Text Word]) AND ("blindness"[MeSH Terms] OR BLINDNESS[Text Word])) AND OLDER[All Fields]) CRITERIO B: ((("epidemiology"[Subheading] OR "epidemiology"[MeSH Terms]) OR EPIDEMIOLOGY[Text Word]) AND MACULOPATHY[All Fields]) CRITERIO C: (((((("epidemiology"[Subheading] OR "prevalence"[MeSH Terms]) OR "epidemiology"[MeSH Terms]) OR "Prevalence"[MeSH Terms]) OR prevalence[Text Word]) AND ("aged"[MeSH Terms] OR aged[Text Word])) AND macular[All Fields]) RESULTADO: 126 referencias para A; 128 referencias para B; 471 para C 224 referencias electas para su lectura, cotejo y análisis: CRITERIO A CRITERIO B CRITERIO C CRITERIO A CRITERIO B CRITERIO C 6 1 12 TITULO 1 5 14 ORIGEN 12 14 186 AUTORES IDIOMA TOTAL CRITERIOS 19 20 215 REVISTA CRIT. Visual acuity in a population aged 70 Department of Oph- Hirvela H; Layears or older; prevalence and causes thalmology, University atikainen L; of visual impairment. of Oulu, Finland. eng Acta Ophthalmol Scand 1995 Apr;73(2):99-104. A Knowledge and beliefs about common Department of Opheye diseases. thalmology and Public Health, University of Sydney, New South Wales, Australia. Attebo K; Mitchell P; Cumming R; Smith W; eng Aust N Z J Ophthalmol 1997 Nov;25(4):283-7. A Dana Center for Preventive Ophthalmology, Johns Hopkins School of Medicine, Baltimore, MD 212879019, USA. [email protected] West SK; eng Epidemiol Rev 2000;22(1):64-70. A Visual impairment in nursing home Department of Ophresidents: the Blue Mountains Eye thalmology, University Study. of Sydney, NSW. [email protected] u Mitchell P; Hayes P; Wang JJ; eng Med J Aust 1997 Jan 20;166(2):73-6. A Looking forward to 20/20: a focus on the epidemiology of eye diseases. Pá gina 37 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TITULO ORIGEN Functional blindness and visual imEpidemiology, Depairment in older adults from three mography and Biomecommunities. try Program, National Institute on Aging, National Institutes of Health, Bethesda 20892. AUTORES REF.: ACEMSA/SET/AC/ac febrero-2001 IDIOMA REVISTA CRIT. Salive ME; Guralnik J; Christen W; Glynn RJ; Colsher P; Ostfeld AM; eng Ophthalmology 1992 Dec;99(12):1840-7. A Canavan YM; Jackson AJ; Stewart A; eng Ulster Med J 1997 Nov;66(2):92-5. A Department of Oph- Wang JJ; Fothalmology, the Uni- ran S; Mitchell versity of Sydney, P; New South Wales, Australia. eng Clin Experiment Ophthalmol 2000 Aug;28(4):268-73. AB Prevalence and visual consequences Department of Oph- Laatikainen L; of macular changes in a population thalmology, University Hirvela H; aged 70 years and older. of Oulu, Finland. eng Acta Ophthalmol Scand 1995 Apr;73(2):105-10. AC A model of the incidence and conseScheie Eye Institute, quences of choroidal neovascularizaDepartment of Ophtion secondary to age-related macular thalmology, University degeneration. Comparative effects of of Pennsylvania current treatment and potential pro- Health System, Philaphylaxis on visual outcomes in highdelphia, USA. risk patients. Lanchoney DM; Maguire MG; Fine SL; eng Arch Ophthalmol 1998 Aug;116(8):1045-52. AC Age-specific prevalence and causes of Department of EpideKlaver CC; blindness and visual impairment in an miology and BiostatisWolfs RC; older population: the Rotterdam Study. tics, Erasmus Univer- Vingerling JR; sity Medical School, Hofman A; de Rotterdam, The NethJong PT; erlands. eng Arch Ophthalmol 1998 May;116(5):653-8. AC Causes of blindness and visual im- Wilmer Eye Institute, pairment in a population of older The Johns Hopkins Americans: The Salisbury Eye Evalua- University, 600 N Woltion Study. fe St, Room 116, Baltimore, MD 21287, USA. [email protected] Munoz B; West SK; Rubin GS; Schein OD; Quigley HA; Bressler SB; BandeenRoche K; eng Arch Ophthalmol 2000 Jun;118(6):819-25. AC Prevalence of serious eye disease and Southampton General visual impairment in a north London Hospital, Southamppopulation: population based, cross ton SO16 6YD. sectional study. Reidy A; Minassian DC; Vafidis G; Joseph J; Farrow S; Wu J; Desai P; Connolly A; eng BMJ 1998 May 30;316(7145):1643-6. AC Munier A; Gunning T; Kenny D; O'Keefe M; eng Br J Ophthalmol 1998 Jun;82(6):6303. AC Dept. of Ophthalmol- Hod Y; Corcia ogy, Carmel Medical Y; Yassur Y; Center Haifa. Geyer O; heb Harefuah 2000 Feb 15;138(4):276-8, 342. AC [Evaluation of moderate and severe Centre Hospitalier Cohen D; Sarvisual impairments in patients attendRegional d'Orleans, tral M; Nounou ing an ophthalmology clinic. A pros- Service d'Ophtalmolo- P; Hamar M; pective study of 1,172 patients] gie, BP 2439, 45032 Drouard ME; Orleans Cedex 1. El Alamy A; Bendeddouche K; fre J Fr Ophtalmol 2000 May;23(5):43743. AC Visual impairment in Northern Ireland. Age-specific prevalence and causes of bilateral and unilateral visual impairment in older Australians: the Blue Mountains Eye Study. Causes of blindness in the adult population of the Republic of Ireland. [Causes of blindness in Israel] Department of Opthalmology, Royal Victoria Hospital, Belfast. National Council for the Blind of Ireland, Dublin, Ireland. Pá gina 38 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TITULO ORIGEN AUTORES REF.: ACEMSA/SET/AC/ac febrero-2001 IDIOMA REVISTA CRIT. The prevalence of blindness and vis- Department of InternaTielsch JM; ual impairment among nursing home tional Health, Johns Javitt JC; Coresidents in Baltimore. Hopkins University leman A; Katz School of Hygiene and J; Sommer A; Public Health, Baltimore, MD 212052103, USA. eng N Engl J Med 1995 May 4;332(18):1205-9. AC Visual acuity and the causes of visual Department of Oph- Attebo K; Mitloss in Australia. The Blue Mountains thalmology, University chell P; Smith Eye Study. of Sydney, Australia. W; eng Ophthalmology 1996 Mar;103(3):35764. AC The cause-specific prevalence of visual impairment in an urban population. The Baltimore Eye Survey. Dana Center for Preventive Ophthalmology, Johns Hopkins University School of Medicine, Baltimore, USA. Rahmani B; Tielsch JM; Katz J; Gottsch J; Quigley H; Javitt J; Sommer A; eng Ophthalmology 1996 Nov;103(11):1721-6. AC Age-related macular degeneration. Department of Ophthalmology, University of Birmingham, UK. O'Shea JG; eng Postgrad Med J 1998 Apr;74(870):203-7. AC Relationship of ocular factors to the incidence of age-related maculopathy. LeClaire JE; eng Arch Ophthalmol 1998 Oct;116(10):1404-5. B Cataract and age-related maculopathy: the Blue Mountains Eye Study. University of Sydney, Wang JJ; MitDepartment of Ophchell PG; thalmology, Sydney, Cumming RG; Australia. Lim R; eng Ophthalmic Epidemiol 1999 Dec;6(4):317-26. B Exposure to diagnostic x-rays and inDepartment of Ophcident age-related eye disease. thalmology and Visual Sciences, University of Wisconsin Medical School, Madison, Wisconsin 537052397, USA. Klein BE; Klein RE; Moss SE; eng Ophthalmic Epidemiol 2000 Mar;7(1):61-5. B Iris color, skin sun sensitivity, and ageDepartment of Ophrelated maculopathy. The Blue Moun- thalmology, University tains Eye Study. of Sydney, Westmead Hospital, Australia. Mitchell P; Smith W; Wang JJ; eng Ophthalmology 1998 Aug;105(8):1359-63. B The prevalence of age-related macuDepartment of Ophlopathy by geographic region and eth- thalmology and Visual nicity. Sciences, University of Wisconsin-Madison, 53705-2397, USA. Klein R; Klein BE; Cruickshanks KJ; eng Prog Retin Eye Res 1999 May;18(3):371-89. B Associations between antioxidant and Department of Ophzinc intake and the 5-year incidence of thalmology and Visual early age-related maculopathy in the Sciences, University Beaver Dam Eye Study. of Wisconsin Medical School, Madison, USA. VandenLangenberg GM; MaresPerlman JA; Klein R; Klein BE; Brady WE; Palta M; eng Am J Epidemiol 1998 Jul 15;148(2):204-14. BC Is age-related maculopathy associated Department of Epide- Klaver CC; Ott with Alzheimer's Disease? The Rot- miology and Biostatis- A; Hofman A; terdam Study. tics, Erasmus UniverAssink JJ; sity Medical School, Breteler MM; Rotterdam, The Nethde Jong PT; erlands. eng Am J Epidemiol 1999 Nov 1;150(9):963-8. BC Reproductive exposures, incident ageDepartment of Ophrelated cataracts, and age-related ma- thalmology and Visual culopathy in women: the beaver dam Sciences, University eye study. of Wisconsin Medical School, Madison, Wisconsin 537052397, USA. eng Am J Ophthalmol 2000 Sep;130(3):322-6. BC Klein BE; Klein R; Lee KE; Pá gina 39 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TITULO ORIGEN AUTORES REF.: ACEMSA/SET/AC/ac febrero-2001 IDIOMA REVISTA CRIT. Genetic risk of age-related maculopa- Department of EpideKlaver CC; thy. Population-based familial aggre- miology and Biostatis- Wolfs RC; Asgation study. tics, Erasmus Universink JJ; van sity Medical School, Duijn CM; Rotterdam, The Neth- Hofman A; de erlands. Jong PT; eng Arch Ophthalmol 1998 Dec;116(12):1646-51. BC Prevalence of age-related maculopaDepartment of Oph- Klein R; Clegg thy in the Atherosclerosis Risk in thalmology and Visual L; Cooper LS; Communities Study. Sciences, University Hubbard LD; of Wisconsin Medical Klein BE; King School, Madison, WN; Folsom USA. AR; [email protected]. edu eng Arch Ophthalmol 1999 Sep;117(9):1203-10. BC Family history and age-related maculopathy: the Blue Mountains Eye Study. National Centre for Epidemiology and Population Health, Australian National University, Canberra, Australian Capital Territory. Smith W; Mitchell P; eng Aust N Z J Ophthalmol 1998 Aug;26(3):203-6. BC Diabetes, fasting blood glucose and Department of Ophage-related maculopathy: The Blue thalmology, University Mountains Eye Study. of Sydney, New South Wales, Australia. [email protected] du.au Mitchell P; Wang JJ; eng Aust N Z J Ophthalmol 1999 JunAug;27(3-4):197-9. BC Department of Oph- Wang JJ; Mitthalmology, the Uni- chell P; Smith versity of Sydney, W; Westmead, NSW, Australia. eng Invest Ophthalmol Vis Sci 1998 Oct;39(11):2167-71. BC Hall N; Sayer AA; Evans J; Rauf A; Cooper C; Wormald R; eng Ophthalmic Epidemiol 1998 Jun;5(2):83-90. BC The VECAT study: methodology and statistical power for measurement of age-related macular features. Vitamin E, Cataract, and Age-related Maculopathy Study. Monash University Tikellis G; Department of Epide- Robman LD; miology & Preventive Harper CA; Medicine Caulfield, Garrett SK; Australia. McNeil JJ; Taylor HR; McCarty CA; eng Ophthalmic Epidemiol 1999 Sep;6(3):181-94. BC Dietary antioxidants and age-related maculopathy: the Blue Mountains Eye Study. National Centre for Smith W; MitEpidemiology and chell P; Webb Population Health, K; Leeder SR; Australian National University, Canberra. eng Ophthalmology 1999 Apr;106(4):7617. BC Racial differences in the prevalence of age-related macular degeneration: the Baltimore Eye Survey. Dana Center for Pre- Friedman DS; ventive Ophthalmol- Katz J; Bressogy, Wilmer Ophthal- ler NM; Rahmological Institute, mani B; Johns Hopkins UniTielsch JM; versity School of Medicine, Baltimore, eng Ophthalmology 1999 Jun;106(6):104955. BC Refractive error and age-related maculopathy: the Blue Mountains Eye Study. Visual acuity and its relationship to MRC Environmental early growth, eye disease, and aging Epidemiology Unit, in north Hertfordshire. Southampton General Hospital, Hants, UK. Pá gina 40 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TITULO ORIGEN Age-related maculopathy in a multiraDepartment of Ophcial United States population: the Na- thalmology and Visual tional Health and Nutrition ExaminaSciences, University tion Survey III. of Wisconsin Medical School, Madison 53705-2397, USA. [email protected]. edu AUTORES REF.: ACEMSA/SET/AC/ac febrero-2001 IDIOMA REVISTA CRIT. Klein R; Klein BE; Jensen SC; MaresPerlman JA; Cruickshanks KJ; Palta M; eng Ophthalmology 1999 Jun;106(6):105665. BC The prevalence of age-related maculopathy: the visual impairment project. Centre for Eye ReVanNewkirk search Australia, The MR; Nanjan University of Mel- MB; Wang JJ; bourne, East Mel- Mitchell P; Tabourne, Australia. ylor HR; McCarty CA; eng Ophthalmology 2000 Aug;107(8):1593-600. BC [Further studies on van der Hoeve's postulate, an antagonism between senile cataract ans senile macular degeneration] Gjessing HG; ger Acta Ophthalmol (Copenh) 1967;45(5):733-43. C Age-related macular degeneration. Macular changes, prevalence and sex ratio. An epidemiological study of 1000 aged individuals. University Eye Clinic, Rigshospitalet, Copenhagen, Denmark. Vinding T; eng Acta Ophthalmol (Copenh) 1989 Dec;67(6):609-16. C Occurrence of eye disorders and need for treatment in the elderly in special dwellings and nursing homes [corrected] Department of Public Rifaat R; KiveHealth Science, Unila SL; versity of Oulu, Finland. eng Acta Ophthalmol (Copenh) 1989 Dec;67(6):657-63. C Visual impairment of age-related macular degeneration. An epidemiological study of 1000 aged individuals. University Eye Clinic, Rigshospitalet, Copenhagen, Denmark. Vinding T; eng Acta Ophthalmol (Copenh) 1990 Apr;68(2):162-7. C Occurrence of drusen, pigmentary changes and exudative changes in the macula with reference to age-related macular degeneration. An epidemiological study of 1000 aged individuals. University Eye Clinic, Rigshospitalet, Copenhagen, Denmark. Vinding T; eng Acta Ophthalmol (Copenh) 1990 Aug;68(4):410-4. C Pigmentation of the eye and hair in relation to age-related macular degeneration. An epidemiological study of 1000 aged individuals. University Eye Clinic, Rigshospitalet, Copenhagen, Denmark. Vinding T; eng Acta Ophthalmol (Copenh) 1990 Feb;68(1):53-8. C Risk factor analysis for atrophic and exudative age-related macular degeneration. An epidemiological study of 1000 aged individuals. University Eye Clinic, Vinding T; ApRigshospitalet, Copleyard M; penhagen, Denmark. Nyboe J; Jensen G; eng Acta Ophthalmol (Copenh) 1992 Feb;70(1):66-72. C The prevalence of macular degeneraLaakso Municipal tion in a cohort of institutionalized ge- Hospital, Helsinki, Finriatric glaucoma patients. land. Perasalo R; eng Acta Ophthalmol (Copenh) 1994 Apr;72(2):175-7. C Current trends in newly registered National Eye Clinic for blindness in Denmark. the Visually Impaired, Hellerup, Denmark. Rosenberg T; Klie F; eng Acta Ophthalmol Scand 1996 Aug;74(4):395-8. C The incidence of registered blindness National Eye Clinic for caused by age-related macular de- the Visually Impaired, generation. Hellerup, Denmark. Rosenberg T; Klie F; eng Acta Ophthalmol Scand 1996 Aug;74(4):399-402. C Age-related macular degeneration in Inuit. Department of Ophthalmology, Odense University Hospital, Denmark. OstenfeldAkerblom A; eng Acta Ophthalmol Scand 1999 Feb;77(1):76-8. C Age-related macular degeneration. An epidemiological study of 1000 elderly individuals. With reference to prevalence, funduscopic findings, visual impairment and risk factors. University Eye Clinic, Rigshospitalet (The National Hospital), Copenhagen. Vinding T; eng Acta Ophthalmol Scand Suppl 1995;39 ( Pt 1)(217):1-32. C Pá gina 41 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TITULO ORIGEN AUTORES REF.: ACEMSA/SET/AC/ac febrero-2001 IDIOMA REVISTA CRIT. Age and sex distribution of some retinal macular diseases: senile and presenile macular degeneration and central serous retinitis. Knave B; Tengroth B; Voss M; eng Acta Ophthalmol Suppl 1984;161(2):95-103. C Prevalence of ocular disease and blindness in a rural area in the eastern region of Iceland during 1980 through 1984. University Eye DeJonasson F; partment, Landakot Thordarson K; Hospital, Reykjavik, Iceland. eng Acta Ophthalmol Suppl 1987;182(9):40-3. C The Framingham Eye Study. I. Outline and major prevalence findings. Kahn HA; Leibowitz HM; Ganley JP; Kini MM; Colton T; Nickerson RS; Dawber TR; eng Am J Epidemiol 1977 Jul;106(1):1732. C The Framingham Eye Study. II. Association of ophthalmic pathology with single variables previously measured in the Framingham Heart Study. Kahn HA; Leibowitz HM; Ganley JP; Kini MM; Colton T; Nickerson RS; Dawber TR; eng Am J Epidemiol 1977 Jul;106(1):3341. C Senile macular degeneration: review of epidemiologic features. Ferris FL; eng Am J Epidemiol 1983 Aug;118(2):13251. C Incidence estimates for lens changes, macular changes, open-angle glaucoma and diabetic retinopathy. Podgor MJ; Leske MC; Ederer F; eng Am J Epidemiol 1983 Aug;118(2):20612. C Factors associated with age-related EpidemiologyGoldberg J; macular degeneration. An analysis of Biometry Program, Flowerdew G; data from the first National Health and School of Public Smith E; BroNutrition Examination Survey. Health, University of Ildy JA; Tso linois-Chicago. MO; eng Am J Epidemiol 1988 Oct;128(4):70010. C The validity of self-reported and surroDepartment of Ophgate-reported cataract and age-related thalmology, University macular degeneration in the Beaver of Wisconsin Medical Dam Eye Study. School, Madison. Linton KL; Klein BE; Klein R; eng Am J Epidemiol 1991 Dec 15;134(12):1438-46. C The Beaver Dam Eye Study: the relaDepartment of Oph- Klein R; Klein tion of age-related maculopathy to thalmology, University BE; Linton KL; smoking. of Wisconsin Medical DeMets DL; School, Madison. eng Am J Epidemiol 1993 Jan 15;137(2):190-200. C Age-related macular degeneration is associated with atherosclerosis. The Rotterdam Study. Department of Oph- Vingerling JR; thalmology, Erasmus Dielemans I; University Medical Bots ML; School Rotterdam, Hofman A; The Netherlands. Grobbee DE; de Jong PT; eng Am J Epidemiol 1995 Aug 15;142(4):404-9. C Relation of smoking to the incidence of age-related maculopathy. The Beaver Dam Eye Study. Dept. of Ophthalmol- Klein R; Klein ogy and Visual Sci- BE; Moss SE; ences, University of Wisconsin-Madison 53705-2397, USA. eng Am J Epidemiol 1998 Jan 15;147(2):103-10. C A comprehensive survey of sequence variation in the ABCA4 (ABCR) gene in Stargardt disease and age-related macular degeneration. Institut fur Humange- Rivera A; Whinetik, Universitat te K; Stohr H; Wurzburg, D-97074 Steiner K; Wurzburg, Germany. Hemmrich N; Grimm T; Jurklies B; Lorenz B; Scholl HP; ApfelstedtSylla E; Weber BH; eng Am J Hum Genet 2000 Oct;67(4):80013. C Pá gina 42 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TITULO ORIGEN AUTORES REF.: ACEMSA/SET/AC/ac febrero-2001 IDIOMA REVISTA CRIT. Prevalence of senile cataract, diabetic retinopathy, senile macular degeneration, and open-angle glaucoma in the Framingham eye study. Kini MM; Leibowitz HM; Colton T; Nickerson RJ; Ganley J; Dawber TR; eng Am J Ophthalmol 1978 Jan;85(1):2834. C Senile lens and senile macular changes in a population-based sample. Sperduto RD; Seigel D; eng Am J Ophthalmol 1980 Jul;90(1):8691. C Prevalence of ocular disease in a population study of subjects 65 years old and older. Martinez GS; Campbell AJ; Reinken J; Allan BC; eng Am J Ophthalmol 1982 Aug;94(2):1819. C Relationship of senile macular degeneration to ocular pigmentation. Weiter JJ; Delori FC; Wing GL; Fitch KA; eng Am J Ophthalmol 1985 Feb 15;99(2):185-7. C The prevalence of macular drusen in postmortem