Extended Day Program Emergency Card/Tarjeta de Emergencia
Anuncio

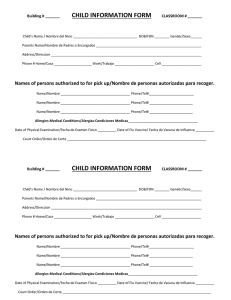
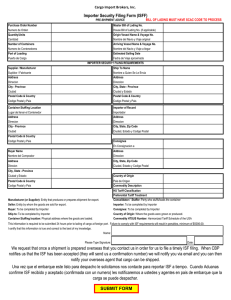
Extended Day Program Emergency Card/Tarjeta de Emergencia PLEASE PRINT OR TYPE/POR FAVOR ESCRIBA EN LETRAS DE MOLDE Grade/Grado:__________________ STUDENT NAME/NOMBRE DEL ESTUDIANTE____________________________________________________________________ Last/Apellido First/Nombre Middle/Segundo Name/Nombre (parent) Relationship/Parentesco _____________________________________________________ Name/Nombre (parent) Relationship/Parentesco Home Address/Direccion:____________________________ Home Address/Direccion:_________________________________ City/Zip/Ciudad/Codigo Postal:________________________ City/Zip/Ciudad/Codigo Postal:_____________________________ Mailing Address (if different) Direccion del Correo (si sea diferente): Birthdate/Nacimiento:_________________ Sex/El sexo: M F ______________________________________________________ Email_______________________________________________ Street/Direccion City/Ciudad Zip/Codigo Postal Email_______________________________________________ Medical Alert/Alerta Medica: Health Problems/Problemas de Salud: Allergies/Alergias: _____________________________________________________________________________________________ Medications taken regularly/Las medicinas tomadas regulamente: _______________________________________________________ (Additional information can be added on the back of the card. Se puede anadir informacion al otro lado de esta tarjeta.) In case of emergency, illness, or accident to the child named above, the school is authorized to release my child as indicated below. Number each item #1,2,3,4,5 in order of desired action. PLEASE COMPLETE ALL INFORMATION./En caso de emergencia, enfermedad o accidente del nino nombrado, la escuela esta autorizada a dejar salir el nino en la manera notada abajo. Ponga los numeros 1,2,3,4,5, para indicar en que orden. COMPLETE TODA LA INFORMACION. # CONTACT MOTHER/ Name/Nombre Llame a la madre # CONTACT FATHER/ Name/Nombre Llame a la padre # BABYSITTER/ Name/Nombre Llame a la Ninera # FRIEND/RELATIVE Name/Nombre Llame a amigo # FAMILY PHYSICIAN/ Name/Nombre Llame al medico familiar Names of other persons authorized to pick up child: Primary Tel. # Secondary Tel. # Primary Tel. # Secondary Tel. # Primary Tel. # Secondary Tel. # Primary Tel. # Secondary Tel. # Primary Tel. # Secondary Tel. # Signature of Parent/Guardian/La Firma del Padre, de la Madre, o Guardian _____________________________ Date/Fecha I/We the undersigned parent(s) of ___________________________________________, a minor and/or a student, do hereby authorize Extended Day Care Provider as agent(s) for the undersigned to consent to any xray examination, anesthetic, medical or surgical diagnosis or treatment and hospital care which is deemed advisable by, and is to be rendered under the general or special supervision of any physician and surgeon licensed under the provisions of the Medical Practices Act on the medical staff of any hospital, whether such diagnosis or treatment is rendered at the office of said physician or at said hospital. It is understood that this authorization if given in advance of any specific diagnosis, treatment or hospital care being required but is given to provide authority and power on the part of our aforesaid agent(s) to give specific consent to any and all such diagnosis, treatment or hospital care which aforementioned physician in the exercise of his/her best judgment may deem advisable. This authorization is given pursuant to the provisions of Section 25.8 of the Civil Code of California. Yo / Nosotros los padres firmantes (s) de ___________________________________________, un menor de edad y / o un estudiante, no autorizan Proveedor de Cuidado Día extendido como agente (s) para el suscrito para consentir a cualquier examen de rayos X, anestesia, diagnóstico médico o quirúrgico o tratamiento y la atención hospitalaria que se consideran aconsejable por, y es a ser prestados bajo la supervisión general o especial de cualquier médico o cirujano con licencia bajo las disposiciones de la Ley de Prácticas Médicas en el personal médico de cualquier hospital, si tal diagnóstico o tratamiento es prestado en la oficina de dicho médico o en dicho hospital. Se entiende que esta autorización si se administra antes de cualquier diagnóstico, tratamiento o centro de cuidado específico que se requiere, pero se da para proporcionar autoridad y poder por parte de nuestro agente antes mencionado (s) para dar consentimiento específico a cualquier y todo tal diagnóstico, tratamiento o atención hospitalaria que el médico mencionado en el ejercicio de su / su mejor juicio estime conveniente. Esta autorización se da conforme a las disposiciones de la Sección 25.8 del Código Civil de California. ___________________________________________________________ _________ Signature of Parent/Guardian/La Firma del Padre de la Madre o Guardian Date/Fecha