19-24. LINFADENECTOMÍA INGUINAL. TÉCNICA QUIRÚRGICA
Anuncio

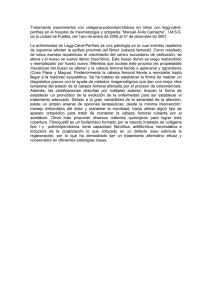
Rev. Arg. Res. Cir 2012; 17(2):19-24. LINFADENECTOMÍA INGUINAL. TÉCNICA QUIRÚRGICA DEL INSTITUTO DE ONCOLOGÍA ÁNGEL H. ROFFO. INGUINAL LYMPHADENECTOMY. INSTITUTE OF ONCOLOGY ANGEL H. ROFFO: SURGICAL TECHNIQUE Cervelo Gonzalo*, Quildrian Sergio§, Daffinoti Anabella£, Chapela Jorge§, Calónico Néstor¥. Departamento de Cirugía de Tumores de Partes Blandas. Instituto de Oncología Ángel H. Roffo. Buenos Aires, Argentina. * Médico Concurrente § Médico de Planta (MAAC) £ Médico de Planta ¥ Jefe de Servicio de Partes Blandas (MAAC) RESEÑA ANATOMICA La región inguino-crural corresponde a la parte medial de la cara anterior de la raíz del muslo. Tiene una forma triangular con su ápice en el extremo inferior. El lado superior corresponde al ligamento inguinal, el lado externo al musculo sartorio y el medial al musculo aductor mediano del muslo. El vértice, inferior, esta formado por la intersección de los haces del músculo sartorio con los del aductor mediano del muslo. Este triángulo así formado corresponde al triángulo de Scarpa (Figura 1). Planos superficiales: Piel y tejido celular subcutáneo. En este plano se encuentra la estación linfoganglionar inguinal superficial, conformada por un grupo variable de 10 a 20 ganglios distribuidos a lo largo del tronco de la safena interna. En el plano subcutáneo existen además formaciones vasculares y nerviosas de escasa importancia práctica en el curso de la intervención. El único elemento nervioso de cierta importancia esta representado por el nervio cutáneo lateral del muslo, proveniente del plexo lumbar, que aparece en esta región a nivel del ligamento inguinal, por dentro de la espina iliaca anterosuperior, descendiendo verticalmente. Se lo encuentra durante la preparación del colgajo lateral. Plano profundo: Este plano se encuentra separado del anterior por la presencia de una estructura fascial que se continua hacia abajo y por fuera con la fascia lata y que asciende hasta el ligamento inguinal, fijándose a él. Esta estructura fascial Fig 1 : Triángulo de Scarpa 1) Nervio Femorocutáneo, 2) Arterias Circunflejas Ilíacas Externas, 3) Arteria y Vena Femoral, 4) Nervio Crural, 5) Arteria Circunfleja Femoral Externa, 6) Músculo sartorio seccionado, 9) ligamento Inguinal, 10) Arteria y Vena Pudenda Externa, 11) Arteria femoral Profunda, 12) Arteria Circunfleja Femoral Interna, 13) Aductor Mediano, 14) Vena Safena Interna. 1) Femoral cutaneous nerve, 2) External iliac circumflex arteries, 3) Femoral artery and vein, 4) Femoral nerve, 5) External femoral circumflex artery, 6) Sectioned sartorius, 9) Inguinal ligament, 10) External pudendal artery and vein, 11) Deep femoral artery, 12) Internal femoral circumflex artery, 13) Adductor longus, 14) Saphenous vein. Inguinal lymphadenectomy includes the removal of lymph nodes and lymph tissue associated with the femoral vessels' path. The main indication for this intervention are metastatic melanomas of the lower extremity, genital region, perineal and abdominal wall skin, whether they are palpable nodes with a positive Fine Needle Aspiration (FNA) biopsy or occult metastases detected by sentinel positive node. Another indication of this procedure includes the inguinal lymph node metastases from carcinoma of the penis, vulva and anus. Local control of the underlying disease and the absence of distant metastases are prerequisites for performing this surgery. ANATOMICAL OVERVIEW The inguinal-femoral region corresponds to the medial part of the anterior aspect of the upper thigh.It has a triangular shape with its apex at the lower end.The upper side corresponds to the inguinal ligament, the external side to the sartorius and the medial side to the adductor longus muscle of the thigh.The vertex, bottom, is formed by the intersection of the muscles fascicles of the sartorius muscle with the adductor longus of the thigh.This triangle thus formed corresponds to the Scarpa triangle (Figure 1). Superficial levels: Skin and subcutaneous tissue.At this level it is find the superficial inguinal lymph node station, consisting of a variable group of 10 to 20 nodes distributed along the inner saphenous trunk. In the subcutaneous plane there are other vascular and nervous formations which have little prac- Pag. 19 Técnica Quirúrgica / Surgical Technique El vaciamiento ganglionar inguinal contempla la extirpación de los ganglios linfáticos y del tejido linfático asociado con el recorrido de los