eyes. Coffey AJ; Brownstein S; eng Am J Ophthalmol 1986 Aug 15;102(2):164-71. C The prevalence of macular drusen in postmortem eyes. Lewis H; Straatsma BR; Foos RY; eng Am J Ophthalmol 1986 Dec 15;102(6):801-3. C Juxtapapillary choroidal neovasculari- Department of Clinical zation in older patients. Ophthalmology, Moorfields Eye Hospital, London, England. Kies JC; Bird AC; eng Am J Ophthalmol 1988 Jan 15;105(1):11-9. C Alcohol intake and age-related maculopathy. Smith W; Mitchell P; eng Am J Ophthalmol 1996 Nov;122(5):743-5. C Familial aggregation of age-related maculopathy. De Jong PT; Klaver CC; Wolfs RC; Assink JJ; Hofman A; eng Am J Ophthalmol 1997 Dec;124(6):862-3. C Familial aggregation of age-related maculopathy. Epidemiology Unit, Seddon JM; Massachusetts Eye Ajani UA; Mitand Ear Infirmary, chell BD; Harvard Medical School, Boston, Massachusetts 02114, USA. [email protected] d.edu eng Am J Ophthalmol 1997 Feb;123(2):199-206. C A review of the literature concerning the epidemiology of senile macular degeneration. Blondin M; Kenya PR; eng Am J Optom Physiol Opt 1981 Aug;58(8):643-7. C Visual hallucinations in patients with Department of PsyHolroyd S; macular degeneration. chiatry and Behavioral Rabins PV; Sciences, Johns Hop- Finkelstein D; kins University School Nicholson MC; of Medicine, BaltiChase GA; more. Wisniewski SC; eng Am J Psychiatry 1992 Dec;149(12):1701-6. C Association among visual hallucinations, visual acuity, and specific eye pathologies in Alzheimer's disease: treatment implications. eng Am J Psychiatry 1999 Dec;156(12):1983-5. C National Centre for Epidemiology and Population Health, Australian National University, Australia. Royal Victoria Infir- Chapman FM; mary, Newcastle, Dickinson J; United Kingdom. McKeith I; Ballard C; Pá gina 43 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TITULO The association of age-related macular degeneration and lens opacities in the aged. ORIGEN AUTORES REF.: ACEMSA/SET/AC/ac febrero-2001 IDIOMA REVISTA CRIT. Epidemiology, De- Liu IY; White mography, and Bi- L; LaCroix AZ; ometry Program, National Institute on Aging, Bethesda, MD 20892. eng Am J Public Health 1989 Jun;79(6):765-9. C Department of Medicine, Brigham and Women's Hospital, Boston, MA, USA. Christen WG; Glynn RJ; Hennekens CH; eng Ann Epidemiol 1996 Jan;6(1):60-6. C A prospective study of alcohol conDepartment of Medisumption and the risk of age-related cine, Brigham and macular degeneration. Women's Hospital and Harvard Medical School, Boston, MA 02215-1204, USA. Ajani UA; Christen WG; Manson JE; Glynn RJ; Schaumberg D; Buring JE; Hennekens CH; eng Ann Epidemiol 1999 Apr;9(3):172-7. C Antioxidants and age-related eye disease. Current and future perspectives. Senile macular degeneration. Henkind P; eng Annu Rev Med 1971;22(1):95-102. C Vision screening in a primary care setting. A missed opportunity? Dana Center for Pre- Strahlman E; ventive Ophthalmol- Ford D; Whelogy, Wilmer Ophthalton P; Sommologic Institute, Balmer A; timore, MD. eng Arch Intern Med 1990 Oct;150(10):2159-64. C Arterial vascular anomalies of the retina. Awan KJ; eng Arch Ophthalmol 1977 Jul;95(7):1197202. C The grading and prevalence of macular degeneration in Chesapeake Bay watermen. Wilmer Ophthal- Bressler NM; mological Institute, Bressler SB; Johns Hopkins Medi- West SK; Fine cal Institutions, Balti- SL; Taylor HR; more, MD. eng Arch Ophthalmol 1989 Jun;107(6):847-52. C Exposure to sunlight and other risk factors for age-related macular degeneration. Dana Center for Pre- West SK; Roventive Ophthalmolsenthal FS; ogy, Wilmer Institute, Bressler NM; Johns Hopkins HospiBressler SB; tal, Baltimore, MD Munoz B; Fine 21205. SL; Taylor HR; eng Arch Ophthalmol 1989 Jun;107(6):875-9. C eng Arch Ophthalmol 1992 Dec;110(12):1701-8. C Cruickshanks KJ; Klein R; Klein BE; eng Arch Ophthalmol 1993 Apr;111(4):514-8. C Wolfe JA; Horton MB; McAteer MB; Szuter CF; Clayton T; eng Arch Ophthalmol 1993 Dec;111(12):1603-4. C Klein R; Klein BE; Wang Q; Moss SE; eng Arch Ophthalmol 1994 Feb;112(2):191-6. C Risk factors for neovascular agerelated macular degeneration. The Eye Disease Case-Control Study Group. Sunlight and age-related macular deDepartment of Ophgeneration. The Beaver Dam Eye Stu- thalmology, University dy. of Wisconsin Medical School, Madison 53705-2397. Race, macular degeneration, and diabetic maculopathy. Is age-related maculopathy associated Department of Ophwith cataracts? thalmology, University of Wisconsin, Madison. Pá gina 44 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TITULO ORIGEN AUTORES REF.: ACEMSA/SET/AC/ac febrero-2001 IDIOMA REVISTA CRIT. Serum antioxidants and age-related Department of OphMaresmacular degeneration in a population- thalmology and Visual Perlman JA; based case-control study. Sciences, University Brady WE; of Wisconsin Medical Klein R; Klein School, Madison, BE; Bowen P; USA. StacewiczSapuntzakis M; Palta M; eng Arch Ophthalmol 1995 Dec;113(12):1518-23. C Dietary fat and age-related maculopaDepartment of Ophthy. thalmology, University of Wisconsin Medical School, Madison, USA. MaresPerlman JA; Brady WE; Klein R; VandenLangenberg GM; Klein BE; Palta M; eng Arch Ophthalmol 1995 Jun;113(6):743-8. C Age-related eye disease and survival. Department of Oph- Klein R; Klein The Beaver Dam Eye Study. thalmology and Visual BE; Moss SE; Sciences, University of Wisconsin Medical School, Madison. eng Arch Ophthalmol 1995 Mar;113(3):333-9. C MaresPerlman JA; Klein R; Klein BE; Greger JL; Brady WE; Palta M; Ritter LL; eng Arch Ophthalmol 1996 Aug;114(8):991-7. C Smith W; Mitchell P; Leeder SR; eng Arch Ophthalmol 1996 Dec;114(12):1518-23. C Department of Oph- Vingerling JR; thalmology, Erasmus Hofman A; University Medical Grobbee DE; School, Rotterdam, de Jong PT; The Netherlands. eng Arch Ophthalmol 1996 Oct;114(10):1193-6. C Cruickshanks KJ; Hamman RF; Klein R; Nondahl DM; Shetterly SM; eng Arch Ophthalmol 1997 Feb;115(2):242-50. C Age-related macular disease in rural Queen's Medical CenPagliarini S; southern Italy. ter, University Hospital Moramarco A; Nottingham, England. Wormald RP; Piguet B; Carresi C; Balacco-Gabrieli C; Sehmi KS; Bird AC; eng Arch Ophthalmol 1997 May;115(5):616-22. C Bird AC; eng Arch Ophthalmol 1997 Oct;115(10):1311-3. C Klein R; Klein BE; Jensen SC; Cruickshanks KJ; eng Arch Ophthalmol 1998 Apr;116(4):506-13. C Association of zinc and antioxidant nuDepartment of Ophtrients with age-related maculopathy. thalmology, University of Wisconsin, Madison, USA. Smoking and age-related maculopathy. The Blue Mountains Eye Study. Age-related macular degeneration and smoking. The Rotterdam Study. National Centre for Epidemiology and Population Health, Australian National University, Canberra, Australia. The prevalence of age-related macuDepartment of Ophlopathy by geographic region and eth- thalmology and Visual nicity. The Colorado-Wisconsin Study Sciences, University of Age-Related Maculopathy. of Wisconsin Medical School, Madison, USA. What is the future of research in agerelated macular disease? The relationship of ocular factors to Department of Ophthe incidence and progression of age- thalmology and Visual related maculopathy. Sciences, University of Wisconsin Medical School, Madison 53705-2397, USA. Pá gina 45 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 TITULO ORIGEN AUTORES IDIOMA REVISTA CRIT. Smoking and age-related macular degeneration. The POLA Study. Pathologies Oculaires Liees a l'Age. INSERM U 500, National Institute of Health and Medical Research, Montpellier, France. [email protected] erm.fr Delcourt C; Diaz JL; Ponton-Sanchez A; Papoz L; eng Arch Ophthalmol 1998 Aug;116(8):1031-5. C Is age-related maculopathy related to Department of Oph- Klein R; Cruhearing loss? thalmology and Visual ickshanks KJ; Sciences, University Klein BE; of Wisconsin Medical Nondahl DM; School, Madison Wiley T; 53705-2397, USA. [email protected]. edu eng Arch Ophthalmol 1998 Mar;116(3):360-5. C Correlation between age-related Department of Oph- Kozobolis VP; macular degeneration and pseudoex- thalmology, University Detorakis ET; foliation syndrome in the population of of Crete, School of Tsilimbaris Crete (Greece). Health Sciences, Var- MK; Vlachonidinoyannion Eye kolis IG; Institute of Crete, Tsambarlakis Greece. IC; Pallikaris IG; eng Arch Ophthalmol 1999 May;117(5):664-9. C Age-related macular degeneration and INSERM Unite 500, Delcourt C; antioxidant status in the POLA study. National Institute of Cristol JP; POLA Study Group. Pathologies OcuHealth and Medical Tessier F; Lelaires Liees a l'Age. Research, Montpellier, ger CL; DesFrance. del- comps B; [email protected] poz L; erm.fr eng Arch Ophthalmol 1999 Oct;117(10):1384-90. C Age-specific causes of bilateral visual impairment. Centre for Eye Research Australia, University of Melbourne, Australia. [email protected] imelb.edu.au Weih LM; VanNewkirk MR; McCarty CA; Taylor HR; eng Arch Ophthalmol 2000 Feb;118(2):264-9. C Dietary fat and fish intake and agerelated maculopathy. National Centre for Epidemiology and Population Health, Australian National University, Australian Capital Territory. [email protected] Smith W; Mitchell P; Leeder SR; eng Arch Ophthalmol 2000 Mar;118(3):401-4. C Prospective study of alcohol consumption and the risk of age-related macular degeneration. Department of NutriCho E; Hantion, Harvard School kinson SE; Wiof Public Health, Bosllett WC; ton, Mass, USA. hpe- Stampfer MJ; [email protected] Spiegelman D; vard.edu Speizer FE; Rimm EB; Seddon JM; eng Arch Ophthalmol 2000 May;118(5):681-8. C Blindness in New South Wales. An estimate of the prevalence and some of the contributing causes. Banks CN; Hutton WK; eng Aust J Ophthalmol 1981 Nov;9(4):2858. C Changing patterns of blindness in Australia. Mitchell P; eng Aust N Z J Ophthalmol 1991 Nov;19(4):265-6. C Chan CW; Billson FA; eng Aust N Z J Ophthalmol 1991 Nov;19(4):321-5. C Visual disability and major causes of blindness in NSW: a study of people aged 50 and over attending the Royal Blind Society 1984 to 1989. Westmead Hospital, New South Wales, Australia. Pá gina 46 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TITULO ORIGEN AUTORES REF.: ACEMSA/SET/AC/ac febrero-2001 IDIOMA REVISTA CRIT. Gender, oestrogen, hormone replacement and age-related macular degeneration: results from the Blue Mountains Eye Study. National Centre for Smith W; MitEpidemiology and chell P; Wang Population Health, JJ; Australian National University, Canberra, Australia. eng Aust N Z J Ophthalmol 1997 May;25 Suppl 1(4):S13-5. C Baseline ophthalmic findings in the vitamin E, cataract and age-related maculopathy (VECAT) study. Centre for Eye Re- Robman LD; search Australia, UniTikellis G; versity of Melbourne, Garrett SK; Victoria, Australia. Harper CA; [email protected] McNeil JJ; Taelb.edu.au ylor HR; McCarty CA; eng Aust N Z J Ophthalmol 1999 Dec;27(6):410-6. C Common causes of blindness and visual handicap in the west of Scotland. Ghafour IM; Allan D; Foulds WS; eng Br J Ophthalmol 1983 Apr;67(4):20913. C Recent trends in the registration of Department of Oph- Thompson JR; blindness and partial sight in Leices- thalmology, University Du L; Rosentershire. of Leicester School of thal AR; Medicine, Leicester Royal Infirmary. eng Br J Ophthalmol 1989 Feb;73(2):95-9. C Visual function and course of basal Department of Ophlaminar drusen combined with vitelli- thalmology, University form macular detachment. of Paris, XII-Creteil, Hopital Intercommunal, France. Cohen SY; Meunier I; Soubrane G; GlacetBernard A; Coscas GJ; eng Br J Ophthalmol 1994 Jun;78(6):43740. C Do patients with age related maculopathy and cataract benefit from cataract surgery? Bristol Eye Hospital. Shuttleworth GN; Luhishi EA; Harrad RA; eng Br J Ophthalmol 1998 Jun;82(6):6116. C ATP binding cassette transporter retina genotypes and age related macular degeneration: an analysis on exudative non-familial Japanese patients. Department of Ophthalmology, Shinshu University School of Medicine, Matsumoto 390-8621, Japan. Kuroiwa S; Kojima H; Kikuchi T; Yoshimura N; eng Br J Ophthalmol 1999 May;83(5):6135. C Visual impairment and cancer: a popu- Finnish Cancer RegisPukkala E; lation-based cohort study in Finland. try, Helsinki. Verkasalo PK; Ojamo M; Rudanko SL; eng Cancer Causes Control 1999 Feb;10(1):13-20. C Wu ZQ; chi Chung Hua Yen Ko Tsa Chih 1992 Jul;28(4):246-7. C Storm of the eye. Macular degeneration: the forgotten plague. Buss DD; eng Contemp Longterm Care 1993 Nov;16(11):62-3, 65-7. C Prevalence of age-related macular degeneration. St. Franziskus Hospi- Pauleikhoff D; tal, Department of Koch JM; Ophthalmology, Munster, Germany. eng Curr Opin Ophthalmol 1995 Jun;6(3):51-6. C [Epidemiologic survey of senile macuDepartment of Ophlar degeneration] thalmology, Chenzhou District People's Hospital, Hunan Province. Nutrition and the epidemiology of cataract and age-related maculopathy. Department of Social and Preventive Medicine, Gauhati Medical College, Assam, India. Sarma U; Brunner E; Evans J; Wormald R; eng Eur J Clin Nutr 1994 Jan;48(1):1-8. C Epidemiology of eye disease in the elDepartment of Comderly. munity and Preventive Medicine, State University of New York, Stony Brook 11794. Hyman L; eng Eye 1987;1 ( Pt 2)(9):330-41. C Pá gina 47 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TITULO ORIGEN Montgomery lecture. Subretinal neoDepartment of Ophvascularisation in senile macular de- thalmology of Creteil, generation. University of Paris-Val de Marne, France. AUTORES REF.: ACEMSA/SET/AC/ac febrero-2001 IDIOMA REVISTA CRIT. Coscas G; eng Eye 1987;1 ( Pt 3)(9):364-78. C Aclimandos WA; Galloway NR; eng Eye 1988;2 ( Pt 4)(1):431-4. C Prevalence of age-related maculopaDepartment of Oph- Dickinson AJ; thy at two points in time in an elderly thalmology, Royal Vic- Sparrow JM; British population. toria Infirmary, NewDuke AM; castle upon Tyne, UK. Thompson JR; Gibson JM; Rosenthal AR; eng Eye 1997;11 ( Pt 3)(6):301-14. C Seven year follow-up of age-related University Department Sparrow JM; maculopathy in an elderly British of Ophthalmology, Dickinson AJ; population. Bristol Eye Hospital, Duke AM; UK. Thompson JR; Gibson JM; Rosenthal AR; eng Eye 1997;11 ( Pt 3)(6):315-24. C Sibling correlations and segregation Department of Biome- Heiba IM; Elsanalysis of age-related maculopathy: try and Genetics, LSU ton RC; Klein the Beaver Dam Eye Study. Medical Center, New BE; Klein R; Orleans 70112-1393. eng Genet Epidemiol 1994;11(1):51-67. C Macular disease in an elderly population. eng Ger J Ophthalmol 1992;1(1):12-5. C Carter TL; eng Geriatrics 1994 Sep;49(9):37-42, 45; quiz 46-7. C Prevalence of low vision in elderly pa- Department of Geriat- Jack CI; Smith tients admitted to an acute geriatric ric Medicine, UniverT; Neoh C; unit in Liverpool: elderly people who sity of Liverpool, UK. Lye M; McGafall are more likely to have low vision. lliard JN; eng Gerontology 1995;41(5):280-5. C The Swedish Retinal Detachment Department of OphRegister. I. A database for epidemiol- thalmology, University ogical and clinical studies. of Linkoping, Sweden. Algvere PV; Jahnberg P; Textorius O; eng Graefes Arch Clin Exp Ophthalmol 1999 Feb;237(2):137-44. C [Age-related macular degeneration: present situation and a glance toward the future] Garzozi HJ; Lang Y; Harris A; heb Harefuah 2000 Apr 2;138(7):567-72. C Retinal venous occlusive disease. Wong VK; eng Hawaii Med J 1997 Oct;56(10):289-91. C Hereditary macular degeneration--a population survey in the country of Vsterbotten, Sweden. Nordstrom S; eng Hereditas 1974;78(1):41-62. C Hereditary maculardegeneration (HMD) in 246 cases traced to one gene-source in central Sweden. Nordstrom S; Barkman Y; eng Hereditas 1977 Feb 3;84(2):163-76. C Central corneal endothelial guttae and age-related macular degeneration: is there an association? St Paul's Eye Unit, Rao GP; Kaye Royal Liverpool UniSB; Agiusversity Hospital, Uni- Fernandez A; ted Kingdom. eng Indian J Ophthalmol 1998 Sep;46(3):145-7. C Report on the nationwide epidemiolDepartment of OphYuzawa M; ogical survey of exudative age-related thalmology, Surugadai Tamakoshi A; macular degeneration in Japan. Hospital of Nihon Uni- Kawamura T; versity, Tokyo, Japan. Ohno Y; Uyama M; Honda T; eng Int Ophthalmol 1997;21(1):1-3. C Blindness in the city of Nottingham (1980-1985). University Eye Hospi- Pauleikhoff D; tal, Essen, Federal Wormald RP; Republic of Germany. Wright L; Wessing A; Bird AC; Age-related vision changes: a primary College of Optometry, care guide. State University of New York (SUNY). Pá gina 48 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TITULO ORIGEN AUTORES REF.: ACEMSA/SET/AC/ac febrero-2001 IDIOMA REVISTA CRIT. The relationship of age-related macuDepartment of Oph- Klein R; Wang lopathy, cataract, and glaucoma to vi- thalmology and Visual Q; Klein BE; sual acuity. Sciences, University Moss SE; of Wisconsin Medical Meuer SM; School, Madison. eng Invest Ophthalmol Vis Sci 1995 Jan;36(1):182-91. C Pattern of age-related maculopathy in Department of OphWang Q; the macular area. The Beaver Dam thalmology and Visual Chappell RJ; Eye Study. Sciences, University Klein R; Eisof Wisconsin Medical ner A; Klein School, Madison BE; Jensen 53705-2397, USA. SC; Moss SE; eng Invest Ophthalmol Vis Sci 1996 Oct;37(11):2234-42. C Risk factors for high-risk proliferative diabetic retinopathy and severe visual loss: Early Treatment Diabetic Retinopathy Study Report #18. University of Wisconsin, Madison, USA. Davis MD; Fisher MR; Gangnon RE; Barton F; Aiello LM; Chew EY; Ferris FL; Knatterud GL; eng Invest Ophthalmol Vis Sci 1998 Feb;39(2):233-52. C Eye screening in the elderly. Mercer's Institute for Research on Ageing, Saint James's Hospital, Dublin. Keane EM; O'Connor M; Coakley D; Walsh JB; eng Ir Med J 1997 Jun-Jul;90(4):141-2. C The relationship between low vision and performance of activities of daily living in nursing home residents. Research Institute, Hebrew Home of Greater Washington, Rockville, MD 20852. Marx MS; Werner P; CohenMansfield J; Feldman R; eng J Am Geriatr Soc 1992 Oct;40(10):1018-20. C Moderate wine consumption is associ- Department of Internal Obisesan TO; ated with decreased odds of developMedicine, Howard Hirsch R; Koing age-related macular degeneration University Hospital, soko O; Carlin NHANES-1. Washington, DC son L; Parrott 20060, USA. M; eng J Am Geriatr Soc 1998 Jan;46(1):1-7. C Visual impairment and falls in older adults: the Blue Mountains Eye Study. Department of Public Ivers RQ; Health and Commu- Cumming RG; nity Medicine, Univer- Mitchell P; Atsity of Sydney, New tebo K; South Wales, Australia. eng J Am Geriatr Soc 1998 Jan;46(1):5864. C The prevalence of macular drusen in a population of patients with known insulin-dependent diabetes mellitus. Alexander LJ; eng J Am Optom Assoc 1985 Oct;56(10):806-10. C Dietary prevention of age-related macular degeneration. Pratt S; eng J Am