Español - SciELO España
Anuncio

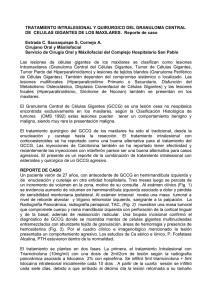
28-4 2/10/06 11:36 Página 231 Rev Esp Cir Oral y Maxilofac 2006;28,4 (julio-agosto):231-236 © 2006 ergon Página del Residente ¿Cuál es su diagnóstico? What should the diagnosis be? Paciente varón de 63 años de edad The case is presented of a 63sin alergias medicamentosas conocidas year-old male patient with no con antecedentes personales de hiperknown drug allergies, a pertensión arterial secundaria a transplansonal history of arterial hyperte renal, cardiopatía isquémica, sordetension as a result of a renal ra neurosensorial e hipertrofia gingival transplant, ischemic carpor medicación inmunosupresora. Pordiopathy, neuro-sensorial tador de prótesis dental parcial remodeafness, and gingival hypervible superior. trophy due to immunosupAcude a nuestras consultas por prepressive medication. sentar una lesión en la encía del maxiHe presented with a gingival lar superior derecho de rápido crecilesion in the right side of the miento en los últimos meses. El pacienmaxilla that had been growte refiere haber tenido una lesión simi- Figura 1. Lesión que abomba en la encía maxilar superior dere- ing rapidly over the previous lar hace años que fue tratada quirúrgi- cha. months. He commented that Figure 1. Lesion bulging in upper right gingiva of maxilla. camente en otro hospital. he had had a similar lesion En la exploración se objetiva una some years previously that lesión de 3 x 2 cm de diámetro que had been treated surgically abomba por vestíbulo en la encía superior derecha, de consistenin another hospital. cia blanda y márgenes mal definidos (Fig. 1). Se solicita OPG, donde On examination he was found to have a lesion that mease observa que la lesión engloba a la pieza dentaria 13, que a su vez sured 3 x 2 cm in diameter that was bulging through the presenta un posible quiste periapical. vestibular gingiva on the upper right side. It was soft in consistency and it had poorly defined margins (Fig. 1). An OPG was requested that showed a lesion encompassing tooth Nº 13 which in turn had a possible periapical cyst. 28-4 2/10/06 11:36 Página 232 Rev Esp Cir Oral y Maxilofac 2006;28,4 (julio-agosto):231-236 © 2006 ergon Página del Residente Granuloma periférico de células gigantes Peripheral granuloma of giant cells M.L. Maniegas Lozano1, J. Giner Díaz1, V. Ordoñez Soblechero1, S. González Luque1, J.M. García Rielo1, R. Martín-Granizo2 Ante la sospecha de una recidiva más agresiva de la lesión previa se decide intervenir quirúrgicamente de nuevo al paciente. Bajo anestesia general e intubación nasotraqueal se realiza resección de la lesión con márgenes de seguridad incluyendo pieza 13 y curetaje del lecho. Para el cierre del defecto se toma colgajo de bola adiposa bucal de Bichat derecho pediculada (Figs. 2, 3 y 4). El postoperatorio es favorable y sin complicaciones. Se revisa al paciente en consultas a los 15 días y a los 3, 6 y 12 meses, estando en todo momento asintomático y sin signos de recidiva (Fig. 5). En el informe anatomopatológico se describe una mucosa oral ulcerada y el hueso subyacente con proliferación de células gigantes multinucleadas e histiocitos con atipias y presencia de dos mitosis por campo de 400 aumentos. Entre las trabéculas óseas hay células proliferativas fusiformes. La zona ulcerada tiene detritus necróticos y supuración. El suelo de la úlcera lo forman las células proliferantes multinucleadas (Figs. 6, 7 y 8). La lesión se diagnostica finalmente como granuloma periférico de células gigantes. As there was a suspicion that this was a more aggressive recurrence of the previous lesion, a second surgical intervention was decided on. Under general anesthesia and with nasotracheal intubation, the lesion was resected with safety margins. Tooth Nº 13 was included and curettage of the bed was carried out. For closing the defect a pedicled flap was harvested of Bichat’s fat pad (Figs. 2, 3 and 4). The postoperative period was favorable and complication-free. The patient was followed at two weeks and at 3, 6 and 12 months. He was always asymptomatic and free of recurrence (Fig. 5). The anatomopathological study revealed an ulcerated oral mucosa and underlying bone with a proliferation of multi-nucleated giant cells and