vasos femorales. La principal indicación de esta intervención son los melanomas metastásicos de la extremidad inferior, región genital, perineal y piel de la pared abdominal; ya sean estos ganglios palpables con PAAF positiva, o metástasis ocultas detectadas por ganglio centinela positivo. Otra indicación de este tipo de procedimiento incluye las metástasis ganglionares inguinales de los carcinomas de pene, vulva y ano. El control local de la enfermedad primaria o de base y la ausencia de metástasis a distancia son requisitos indispensables para la realización de esta cirugía. Técnica Quirúrgica . Surgical Technique envuelve la cara lateral del muslo, se desdobla al llegar al sartorio constituyendo la fascia propia y se continua hasta encontrar el borde del musculo aductor mediano del muslo. Entre las dos hojas de esta fascia se forma un espacio que es conocido como conducto crural, ocupado por los vasos femorales, algunos nervios y los ganglios linfáticos profundos. El anillo crural esta delimitado por fuera por la bandeleta iliopectínea, por dentro por el borde arqueado del ligamento lacunar, por arriba por el ligamento inguinal y por debajo por la cresta pectínea reforzada por el ligamento de Cooper. La parte lateral del anillo crural esta ocupada por la arteria femoral y por dentro de esta por la vena femoral. Entre la vena femoral y el borde libre del ligamento lacunar queda un espacio que suele estar ocupado por un ganglio linfático (de Cloquet), el cual es el más alto de los ganglios linfáticos inguinales profundos. Este grupo de dispone en el conducto crural por dentro de la vena femoral, recogiendo la linfa de los tejidos profundos de la extremidad inferior y reciben los vasos linfáticos aferentes provenientes de los ganglios linfáticos inguinales superficiales. Desde el grupo profundo la red linfática de propaga a lo largo del conducto crural hacia arriba hasta el anillo crural y luego hasta la cadena de los ganglios linfáticos ilíacos externos. Por fuera de la arteria y debajo de la fascia ilíaca que envuelve al musculo psoas ilíaco, transcurre el nervio crural, que un poco debajo del ligamento se divide en sus ramas terminales, por lo general cuatro, fácilmente identificables durante el curso de la linfadenectomía, entre el borde medial del sartorio y la arteria que pasa por debajo de la aponeurosis del musculo psoas. La vena femoral recibe en el conducto crural, unos 4-5 cm debajo del ligamento inguinal, a la vena safena interna. Durante el recorrido por el triángulo de Scarpa la arteria femoral emite numerosas ramas colaterales, entre ellas la circunfleja interna y externa del fémur, la circunfleja ilíaca superficial, la epigástrica, la arteria pudenda externa superior e inferior y la femoral profunda. Las intimas relaciones entre los ganglios linfáticos profundos y los vasos linfáticos, por un lado y los vasos femorales, especialmente la vena, por le otro, requieren particular cuidado en la “limpieza” de los troncos vasculares principales extirpando en la medida de lo posible la adventicia y el tejido periadventicial en el curso de la intervención. TECNICA QUIRURGICA Preparación del paciente Se rasura al paciente desde la región infraumbilical hasta el pubis y después a lo largo del muslo hasta la rodilla. Se lava la piel con soluciones antisépticas. La intervención de realiza bajo anestesia Pag. 20 tical importance in the course of the intervention.The only nervous element of some importance is represented by the lateral cutaneous nerve of the thigh, from the lumbar plexus, which appears in this region at the inguinal ligament on the inside of the anterior superior iliac spine, descending vertically. It is found during preparation of the side flap. Deep level: This plane is separated from the former by the presence of a fascial structure that continues down and externally to the fascia lata, which turns upwards to the inguinal ligament, firmly attaching to it.This fascial structure wraps the lateral thigh, unfolds to reach the sartorius constituting its own fascia and it continues to find the edge of the thigh adductor longus muscle.Between the two leaves of this fascia a space is formed known as crural canal, occupied by the femoral vessels, nerves and some deep lymph nodes. The crural ring is bounded on the outside by the taenia iliopectineal, on the inside by the lacunar ligament, above by the inguinal ligament and below by the ridge dentate reinforced by Cooper's ligament. The crural ring side is occupied by the femoral artery