Optom Assoc 1999 Jan;70(1):39-47. C ARMD is robbing older people blind-and stealing their independence, too. Perry DP; eng J Am Optom Assoc 1999 Jan;70(1):79. C Mitchell RA; eng J Epidemiol Community Health 1993 Feb;47(1):42-5. C Perdriel G; fre J Fr Ophtalmol 1984;7(2):89-91. C Prevalence of age related macular de- Department of Behavgeneration in persons aged 50 years ioural Sciences, Facand over resident in Australia. ulty of Health Sciences, University of Sydney, Lidcombe, NSW, Australia. [Senile macular degeneration and its treatment] Pá gina 49 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TITULO ORIGEN AUTORES REVISTA CRIT. fre J Fr Ophtalmol 1999 May;22(4):431-7. C Peyraud-Gilly VM; Daubas P; Joly T; Filliard G; MonrouxRousseau S; fre J Fr Ophtalmol 2000 May;23(5):472-4. C Hooge Burch, Centre Evenhuis HM; for people with Intellectual Disability, Zwammerdam, The Netherlands. eng J Intellect Disabil Res 1995 Feb;39 ( Pt 1)(1):19-25. C [Visual acuity and ocular diseases in Service d'OphtalmoloTaiel-Sartral aged residents of nursing homes: stugie, CHR Orleans. M; Nounou P; dy of 219 persons in Orleans] Rea C; el Alamy A; Bendeddouche K; Boumezrag M; Milcamps R; Cohen D; [Macular functions in professional di- Service d'Ophtalmolovers] gie, Hopital d'Instruction des Armees Sainte-Anne, F 83000 Toulon Naval. [email protected] om Medical aspects of ageing in a population with intellectual disability: I. Visual impairment. Sunlight and age-related eye disease. REF.: ACEMSA/SET/AC/ac febrero-2001 IDIOMA Department of Anatomy and Cell Biology, Jules Stein Eye Institute, Los Angeles, California. Young RW; eng J Natl Med Assoc 1992 Apr;84(4):3538. C Macular degeneration: how big is the University of Alabama problem? Medical Center, Birmingham. Cheraskin E; eng J Natl Med Assoc 1992 Oct;84(10):873-6. C Visual hallucinations in patients from Department of Psyan ophthalmology clinic and medical chiatry and Behavioral clinic population. Sciences, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA. Holroyd S; Rabins PV; Finkelstein D; Lavrisha M; eng J Nerv Ment Dis 1994 May;182(5):273-6. C A three-year follow-up study of visual Department of Psyhallucinations in patients with macular chiatric Medicine, Unidegeneration. versity of Virginia School of Medicine, Blue Ridge Hospital, Charlottesville, Virginia 22901, USA. Holroyd S; Rabins PV; eng J Nerv Ment Dis 1996 Mar;184(3):1889. C Imes CB; Peck C; eng J Okla State Med Assoc 1993 Jun;86(6):279-83. C Age-related macular degeneration: new treatments show promise. DuBosar R; eng J Ophthalmic Nurs Technol 1999 MarApr;18(2):60-4. C Visual handicap in south-east Scotland. Princess Alexandra Balatsoukas Eye Pavilion, Edin- DD; Sioulis C; burgh, UK. Parisi A; Millar GT; eng J R Coll Surg Edinb 1995 Feb;40(1):49-51. C Prevalence of ocular diseases in Dept. of Epidemiology Costacou T; South Carolina. and Biostatistics, USC Mayer-Davis School of Public EJ; Davis RM; Health, Columbia 29208, USA. eng J S C Med Assoc 2000 Jun;96(6):2516. C Vision quality of elderly Oklahomans. Department of Ophthalmology, Baptist Medical Center, Oklahoma City. Pá gina 50 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TITULO ORIGEN AUTORES REF.: ACEMSA/SET/AC/ac febrero-2001 IDIOMA REVISTA CRIT. Dietary carotenoids, vitamins A, C, and E, and advanced age-related macular degeneration. Eye Disease Case-Control Study Group. Epidemiology Unit, Massachusetts Eye and Ear Infirmary, Boston 02114. Seddon JM; Ajani UA; Sperduto RD; Hiller R; Blair N; Burton TC; Farber MD; Gragoudas ES; Haller J; Miller DT; et al.; eng JAMA 1994 Nov 9;272(18):1413-20. C A prospective study of cigarette smoking and age-related macular degeneration in women. Epidemiology Unit, Massachusetts Eye and Ear Infirmary, Boston, MA 02114, USA. Seddon JM; Willett WC; Speizer FE; Hankinson SE; eng JAMA 1996 Oct 9;276(14):1141-6. C A prospective study of cigarette smok- Division of Preventive ing and risk of age-related macular Medicine, Department degeneration in men. of Medicine, Brigham and Women's Hospital, Boston, Mass, USA. Christen WG; Glynn RJ; Manson JE; Ajani UA; Buring JE; eng JAMA 1996 Oct 9;276(14):1147-51. C [Incidence, age and occupational distribution of senile and myopic macular degeneration] Fulle HH; ger Klin Monatsbl Augenheilkd 1968;153(4):578-88. C [Cause of blindness in Bavaria. Evaluation of a representative sample from blindness compensation records of Upper Bavaria] Augenklinik, UniversiKrumpaszky tat Munchen. HG; Klauss V; ger Klin Monatsbl Augenheilkd 1992 Feb;200(2):142-6. C Graf M; Halbach E; Kaufmann H; ger Klin Monatsbl Augenheilkd 1999 Jul;215(1):50-5. C [Causes of blindness in Hessia in Augenklinik fur 1996] Schielbehandlung und Neuroophthalmologie der Justus-LiebigUniversitat Giessen. [Age related macular degeneration as a cause of blindness] Katedry i Kliniki Okulistyki Collegium Medicum UJ, Krakow. Starzycka M; Slomska J; pol Klin Oczna 1997;99(4):253-5. C [Epidemiology and risk factors for age related macular degeneration] Katedry i Kliniki Okulistyki Collegium Medicum UJ w Krakowie. Starzycka M; pol Klin Oczna 1997;99(4):271-5. C Age-related macular degeneration: a leading cause of blindness. Department of Ophthalmology, Victoria Hospital, Blackpool, United Kingdom. O'Shea JG; eng Med J Aust 1996 Nov 18;165(10):5614. C Visual impairment in nursing home Department of Ophresidents: the Blue Mountains Eye thalmology, University Study. of Sydney, NSW. [email protected] u "Smoking is a major cause of blindness". Mitchell P; Hayes P; Wang JJ; eng Med J Aust 1997 Jan 20;166(2):73-6. C Mitchell P; Chapman S; Smith W; eng Med J Aust 1999 Aug 16;171(4):1734. C Programme de PreNegrel AD; vention de la Cecite, Avognon Z; l'Organisation Mon- Minassian DC; diale de la Sante, Babagbeto M; Geneve, Suisse. Oussa G; Bassabi S; fre Med Trop (Mars) 1995;55(4 Pt 2):40914. C [Blindness in Benin] Pá gina 51 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TITULO The natural history of geographic atrophy, the advanced atrophic form of age-related macular degeneration. ORIGEN The Wilmer Ophthalmological Institute, The Johns Hopkins University School of Medicine, Baltimore, MD 21205, USA. [email protected] AUTORES REF.: ACEMSA/SET/AC/ac febrero-2001 IDIOMA REVISTA CRIT. Sunness JS; eng Mol Vis 1999 Nov 3;5(12):25. C Dana Center for PreSommer A; ventive OphthalmolTielsch JM; ogy, Johns Hopkins Katz J; QuigSchool of Hygiene and ley HA; Public Health, BaltiGottsch JD; more, MD. Javitt JC; Martone JF; Royall RM; Witt KA; Ezrine S; eng N Engl J Med 1991 Nov 14;325(20):1412-7. C Hofman A; Boerlage PA; Bots ML; den Breeijen JH; de Bruijn AM; Grobbee DE; Hoes AW; de Jong PT; Koenders MJ; Odding E; et al.; dut Ned Tijdschr Geneeskd 1995 Sep 30;139(39):1975-8. C [Macular diseases in the elderly person] Matsui M; jpn Nippon Ganka Gakkai Zasshi 1989 Sep;93(9):883-907. C [Epidemiology, risk factors and pathogenesis of age-related macular degeneration] Yuzawa M; jpn Nippon Ganka Gakkai Zasshi 1997 Sep;101(9):705-6. C Visual loss in geriatric residents of northwestern Ohio nursing homes. Kiess RD; Kollarits CR; Mehelas TJ; Slak S; Burns RJ; Todia WJ; eng Ohio State Med J 1984 Mar;80(3):2357. C [Solar radiation and choroidal neovascularization. An epidemiologic study] GastroCorreia J; Coutinho MF; Maria J; da Silva AC; Rosas V; Martins N; Prezia F; fre Ophtalmologie 1988 Apr-Jun;2(2):1779. C Prevalence and causes of blindness in Dept. Ophthalmol., Newland HS; the South Australian population aged Royal Adelaide Hospi- Hiller JE; Cas50 and over. tal, Australia. son RJ; Obermeder S; eng Ophthalmic Epidemiol 1996 Jun;3(2):97-107. C Visual sensitivity and age-related eye diseases. The Beaver Dam Eye Study. Racial differences in the causespecific prevalence of blindness in east Baltimore. [Prevalence of chronic diseases in the Erasmus Universiteit, elderly; the ERGO study (Erasmus Instituut Epidemiologie Rotterdam Health and the Elderly)] en Biostatistiek, Rotterdam. Dept. Ophthalmol. & Visual Sci., Univ. of Wisconsin Med. Sch., Madison, USA. Klein BE; Klein R; Jensen SC; eng Ophthalmic Epidemiol 1996 Mar;3(1):47-55. C The Wisconsin Age-related Macular University Department Degeneration grading system: perof Ophthalmology, formance in an independent centre. Bristol Eye Hospital, U.K. Sparrow JM; Dickinson AJ; Duke AM; eng Ophthalmic Epidemiol 1997 Mar;4(1):49-55. C University of Sydney, Wang JJ; MitDepartment of Ophchell PG; thalmology, Sydney, Cumming RG; Australia. Lim R; eng Ophthalmic Epidemiol 1999 Dec;6(4):317-26. C Cataract and age-related maculopathy: the Blue Mountains Eye Study. Pá gina 52 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TITULO ORIGEN AUTORES REF.: ACEMSA/SET/AC/ac febrero-2001 IDIOMA REVISTA CRIT. Methodology of the VECAT study: vitamin E intervention in cataract and age-related maculopathy. Monash University Garrett SK; Medical School De- McNeil JJ; Sipartment of Epidemilagy C; Sinology & Preventive clair M; ThoMedicine Prahran, mas AP; Australia. siRobman LP; [email protected] McCarty CA; nash.edu.au Tikellis G; Taylor HR; eng Ophthalmic Epidemiol 1999 Sep;6(3):195-208. C A practice-based survey of familial age-related maculopathy. Seneca Eye Sur- Keverline MR; geons, Warren, PA, Mah TS; KeUSA. verline PO; Gorin MB; eng Ophthalmic Genet 1998 Mar;19(1):1926. C Causes of blindness and partial sight School of Optometry, Yap M; Weatin the Bradford Metropolitan District University of Bradford, herill J; from 1980 to 1985. UK. eng Ophthalmic Physiol Opt 1989 Jul;9(3):289-92. C Weber U; Michaelis L; Wirth KE; ger Ophthalmologe 1993 Oct;90(5):486-9. C [Incidence of posterior vitreous detachment in eyes with and without age-related macular degeneration. An ultrasonic study] Augenklinik, Stad- Weber-Krause tische Kliniken Frank- B; Eckardt U; furt am Main/Hochst. ger Ophthalmologe 1996 Dec;93(6):660-5. C [Age-related macular degeneration. 1. Epidemiology, pathogenesis and differential diagnosis] Augenabteilung, St. Pauleikhoff D; Franziskus-Hospital, Holz FG; Munster. ger Ophthalmologe 1996 Jun;93(3):299315. C [New blindness incidents in Wurttemberg-Hohenzollern] Institut fur MedizKrumpaszky inische Informations- HG; Haas A; verarbeitung, TubinKlauss V; gen. Selbmann HK; ger Ophthalmologe 1997 Mar;94(3):234-6. C Association between drusen and some of the risk factors for coronary artery disease. Vidaurri JS; Pe'er J; Halfon ST; Halperin G; Zauberman H; eng Ophthalmologica 1984;188(4):243-7. C Blindness incidence in Germany. A Institute for Medical Krumpaszky population-based study from Wurt- Information Process- HG; Ludtke R; temberg-Hohenzollern. ing, University of TubMickler A; ingen, Germany. Klauss V; hans.krumpaszky@dg Selbmann HK; n.de eng Ophthalmologica 1999;213(3):176-82. C eng Ophthalmology 1987 Sep;94(9):11915. C Moss SE; Klein R; Klein BE; eng Ophthalmology 1988 Oct;95(10):13408. C Eye disease in a geriatric nursing hoDepartment of Oph- Whitmore WG; me population. thalmology, New York Hospital-Cornell University Medical Center, New York. eng Ophthalmology 1989 Mar;96(3):393-8. C Prevalence of age-related maculopaDepartment of Oph- Klein R; Klein thy. The Beaver Dam Eye Study. thalmology, University BE; Linton KL; of Wisconsin, Madison 53792. eng Ophthalmology 1992 Jun;99(6):93343. C [Serum lipids and vitamins in senile macular degeneration] The dimensions of the problem of eye disease among the elderly. Augenklinik des Akademischen Lehrkrankenhauses Braunschweig, Universitat Dusseldorf. Department of Oph- Pizzarello LD; thalmology, Columbia University College of Physicians and Surgeons, New York, NY. The incidence of vision loss in a diaDepartment of Ophbetic population. thalmology, University of Wisconsin Medical School, Madison. Pá gina 53 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TITULO ORIGEN AUTORES REF.: ACEMSA/SET/AC/ac febrero-2001 IDIOMA REVISTA CRIT. Diabetes, hyperglycemia, and ageDepartment of Oph- Klein R; Klein related maculopathy. The Beaver Dam thalmology, University BE; Moss SE; Eye Study. of Wisconsin, Madison 53792-3220. eng Ophthalmology 1992 Oct;99(10):152734. C The relationship of cardiovascular dis- University of Wiscon- Klein R; Klein ease and its risk factors to age-related sin, Department of BE; Franke T; maculopathy. The Beaver Dam Eye Ophthalmology, MadiStudy. son 53792-3220. eng Ophthalmology 1993 Mar;100(3):40614. C Department of Oph- Vingerling JR; thalmology, Erasmus Dielemans I; University Medical Hofman A; School, Rotterdam, Grobbee DE; The Netherlands. Hijmering M; Kramer CF; de Jong PT; eng Ophthalmology 1995 Feb;102(2):20510. C Racial/ethnic differences in ageDepartment of Oph- Klein R; Rowrelated maculopathy. Third National thalmology and Visual land ML; HarHealth and Nutrition Examination SurSciences, University ris MI; vey. of Wisconsin Medical School, Madison. eng Ophthalmology 1995 Mar;102(3):37181. C Mitchell P; Smith W; Attebo K; Wang JJ; eng Ophthalmology 1995 Oct;102(10):1450-60. C Rosenblatt I; Loewenstein A; Lazar M; Yassur Y; eng Ophthalmology 1996 Feb;103(2):1967. C Risk factors of age-related maculopaDepartment of OphHirvela H; thy in a population 70 years of age or thalmology, University Luukinen H; older. of Oulu, Finland. Laara E; Sc L; Laatikainen L; eng Ophthalmology 1996 Jun;103(6):8717. C Sensitivity, specificity, and predictive Doheny Eye Institute, Ariyasu RG; values of screening tests for eye conDepartment of Oph- Lee PP; Linton ditions in a clinic-based population. thalmology, Los AngeKP; LaBree les, CA 90033, USA. LD; Azen SP; Siu AL; eng Ophthalmology 1996 Nov;103(11):1751-60. C The five-year incidence and progresDepartment of Ophsion of age-related maculopathy: the thalmology and Visual Beaver Dam Eye Study. Sciences, University of Wisconsin Medical School, Madison 53705-2397, USA. Klein R; Klein BE; Jensen SC; Meuer SM; eng Ophthalmology 1997 Jan;104(1):7-21. C McMaster University, Division of Geriatric Medicine, Hamilton, Ontario, Canada. Darzins P; Mitchell P; Heller RF; eng Ophthalmology 1997 May;104(5):7706. C The relation of cardiovascular disease Department of Ophand its risk factors to the 5-year inci- thalmology and Visual dence of age-related maculopathy: the Sciences, University Beaver Dam Eye Study. of Wisconsin Medical School, Madison 53705-2397, USA. Klein R; Klein BE; Jensen SC; eng Ophthalmology 1997 Nov;104(11):1804-12. C Alcohol consumption and the 5-year Department of Ophincidence of age-related maculopathy: thalmology and Visual the Beaver Dam eye study. Sciences, University of Wisconsin Medical School, Madison 53705-2397, USA. Moss SE; Klein R; Klein BE; Jensen SC; Meuer SM; eng Ophthalmology 1998 May;105(5):78994. C The prevalence of age-related maculopathy in the Rotterdam Study. Prevalence of age-related maculopaDepartment of Ophthy in Australia. The Blue Mountains thalmology, University Eye Study. of Sydney, Westmead, Australia. ARM in Rotterdam Study. Sun exposure and age-related macular degeneration. An Australian casecontrol study. Pá gina 54 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TITULO REVISTA CRIT. eng Ophthalmology 1999 Feb;106(2):21522. C eng Ophthalmology 2000 Dec;107(12):2203-8. C eng Ophthalmology 2000 Dec;107(12):2224-32. C Mitchell RA; eng Optom Vis Sci 1993 Feb;70(2):102-6. C Long-term drusen study. VA Greater Los Ange- Sarraf D; Gin les Healthcare Sys- T; Yu F; Brantem, Ophthalmology non A; Owens Section, and the Jules SL; Bird AC; Stein Eye Institute, UCLA School of Medicine, California, USA. eng Retina 1999;19(6):513-9. C Associations of antioxidant enzymes with cataract and age-related macular degeneration. The POLA Study. Pathologies Oculaires Liees a l'Age. Visual impairment and eye diseases in elderly institutionalized Australians. ORIGEN AUTORES REF.: ACEMSA/SET/AC/ac febrero-2001 INSERM Unite 500, Delcourt C; Montpellier, France. Cristol JP; Leger CL; Descomps B; Papoz L; Centre for Eye Research Australia, University of Melbourne, Melbourne, Australia. VanNewkirk MR; Weih L; McCarty CA; Stanislavsky YL; Keeffe JE; Taylor HR; Risk factors associated with age- AREDS Coordinating related macular degeneration. A case- Center, The EMMES control study in the age-related eye Corporation, 11325 disease study: age-related eye disSeven Locks Road, ease study report number 3. AgeSuite 214, Potomac, Related Eye Disease Study Research MD 20854-3205, USA. Group. [email protected] Contrast sensitivity in elderly subjects Department of Behavwith a diagnosed ocular disease. ioural Sciences, The Faculty of Health Sciences, University of Sydney, New South Wales, Australia. IDIOMA [Age-related macular degeneration] Departamento de Of- Garcia Layana talmologia, Facultad A; de Medicina, Universidad de Navarra. spa Rev Med Univ Navarra 1998 JanMar;42(1):42-8. C [Macular degeneration related to age] Soubrane G; Coscas G; fre Rev Prat 1989 May 11;39(14):1196200. C [Age related macular degeneration and subretinal neovessels. Primary cause of acquired blindness in adults in France] Coscas G; fre Rev Prat 1991 Nov 1;41(23):2320-2. C Soubrane G; Coscas G; fre Rev Prat 1996 Sep 15;46(14):1722-9. C The Framingham eye study: introduction to the monograph. Kreuger DE; Milton RC; Maunder LR; eng Surv Ophthalmol 1980 MayJun;24(6):614-20. C The Beaver Dam Eye Study: the relation of age-related maculopathy to smoking. Schwartz D; eng Surv Ophthalmol 1994 JulAug;39(1):84-5. C An international classification and grading system for age-related maculopathy and age-related macular degeneration. The International ARM Epidemiological Study Group. Bird AC; Bressler NM; Bressler SB; Chisholm IH; Coscas G; Davis MD; de Jong PT; Klaver CC; Klein BE; Klein R; et al.; eng Surv Ophthalmol 1995 MarApr;39(5):367-74. C [Age-related macular degeneration] Clinique ophtalmologique universitaire, Universite Paris XII, Creteil. Pá gina 55 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad TITULO Visible light and risk of age-related macular degeneration. ORIGEN AUTORES REF.: ACEMSA/SET/AC/ac febrero-2001 IDIOMA REVISTA CRIT. Dana Center for PreTaylor HR; ventive OphthalmolMunoz B; ogy, Wilmer Institute, West S; Johns Hopkins Uni- Bressler NM; versity, Baltimore, MaBressler SB; ryland. Rosenthal FS; eng Trans Am Ophthalmol Soc 1990;88(1):163-73; discussion 173-8. C Are sex hormones associated with Department of OphKlein BE; age-related maculopathy in women? thalmology and Visual Klein R; JenThe Beaver Dam Eye Study. Sciences, University sen SC; Ritter of Wisconsin Medical LL; School, Madison. eng Trans Am Ophthalmol Soc 1994;92(1):289-95; discussion 295-7. C A twin study on age-related macular degeneration. Meyers SM; eng Trans Am Ophthalmol Soc 1994;92(1):775-843. C Investigation of senile macular degeneration. Marmion VJ; eng Trans Ophthalmol Soc U K 1974;94(4):1033-9. C A study of the prevalence of eye disease in the elderly in an English community. Gibson JM; Rosenthal AR; Lavery J; eng