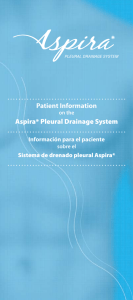
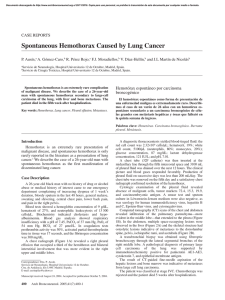
VOLUME 3 4 • NUMBER 6 • FEBRUARY 20, 2016 JOURNAL OF CLINICAL ONCOLOGY D I A G N O S I S I N O N C O L O G Y Dasatinib-Related Pulmonary Toxicity Mimicking an Atypical Infection Case Report A 49-year-old white woman with chronic myeloid leukemia (CML) presented to the hospital with several weeks of increasing dry cough, dyspnea on exertion, and low-grade fevers. She was first diagnosed with CML in chronic phase in October 2009 when she presented with marked leukocytosis and thrombocytosis. After brief cytoreduction with hydroxyurea, she was started on imatinib 400 mg daily, which she tolerated well. Approximately 8 months later, she developed marked pancytopenia, and imatinib was discontinued. Her blood counts recovered several weeks after cessation of treatment, but her bone marrow cytogenetics remained 95% Ph⫹. Therapy was then changed to dasatinib 100 mg daily, but after about 6 weeks, she again developed pancytopenia. Her blood counts recovered after dasatinib was held, but then decreased again on resuming the drug at a lower dose. Because of the lack of a cytogenetic response, in April 2011, she received an allogeneic hematopoietic stem-cell transplantation from a matched unrelated male donor after conditioning with fludarabine, melphalan, and alemtuzumab. She had no post-transplantation complications or graft versus host disease. Her bone marrow exams became morphologically and cytogenetically normal. However, her BCR-ABL quantitative polymerase chain reaction assay remained positive at a low level 1 year after transplantation, and therefore she restarted dasatinib at 100 mg daily. Within several days of starting dasatinib, she developed a dry cough that became progressively worse over the following several weeks. In addition, she experienced low-grade fevers, myalgia, and dyspnea. On admission to hospital, she was febrile to 38.7 C, tachycardic with a heart rate of 112 beats/minute, and breathing at 20 breaths/minute. She was hypoxemic, requiring 2 to 4 L of supplemental oxygen through a nasal cannula. Chest examination revealed diffuse, bilateral rales. The remainder of the physical examination was unremarkable. Her medications before admission included dasatinib 100 mg daily, valacyclovir 1,000 mg three times daily, and a multivitamin. All of her post-transplantation immunizations were up to date. Her past medical history included a 24 pack-year smoking history, although she had quit 5 years earlier. She reported no recent environmental exposures or sick contacts. Her WBC count was 5,000/L with 58% granulocytes, 24% lymphocytes, 8% monocytes, and 3% eosinophils. The hemoglobin level was 8.8 g/dL and platelets 162,000/L. Chemistries, including electrolytes and renal and liver functions, were normal. Chest radiograph revealed bilateral nodular and reticular interstitial opacities with small pleural effusions (Fig 1) that were new compared with a radiograph less than 2 months earlier. A computed tomography (CT) scan of chest showed bilateral nodular airspace opacities with diffuse ground glass components predominantly in the upper and middle lobes (Fig 2A). In addition, there was interval e46 © 2014 by American Society of Clinical Oncology Fig 1. development of mediastinal lymphadenopathy in the peritracheal, subcarinal, and pretracheal spaces. The differential for the CT findings included fungal or atypical infection, hypersensitivity reaction due to dasatinib, and possible malignancy. Treatment was initiated with broad-spectrum antimicrobials including cefepime, azithromycin, vancomycin, metronidazole, and voriconazole. Dasatinib was discontinued. She underwent a bronchoscopy with bronchoalveolar lavage and transbronchial biopsy of the right upper lobe. Fluid analysis from the washings showed a total WBC count of 360/L with 27% neutrophils, 18% lymphocytes, 54% macrophages, and 1% eosinophils. Gram stain, acid fast, bacterial, and fungal cultures returned negative for infection. Fungal stains on the biopsy specimen were negative; cytology demonstrated reactive cellular changes. There were nonspecific findings of focal lymphocytic aggregates within the lung parenchyma, mild type II pneumocyte hyperplasia, scattered fibrin exudates, mild interstitial thickening, and intra-alveolar macrophages. The remainder of the infectious work-up, including bacterial and fungal blood cultures, urine culture, respiratory viral panel, parvovirus serology, streptococcal pneumonia antigen, Legionella antigen, Aspergillus antigen, and histoplasmosis antigen returned