atypical histiocytes and the presence of two mitoses per field at x 400 magnifications. Among the bone trabeculae there were proliferative spindle cells. The ulcerated area had necrotic detritus and suppuration. The ulcer base was made up of multi-nucleated proliferative cells (Figs. 6, 7 and 8). The lesion was finally diagnosed as peripheral granuloma of giant cells. Discusión Las lesiones de células gigantes constituyen un conjunto de procesos patológicos muy amplio y diverso, tanto en sus características biológicas como morfológicas. Histológicamente pueden asemejarse mucho debido a la presencia de células gigantes. La clave para una correcta clasificación y diagnóstico radica en su compor- 1 Médico residente 2 Médico adjunto Servicio de Cirugía Oral y Maxilofacial. (Jefe de Servicio: Dr. A Berguer) Hospital Clínico San Carlos, Madrid, España Correspondencia: Lourdes Maniegas Servicio de Cirugía Oral y Maxilofacial Hospital Clínico San Carlos C/ Prof. Martín Lagos s/n 28040 Madrid, España Email: [email protected] Discussion Giant cell lesions constitute a group of pathological processes that is very wide and diverse from the biological as well as morphological point of view. Histologically they can resemble each other as a result of the presence of giant cells. When trying to choose suitable treatment in order to obtain a favorable prognosis, the key for their correct classification and diagnosis lies in their clinical behavior and in their radiological and histological features. From a pathological point of view they can be divided into three large groups:1 1. Reactive Lesions. Brown tumor of hyperparathyroidism, hemophilic pseudotumor and intraosseous hemorrhage. 2. Benign lesions. Giant cell granuloma or reparative granuloma, non-ossifying fibroma, giant cell tumor, aneurys- 28-4 2/10/06 11:36 Página 233 M.L. Maniegas Lozano y cols. Rev Esp Cir Oral y Maxilofac 2006;28,4 (julio-agosto):231-236 © 2006 ergon 233 tamiento clínico y en sus patrones radiomal bone cyst, chondroblaslógico e histológico, sobre todo a la hora toma, chondromyxoid fibrode seleccionar un adecuado tratamienma, Langerhans cell histioto y obtener un pronóstico favorable. cytosis, pigmented villonDesde un punto de vista patológiodular synovitis. co pueden dividirse en tres grandes gru3. Malignant lesions: pos:1 Osteosarcoma, malignant 1. Lesiones reactivas: Tumor pardo del fibrous histiocytoma, clear hiperparatiroidismo, pseudotumor cell chondrosarcoma, hemofílico y hemorragia intraósea. metastatic carcinoma. 2. Lesiones benignas: Granuloma de Giant cell granuloma was células gigantes o granuloma repafirst described by Jaffe2 in 1953 as a lesional reaction rador, fibroma no osificante, tumor with a reparative purpose. de células gigantes, quiste óseo aneu- Figura 2. Resección quirúrgica de la lesión. However, later studies have rismático, condroblastoma, fibroma Figure 2. Surgical resection of lesion. since shown that the reparcondromixoide, histiocitosis de céluative characteristics are minlas de Langerhans, sinovitis pigmenimal. It is a benign lesion that tada vellonodular. constitutes 7% of all benign 3. Lesiones malignas: Osteosarcoma, histumors that appear in the tiocitoma fibroso maligno, condromandible.3 It has been sarcoma de células claras, carcinoma defined by the WHO as an metastático. intraosseous lesion consistEl granuloma de células gigantes fue ing of cellular fibrous tissue descrito por primera vez por Jaffe,2 en 1953 como una respuesta lesional con that contains multiple hemfines reparativos; sin embargo, estudios orrhagic foci and multinuposteriores han puesto de manifiesto las cleated giant cell aggregates características escasamente reparativas and occasionally bony tradel mismo. Es una lesión benigna que beculae.4 constituye el 7% de los tumores benig- Figura 3. Obtención de bola adiposa bucal de Bichat derecha pedi- It is found more frequently in the mandible than in the nos que aparecen en la mandíbula,3 y es culada. definida por la OMS como una “lesión Figure 3. Harvesting of right-sided pedicled flap of Bichat’s fat pad. maxilla (2:1) although it can intraósea formada por tejido celular also appear in the orbit, fibroso que contiene múltiples focos paranasal bones, cranium hemorrágicos y agregados de