Trans Ophthalmol Soc U K 1985;104 ( Pt 2)(2):196-203. C [Visual handicaps among the elderly in nursing homes. A pilot study] Krarup JC; Goldschmidt E; dan Ugeskr Laeger 1980 Jul 14;142(29):1897-8. C Pá gina 56 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 ANEXO 5 Pá gina 57 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Photodynamic therapy for age-related macular degeneration SMM-report nr.3/2000 The Norwegian Centre for Health Technology Assessment The Steering committee of the Norwegian Centre for Health Technology Assessment (SMM) decided in December 1999 to assess photodynamic therapy for age-related macular degeneration. This is a new therapeutic modality and the Steering committee wished to perform an early evaluation before the method become widespread in the Norwegian health system. SMM established an expert group that started their work in February 2000. The expert group was constituted by: Professor Johan H. Seland (chairman), Haukeland University Hospital Chief Departmental Physician Ragnheidur Bragadottir, Ullevål University Hospital Senior Physician Christian Hedels, Vestfold County Hospital Professor Per Syrdalen, The National Hospital Dr. Søren Holm, Centre for Social Ethics and Policy, University of Manchester, was invited to make an ethical consideration on the treatment of age-related macular degeneration. His contribution is found in Chapter 10. Medical consultant Inge Kjønniksen, SMM, has been project leader, assisted by medical consultant Krystyna Hviding. The report has been approved by the Steering committee for SMM. Berit Mørland Inge Kjønniksen Director Medical consultant Content 1. Dictionary * 2. Summary * 3. Introduction * 4. Epidemiology * 5. Norwegian participation in clinical research * 6. Photodynamic treatment of subfoveal CNV * 7. Equipment, competence and resources needed in Norway * 8. Organisational consequences * 9. Cost analyses, social consequences * 10. Ethical considerations * 11. Alternative treatments * 12. Indication for photodynamic treatment in other eye diseases * 13. Conclusions * 14. References * 1. Dictionary AMD Age-related macular degeneration ARM Age-related maculopathy – precursor to AMD CNV Choroidal neovascularisation/newly formed and pathological vessels constituting membranes in the area of the visual acuity centre. DRG Diagnosis-related groups – system for calculating treatment costs in hospitals Fovea Area in the retina responsible for visual acuity ISF Activity-based funding – funding based on DRG Classic Cluster of blood vessels that has penetrated the pigment epithelium Mixed Mixture of "occult" and "classic" NOK Norwegian monetary unit, 1 ECU = 8.2 NOK Occult Cluster of blood vessels beneath the pigment epithelium PDT Photodynamic therapy RTV Rikstrygdeverket/The National Insurance Institution – funds all out-patient treatment except day-surgery Pá gina 58 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 TAP-study Treatment of Age-related Macular Degeneration with Photodynamic Therapy (TAP) trial (phase III study including patients with a mixture of classic and occult lesions) VIP-study Verteporfin in Photodynamic Therapy (VIP) trial (phase III study with patients having only classic or occult lesions) 2. Summary Age-related macular degeneration is a leading cause of loss of vision among elderly, and these patients have previously lacked therapeutic options. The disease can be either nonexudative (dry) or exudative. This report deals with photodynamic therapy, which is a new therapeutic modality for the most serious exudative subform. Untreated these patients undergo rapid loss of their central vision due to uncontrolled blood vessel proliferation in a process called choroidal neovascularisation (CNV). Several new therapeutic options are presently being tested to control the disease, and photodynamic therapy has so far proven most promising. The rationale is to inject photoreactive drugs, which are concentrated in the abnormal blood vessels in the eye fundus. Subsequently, these vessels are illuminated with light of a specific wavelength thereby transforming the drugs to become reactive and to exert local tissue toxicity. The aim is to destroy abnormal vessels and to prevent further blood vessel proliferation. Several photoreactive drugs are being developed, but published results from clinical phase-III trials are only available for Verteporfin. Recently, the 2-year results were published at a symposium. The overall results showed that after 24 months of therapy had 47% of the treated patients a loss of vision of three reading lines (Snellen lines) or more, whereas corresponding number for the control group was 62%. Thus, 15% of the patients received benefit from the treatment. Thirteen percent of the patients experienced an improvement in visual acuity. Sub-group analysis indicated that beneficial effects were mainly confined to patients having predominantly "classic" lesions, of which 28% were treated with positive results. The therapy resulted in few adverse effects. Long term efficiency beyond 2-year of treatment is not known, and the therapy do not benefit patients with advanced disease. In Norway, approximately 800 new patients having mainly "classic" lesions are yearly eligible for the treatment. Possibly, these patients will need on average 3-4 and approximately 2 sessions during the first and second year of treatment, respectively. The report also contains simplified evaluations of cost-analyses and social consequences together with descriptions of alternative treatment regimens. It is advocated that many elderly have a reduced level of physical activity that benefits from adequate vision (reading etc.). Even with small therapeutic gains, improved vision could therefore be very important for these patients. The main conclusions are that photodynamic therapy is so far the most effective treatment for exudative age-related macular degeneration. The therapy is only effective on a subset of the patients. More data is needed on long-term efficiency before conclusions whether the therapy should be widely implemented or not. 3. Introduction Macular degeneration is a retinal disease involving the macula (yellow spot). Central in this area is a pit called the fovea, which is responsible for visual acuity. The illness affects two age groups: 1) A rarely seen and hereditary juvenile form, and 2) the age-related form mainly affecting people above 60 years and increasing in frequency with age. The underlying cause of macular degeneration is unknown. The exact number of people in Norway with the disease is uncertain, but estimates have been made that about 20% of the population above 85 years are more or less affected. Age-related macular degeneration (AMD) can be either nonexudative (dry) or exudative. The nonexudative form involves a variety of presentations and develops slowly over years with gradual visual impairment. The condition constitutes about 90% of all cases of macular degeneration, and lacks efficient treatment. It is important that patients with the dry form are regularly examined since the condition can progress to the more serious exudative form. Pá gina 59 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Patients having the exudative form rapidly undergo loss of their central vision. Small, but leaky and abnormal blood vessels form under the macula in a process called choroidal neovascularisation (CNV). These vessels constitute membranes, they leak fluid and may rupture. The result is scar formation and macular damage. Untreated the process will lead to marked visual impairment over a period of 3 – 24 months. Peripheral vision will be intact, but the ability for example, to read, drive cars and to recognise faces will be lost. The exudative form constitutes only 10% of the patients, but is responsible for about 90% of all cases of severe visual impairment in patients with age-related macular degeneration. This report deals with a new therapy for this, the most serious subform. Many therapies have been tried for age-related macular degeneration, but few have been effective. Despite an unknown pathogenesis, control of neovascularisation is important. This can be done with laser photocoagulation (using "hot" laser), however, this treatment has been shown also to destroy the light-sensitive cells in the retina and can only be used on lesions outside the fovea (that is, only about 10% of all patients with exudative form). The other 90% of the patients have subfoveal damage (see Figure 1) and can therefore not be treated with traditional laser. Thus, other treatment regimens have been tried including X-radiation, surgery, angiostatic drugs and photodynamic therapy (see Chapter 11). Figure 1(A): Fovea is centrally localised in the macula (circle). The localisation of CNV can be completely or partly covered by the fovea (B) or outside the fovea (C). Conventional laser can be used in alternative C. In B photodynamic therapy can be a therapeutic option. 4. Epidemiology The epidemiology of age-related macular degeneration has been poorly studied in Norway, and data must therefore be extrapolated from population studies in Europe, USA and Australia (1-3). The reported prevalences vary somewhat, but the differences can partly be explained with the different methods and criteria used in the studies. The incidence and prevalence in Norway, probably, do not differ strongly from that reported in these countries. The Beaver Dam Eye Study from USA (4) used their own classification system for the evaluation of retinal photographs and gave data for both prevalence and incidence. The study estimated that the prevalence of exudative age-related macular degeneration is 1.2% in people 43 – 86 years of age. The 5-year incidence for the same group was 0.6%. Prevalence correlated strongly with age increasing from 0.1% in people being 43-54 years and 7.5% for people over 75 years. In people older than 85 years the prevalence is about 20%. Extrapolating the data found in The Beaver Dam Eye Study to the Norwegian society (4.5 million inhabitants) gives a prevalence of 20 400 patients with exudative age-related macular degeneration in people older than 45 years (incidence about 2,000 new patient per year). Of these 2,000 about 40% would meet the criteria for photodynamic treatment, i.e., 800 new patients each year. 5. Norwegian participation in clinical research Haukeland Sykehus participates in a multi-center study together with eight European universities. The purpose is to investigate the prevalence of ARM and AMD (see dictionary) and to correlate the UV irradiation on the different latitudes, nutritional and antioxidative status. The study has recently begun and is expected to enrol about 5-6,000 subjects. It is co-ordinated by Prof. Fletcher, London School of Hygiene and Tropical Medicine, and data collection and analyses will be finished by 2002/2003. Presently in Norway three hospitals are involved in photodynamic trials (VIP- and TAP- studies, see dictionary). These are The National Hospital, Vestfold County Hospital and Vest-Agder County Hospital. The trials are partly funded by a drug company (Ciba Vision). 6. Photodynamic treatment of subfoveal CNV The premise of photodynamic therapy is to inject an inactive drug (prodrug) which accumulates in diseased tissues. Irradiation with light of a specific wavelength activates the drug, and a selective release of free radicals leads to local cellular damage. The principle is known from other medical specialities including cancer treatment. Pá gina 60 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Table 1 summarises the different drugs in clinical trials and which clinical phase the drugs have reached (5): Table 1 Verteporfin Visudyne 690nm, 150 J/cm2 2-year data from phase III clinical studies known SnET2 Purlytin 664nm, 36-126 J/cm2 Currently in phase III trial Lutetium taxaphyrin Lutex/Optrin 732nm, 75-125 J/cm2 Currently in phase I/II trial Mono-L-aspartyl chori- Npe6 664nm, 2,3-7,5 J/ cm2 In preclinical studies ne e-6 ATX-S10 670nm, 7,4 J/ cm2 In preclinical studies In case of photodynamic treatment of macular degeneration the drug is injected intravenously, and the drug concentrates in endothelial cells in the CNV. After a washout-time the CNV is illuminated with nonthermal laser light. As opposed to traditional "hot" laser, nonthermal light does not result in retinal damage. The light-activated drug selectively destroys CNV without harming the overlying sensory retina, expectantly, to reduce vascular leakage and to stabilise or increase visual acuity. Initial experience has shown that CNV can reappear, and that the treatment must be repeated several times per year. Adverse effects Adverse effects have been best studied and published for Verteporfin (6). Extravasal injection of Verteporfin will lead to serious and painful skin lesions including necrosis. Such effects are difficult to avoid completely, but the incidence can be kept to a minimum by maintaining strict to guidelines and thorough training. Transient visual disturbances and back pain can be experienced by some during injection. Allergic reactions are rarely seen for Verteporfin (6). Clinical phase III-studies Twelve-month data from the TAP–study with subgroup analyses were published October 1999 (6). Two-year results from this study were presented at The Association for Research in Vision and Ophthalmology (ARVO) yearly conference in Florida held in May this year (7). Notably, the results sited below have not been subjected to publication in international peer-review journals. A total of 403 patients with age-related macular degeneration were treated with photodynamic therapy using Verteporfin and compared to 207 sham treated placebo patients. Mean age of participating patients was 75 years and the groups were comparable at the start of treatment. During the first year the patients needed 3.4 treatments, reducing in frequency to 2.1 treatments in the second year. The overall results showed that after 24 months 47% of the treated patients had a visual loss of three lines or more of best corrected distant visual acuity measured on a standard visual acuity chart, whereas the corresponding numbers from the control group was 62%. Thus, 15% of the patients received benefit from the treatment. Thirteen percent of the treated patients had improvement in their visual acuity. The results showed a significant difference of the two groups in favour of active treatment. The subgroup that showed best therapeutic response had mainly classic lesions (Figure 2). Twenty-eight percent of these patients received beneficial treatment effects. It is not known at the present stage if the treatment permanently will stop disease progression thereby resulting in better vision outcome compared to no treatment. Only about 40% of the patients with exudative age-related macular degeneration have predominantly classic CNVs. The other 60% have fluorescein angiograms characterised as predominantly "occult" lesions. These patients receive no benefit from the treatment and in reality, still lack a therapeutic option. Figure 2 illustrates the different types of CNV lesions. The 1-year results from another and related study (VIP-study) were released in May this year. Similarly, the results indicate that patients with only occult lesions do not benefit from the treatment (8). Figure 2 Figure 2 shows fluorescein angiographic subtypes of different CNV types: classic, occult and mixed lesions containing both classic and occult components. The term "predominantly classic" Pá gina 61 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 is used to describe the latter subtype if the classic component is equal to or greater than 50% of the area of the entire CNV lesion. 7. Equipment, competence and resources needed in Norway Ophthalmologists diagnose age-related macular degeneration after clinical examination. For this the ophthalmologists usually have all necessary equipment. Opticians meet potential patients with age-related macular degeneration in their daily practice and evaluate their visual function. However, they do not have the expertise to diagnose and select patients for treatment, but they can be an important source of referral to specialists. Selection of eligible patients requires standard diagnostic equipment in addition to camera to perform fluorescein angiograms (= investigations of the blood circulation) of the eye retina. Laser: Standard laser employed in other eye treatments cannot be used for photodynamic treatment. Each photodynamic drug requires a special wavelength generated by dedicated lasers. These lasers must be bought or leased, and a 689 nm laser costs approximately (Nov. 1999): NOK 101,000 (VAT excluded). Competence: There will be a need to increase the interest for diagnostic services and therapy of macular diseases. However, with the availability of new therapeutic options this interest might be stimulated. The treatment can be performed in an outpatient setting, and can therefore be performed by qualified ophthalmologists outside hospitals. Economic incentives will also determine whether this therapeutic modality will be available outside hospitals. Resources: To perform necessary diagnosis and treatment in Norway there are 21 eye departments in public hospitals and 320 ophthalmologists. In addition there will be a need for personnel responsible for performing angiographies, intravenous drug administration, patient surveillance and laser treatment. Few eye departments have photographers in full-time positions. Each patient will need a photographic investigation of his or her fundus and fluorescein angiographic examination in addition to photodynamic treatment approximately every third month. Each examination/treatment will require about 2-4 hours spent by health care personnel. Drug cost will, however, represent the major part of the medical expenses (see below). 8. Organisational consequences There is still lacking long-term evidence (exceeding two years) proving that photodynamic therapy results in significantly better visual acuity compared to placebo. Until such evidence has been provided it would be natural to offer the treatment in a limited scale. If this treatment modality gives long-term benefits, it would be natural to offer the treatment and follow-up in all eye departments in the country comparable to other eye diseases. The treatment could also be offered by ophthalmologists outside hospitals. In hospitals photodynamic therapy would increase the demand for diagnostic services, and would thereby also influence the capacity of ophthalmologists and other departmental resources for traditional tasks. The diagnostic steps and principles of photodynamic therapy are not very different from other eye procedures, and the need for special training should be moderate. If photodynamic therapy should be offered widely, there will be a need to inform general practitioners and opticians. 