negative. Despite 1 week of broad-spectrum antibiotic and antifungal treatment as well as discontinuation of dasatinib, her fevers persisted, and her dyspnea and hypoxia worsened. A repeat CT of the chest showed increasing nodular airspace opacities, particularly in the upper lobes, as well as interval development of bilateral pleural effusions Journal of Clinical Oncology, Vol 34, No 6 (February 20), 2016: pp e46-e48 Information downloaded from jco.ascopubs.org and provided by at UAMS Library on March 2, 2016 from 186.125.93.125 Copyright © 2016 American Society of Clinical Oncology. All rights reserved. Jasielec and Larson A B Fig 2. (Fig 2B). Because of concern for dasatinib-related pulmonary toxicity, she was started on high-dose corticosteroids (methylprednisolone 1 mg/kg/d). Within 2 days of starting steroids, her respiratory status began improving. The following week she was weaned off supplemental oxygen and was able to ambulate without dyspnea. She remained afebrile, and her cough improved. Her antibiotics were discontinued, and she was discharged home. She was tapered off prednisone over 4 weeks, and her symptoms have not recurred. Discussion The use of the tyrosine kinase inhibitors (TKIs) imatinib, dasatinib, and nilotinib has greatly improved outcomes for patients with CML. However, TKIs are not specific for bcr-abl1, and have a variety of off-target effects and unique adverse effect profiles that may be related to their differential kinase inhibition in vivo. For example, imatinib is more likely to cause fluid retention, including superficial and peripheral edema, whereas this is less common with the other two TKIs. Patients treated with nilotinib are more likely to develop elevations in pancreatic and hepatic enzymes, bilirubin, and glucose, and peripheral arterial occlusive disease has also been reported. Dasatinib is a potent second-generation TKI that is approved for patients with imatinib intolerance or resistance, as well as more recently for newly diagnosed CML.1 Pulmonary complications and especially pleural effusions are nonhematologic adverse effects of dasatinib, and more recently, cases of pulmonary arterial hypertension have also been reported.2 In clinical trials, pleural effusions occurred in approximately 10% to 20% of dasatinib-treated patients, at intervals from 5 to 28 weeks after initiation of therapy and as late as several years.3 Both higher doses (140 mg daily) and a twice-daily dosing schedule have been associated with an increased incidence of pleural effusions.4 In addition, multiple other risk factors including older age, longer duration of treatment, phase of disease (acute or blast phase), underlying autoimmune diseases, arterial hypertension, hypercholesterolemia, and rash have been correlated with the development of pleural effusions while taking dasatinib.4,5 Although the mechanism of dasatinib-associated pleural effusions has not been clearly elucidated, it is hypothesized that it may be www.jco.org related to inhibition of the SRC (v-src, sarcoma viral oncogene homolog) family of kinases expressed in lymphocytes. Furthermore, because some patients treated with dasatinib develop lymphocytosis in peripheral blood and pleural fluid, the development of pleural effusions may be an immune-mediated process.6-8 In most cases, these effusions respond to a short course of corticosteroids and diuretics and usually do not recur after resuming the drug at a lower dose.3,7 Pulmonary infiltrates and interstitial changes associated with dasatinib have not been well described. In one case series of 40 patients treated with dasatinib, nine patients (22.5%) developed pulmonary symptoms, and seven of the nine were found to have lung parenchymal changes on imaging; these included septal thickening and ground-glass opacities plus concurrent pleural effusions in about half of the patients.6 These changes occurred between 1 month and 2 years after initiation of treatment. Similar to cases of isolated pleural effusions, the pleural fluid, bronchoalveolar lavage, and pleural biopsies showed a lymphocytic predominance. In the majority of the patients, pulmonary symptoms resolved within 1 week after dasatinib interruption and did not recur in three of the four patients in whom dasatinib was restarted at a lower dose. For those with pleural effusions, diuretics were found to be ineffective. One patient was treated effectively with steroids, supporting an immune-mediated phenomenon. In addition, one other case of dasatinib-associated alveolar pneumonia that responded to steroids has been reported.9 Here we present a case of