and in its inner side by the femoral vein. Between the femoral vein and the free edge of the lacunar ligament there is a space that is usually occupied by a lymph node (Cloquet's), which is the highest of the deep inguinal lymph nodes.This group positions itself inside the femoral canal medial to the femoral vein, collecting the lymph from the deep tissues of the lower limb and receive afferent lymphatic vessels from superficial inguinal lymph nodes. From the group of deep lymphatic network propagates along the femoral canal up to the crural ring and then to external iliac lymph nodes.Lateral to the artery and below the iliac fascia surrounding the iliopsoas muscle, the femoral nerve passes, which in turn divides a little below the inguinal ligament into its terminal branches, usually four, easily identifiable during the course of lymphadenectomy , between the medial border of the sartorius and the artery that goes under the psoas muscle aponeurosis.The femoral vein receives at the crural canal, about 4-5 cm below the inguinal ligament, the internal saphenous vein.During its course through the Scarpa's triangle the femoral artery provide numerous collateral branches, including internal and external femoral circumflex, surfacial iliac circumflex, the epigastric artery, superior and inferior external pudendal artery and the deep femoral artery. The close relationship between the deep lymph nodes and lymph vessels, on the one hand and the femoral vessels especially the vein on the another, require particular care in the "cleaning" of the main vascular trunks removing as far as possible the periadventitial tissue and adventitia during the intervention. Rev. Arg. Res. Cir 2012; 17(2):19-24. Incisión El plano cutáneo se secciona con dos incisiones ligeramente curvas que convergen en los extremos. El losange cutáneo delimitado de esta manera esta centrado en una línea moderadamente oblicua desde arriba hacia abajo y desde afuera ha- SURGICAL TECHNIQUE Patient Preparation The patient is shaved from the infraumbilical region to the pubis and then along the thigh to the knee. The skin is washed with antiseptic solutions. The intervention is performed under general anesthesia or, if the patient's condition required under epidural anesthesia. The patient is placed supine on the operating table with Fig 2. Posición del Paciente Patient Position the limb to be operated with the knee moderately flexed and rotated outward over the hip joint (Figure 2).This position is extremely important because it exposes the femoral triangle and makes its content more accessible to the surgeon. In male patients, the scrotum and genitals are covered with a gauze and moved to the opposite side or can be sutured with a sitch to the contralateral thigh. The surgeon position himself on the same side as the limb in which he will perform the surgery. Incision Fig 3 : Incisiones. Incisions cia adentro que empieza 5 cm encima y por dentro de la espina ilíaca anterosuperior y desciende hasta el vértice del triángulo de Scarpa, a unos 10-12 cm del ligamento inguinal. La utilidad de preparar este islote de piel que, por estar unido con la pieza quirúrgica se eliminara después con esta, consiste en escindir un segmento cutáneo con alto riesgo de necrosis postoperatoria. En efecto, con la preparación de los colgajos una amplia área de la piel queda privada de sus pedículos vasculares directos y el riesgo de necrosis es más grande cuanto más se aproxima al margen de sección. Algunos autores proponen una incisión en S itálica o en “palo de hockey”, que empieza con una porción vertical cerca de 5 cm sobre la pared abdominal hasta la espina ilíaca anterosuperior, desciende hacia adentro paralelamente al ligamento inguinal hasta el tubérculo pubiano y luego se torna vertical sobre el triángulo de Scarpa, para finalizar en el vértice de este. Dicha incisión presenta la ventaja práctica en los casos en que se había hecho una biopsia inguinal previa empleando una incisión horizontal, al Skin is sectioned with two slightly curved incisions that converge at the ends. The skin losange thus delimited is centered on a moderately sloping line from the top down and from the outside to the midline beginning 5 cm above and medial to the anterosuperior iliac spine and down to the apex of Scarpa's triangle, about 10 -12 cm from the inguinal ligament. The usefulness of preparing this skin islet , since it is connected with the surgical specimen to be removed, is to remove a segment with high risk of skin necrosis