9. Cost analyses, social consequences Exudative macular degeneration tapers off after 2-5 years if no treatment is given. In the end most patients have permanently lost their central vision (9). This loss creates a need for assistive devices (optical and electronoptical) and reduces the degree of independence in daily activities of the involved patients. Costs Present costs Patients with age-related macular degeneration have had limited therapeutic options, and most public expenses have been connected to medical consultations and assistive devices. Patient in the final phase of the illness will often need training and courses for blind people, home help or need to be institutionalised. Central for Assistive Devices in Oslo informs that patients with agerelated macular degeneration constitute about 95% of all patients that receive assistive devices for visual impairment, and that this probably is representative for the whole nation. Pá gina 62 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Patients with age-related macular degeneration need both optical devices (magnifying glasses, telescopes etc.) and electron optical devices (magnifying video-systems, reading machines). The National Insurance Institution informs that in 1998 about NOK 49.4 million was given in support for these kind of assistive devices, whereas NOK 57 million was given to the whole group of patients with visual handicaps. Electron optical devices, mainly magnifying video-systems constitutes about 80% of all expenses for this patient group (personal communication). Cost of treatment with photodynamic therapy Photodynamic therapy is a new modality and can lead to considerable changes in expenses in this patient group, which today only receives practical support. Of the therapeutic agents that today are in clinical trials, only Verteporfin is commercially available. Verteporfin is available in Norway only on named patient use, and a marketing authorisation has been submitted. Drug needed for each treatment costs about NOK 13,000 from the pharmacies. The initial results from the clinical trials show that each patient needs in average 5.5 treatments during the first two years of treatment (TAP-study). Table 2. Estimated drug expenses for the treatment of one eye with Verteporfin based on data from the TAP-study. 1. year 3.4 44,200 44,200 2. year 2.1 27,300 71,500 In addition, early costs of hospitals and personnel time are estimated to be NOK 5-10,000. Available data from the clinical trials do not allow more accurate calculation of treatment costs. The costs described above are calculated per eye. While age-related macular degeneration is often a bilateral disease, the disease progression rarely follows the same time course in both eyes. The majority of the patients will require separate treatment for each eye and the minority could have their eyes treated simultaneously at a reduced cost. We have not included the latter scenario into our calculations. The hospitals fund these treatment costs through ordinary financial channels (ISF/DRG 36). Corresponding RTV-funding (see dictionary) for ophthalmologist in private practice does not exist. With drug and personnel costs reaching about NOK 85,000 over a 2-year period few patients are able to pay for the treatment themselves. The yearly incidence in Norway is about 800 eligible patients available for photodynamic treatment. These patients will need in average 5.5 treatments during the first two years, i.e., 4,400 treatments, representing a yearly price of NOK 44 million in medical costs only. Drug costs dominate and changes in drug pricing will strongly influence overall costs. Social consequences As stipulated above the total treatment costs approximately NOK 85,000 per patient per eye during the first two years of treatment. In addition comes the continued need for assistive devices for people with reduced vision due to the disease, and the treatment will probably not result in overall savings. This is a group of patients at relatively advanced age, and the greatest health gain will be an increased quality of life experienced by the patients. Savings due to the new treatment are difficult to estimate. If photodynamic therapy saves visual acuity for longer times, overall savings may in the end be reached. Preliminary results are promising, and in the future the patients may need less home help and postponed institutionalisation. Quality of life A study of 86 elderly patients with age-related macular degeneration found that the illness had a negative influence on their quality of life, functional status and psychological welfare. The patients conducted several well-recognised tests (Quality of Well-being Scale, the Instrumental Activities of Daily Living Index, Self-rated General Health Status, Profile of Mood Scale), and the results showed a significant difference between the patients and a comparable group of patients without macular degeneration. The different quality of life parameters could be compared with chronic diseases such as rheumatoid artrithis and chronic obstructive lung disease (10). The greatest health gain achieved with photodynamic therapy is probably an increased quality of life. Patients with sustained vision have increased chances to manage themselves without help for a longer period of time. Collection of quality of life data is ongoing in several clinical stud- Pá gina 63 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 ies, but the results have not yet been published. Thus, we have no results that can be expressed in QALYs. High treatment costs implicate that social costs, ethics and the treatments long-term efficiencies are included in an overall assessment. 10. Ethical considerations Every treatment of age-related macular degeneration raises difficult questions concerning allocation of resources, because the outcomes, both concerning health and quality of life, are limited by the advanced age of the patients. Several of the patients treated with photodynamic therapy will die due to natural causes during a relative short time span. It follows that despite the method being proven effective, the involved health economics can be difficult to compare to other treatments used in health care. One ethical consideration is to measure the value to preserve vision in an older patient. How does loss of vision influence the quality of life of elderly people? On one hand it can be advocated that loss of vision in the elderly is more difficult to handle than corresponding loss among younger persons. Elderly patients may have major problems with adjustments and often the health care given to this group isn’t as good as that given to younger patients. Loss of vision is an important reason for elderly to abandon their own housing and seek institutionalisation, and gives a loss in social function and status (and thereby resulting in considerable increased social costs). On the other hand, age-related vision loss can be advocated to be generally less straining because the elderly already have a reduced level of physical activity. The argument, however, is not very good since many elderly perform activities dependent on reasonable vision (e.g., reading). The short expected life span of the patients should therefore not be too strongly emphasised when resources are to be allocated to the treatment. The yield gained by the treatment is so important that the patients should get as much as possible out of it, in spite of the fact that the improvement might be incremental. Another approach for performing ethical considerations could be to do a real cost-utility analysis. It might be possible that treatment of age-related macular degeneration does not end up being worse than other treatments used in health care. Loss of vision leads to a considerable loss in quality of life. Elderly cannot be expected to adjust to the situation, thereby causing a permanent loss in quality of life. Therefore, in the terms of e.g., QALYs, there will be a considerable gain in QALYs each year that loss of vision is avoided. In a calculation of QALY per capital invested, probably the short-term result of the treatment (partly due to the need for repeated treatments, partly to short expected life span) could probably be compensated. Another problem related to theoretical decision-making that also has ethical components, raised by new treatments for age-related macular degeneration is how to handle the uncertainty regarding the long-term efficiency beyond two years. This is especially emphasised by the fact that the treatment requires special apparatuses. However, even if the effect should be limited to a 2-year postponement of the disease, would this result in a rather important health gain for the patients? The question is therefore: "Should the treatment be implemented despite the uncertainties regarding the long-term effects?" If "yes", the uncertainties regarding the long-term effects consequently are of no concern. If "no", an approach could be to make estimates of duration and magnitude of the possible effects. The probability of these estimates should also be assessed. The estimates could then be used in modelling to help decision-making. 11. Alternative treatments Conventional laser treatments Previously, only conventional laser treatment has been the only proven therapeutic modality for exudative macular degeneration. However, the Macular Photocoagulation Study, MPS (11) showed that this treatment could only be used by 15% of the patients having small and well confined lesion. Of these 15% nearly one-half of them have lesions covered by the fovea and where the use of conventional laser would result in immediate reduction in vision. Of those patients that originally have lesions outside the fovea, above 50% experience recurrence after the first treatment. These recurrences often have a subfoveal location, and repeated laser treatment would thus lead to further reduction of vision. Pá gina 64 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Other treatment modalities In addition to photodynamic therapy several other treatment modalities have been tried. Previous, but small studies have been promising regarding both radiation therapy and treatment with interferon alfa-2a. Recently, the results from larger, prospectively randomised studies were published, but unfortunately, without showing positive effects (12,13). Transpupillary thermotherapy (TTT) is a new treatment under investigation for occult subfoveal membranes (14). The latter technique is now under evaluation at The National Hospital, and it is too early to draw conclusions about clinical effects. Advanced retinal surgery gives possibilities today to remove CNV and coagulated tissues beneath the retina. In case of age-related macular degeneration the CNV is located under the pigment epithelium, a cell-layer necessary for the function of the photoreceptors. When the membrane is removed, concurrently the pigment epithelium is removed, and this leads to an inferior result of the surgery. Several clinics perform experimental transplantation of pigment epithelium (15). In addition to submacular surgery there are ongoing pilot studies where the retina is removed (translocation surgery) resulting in CNV-membranes that originally were located subfoveally. After translocation the membranes can be treated with conventional laser. Coagulation in CNV can also be treated with injection of gas and anticoagulative drugs given by intraocular administration (16). The patient can thereafter lie in a face down position that allows the gas to press the blood away from the macula to prevent central vision loss. Approaches to inhibit angiogenesis are also investigated. Animal studies with angiostatic substances e.g., thalidomide have been shown to inhibit vessel growth (17). Age-related macular degeneration has probably a multifactorial causality. Theories have been proposed that prophylactic supplementation of antioxidants could prevent the disease. These theories could be difficult to assess since this would require very large and long-lasting studies. One such study has been ongoing for several years, and the results have not yet been published (18). Soft drusen (ARM) represent retinal changes that increase the risk exudative age-related macular degeneration. These drusen are often reduced in number and area after laser treatment (19). Studies are underway to investigate if such treatment also reduce the risk for developing CNV. 12. Indication for photodynamic treatment in other eye diseases Pathological blood vessels can also be formed in the eye fundus in diseases other than agerelated macular degeneration. Examples of such conditions are severe myopia, ocular histoplasmosis syndrome, "angioid streaks" and von Hippel Lindau syndrome. It is possible that photodynamic treatment could be effective since the pathological blood vessels are both limited and localised. Several studies are ongoing to investigate the effectiveness of photodynamic therapy in these conditions. 13. Conclusions • Photodynamic therapy is so far the most effective treatment described for exudative subfoveal age-related macular degeneration. • In cases where the macular lesions are located outside the fovea, conventional laser should still be the treatment of choice. • Photodynamic therapy only works in the early stages of the illness. • The therapy is very costly and requires careful selection of the patients. • More data is needed on long-term efficiency before conclusions whether the therapy should be widely implemented or not. 1. References 1. Vingerling JR, Dielemans I, Hofman A, Grobbee DE, Hijmering M, Kramer CF, de Jong PT. The prevalence of age-related maculopa- Pá gina 65 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 thy in the Rotterdam Study. Ophthalmology. 1995;102(2):205-10. 2. Klein R, Klein BE, Moss SE, Linton KL. The Beaver Dam Eye Study. Retinopathy in adults with newly discovered and previously diagnosed diabetes mellitus. Ophthalmology. 1992;99(1):58-62. 3. Mitchell P, Smith W, Attebo K, Wang JJ. Prevalence of age-related maculopathy in Australia. The Blue Mountains Eye Study. Ophthalmology. 1995;102(10):1450-60. 4. Klein R, Klein BE, Linton KL. Prevalence of age-related maculopathy. The Beaver Dam Eye Study. Ophthalmology. 1992;99(6):93343. 5. Blumenkranz, M.S. Status of photodynamic drugs and photodynamic trials, Vitreoretinal update/subspeciality day. San Francisco. 1999; Amer.Acad.Ophthalmol. 6. Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin: one-year results of 2 randomized clinical trials--TAP report. Treatment of age-related macular degeneration with photodynamic therapy (TAP) Study Group. Arch.Ophthalmol. 1999;117(10):1329-45. 7. Blumenkranz, M. S. TAP 24-month topline data. 5-3-2000. Internet Communication: http://www.visudyne.wwwebposium.com/pw/html/ index.html 8. Singerman, L. VIP 12-month topline data. 5-3-2000 Internet Communication: http://www.visudyne.wwwebposium.com/pw/html/index.html 9. Fine SL, Berger JW, Maguire MG, Ho AC. Age-related macular degeneration. N.Engl.J.Med.2000.Feb.17.;342.(7.):483.-92. 342(7):483-92. 10. Williams RA, Brody BL, Thomas RG, Kaplan RM, Brown SI. The psychosocial impact of macular degeneration. Arch Ophthalmol 1998;116(4):514-20. 11. Argon laser photocoagulation for neovascular maculopathy. Fiveyear results from randomized clinical trials. Macular Photocoagulation Study Group. Arch.Ophthalmol. 1991;109(8):1109-14. 12. Interferon alfa-2a is ineffective for patients with choroidal neovascularization secondary to age-related macular degeneration. Results of a prospective randomized placebo-controlled clinical trial. Pharmacological Therapy for Macular Degeneration Study Group. Arch.Ophthalmol. 1997;115(7):865-72. 13. A prospective, randomized, double-masked trial on radiation therapy for neovascular age-related macular degeneration (RAD Study). Radiation Therapy for Age-related Macular Degeneration. Ophthalmology 1999;106(12):2239-47. 14. Reichel E, Berrocal AM, Ip M, Kroll AJ, Desai V, Duker JS, Puliafito CA. Transpupillary thermotherapy of occult subfoveal chor- Pá gina 66 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 oidal neovascularization in patients with age-related macular degeneration. Ophthalmology 1999;106(10):1908-14. 15. Crafoord, S. Experimental transplantation of retinal and iris pigment epithelial cells into the subretinal space. Linköping University Medical Dissertations No. 629 2000; Linköping University; 16. Hassan AS, Johnson MW, Schneiderman TE, Regillo CD, Tornambe PE, Poliner LS, Blodi BA, Elner SG. Management of submacular hemorrhage with intravitreous tissue plasminogen activator injection and pneumatic displacement. Ophthalmology 1999;106(10):1900-6. 17. D'Amato RJ, Loughnan MS, Flynn E, Folkman J. Thalidomide is an inhibitor of angiogenesis. Proc.Natl.Acad.Sci.U.S.A. 1994;91(9):4082-5. 18. VandenLangenberg GM, Mares-Perlman JA, Klein R, Klein BE, Brady WE, Palta M. Associations between antioxidant and zinc intake and the 5-year incidence of early age-related maculopathy in the Beaver Dam Eye Study. Am J Epidemiol. 1998;148(2):204-14. 