células and the small bones of the gigantes multinucleadas y, ocasionalhands and feet. It has a mente, trabéculas óseas”.4 predilection for the anterior Se localiza con más frecuencia en la region of the mandible, mandíbula que en el maxilar superior although it can also appear (2:1), aunque también puede aparecer from premolars to molars. en órbita, huesos paranasales, cráneo y However, in the maxilla, findhuesos pequeños de manos y pies. Tiene ing it distally to the canines predilección por la región anterior manis unusual. It manifests more dibular, aunque también puede aparecer frequently in females (2:1) desde premolares a molares. En cambio and during the first three en el maxilar superior es raro que se locadecades in life, and it affects lice distal a los caninos. Se manifiesta con mainly children and young Figura 4. Cierre del defecto con el colgajo de bola adiposa y sutumás frecuencia en el sexo femenino (2:1) ra con seda y aguja cilíndrica. adults.5,6 Its origin is y en las tres primeras décadas de la vida, Figure 4. Closure of the defect with fat pad flap and silk suturing and unknown, although it is thought to have a genetic afectando fundamentalmente a niños y cylindrical needle. determinant and to be relatadultos jóvenes.5,6 Su origen es desconocido, aunque se piensa que pueden existir determinantes genétied to previous trauma and/or inflammation. cos, así como antecedentes traumáticos y/o inflamatorios. Most patients are asymptomatic, although there may La mayoría de los pacientes se muestran asintomáticos, aunque be swelling around the face or in the oral cavity. There may puede aparecer tumefacción facial o en la cavidad oral. Además be an onset of pain, tooth mobility, facial asymmetry and, 28-4 2/10/06 234 11:36 Página 234 Rev Esp Cir Oral y Maxilofac 2006;28,4 (julio-agosto):231-236 © 2006 ergon puede debutar con dolor, movilidad dentaria, asimetría facial y, con menos frecuencia, parestesias. Esto es así debido a que la lesión, aun teniendo un crecimiento expansivo, no invade las vainas perineurales.7,8 Las lesiones con un crecimiento más lento son las asintomáticas y las que se diagnostican de forma casual en radiografías rutinarias, mientras que aquellas con un crecimiento más agresivo presentan dolor, tumefacción facial y destrucción tisular marcada. Estas últimas tienen más tendencia a la recidiva y su tratamiento es más controvertido.7 El diagnóstico radiológico puede ser muy variable, desde lesiones uniloculares bien definidas a áreas multiloculares con patrón en pompas de jabón, adelgazamiento cortical, bordes irregulares o rizólisis.6 La capa ósea que rodea a la lesión suele ser delgada con o sin destrucción ósea. En la ortopantomografía lo más habitual es encontrar lisis ósea, aunque en el maxilar superior pueden aparecer zonas de radiocondensación en “reloj de arena”.5 El patrón radiológico inespecífico tanto de la OPG como de la TC hace que el granuloma de células gigantes sea indistinguible de otras lesiones óseas radiolúcidas como el quiste odontogénico, quiste óseo aneurismático, ameloblastoma, mixoma odontogénico y fibroma odontogénico.9 En imágenes de RM con contraste yodado o gadolinio intravenoso se aprecia realce de la lesión con una señal débil en las secuencias T1 y más intensa en T2. Se describen además tabiques fibrosos hipointensos. Las áreas quísticas son infrecuentes, y cuando aparecen, constituyen un pequeño porcentaje de la lesión. Del mismo modo pueden apreciarse imágenes de calcificación en su interior.9 Histológicamente se observa un estroma fibrocelular con células gigantes multinucleadas (5-10 núcleos por célula), fibroblastos y células en huso rodeadas por focos hemorrágicos. Es característica la formación de hueso reactivo y una gran actividad osteoblástica. No suelen observarse atipias. Las células en huso tienen actividad osteoclástica. Granuloma periférico de células gigantes Figura 5. Ortopantomografía 6 meses tras la resección de la lesión. No se observan signos radiográficos de recidiva y sí una correcta osificación del lecho. Figure 5. Orthopantomography 6 months after lesion resection. No radiographic evidence of recurrence and correct ossification of the bed can be observed. Figura 6. Vista macroscópica de la pieza tras su resección