after surgery. Indeed, with the preparation of the flaps a wide area of the skin is deprived of its direct vascular pedicle and the risk of necrosis is larger the closer to the sectioned edge. Some authors propose a cut in italic S or "hockey stick", which begins with a vertical portion about 5 cm above the abdominal wall to the anterior superior iliac spine, down inward parallel to the inguinal ligament to the pubic tubercle and then becomes vertical on Scarpa's triangle, to finish at the top of it. This incision has the advantage in whom a previous inguinal biopsy was done using a horizontal incision, because it easily include the scar tissue within the horizontal portion of the incision and a better cosmetic and practical result. Other authors propose a more oblique incision crossing the inguinal ligament from the outside in and from the top down, saying that they assure Pag. 21 Técnica Quirúrgica / Surgical Technique general o, si las condiciones del paciente lo requieren, bajo anestesia peridural. Se coloca al paciente en decúbito dorsal sobre la mesa operatoria con la extremidad que se ha de operar moderadamente flexionada con la rodilla y rotada hacia afuera sobre la articulación de la cadera (Figura 2). Esta posición es de extraordinaria importancia porque expone el triangulo crural y hace que su contenido sea mas accesible para el cirujano. En el varón, el escroto y los genitales se cubren con una compresa y se desplazan hacia el lado opuesto o se puede suturar con un punto el escroto al muslo contralateral. El cirujano se pone del mismo lado que la extremidad en la cual opera. Técnica Quirúrgica . Surgical Technique poder incluir fácilmente el área de la cicatriz precedente en la porción horizontal de la incisión y se obtiene un resultado estético y funcional más satisfactorio. Otros autores proponen una incisión más oblicua que cruza al ligamento inguinal de afuera hacia adentro y de arriba hacia abajo, argumentando que de esta manera se garantiza un mayor respeto de las estructuras vasculares cutáneas y permitiría reducir el riesgo de necrosis de los colgajos. La Figura 3 muestra los diversos tipos de incisiones que se pueden realizar para este procedimiento. Siempre que exista una cicatriz de biopsia previa, ésta debe ser incluida en la incisión. Disección inguino-crural Se procede a preparar los colgajos cutáneos. Para este fin mientras el ayudante estira hacia arriba y al lado opuesto el borde cutáneo, se extirpa todo el tejido adiposo subcutáneo hasta el plano fascial subyacente. En la preparación de los dos colgajos el límite lateral está representado por el borde del musculo sartorio (Figura 4); el límite medial por el borde del musculo aductor mediano del muslo (Figura 5); arriba y abajo los extremos de la incisión cu- Fig 4: Disección del colgajo lateral hasta el Sartorio Lateral flap dissection until Sartorio Inguinal-femoral Dissection Skin flaps are prepared. To this end the assistant stretches upward and to the opposite side the skin flap, and all the subcutaneous fat to the underlying fascial plane is removed.In the preparation of t he two lateral flaps, the limit is represented by the sartorius muscle edge (Figure 4); the medial limit of the edge of the thigh adductor longus muscle (Figure 5); above and below the ends of the skin incision represent the boundaries of the dissection. Upward dissection should continue to expose the inguinal arch and major oblique (Figure 6). The incision should be made on the inside above the thigh adductor longus muscle and laterally to the sartorius from the inguinal ligament to Scarpa's triangle vertex . At this point by the lower end of the operative field, the trunk of the saphenous vein can be isolated in the adipose tissue thickness above the Fig 5: Colgajo medial hasta el Aductor Mediano Fig 6: Exposición de Oblicuo Mayor y Arcada Inguinal Flap medial to the adductor medium tánea representan los límites de la disección. Hacia arriba la disección se debe continuar hasta exponer la arcada inguinal y el oblicuo mayor (Figura 6). Se incide por dentro encima del musculo aductor mediano del muslo y por fuera sobre el musculo sartorio, desde el ligamento inguinal hasta el vértice triangulo de Scarpa. En este punto del extremo inferior del campo operatorio se puede aislar en el espesor del tejido adiposo suprafascial el tronco de la vena safena interna, a la cual se secciona entre ligaduras de lino (Figura 7). Ahora el cirujano estira lateralmente el plano fascial y todo el tejido que lo cubre