19. Frennesson IC, Nilsson SE. Effects of argon (green) laser treatment of soft drusen in early age-related maculopathy: a 6 month prospective study. Br.J Ophthalmol 1995;79(10):905-9. Senter for medisinsk metodevurdering (SMM) The Norwegian Centre for Health Technology Assessment, SINTEF Unimed, Forskningsveien 1, Postboks 124 Blindern, 0314 OSLO Direktørr Berit Mørland Informasjonskonsulent Berit Kolberg Rossiné Tlf: 47 22 06 79 61 Faks: 47 22 06 79 79 E-post: [email protected] Pá gina 67 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 ANEXO 6 Pá gina 68 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 69 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 70 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 71 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 72 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 73 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 74 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 75 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 76 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 77 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 78 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 79 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 80 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 81 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 82 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 ANEXO 7 Pá gina 83 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 84 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 85 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 86 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 87 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 88 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 89 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 ANEXO 8 Pá gina 90 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Photodynamic therapy for neovascular age-related macular degeneration Wormald R, Evans J, Smeeth L This review should be cited as: Wormald R, Evans J, Smeeth L. Photodynamic therapy for neovascular age-related macular degeneration (Cochrane Review). In: The Cochrane Library, Issue 1, 2001. Oxford: Update Software. A substantive amendment to this systematic review was last made on 22 February 2000. Cochrane reviews are regularly checked and updated if necessary. Background: In neovascular age-related macular degeneration, new vessels grow under the retina, distorting vision and leading to scarring. This is further exacerbated if the blood vessels leak. Photodynamic therapy, originally used in cancer treatment, has been investigated as a way to treat the neovascular membranes without affecting the retina. Objectives: The aim of this review is to examine the evidence for the safety and effectiveness of photodynamic therapy in the treatment of neovascular age-related macular degeneration. Search strategy: We searched for trials in the Cochrane Eyes and Vision Group specialised register (available in CENTRAL), the Cochrane Controlled Trials Register - CENTRAL, MEDLINE and EMBASE. We used the Science Citation Index to search for reports that cited identified relevant study reports. We contacted experts in the field for further trials information, and we searched the reference lists of identified relevant studies for further trial reports. Selection criteria: We included randomised trials of photodynamic therapy in people with choroidal neovascularisation due to age-related macular degeneration. Data collection and analysis: Two reviewers extracted the data independently. Meta analysis was not performed. Main results: One published trial was identified. Outcome data were available at 12 months after the first treatment. Patients received an average of 3.7 treatments. The relative risk of losing three or more lines of visual acuity at 12 months comparing the intervention with the control group was 0.72 (95% confidence interval 0.61 to 0.86). The relative risk of losing six or more lines of visual acuity at 12 months comparing the intervention Pá gina 91 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 with the control group was 0.62 (95% confidence interval 0.44 to 0.87). Subgroup analyses suggest that the benefits may be confined to people with no occult choroidal neovascularisation. Reviewers' conclusions: Photodynamic therapy in people with classic choroidal neovascularisation due to age-related macular degeneration is effective in preventing visual loss. This evidence is drawn from a subgroup analysis of 143 participants in one trial. Outcomes and potential adverse effects of this treatment should be monitored closely. There is no evidence that photodynamic therapy is beneficial for people with evidence of occult choroidal neovascularisation. These people should be offered treatment in the context of a randomised trial. Background Age-related macular degeneration (ARMD) is a disease affecting the macula, the central area of the retina. The disease is defined as degeneration of the macula in older people (aged over 50) with no other apparent cause for the degeneration. There are several signs in the retina that are associated with increasing age and increased risk of developing age-related macular degeneration. These signs, known as age-related maculopathy, include the presence of drusen (yellow spots maculopathy, include the presence of drusen (yellow spots beneath the retina) and pigmentary disturbance. In general age-related maculopathy is not associated with visual loss. Some people with age-related maculopathy will go on to develop age-related macular degeneration. There are two main types of age-related macular degeneration. In geographic atrophy or dry age-related macular degeneration, the retinal pigment epithelium is lost completely in localised areas. In neovascular or wet age-related macular degeneration, sub-retinal neovascular membranes (new blood vessels) develop beneath the retina. These are associated with scarring of the retina that affects vision. The new vessels can leak, causing haemorrhage that leads to larger scars, or macular oedema and significant loss of vision. This review is concerned with treatment for neovascular age-related macular degeneration. Subretinal neovascular membranes are defined as classic or occult according to their appearance on fluorescein angiography, in which fluorescent dye is injected intravenously and imaged as it passes through the blood vessels of the eye. Classic membranes are clearly delineated and leak fluorescein uniformly. Occult membranes are often hidden or their extent is hard to delineate, and fluorescein leakage is patchy. Some lesions may have classic and occult components. Pá gina 92 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Trials have shown that early laser photocoagulation of classic extra-foveal membranes (those not directly underneath the fovea at the centre of the macula) could delay the loss of vision in a small number of patients (MPS 1994). However, most patients present with sub-foveal membranes, and whilst photocoagulation can limit the extent of the subsequent visual loss, it causes immediate loss of central vision due to the concurrent destruction of the overlying retina. Photodynamic therapy, originally used in the treatment of cancer, has been investigated as a way to treat the neovascular membranes without affecting the retina. Photoreactive chemicals are injected into the patient and irradiated with light as they pass through the neovascular membranes. This light is strong enough to activate the chemicals, causing them to emit free radicals that destroy the blood vessels, but is not strong enough to cause damage to the overlying retina. Objectives The aim of this review is to examine the evidence for the safety and effectiveness of photodynamic therapy in the treatment of neovascular age-related macular degeneration. Criteria for considering studies for this review Types of studies We included randomised controlled trials. Types of participants Participants were people with neovascular age-related macular degeneration as defined by the study investigators. Types of intervention We included any study in which photodynamic therapy was compared to another treatment, placebo or no treatment. Types of outcome measures Pá gina 93 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 We included the following outcomes: (1) (2) (3) (4) prevention of visual loss new vessel growth quality of life measures any adverse outcomes as reported in trials We used the following definitions: Visual loss: Any well-defined outcome based on visual acuity was used depending on the way in which authors presented trial data. Other validated measures of visual loss, such as contrast sensitivity, were used where available. Quality of life: Any validated measurement scale which aims to measure the impact of visual function loss on quality of life of participants. Search strategy for identification of studies See: Collaborative Review Group search strategy We searched for trials in the Cochrane Controlled Trials Register - CENTRAL, the Cochrane Eyes and Vision Group specialised register (available in the CENTRAL), MEDLINE and EMBASE. We used the following strategy to search the CENTRAL Issue 4 1999: #1 MACULAR-DEGENERATION:ME #2 RETINAL-DEGENERATION:ME #3 #3 NEOVASCULARIZATION-PATHOLOGIC*:ME #4 (MACULA or MACULAR) or RETINA or RETINAL or CHOROID or CHOROIDAL near (DEGENERATION or NEOVASCULARIZATION)) #5 MACULOPATHY #6 #1 or #2 or #3)or #4 or #5 #7 PHOTOCHEMOTHERAPY*:ME #8 PHOTOSENSITIZING-AGENTS*:ME #9 (PHOTOSENSITIZING or PHOTOSENSITISING) or PHOTODYNAMIC or PDT or VERTEPORFIN or VISUDYNE #10 #7 or #8 or #9 #11 #6 and #10 We used the following strategy to search Medline 1966 to October 1999: Pá gina 94 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 SilverPlatterASCII 3.0DOSNSelected Databases #1 "MACULAR-DEGENERATION"/ all subheadings #2 "RETINAL-DEGENERATION"/ all subheadings #3 "CHOROIDAL-NEOVASCULARIZATION"/ all subheadings #4 (MACUL* or RETINA* or CHOROID*) near (DEGENER* or NEOVASC*) in TI,AB #5 MACULOPATHY in TI,AB #6 #1 or #2 or #3 or #4 or #5 #7 explode "PHOTOCHEMOTHERAPY"/ all subheadings #8 explode "PHOTOSENSITIZING-AGENTS"/ all subheadings #9 (PHOTOSENSITI?ING?AGENTS or 'PHOTOSENSITI?ING AGENTS' or PORPHYRIN* or BENZOPORPHYRIN) in NM,TI,AB #10 (PHOTODYNAMIC or PDT) in TI,AB #11 VERTEPORFIN or VISUDYNE in TI,AB #12 #7 or #8 or #9 or #10 or #11 #13 #6 and #12 We used the following strategy to search Embase 1980 to September 1999: SilverPlatterASCII 3.0DOSNSelected Databases #1 explode "RETINA-MACULA-DEGENERATION"/ all subheadings #2 "RETINA-DEGENERATION"/ all subheadings #3 "NEOVASCULARIZATION-(PATHOLOGY)"/ all subheadings #4 "SUBRETINAL-NEOVASCULARIZATION"/ all subheadings #5 (MACUL* or RETINA* or CHOROID*) near (DEGENER* or NEOVASC*) in TI,AB #6 MACULOPATHY in TI,AB #7 #1 or #2 or #3 or #4 or #5 or #6 #8 "PHOTODYNAMIC-THERAPY"/ all subheadings #9 explode "PHOTOSENSITIZING-AGENT"/ all subheadings #10 (PHOTODYNAMIC or PDT) in TI,AB #11 (PHOTOSENSITI?ING AGENT* or VERTEPORFIN or VISUDYNE) in RN,TI,AB #12 #8 or #9 or #10 or #11 #13 #7 and #12 We used the Science Citation Index to search for reports that cited identified relevant study reports. We contacted experts in the field for information about further trials, and we searched the reference lists of identified relevant studies for further trial reports. Methods of the review Selection of trials Two reviewers independently scanned the titles and abstracts resulting from the electronic searches. We obtained full copies of all potentially or definitely relevant articles. Two reviewers assessed the full copies according to the 'Criteria for Pá gina 95 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 considering studies for this review'. Only articles meeting these criteria were assessed for quality. Assessment of methodological quality Two reviewers independently assessed study quality according to methods set out in the Section 6 of the Cochrane Reviewer's Handbook. Reviewers were not masked to any trial details during the assessment. Four parameters of quality were considered: allocation concealment and method of allocation to treatment, masking of providers and recipients of care, masking of outcome assessment, and completeness of follow-up. Each parameter of trial quality was graded: A - adequate; B - unclear; C - inadequate. Disagreement between the reviewers on assessments was resolved by discussion. We contacted the trial authors for clarification on any parameter graded B - unclear, and we excluded any trial scoring C - inadequate on allocation concealment. We constructed an overall score of quality for each trial as follows: 1 - Low risk of bias - All parameters graded A - adequate 2 - Moderate risk of bias - One parameter graded C - inadequate 3 - High risk of bias - Two or more parameters graded C inadequate Data collection Two reviewers independently extracted data using a form developed for use by the Cochrane Eyes and Vision Group (available from the editorial base). We resolved discrepancies by discussion. Two reviewers independently entered data into RevMan 4.0.4 and we checked any inconsistencies between the two against the study report. Data synthesis Our original data analysis plan was to Our original data analysis plan was to summarise data from studies collecting similar outcome measures with similar follow-up times using the Peto method, after testing for heterogeneity between trial results using a standard chi-square test. At present only one trial is included in this review so no data synthesis was necessary. The main outcome analysed, loss of 3 or more lines of visual acuity at 12 months follow-up, occurred relatively frequently in the trial cohort. The odds ratio, therefore, does not approximate to the relative risk. We present relative risks in this review. We planned to conduct sensitivity analyses to determine the effect of excluding studies given an overall grade of 3 - high risk of bias but this has not been necessary to date. Description of studies The electronic searches identified 76 reports. We found one Pá gina 96 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 randomised controlled trial (TAP 1). This multicentre study investigated the safety and effectiveness of verteporfin (Visudyne; CIBA Vision Corp, Dulth,GA) and was conducted in 22 ophthalmology practices in Europe and North America. Participants were people with subfoveal choroidal neovascularisation (CNV) caused by age-related macular degeneration. The majority of participants were white (98%) with a mean age of 75 years. Verteporfin (six milligrams per square meter of body surface area) was compared to placebo (5% dextrose in water) administered via intravenous infusion of 30 millilitres over 10 minutes. This was followed after 15 minutes by application of eighty three seconds of laser light at 689 nm delivered 50 Joules per square centimetre at an intensity of 600 mW/cm squared using a spot size with a diameter 1000 microns larger than the greatest linear dimension of the CNV lesion. Participants in the trial were reviewed every three months when visual acuity and repeat fluorescein angiography performed. If the trial surgeon judged a recurrence of the membrane to be present or a persistence of the previous lesion, then repeat treatment was undertaken. In the phase 1 and 2 studies, it was concluded that up to five treatments were necessary to stabilise the situation (Miller 1999; Schmidt-Erfurth 1999). A mean of 3.4 treatments were delivered to the treatment group and 3.7 to the controls. TAP 1 was originally devised as two concurrent trials in order to comply with regulatory agency requirements. The study protocols were identical. Ten of the clinical centres were assigned to study A and 12 to study B. As the results of the trials were similar and the investigators analysed and presented the data as one trial, we have also assessed it as one trial. Methodological quality TAP 1 was a high quality study. Allocation of treatment group was by opaque serially numbered sealed envelopes. The baseline characteristics of the participants by treatment group were published. The groups were well balanced with respect to a variety of demographic and clinical variables. Only one eye per person was treated. Reasonable attempts were made to mask the ophthalmologist, patient, vision examiner and Photograph Reading Center Personnel. As verteporfin and placebo were different colours (green versus colourless) the solutions and the intravenous tubing were covered with foil. The fundus appearance does not change during treatment to indicate whether verteporfin or placebo had been infused. There is no other physical evidence of treatment as verteporfin dye is excreted in the faeces and does not cause any colour change. Nor Pá gina 97 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 does it alter the colour of the skin or urine so that it was unlikely the patient was aware of their treatment or control status. The study investigators reported two instances where the patients were unmasked having noted a green solution and a further four cases where the ophthalmologists were unmasked. Rates of follow-up were high (94%) and were similar between the two treatment groups. The analysis was intention-to-treat and subgroup analyses were planned a priori. Results The realistic aim of photodynamic therapy is to slow progression of Age related macular degeneration (ARMD), not to produce normal vision. Outcomes are therefore expressed as risks of a poor outcome, rather than as improvements in vision. All results refer to the TAP 1 study. The relative risk of losing three or more lines of visual acuity at 12 months comparing the intervention with the control group was 0.72 (95% confidence interval 0.61 to 0.86). The relative risk reduction was therefore 0.28 (95% confidence interval 0.14 to 0.39). The relative risk of losing six or more lines of visual acuity at 12 months comparing the intervention with the control group was 0.62 (95% confidence interval 0.44 to 0.87). The relative risk reduction was therefore 0.38 (95% confidence interval 0.13 to 0.56). The mean number of lines of vision lost at 12 months was 2.2 in the intervention group and 3.5 in the control group. The difference was 1.3 with fewer lines lost in the intervention group. The P value for the difference in the mean number of lines lost was given in the trial report as P <0.001 (Wilcoxon rank sum test). The standard deviations for the mean numbers of lines lost were not given in the published report and we therefore could not calculate a confidence interval. We hope to include this in a future version of this review. Subgroup analyses Subgroup analyses were specified a priori (Bressler N, personal communication). Outcome data for these subgroups are only available for the outcome 'risk of losing 3 or more lines'. The proportion of the lesion comprised of classic choroidal neovascularisation (CNV) was estimated as 0%, greater than 0% but less than 50% and greater than 50%. The proportion was unknown in four participants (three in the treatment group and one in the control group). The sub-group analysis was therefore based on a total of 399 eyes. The relative risks in these three groups of Pá gina 98 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 losing three or more lines of visual acuity at 12 months comparing the intervention with the control group were: 0.54 for 0% CNV; 0.99 for greater than 0% but less than 50% CNV and 0.54 for greater than 50%. These results suggest there was a reduction in the risk of loss of vision when classic CNV was absent or when greater than 50% of the lesion was comprised of classic CNV. However there was no reduction in risk when between 0% and 50% of the lesion was comprised of classic CNV. The test for effect modification between these three sub-groups was highly significant (chi-squared 10.74, 2 degrees of freedom, P <0.001). The inconsistencies in these results are discussed below. The other subgroup analysis was undertaken on the basis of the presence or absence of occult CNV. The relative risks of losing three or more lines of visual acuity at 12 months comparing the intervention with the control group were 0.90 if occult CNV was present (95% confidence interval 0.73 to 1.11) and 0.34 if occult CNV was absent (95% confidence interval 0.22 to 0.51). The test for effect modification between these two subgroups was highly significant (chi-squared 17.63, 1 