quirúrgica. Figure 6. Macroscopic view of the specimen following surgical resection. Figura 7. Presencia de trabéculas óseas con grados variables de mineralización rodeadas de células fusiformes y células gigantes multinucleadas (HE x 240). Figure 7. Presence of bone trabeculae with variable degrees of mineralization surrounded by spindle cells and multinucleated giant cells (HE x 240). more unusually paresthesias. This is as a result of the lesion not invading the perineural sheath, despite showing an expansive growth pattern.7,8 The slower growing lesions are asymptomatic and they tend to be diagnosed by chance in routine radiographies. Those with more aggressive growth are painful, and there is facial swelling and obvious tissue destruction. They are more likely to recur and their treatment is more contested.7 Radiological diagnosis can vary substantially from welldefined unilocular lesions to multilocular areas with a soap bubble pattern, cortical thinning, irregular borders or rhizolysis.6 The layer of bone around the lesion tends to be thin and there may or may not be bone destruction. It is common to find bone lysis in the orthopantomography, although there may be areas of “hour glass” radio-condensation in the maxilla.5 The unspecific signs in the radiological pattern found in the OPG as well as in the CT scan result in giant cell granuloma being indistinguishable from other radiolucid bone lesions such as the odontogenic cyst, aneurysmal bone cyst, ameloblastoma, odontogenic myxoma and odontogenic fibroma.9 The lesion is highlighted in MR images when iodinated contrast material or intravenous gadolinium is used. A low signal will appear on T1 weighted sequences, which will be more intense on T2. Fibrous hypointense walls have also been described. Cystic areas are uncommon and they make up just a small percentage of the lesion when they do 28-4 2/10/06 11:36 Página 235 M.L. Maniegas Lozano y cols. Rev Esp Cir Oral y Maxilofac 2006;28,4 (julio-agosto):231-236 © 2006 ergon 235 El diagnóstico diferencial debe realiappear. Calcification areas zarse con las siguientes entidades: quiscan also be appreciated in te óseo aneurismático, querubismo (son the interior.9 Histologically a fibrocellular típicas las lesiones multifocales mandistroma can be observed with bulares bilaterales),5 tumor pardo del hiperparatiroidismo (se observa aumengiant multinucleated cells (5to del calcio sérico, fosfatasa alcalina y 10 nuclei per cell), fibroblasts hormona paratiroidea y disminución de and spindle cells surrounded fósforo sérico),9 ameloblastoma, displaby hemorrhagic foci. The forsia fibrosa y tumor de células gigantes mation of reactive bone and (se localiza fundamentalmente en la epía large amount osteoblastic fisis de huesos largos, cráneo, huesos activity is typical. Atypia faciales y senos paranasales, se manifiesta tends not to be observed. en torno a los 40-50 años y en el corte Spindle cells tend to have histológico se aprecian muchos más Figura 8. Zona ulcerada de la mucosa gingival por la compresión osteoclastic activity. núcleos en las células gigantes y una dis- del granuloma subyacente (HE x 100) The differential diagnosis tribución más regular por todo el Figure 8. Ulcerated area of gingival mucosa as a result of compres- should be carried out with sion by the underlying granuloma (HE x 100). tumor).1 the following entities: El tratamiento del granuloma de céluaneurysmal bone cyst, cherulas gigantes es inicialmente quirúrgico, aunque actualmente exisbism (bilateral multifocal lesions are typical in the mandible),5 brown tumor of hyperparathyroidism (an increase of serum ten otras opciones de tratamiento igualmente recomendadas. La calcium, alkaline phosphate and parathyroid hormone and cirugía consiste en la resección de la lesión y el curetaje exhaustivo a reduction of serum phosphate),9 ameloblastoma, fibrous de las raíces dentarias y paredes óseas remanentes. Los dientes dysplasia and giant cell tumor (located chiefly in the epienglobados en la lesión deben ser endodonciados previamente a physis of long bones, the cranium, facial bones and paranasal la cirugía para garantizar su preservación. Este tratamiento ha demossinuses, it appears around the 40 to 50 age mark. The histrado altas tasas