y contiene los ganglios linfáticos inguinales, así como el tronco de la vena safena interna, y emprende una delicada disección del tejido subfascial hasta llegar junto a la pared de la vena femoral, cuya adventicia se incide y Pag. 22 a greater respect for cutaneous vascular structures and that it reduces the risk of necrosis of the flaps. Figure 3 shows the various types of incisions that can be made for this procedure. Whenever you have a previous biopsy scar, it must be included in the incision Exposure a major oblique and inguinal tract muscles levels. It should be sectioned between ligatures (Figure 7). Now the surgeon laterally stretches the fascial plane Fig 7: Safena Interna en vértice del triángulo de Scarpa. Saphenous in Scarpa’s triangle vertex and all the tissue that surrounds it and that contains the inguinal lymph nodes, as well as the trunk of the saphenous vein, and undertakes a delicate subfascial tissue dissection until near the wall of the femoral vein whose adventitia is sectioned and dissected. This maneuver allows us to correctly visualized the saphenous vein outfall into the femoral vein, so that is isolated and sectioned. All arterial and venous branches should be desprende. Esta maniobra permite evidenciar la desembocadura de la safena en la femoral, de modo que se aísla y se secciona entre ligaduras de lino. Se deben ligar las diversas ramas colaterales arteriales y venosas que van apareciendo. La disección continua hacia afuera con el aislamiento y esqueletización de la arteria femoral, Fig 8: Adventicia de vasos femorales Femoral vessels adventitia Fig 9: Linfadenectomía Terminada Completed Lymphadenectomy la cual se reconoce desplazando delicadamente la pieza quirúrgica hacia afuera para poner en tensión los tejidos periadventiciales (Figura 8). Liberada así la arteria femoral, se visualizan por fuera de ella el nervio femoral y también el musculo sartorio. La última fase de este tiempo consiste en desprender de la aponeurosis del musculo oblicuo el tejido adiposo que esta encima del ligamento inguinal. Se obtiene así la pieza operatoria representada por encima de la fascia lata por el tejido adiposo de la ingle, los ganglios linfáticos inguinales superficiales y el tronco de la vena safena interna y por debajo por la fascia del tejido conectivo periadventicial, la túnica adventicia de los vasos femorales y los ganglios linfáticos inguinales profundos. Al finalizar la disección se pueden visualizar en el campo operatorio la arteria y la vena femoral, y por fuera de la arteria el nervio crural, que justo debajo del ligamento inguinal se divide en sus ramas terminales (Figura 9). sectioned. Dissection continues laterally with isolation and skeletonization of the femoral artery, which is recognized by gently moving outward the surgical specimen in orden to put tension into the surrounding tissues (Figure 8). Once liberated the femoral artery as described, the femoral nerve and the sartorius muscle are shown. The last thing to do at this time is to detach fatty tissue above the inguinal ligament from the oblique aponeurosis. This gives the specimen represented above the fascia lata by the adipose tissue in the groin, superficial inguinal lymph nodes and trunk of the saphenous vein and underneath the fascia by the surrounding connective tissue, the adventitia of femoral vessels and the deep inguinal lymph nodes. After finishing the dissection it should be displayed in the surgery field the femoral artery and vein and the femoral nerve outside the artery, which divides into its terminal branches just below the inguinal ligament (Figure 9). Closure The inguinal ligament can be fixed with one or two stiches to Cooper's ligament, aiming to prevent and to to limit the occurrence of femoral hernias. To complete reconstruction in 1948 Baronofsky proposed a technique which consisted in rotating the sartorius muscle above the femoral vessels. For this purpose, the muscle should be isolated at its insertion into the anterior superior iliac spine and sectioned (Figure 10).The muscular body is released taking care not to damage its the vascular pedicle reaching the muscle in its middle portion.Onceprepared, the sartorius muscleit is rotated inwards and its proximal end secured with resorbable stitches to the Cierre Se puede fijar el ligamento inguinal con uno o dos puntos al ligamento de Cooper, a los efectos de limitar la aparición de hernias crurales en este sitio. Para completar la reconstrucción, en 1948 Baronofsky propuso una técnica