dasatinib induced interstitial lung disease that mimicked a post-transplantation pulmonary infection. Although the exact mechanism of this reaction is unclear, druginduced interstitial changes have been previously described, and the nonspecific findings on biopsies are often difficult to characterize.10 Interestingly, our patient had received dasatinib previously, before her allogeneic transplant, and had not had any pulmonary symptoms at that time. We speculate that her symptoms occurred after immune reconstitution and were secondary to some activation of the donorderived immune system. Furthermore, the lymphocyte aggregates seen on trans-bronchial biopsy as well as the brisk response to corticosteroids further support an immune-mediated drug reaction. Thus, clinicians should be aware that dasatinib causes not only isolated pleural © 2014 by American Society of Clinical Oncology Information downloaded from jco.ascopubs.org and provided by at UAMS Library on March 2, 2016 from 186.125.93.125 Copyright © 2016 American Society of Clinical Oncology. All rights reserved. e47 Diagnosis in Oncology effusions, but also striking noninfectious pulmonary parenchymal changes that may require steroid therapy. REFERENCES 2. Montani D, Bergot E, Günther S, et al: Pulmonary arterial hypertension in patients treated by dasatinib. Circulation 125:2128-2137, 2012 3. Quintás-Cardama A, Kantarjian H, O’brien S, et al: Pleural effusion in patients with chronic myelogenous leukemia treated with dasatinib after imatinib failure. J Clin Oncol 25:3908-3914, 2007 4. Breccia M, Latagliata R, Stagno F, et al: Charlson comorbidity index and adult comorbidity evaluation-27 scores might predict treatment compliance and development of pleural effusions in elderly patients with chronic myeloid leukemia treated with second-line dasatinib. Haematologica 96:1457-1461, 2011 5. Valent, P: Severe adverse events associated with the use of second-line BCR/ABL tyrosine kinase inhibitors: Preferential occurrence in patients with comorbidities. Haematologica 96:1395-1397, 2011 6. Bergeron A, Réa D, Levy V, et al: Lung abnormalities after dasatinib treatment for chronic myeloid leukemia: A case series. Am J Respir Crit Care Med 176:814-818, 2007 7. Porkka K, Khoury HJ, Paquette RL, et al: Dasatinib 100 mg once daily minimizes the occurrence of pleural effusion in patients with chronic myeloid leukemia in chronic phase and efficacy is unaffected in patients who develop pleural effusion. Cancer 116:377-386, 2010 8. Nagata Y, Ohashi K, Fukuda S, et al: Clinical features of dasatinib-induced large granular lymphocytosis and pleural effusion. Int J Hematol 91:799-807, 2010 9. Radaelli F, Bramanti S, Fantini NN, et al: Dasatinib-related alveolar pneumonia responsive to corticosteroids. Leuk Lymphoma 47:1180-1181, 2006 10. Schwaiblmair M, Behr W, Haeckel T, et al: Drug induced interstitial lung disease. Open Respir Med J 6:63-74, 2012 1. Kantarjian HM, Shah NP, Cortes JE, et al: Dasatinib or imatinib in newly diagnosed chronic-phase chronic myeloid leukemia: 2-year follow-up from a randomized phase 3 trial (DASISION). Blood 119:1123-1129, 2012 DOI: 10.1200/JCO.2013.50.1981; published online ahead of print at www.jco.org on June 23, 2014 Jagoda K. Jasielec and Richard A. Larson The University of Chicago, Chicago IL AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST Although all authors completed the disclosure declaration, the following author(s) and/or an author’s immediate family member(s) indicated a financial or other interest that is relevant to the subject matter under consideration in this article. Certain relationships marked with a “U” are those for which no compensation was received; those relationships marked with a “C” were compensated. For a detailed description of the disclosure categories, or for more information about ASCO’s conflict of interest policy, please refer to the Author Disclosure Declaration and the Disclosures of Potential Conflicts of Interest section in Information for Contributors. Employment or Leadership Position: None Consultant or Advisory Role: Richard A. Larson, Bristol-Myers Squibb (C), Novartis (C) Stock Ownership: None Honoraria: None Research Funding: Richard A. Larson, Bristol-Myers Squibb, Novartis Expert Testimony: None Patents, Royalties, and Licenses: None Other Remuneration: None ■ ■ ■ e48 © 2014 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY Information downloaded from jco.ascopubs.org and provided by at UAMS Library on March 2, 2016 from 186.125.93.125 Copyright © 2016 American Society of Clinical Oncology. All rights reserved.