de curación con escasas recurrencia.8,10 A pesar de esto, un pequeño porcentaje de las lesiones son agresivas y destological section will show many more nuclei in giant cells truyen o perforan la cortical ósea, forzando un tratamiento igualand a more regular distribution through out the tumor).1 Treatment for giant cell granuloma is initially surgical, mente más agresivo con excisiones locales y márgenes de resección although there are currently other therapeutic options that amplios, pérdida de piezas dentarias y defectos en la continuidad are equally recommendable. Surgery consists in carrying out tisular que hacen necesaria una reconstrucción estética y funcional. a resection of the lesion and exhaustive curettage of the denA raíz de esto han surgido en los últimos años alternativas teratal roots and the remaining bony walls. The teeth enveloped péuticas no quirúrgicas que han demostrados buenos resultados by the lesion should have root canal treatment prior to the frente a lesiones agresivas.5,12-18 • Corticoides intralesionales: Su posible utilidad surge en relación surgery in order to guarantee their preservation. This treatcon las similitudes microscópicas observadas en la sarcoidosis y ment has achieved high cure rates with few cases of recurlas lesiones de células gigantes. El mecanismo de acción está rence.8,10 Despite this, a small percentage of these lesions are aggressive and they will destroy or perforate cortical bone basado en la inhibición de la actividad osteoclástica, que proresulting in the need for more aggressive treatment such voca una regeneración ósea más rápida, incluyendo los conas local excision and wide resection margins. Teeth may tornos perdidos. El protocolo de tratamiento consiste en 6 inyecbe lost and there may be defects in tissue continuity making ciones semanales.11 Algunos estudios han demostrado buenos resultados a pesar de ser una terapia contraindicada en deteraesthetic and functional reconstruction necessary. As a result minadas situaciones médicas (DM, úlcera péptica, estados de of this, non-surgical therapeutic alternatives have arisen over inmunodepresión, etc.).12,13 the last few years that have had good results with regard to • Calcitonina subcutánea: Se habla de ella por primera vez en 1993 aggressive lesions.5,12-18 • Intralesional corticoids: The possibility of using these arisy a partir de entonces han aparecido en la literatura numerosos es as a result of the microscopic similarity observed in apuntes a cerca de su utilidad en el tratamiento del granulosarcoidosis and in giant cell lesions. The action mechama de células gigantes.12 Presenta un mecanismo de acción similar al del tumor pardo del hiperparatiroidismo, basado en la prenism is based on the inhibition of osteoclastic activity sencia de receptores de calcitonina en lesiones con células giganleading to faster bone regeneration to include the contes que inhiben la resorción ósea osteoclástica y actúan sobre tours that have been lost. The treatment protocol conalgún tipo de célula presente en la lesión. La hormona responsists of 6 weekly injections.11 Some studies have demonstrated good results despite being contraindicated in cersable, si existe, aún no ha sido identificada.11,14 Tras un año de tratamiento con calcitonina se observan remisiones completas tain medical situations (DM, peptic ulcer, immunodede la lesión sin signos aparentes de recidiva.15,16 Aun así la terapressive conditions, etc.).12,13 28-4 2/10/06 236 11:36 Página 236 Rev Esp Cir Oral y Maxilofac 2006;28,4 (julio-agosto):231-236 © 2006 ergon pia con calcitonina resulta incómoda y de larga duración, lo que hace que sea mal tolerada por determinados pacientes, por ejemplo en niños.15 En su estudio, Pogrel concluye que aun siendo una terapia viable para el tratamiento de estas lesiones, debido al handicap de la duración del tratamiento, lo más adecuado sería reservarla para lesiones múltiples, agresivas y recurrentes.11 • Interferón alfa: El mecanismo de acción presume la naturaleza vascular de la lesión. El interferón suprime la angiogénesis provocando de este modo la involución de la lesión.17 El papel de estos tratamientos debe ser investigado en mayor profundidad con el fin de conseguir resultados satisfactorios que permitan curaciones completas y eviten recidivas. Finalmente deben realizarse controles periódicos durante 1-2 años ante la posibilidad de recidiva (11-49%), que se ve incrementada en lesiones agresivas con destrucción local, crecimiento rápido, rizólisis y parestesias, así como en gente joven y en lesiones localizadas en maxilar superior,5 como ocurre en el presente caso clínico. Bibliografía 1. Rosenberg AE, Nielsen GP. Giant-cell containing lesions of bone and their differential diagnosis. Curr Diag Pathol 2001;7:235-46. 