que consiste en rotar el musculo sartorio encima de los vasos femorales. Para ello, se aísla al músculo en su inserción en la espina ilíaca anterosuperior y se lo secciona (figura 10). El cuerpo muscular se libera tomando precaución de no interrumpir el pedículo vascular que llega al músculo en su tercio medio. Preparado así, se rota al músculo sartorio hacia adentro y su extremo proximal se fija con puntos de sutura de material Fig 10: Sección del Sartorio Sartorius transection Fig 11: Sartorio cubriendo vasos Femorales. Femoral vessels covering Sartorio inguinal ligament (Figure 11). These maneuvers are important because they are a valuable resource for protection of the femoral pedicle from exposure through skin flap necrosis. In addition, the rotation of the sartorius muscle greatly reduces residual cavity that forms in Pag. 23 Técnica Quirúrgica / Surgical Technique Rev. Arg. Res. Cir 2012; 17(2):19-24. Técnica Quirúrgica . Surgical Technique reabsorbible al ligamento inguinal (figura 11). Estas maniobras son importantes porque constituyen un valioso recurso de protección para el pedículo vascular femoral en los casos en que se creen soluciones de continuidad en el plano cutáneo por necrosis de los colgajos. Además, la rotación del musculo sartorio reduce mucho la cavidad residual que se forma en el triángulo de Scarpa después de la extirpación de los ganglios linfáticos inguinocrurales y del tejido adiposo de la ingle y se elimina así un espacio muerto donde podría acumularse liquido seroso. Así como también, el musculo colocado de esta manera ofrece un plano de apoyo al cual pueden adherirse los colgajos cutáneos, que solo pueden conservar su vitalidad estando en contacto con un tejido bien irrigado como un músculo. La remoción de las acumulaciones sanguíneas y serosas se asegura con la colocación de un drenaje de látex colocado en el lecho operatorio, exteriorizado por contrabertura por debajo del extremo inferior de la herida. Se procede a realizar el cierre del tejido subcutáneo con puntos separados de material reabsorbible y finalmente el cierre de la piel con puntos separados de nylon (Figura 12). Scarpa's triangle after the removal of lymph nodes and inguinocrural fat and eliminates a dead space where serous fluid may accumulate. And also, the muscle thus positioned provides a supporting surface on which to the skin flaps can adhere, that can only retain their vitality only being in close contact with a well perfused tissue such as muscle. Removal of blood and serous accumulations is secured by placing a latex drain in the surgical bed, externalising it through counteropening below the lower end of the wound. Next step is the closure of the subcutaneous tissue with resorbable sutures and finally the closing of the skin with nylon simple stitch sutures (Figure 12) Control postoperatorio Postoperative Control No retirar el drenaje antes de los 5 a 7 días y nunca antes de que la secreción sea menor a 50 – 60 ml diarios. No indicar la deambulación antes del tercer día postoperatorio para favorecer la creación de suficientes adherencias entre el plano dérmico y el muscular. Indicar medidas de trombo profilaxis, preferiblemente HBPM. Utilizar vendaje elástico de la extremidad operada durante el postoperatorio inmediato, así como también cuando se inicia la deambulación, con el fin de reducir la incidencia de linfedema postoperatorio. La antibioticoterapia sólo es útil en presencia de signos clínicos de infección, y en caso de ser necesario utilizamos cefalosporinas de primera generación. Fig 12: Cierre de piel, celular y drenaje Skin closure and drainage Drainage removal should be done within 5 to 7 days and never before the discharge is less than 50-60 ml daily. Deambulation should not be indicated before the third postoperative day to help create sufficient adhesion between the dermal and muscular planes. Thrombus prophylaxis measures, preferably LMWH should be indicated. In order to reduce the incidence of postoperative lymphedema it is recommended thte use of an elastic bandage on the operated limb during the immediate postoperative period, as well as when walking is started. Antibiotic therapy is only usefwhen clinical signs of infection are present, and if necessary firstgeneration cephalosporins should be used. Bibliografía 1.Groshong LE. A technique for radical groin dissection. Surg Gynecol Obstet. 1973; 136:986-90. 2.Veronesi U. 1991. Cirugía Oncologica. Tumores Cutáneos. 1ra Edición. Editorial Medica Panamericana. 779-784 Pag. 24