degree of freedom, P <0.001). The 95% confidence intervals for these two sub-groups do not overlap, nor do the 99% confidence intervals. Numbers needed to treat We calculated the numbers needed to treat (NNTs) to prevent one person losing three or more lines and, where possible, one person losing six or more lines of vision at 12 months. These NNTs are derived from the study population, that is, people with subfoveal CNV and a baseline visual acuity of between 20/40 and 20/200. They refer to an average of 3.4 treatments of photodynamic therapy using verteporfin over a 12 month period. The NNT to prevent one person losing three or more lines of vision was 6.7 (95% confidence interval 4.3 to 14.3). The NNT to prevent one person losing six or more lines of vision was 11.1 (95% confidence interval 6.3 to 50). Because of the inconsistencies in the results of subgroup analysis for the proportion of the lesion comprised of classic CNV, we did not classic CNV, we did not calculate NNTs for these subgroups. For the subgroup analysis according to the presence or absence of occult CNV, the NNTs are as follows. The NNT to prevent one person with occult CNV present losing three or more lines of vision was 20 (95% confidence interval number needed to benefit 7.1 to infinity to number needed to harm 20). The NNT to prevent one person with no occult CNV present losing three or more lines of vision was two (95% confidence interval 1.6 to 3.3). Summary of analyses MetaView: Tables and Figures The figures and graphs in Cochrane Reviews display the Peto Odds Ratio and the Weighted Mean Difference by default. These are not always the methods used by reviewers when combining data in their review. You should check the text of the review for a description Pá gina 99 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 of the statistical methods used. Discussion Age related macular degeneration is the most common cause of irreversible visual impairment in Western countries and the population burden of the disease is increasing as the population ages. Its incidence increases steeply after the age of 70 years, but it also occurs in younger age groups and it is probably among the most common causes of sight loss in people in their 50's and 60's. Its precise cause is unknown but both genetic and environmental factors are thought to be relevant. The absence to date of any effective treatment (except for the few in whom laser photocoagulation works) means that there will be intense interest in photodynamic therapy for the many millions of sufferers of the disease worldwide. Unfortunately, photodynamic therapy, like photocoagulation, can only be effective during the proliferative stage of the disease while the neovascular process is active. It cannot have any effect once sight is lost and the scarring process is complete. Therefore, like so many other degenerative processes of the neuroretina, once the damage is done, nothing can be done to restore function. Most sufferers of the condition have established sight loss and for these, the publicity surrounding the launch of Visudyne (verteporfin) will have raised false hopes. Nevertheless, the evidence presented in this review from the only trial so far reported looks promising. A key question is how long the effect of treatment will last and whether repeated treatments would be required in the longer term. Important information on this is awaited from the TAP studies and from others. Another important issue is how many presenting patients will benefit or be treatable. Quite apart from the problem of accessing specialist services in time is the question of the proportion of lesions that will actually be treatable. The evidence reported here clearly suggests that purely 'classic' neovascular membranes do well. However when occult neovascular membranes are present, then the outcome is much less certain and indeed, there is no evidence of the treatment being effective in this circumstance. 'Occult' vessels mean that the extent of the membrane cannot be clearly defined and so it is not surprising that treatment is found to be less effective simply because the laser energy cannot be reliably aimed at all of the membrane. We are not told in the available reports the extent to which clinicians and indeed the trial reading centre are able to agree about the subgroup classification of 'classic' or 'occult' lesions. It is likely that there is much variation in opinion on this. The necessary skill to report on fluorescein angiograms and recognise different lesion types is highly refined. Most experts assert that the stereo images are required to be able to locate the position in depth of staining or fluorescein leaks. Stereophotography requires either a Pá gina 100 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 dedicated camera equipped to take simultaneous stereo images or a skilled photographer who takes sequential images slightly laterally displaced from one another providing a non-simultaneous or pseudo-stereo image. The natural history of the growth of subretinal The natural history of the growth of subretinal membranes varies from individual to individual. They may be aggressive and rapidly growing or indolent. This is the kind of individual factor that will influence the likelihood of a patient being in a position to benefit from this treatment. The trial report does not comment on the proportion of patients presenting to the trial centres that had treatable lesions. The verbal estimate from one trialist was approximately 25% and of another expert, between 5 and 7%. This is of crucial importance in estimating the impact of this new treatment on health care budgets. The first subgroup analysis (presence or absence of occult choroidal neovascularisation (CNV)) provides some pointers to which people will benefit from treatment, although any conclusions can only be tentative. The effect of treatment on people with occult CNV present was small and did not approach statistical significance. There appeared to be a far greater beneficial effect in people with no occult CNV present. However this finding was based on a total of only 143 eyes (94 in the treatment group and 49 in the control group). There is a need for great caution in interpreting a result based on this relatively small subgroup. The second subgroup analysis (percentage of lesion comprised of classic CNV) produced a somewhat surprising result. Whilst it is difficult to think of a good biological explanation for the observed results, there are two likely explanations for the inconsistent results observed. Firstly the effects observed in the subgroups could be a statistical artefact (Yusuf 1991). The following factors could have contributed to this: the relatively small numbers in the three subgroups; the multiple testing inherent in such subgroup analyses; and the fact that even though the subgroup analysis was specified a priori, the trial was not specifically powered to explore effects in these subgroups. Another explanation for the observed subgroup effects could be misclassification bias. As discussed above, determining the percentage of a lesion that is composed of classic CNV is unlikely to be an exact science. Inter or intra-observer variation could have contributed to the somewhat puzzling results obtained for the subgroup analysis based on the percentage of the lesion comprised of classic CNV. For example, some people with a small amount of classic CNV (between 0% and 50%) could have been erroneously judged to have no classic CNV or vice-versa. Because of the relatively small numbers in the subgroups, misclassification resulting in a different outcome would have been required in only a small number of people to explain the inconsistencies observed. In the 0% classic CNV subgroup, an alteration of 1 one in the numbers of people losing less than three lines of vision at 12 months in both the treatment and control groups is sufficient to make the result for the subgroup non-significant (i.e. if 15 Pá gina 101 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 people in the treatment group and 12 people in the control group lost three or more lines, the relative risk for the sub-group would have been 0.63 (95% confidence interval 0.37 to 1.05, P=0.09). This illustrates the fragility of this subgroup analysis and the caution needed in its interpretation. ARMD is a bilateral disease although one eye is usually affected before the other. With a lesion present in one eye, the annual cumulative incidence of a lesion in the second eye is estimated to be about 15%. It is common practice now for clinicians to advise patients already afflicted with a lesion in one eye to be watchful for the onset of symptoms in the second eye and to present as soon as those symptoms are noticed so that the chances of catching the lesion in the second eye in time are improved. This often entails the provision of an Amsler grid, a simple chart on which a number of gridlines are printed around a central fixation spot. The patient is instructed to examine the grid and to look for focal distortion of the lines in the grid which would indicate local elevation of the retina as a result of the growth of an underlying membrane. This strategy membrane. This strategy offers the best hope of saving sight with this new treatment at least in places where access to a qualified ophthalmologist can be slow. It should also be recalled that this treatment does not restore sight but rather, prevents further deterioration. Sustaining numerous assessments which involve relative invasive treatments may have an adverse effect on the patient. Without patient orientated outcomes in this trial, we cannot comment on the patient's perspective on the experience of Visudyne therapy. It is likely that in most cases, especially where loss of sight of the second eye is threatened, that patients will be willing to undergo all the necessary interventions, even when the probability of success is small. The trial was too small to assess rare important adverse effects although it does provide evidence that there are no common short-term adverse effects of treatment. This trial appears to have been performed to high standards and was closely supervised by the Food and Drugs Administration of the USA. The trial was sponsored by the manufacturers of the drug (CIBA Vision) and declared potential conflicts of interest exist for a number of the trialists who hold interests in the manufacturer of the laser technology. This makes detailed scrutiny of reports of the trial essential. That numerous protocol revisions were registered with the Institutional Review Bodies throughout the study and after completion of follow up is also of concern. Although we have not yet had access to the main protocol or the revisions, a CIBA representative has assured us that these were not substantive and in particular, there were no changes to Pá gina 102 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 the a priori determinants of the primary outcomes. Reviewers' conclusions Implications for practice This review provides evidence that photodynamic therapy in people with classic choroidal neovascularisation due to age-related macular degeneration is effective in preventing visual loss. This evidence is drawn from a subgroup analysis of the results of one trial (143 people). In our opinion, further trials should be conducted to verify this finding. Given the current level of interest in photodynamic therapy, and the fact that the effect was strong (NNT of two to prevent a doubling of the visual angle) we envisage that there will be little enthusiasm for further trials. Policy makers and clinicians should be aware, if they introduce this therapy, that the estimates of beneficial outcome are based on treatment of 143 eyes only. Outcomes and potential adverse effects of this treatment should be monitored closely. Clinicians need to have the expertise and resources to exclude people with occult choroidal neovascularisation. There is no evidence that photodynamic therapy is beneficial for people with evidence of occult choroidal neovascularisation. These people should be offered treatment in the context of a randomised controlled trial. There are major implications for health services, both in terms of potential expenditure and organisation, if photodynamic therapy is to be introduced. Where referral to an ophthalmologist is through a primary care network, facilities for the recognition of this condition in its early stages are needed. There is potential for an enormous increase in referral of people with early age-related maculopathy for assessment, in case an early treatable lesion is present. This could swamp already overstretched facilities at the secondary care level. Extra resources will be required at the secondary care level to manage increased referrals, for the necessary technology to diagnose treatable lesions and to deliver treatment. Implications for research Further independent trials of verteporfin are required to establish that the effects seen in this study are consistent and to determine important questions not yet addressed - particularly relating to quality of life and cost. Longer term outcomes are also needed both from the efficacy and safety perspective. Descriptive epidemiology on the population at Descriptive epidemiology on the population at risk and the numbers Pá gina 103 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 likely to benefit is essential to estimate the impact of this new treatment on health service resources. We need to establish how people in need of treatment can access it in time. Surveillance for possible rare but severe adverse effects will be required. Acknowledgements We would like to thank Neil Bressler MD, Simon Harding FRCOphth and Javed Bhatti (CIBA Vision) for providing information about the TAP1 study. Usha Chakravarthy (Queens University, Belfast) and Bob Thompson (Macular Disease Society) provided useful comments on the review. Potential conflict of interest None known Characteristics of included studies Table: Characteristics of included studies References References to studies included in this review TAP 1 {published and unpublished data} Treatment of Age-related Macular Degeneration With Photodynamic Therapy (TAP) Study Group. Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin. Archives of Ophthalmology 1999;117:1329-1345. * indicates the major publication for the study Additional references Fine 1999 Fine SL. Photodynamic therapy with verteporfin is effective for selected patients with neovascular age-related macular degeneration. Archives of Ophthalmology 1999;117(10):1400-1402. Pá gina 104 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Miller 1999 Miller JW, Schmidt-Erfurth U, Sickenberg M, Pournaras CJ, Laqua H, Barbazetto I, Zografos L, Piguet B, Donati G, Lane AM, Birngruber R, van den Berg H, Strong A, Manjuris U, Gray T, Fsadni M, Bressler NM, Gragoudas ES. Photodynamic therapy with verteporfin for choroidal neovascularisation caused by age-related macular degeneration. Results of a single treatment in a phase 1 and 2 study. Archives of Ophthalmology 1999;117(9):1161-1173. MPS 1994 Macular photocoagulation study group. Laser photocoagulation for juxtafoveal choroidal neovascularization: five year results from randomized clinical trials. Arch Ophthalmol 1994;112:500-509. Schmidt-Erfurth 1999 Schmidt-Erfurth U, Miller JW, Sickenberg M, Laqua H, Barbazetto I, Gragoudas ES, Zografos L, Piguet B, Pournaras CJ, Donati G, Lane AM, Birngruber R, Zografos L, van den Berg H, Strong A, Manjuris U, Gray T, Fsadni M, Bressler NM. Photodynamic therapy with verteporfin for choroidal neovascularisation caused by age-related macular degeneration. Results of retreatment in a phase 1 and 2 study. Archives of Ophthalmology 1999;117(9):1177-1187. Yusuf 1991 Yusuf S, Wittes J, Probstfield J, Tyroler HA. Analysis and interpretation of treatment effects in subgroups of patients in randomized clinical trials. JAMA 1991;266(1):93-98. Coversheet Title Photodynamic therapy for neovascular age-related macular degeneration Reviewer(s) Wormald R, Evans J, Smeeth L Pá gina 105 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Contribution of Reviewer(s) All three reviewers participated in protocol development, study selection and assessment and writing up of the final review. Liam Smeeth and Jennifer Evans abstracted data and entered it onto Revman. Issue protocol first published: Information not available Issue review first published: 2000 Issue 2 Date of most recent amendment: 29 November 2000 Date of most recent substantive amendment: 22 February 2000 Most recent changes: Information not supplied by reviewer Date new studies sought but none found: Information not supplied by reviewer Date new studies found but not yet included/excluded: Information not supplied by reviewer Date new studies found and included/excluded: Information not supplied by supplied by reviewer Date reviewers' conclusions section amended: Information not supplied by reviewer Contact address: Mr Richard Wormald MA MB MSc FRCS FRCOphth Consultant Ophthalmologist and Honorary Senior Lecturer Research and Development Department Moorfields Eye Hospital and Institute of Ophthalmology (UCL) City Road London UK EC1V 2PD Telephone: +44 20 7566 2818 Facsimile: +44 20 7608 6925 Pá gina 106 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 E-mail: [email protected] For information on the editorial group see: Cochrane Eyes and Vision Group Extramural sources of support to the review NHS Exectutive London, Research and Development UK Intramural sources of support to the review Moorfields Eye Hospital NHS Trust UK Synopsis PHOTODYNAMIC THERAPY MAY REDUCE VISION LOSS CAUSED BY ONE TYPE OF AGE-RELATED MACULAR DEGENERATION BUT MORE RESEARCH IS NEEDED Age-related macular degeneration (ARMD) affects the macula, the centre of the retina (the light-sensitive area inside the eye). One type is called 'wet' or neovascular, as new blood vessels develop in the macula. These can leak and scar the eye, causing vision loss. Photodynamic therapy involves injecting chemicals, then radiating light as they flow through these new blood vessels. This aims to activate the chemicals enough to destroy the vessels, but not enough to hurt the eye. The review found some evidence that this may reduce vision loss caused by 'classic' neovascular ARMD, but more research is needed. Keywords Human; Macular Degeneration/*drug therapy; Neovascularization, Pathologic; *Photochemotherapy; Photosensitizing Agents/*therapeutic use; CRG Code: HM-EYES Cochrane Library number: CD002030 Pá gina 107 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 ANEXO 9 Pá gina 108 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Retina/Vitreous Visudyne looks promising for treating wet AMD But will the new procedure break the Medicare