2. Jaffe HL. Giant-cell reparative granuloma, traumatic bone cyst and fibrous dysplasia of the jawbones. Oral Surg Oral Med Oral Pathol 1953; 6:159-75. 3. Austin LT, Dahlin CD, Royer QR. Giant-cell reparative granuloma and related conditions affecting the jawbones. Oral Surg Oral Med Oral Pathol 1959;12:1285. 4. Kramer IRH, Pindborg JJ, Shear M. Histological typing of odontogenic tumors (2ª ed.) Springer Verlag 1991;p.p.31. 5. de Lange y cols. Clinical and radiological features of central giant-cell lesions of the jaw. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;99:464-70. 6. Donado M. Cirugía bucal. Masson 2005; p.p.827-8. 7. Üstündag E, y cols. Central giant-cell granuloma. Int J Pediatr Otorhinolaryngol 2002;65:143-6. 8. Bataineh, Al-Khateeb, Rawashdah. The surgical treatment of central giant-cell granuloma of the mandible. J Oral Maxillofac Surg 2002;60: 756-61. 9. Çakirer S. Quiz case. Eur J Radiol 2002;44:24-7. 10. Stern M, Eisenbud L. Management of giant-cell lesions of the jaws. Oral Maxillofac Surg Clin North Am 1991;3:165. 11. Pogrel MA. Calcitonin therapy for central giant-cell granuloma. J Oral Maxillofac Surg 2003;61:649-53. 12. Kermer C, Millesi W, Watzke IM. Local injection of corticosteroids for central giant-cell granuloma: a case report. Int J Oral Maxillofac Surg 1994;23:366. 13. Rajeevan NS, Soumithran CS. Intralesional corticosteroid injection for central giant-cell granuloma: a case report. Int J Oral Maxillofac Surg 1998;27:303. 14. Harris M. Central giant-cell granulomas of the jaw regress with calcitonin therapy. Br J Oral Maxillofac Surg 1993;31:89. 15. de Lange J, y cols. Treatment of central giant-cell granuloma of the jaw with calcitonin. Int J Oral Maxillofac Surg 1999;28:372. 16. Rosenberg AJ, y cols. Calcitonin therapy in large or recurrent central giant-cell granulomas of the lower jaw. Ned Tijdschr Geneeskd 1997; 141:335. 17. Kaban LB, y cols. Antiangiogenic therapy of a recurrent giant-cell tumor of the mandible with INFa2a. Pediatrics 1999;103:1145. Granuloma periférico de células gigantes • Subcutaneous calcitonin: This was first described in 1993 and numerous references have since appeared in the literature with regard to its use when treating giant cell granuloma.12 It has an action mechanism that is similar to that of the brown tumor of hyperparathyroidism, based on the presence of calcitonin receptors in lesions with giant cells that inhibit osteoclastic bone resorption and that act on a type of cell that is present in the lesion. The hormone responsible, should it exist, has yet to be identified.11,14 After a year of treatment with calcitonin, complete remission of the lesion has been observed with no apparent signs of recurrence.15,16 Calcitonin therapy is still unpleasant and lengthy, which results in it being poorly tolerated by some patients such as children.15 In a study, Pogrel concludes that, while it is still a viable therapy for treating these lesions, given the handicap concerning treatment length, it would be appropriate to reserve it for multiple, aggressive or for recurrent lesions.11 • Interferon Alpha: The action mechanism assumes the vascular nature of the lesion. Interferon suppresses angiogenesis provoking the involution of the lesion.17 The role played by these therapies should be further investigated so that satisfactory results permitting complete cures can be achieved and recurrences avoided. Finally, periodic follow-ups should be carried out over a 1-2 year period given the possibility of recurrence (11-49%), which increases in aggressive lesions causing local destruction, rapid growth, rhizolysis and paresthesias, also in young people and in lesions located in the maxilla5 as occurred in the present case report.