bank? With 65,000 procedures performed in 2000, the question is apt. by Irving J. Arons Special to Ocular Surgery News January 15, 2001 Last year at this time I reported that Visudyne photodynamic therapy (PDT), along with several other PDT treatments in the pipeline, appeared promising for those afflicted with predominantly classic, wet age-related macular degeneration. This year the technology has come to the market, and good results are being reported but financial questions remain. My earlier report was filed following the 1999 American Academy of Ophthalmology (AAO) meeting (“Laser treatments for AMD show promise,” Jan. 15, 2000, issue), One question posed by industry analysts during that meeting was how, when these new techniques came to market, would the Health Care Financing Administration (HCFA) handle the reimbursement issues without bankrupting Medicare? Well, the inevitable has happened. Visudyne therapy (verteporfin for injection, marketed for QLT Inc. by CIBA Vision) for predominantly classic wet AMD was approved for marketing by the Food and Drug Administration in April 2000. Since then, thousands of AMD patients have flooded retinal surgeons’ offices seeking treatment. The approval was based on the 12-month data from two 24-month randomized, double-masked, placebocontrolled phase 3 clinical trials known as the Treatment of AMD with Photodynamic therapy (TAP) Investigation. Results of the TAP studies were published in the October 1999 issue of Archives of Ophthalmology. The TAP 12-month findings showed that in 243 patients with predominantly classic wet choroidal neovascularization (CNV), vision remained stable or improved in 67% of patients treated with Visudyne therapy versus 39% of patients in the placebo arm of the study. Additional data released this past summer showed that the beneficial effect and the favorable safety profile of Visudyne therapy that was observed at the 12-month time point was maintained out to 2 years, with fewer treatments required in the second year (see clinical results update below). Market size and reimbursement It is estimated that some 65,000 U.S. PDT treatments, both primary and retreatments, were done in 2000, producing $90 million to $100 million in drug revenues for QLT/CIBA Vision. If analysts’ projections continue to hold up, the drug could reach more than $200 million in sales in 2001 — and as high as $500 to $700 million by 2003. Pá gina 109 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 But the picture isn’t all rosy. In November, HCFA issued its revised National Policy for Reimbursement, calling Visudyne therapy a “medically reasonable and necessary treatment.” The agency also expanded somewhat the number of patients who can receive treatment (those presenting with at least 50% classic symptoms from a fluorescein angiogram) and how often retreatments can occur — up to 6 treatments over 24 months, although recent field interviews/surveys show that fewer retreatments are occurring in practice over an extended time. (The TAP inclusion criteria included having visual acuities between 20/40 and 20/200, and lesions greater in size than 0.5 mm. On average, 5.6 treatments were reported over the 2year period.) However, the agency cut the expected physician reimbursement for the treatment — including infusion, use of the laser and staff overheads — to $341 from the $500-to-$700 reimbursement figure expected (and previously paid for laser photocoagulation). When added to the drug reimbursement ($1,458), Visudyne PDT therapy total reimbursement will be $1,799 in 2001. Taken against the cost to administer the treatment, according to a Dain Rauscher Wessels analysis, a high-volume practice could expect a profit per procedure of about $500, while a low-volume practice might only clear $135, not including the physician’s fee! This total is down from the $900 profit that high-volume practices could have expected under the older laser photocoagulation rates, and about $550 for lower-volume practices. With between 1,200 and 1,300 practicing retinal specialists in the United States, we estimate that there are currently about 600 PDT activation lasers (from either Zeiss Humphrey or Coherent Medical) in use in the United States, with an additional 600 in use worldwide. In a poll of 67 retinal practices conducted by Leerink Swann & Company in November 2000, 82% of respondents stated that the new level of reimbursement from HCFA was below expectations and inadequate. At an AMD press conference held during this year’s AAO meeting before the HCFA announcement, Mark Blumenkranz, MD, noted that Visudyne treatment may end up being offered only at larger medical centers or academic centers if the reimbursement issues are not satisfactorily resolved. Medicare cost I have attempted to calculate the potential cost to the Medicare system for PDT for the year 2000 and beyond. The cost for 2000 depends on how many people actually underwent the treatment, which in turn depends on how many of the 200,000 to 350,000 of the current AMD pool met the acceptance criteria. The wet form of AMD accounts for about 10% to 15% of the total AMD population, or 1.3 to 1.5 million people in the United States, plus another 200,000 new cases diagnosed each year (and 400,000 more worldwide). The predominantly classic form represents about 10% to 15% of the total wet form population, or approximately 130,000 to 250,000 people that could now be treated, with an additional 20,000 to 30,000 being diagnosed and entering the potential treatment pool each year, not taking into account additional patients with diseases such as pathological myopia, which should be added to the Visudyne labeling sometime in mid-2001. The cost to Medicare for Visudyne PDT in 2000 could conceivably have ranged from $160 million to $280 million, assuming that one-third of the current pool elected treatment, half of those were eligible (many in the pool may have already lost too much vision to be treatable) and the cost to the system is $1,799 per procedure ($1,458 for the drug — or less depending on the copay — plus $341 for treatment) with an average of three treatments needed over the course of the first year. (This calculation assumes that 60% of recipients have Medicaid and Medicare pays 80% of the drug cost, with the recipient paying the remaining 20% co-pay. The actual cost for 2000, based on 65,000 doses, was closer to $115 million.) In subsequent years, with another third of those eligible entering treatment, along with additional retreatments for some of those already started on their initial course of treatment, Medicare costs could average over $250 million a year. And when other eye diseases and treatment modalities are approved, the cost can only rise. Another factor is the subjective nature of the diagnosis. Those patients with marginal classic symptoms may be included in the treatment class, as this might be their only hope for retaining vision. Improved quality of life On a more positive note, Dr. Sanjay Sharma of Queens University in Kingston, Ontario, presented a paper during the AAO meeting on a decision-making model for measuring the impact of Visudyne therapy on Pá gina 110 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 the quality of life of those with AMD. He concluded that PDT is a very effective treatment for AMD, and that patients who are still able to drive could expect a 10.7% improvement in quality of life if they received the treatment, while patients who were legally blind could expect a 7.8% improvement. This compares to those who have lost significant vision, who are assessed as having a 40% reduction in their quality of life. With the looming crisis in vision loss as baby boomers advance into their middle and senior years over the next decade, more than 500,000 people a year will be diagnosed with AMD, and without treatment will become more dependent on others (and possibly on the welfare system). As Dr. Sharma’s model suggests, “For one patient with macular degeneration to obtain one quality of life-adjusted year, PDT will cost a managed care organization $86,721. If the treatment proves effective over the entire duration of a patient’s life, this cost will fall dramatically.” Left unsaid is the potential cost to the system for legally blind people unable to avail themselves of the treatment. Clinical update — PDT trials During the AAO Vitreoretinal Update meeting, Susan Bressler, MD, provided 24-month data for the TAP study. The data reiterated the significant difference in eyes treated with PDT versus the placebo control, with 53% of the Visudyne patients losing less than 15 letters (three lines) of visual acuity, compared to 38% for the placebo group. The subgroup results for predominantly classic patients showed even better results, but they were not so good for those with minimally classic or nonclassic disease. For those with predominantly classic lesions, 59% lost less than 15 letters, versus 31% of the placebo group; in the minimally classic group, 48% lost less than 15 letters, versus 44% getting the placebo; and 56% versus 30% for the nonclassic disease group. Dr. Bressler concluded that the results seen at 12 months were sustained at 24 months, with even more compelling evidence to use Visudyne therapy for patients with classic wet AMD. The additional benefits of the 24-month TAP trial were limited, but included slower lesion growth, reduced leakage and stable contrast sensitivity. The average number of treatments of the group during the second year was 2.2 out of a possible maximum of 4, resulting in an average number of treatments over the 2-year period of 5.6 out of a maximum of 8. Joan Miller, MD, reported on the 12-month results of the Verteporfin in Photodynamic Therapy (VIP) study for pathologic myopia taking place at 28 clinical centers worldwide. In this case, 72% of those treated achieved less than 8 letter loss (less than 1.5 lines) compared to 44% in the placebo group. Dr. Miller concluded that VIP treatment resulted in a significantly increased incidence of stability or improved visual acuity, with no evidence of ocular or systemic tissue risk. The VIP trial was focused on two groups of patients; those with pathologic myopia and those with earlier stage AMD than in the TAP study (that is, either those with occult lesions or those with classic lesions but better than 20/40 vision). While the VIP trial was intended to expand the population for Visudyne-eligible patients, it was less definitive than TAP. Statistical benefits were experienced among those in the pathologic myopia group, but there were no statistically significant differences or advantages for those with earlier stage AMD treated with Visudyne compared to placebo. At the AAO’s AMD press conference, Dr. Blumenkranz, coordinator for the Pharmacyclics/Alcon Labs trials of Optrin (LuTex), said that the phase 1 and 2 clinical trials for that drug had been completed and were being evaluated prior to recruiting patients for phase 3 trials. (It was also learned that a Zeiss diode laser is being used for activation, not the Diomed system as reported in my article last year.) Edgar Thomas, MD, head of the Miravant/Pharmacia & Upjohn trial of Photopoint (purlytin), said the drug was completing phase 3 trials with nothing new to report. Laser treatments Elias Reichel, MD, reported on the results to date in the ongoing multicenter clinical trial to treat occult wet AMD, the most prevalent form of the disease, with low-intensity laser energy, in the transpupillary thermotherapy (TTT) for CNV trial. Unlike PDT, this trial used the Iridex Iris Medical SLx 810 nm diode laser in its unique long-pulse mode to treat the lesions without the need for a photoactive drug. He reported that after 1 year, 80% of patients with occult wet AMD treated with the laser experienced a halt in new vessel growth and that 70% had stable or improved vision, with no signs of damage to the photore- Pá gina 111 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 ceptor cells of the retina. TTT appears to stop the evolution of the exudative process, and may avoid development of or progression to the classic form. (Traditionally, half of all cases of occult AMD move into the classic form, with profound visual loss.) Anecdotal evidence indicates that TTT is doing quite well in the field, but the reimbursement picture remains cloudy. According to Iridex, reimbursements for this treatment, which are left up to the discretion of local Medicare carriers, range from a low of $127 to a high of $700. Until this discrepancy and confusion is cleared up, and published peer-reviewed studies on its success begin to appear, TTT will be slow to be accepted by most retinal surgeons. Clinical update — dry AMD At the Iridex booth, a number of speakers provided updates on the ongoing work with both therapeutic and prophylactic treatments for the dry form of AMD. In a pilot study their 810 nm diode laser was used in a grid-pattern therapy on nonexudative soft drusen, with resorption of drusen seen in 68% of treated eyes and visual acuity improvement in 24% of a subset of treated eyes after a single treatment. The company continues to sponsor additional work in both therapeutic and prophylactic trials. In the therapeutic study, the 4-year follow-up of the original pilot study showed continued improvement in 78% of treated eyes, defined as a reduction of 50% or more of drusen from baseline, versus only 8% of eyes not treated but observed. This resulted in visual acuity improvement by two or more lines in 14% of treated eyes, which suggests a therapeutic benefit for patients with dry AMD who have lost two or more lines of acuity due to the presence of central soft drusen. In the ongoing prophylactic study, Prophylactic Treatment of AMD, a total of 35 neovascular events have occurred in 4 years in the 22% of eyes nonresponsive to treatment, with half occurring in the observed eyes and half in the treated eyes, indicating no treatment harm or benefit. However, in the 78% of eyes that responded to treatment with a significant reduction in drusen, only one eye developed CNV. The study authors suggest that a prophylactic treatment that effectively promotes drusen resorption may be effective in reducing or delaying progression to CNV. It is beginning to appear that the once-dreaded AMD disease, and the visual loss accompanying it in its worst cases, will become treatable for the vast majority of those who contract it over the next decade. This calculation assumes (or less, depending on the co-pay). For Your Information: • Irving J. Arons is managing director of Spectrum Consulting with offices at 4 Harvard St., Peabody, MA 01960; phone and fax: (978) 531-0939; email: [email protected]. Mr. Arons has no direct financial interest in any of the products mentioned in this article, nor is he a paid consultant for any companies mentioned. Copyright 2001, SLACK Incorporated. Revised 5 January 2001. Pá gina 112 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 ANEXO 10 Pá gina 113 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 114 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 115 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 116 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 117 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 118 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 119 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 120 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 121 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 122 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 123 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 124 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 125 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 ANEXO 11 Pá gina 126 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 127 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 128 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 129 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 130 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 131 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 132 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 133 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 134 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 135 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 136 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 137 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 138 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 139 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 140 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 141 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 142 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 143 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 144 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 145 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 146 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 147 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 148 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 149 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 150 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 151 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 152 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 153 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 154 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 155 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 156 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 157 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 158 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 159 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 160 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 161 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 162 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 163 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 164 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 165 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 166 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 167 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 168 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 169 de 170 INFORME VALORATIVO A DEMANDA Terapia Fotodinámica en el tratamiento de la Degeneración Macular Asociada a la Edad REF.: ACEMSA/SET/AC/ac febrero-2001 Pá gina 170 de 170
 0
0
Anuncio
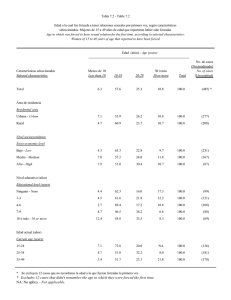
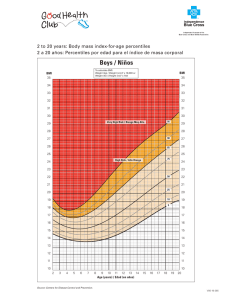
Descargar
Anuncio
Añadir este documento a la recogida (s)
Puede agregar este documento a su colección de estudio (s)
Iniciar sesión Disponible sólo para usuarios autorizadosAñadir a este documento guardado
Puede agregar este documento a su lista guardada
Iniciar sesión Disponible sólo para usuarios autorizados