pmr new patient paperwork
Anuncio

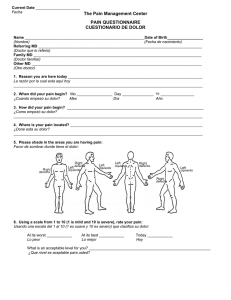
Premier Medical Rehab - LaPlace NEW PATIENT INFORMATION The following is needed so we can better serve you as a patient. PLEASE PRINT Date____________________ Patient’s full name_____________________________________________________________________ Birthdate_________________ Mailing address Age_____________ Social Security Number___________________ ________________________________________ City, State, Zip ________________________________________ Home Phone __________________ Cell Phone ___________________ Email Address _______________________________________________________ Employer _____________________________Occupation_________________ Work Phone________________ Sex: Male Female Marital Status: (circle one) Married Single Legally Separated Divorced Widowed Other ________________ Number of children __________________ Are You Pregnant? Yes No Date of your last menstrual period ________________ Emergency Contact Person/ Relationship ____________________________________Phone________________ History Information Was your injury related to: Employment / Automobile Accident / Other Date of Injury _________________________ Did you see any other doctors or were you taken to the hospital for this accident? Describe. ___________ _____________________________________________________________________________________ Have you had any surgeries in your lifetime? Yes No If yes, describe. ________________________________________________________________________ Briefly describe the pain that you are having as a result of your injury. _____________________________________________________________________________________ _____________________________________________________________________________________ Briefly describe your accident_____________________________________________________________ _____________________________________________________________________________________ Which Pharmacy do you use? _____________________________________ City/ State _____________________ Patient Name_____________________________________________ Date of Accident __________________________________________ Attorney Information Name ______________________ Address ______________________ City, State, Zip ______________________ Phone Number ______________________ Insurance Information Company ___________________________ Claim # _____________________________ Adjuster _____________________________ Adjuster Contact ______________________ Adjuster Fax__________________________ Address _____________________________ ____________________________________ Patient Name _____________________________________ Room___________ Date of Birth ______________________ Pharmacy? ______________________ Check ALL that describe your pain: (Marque todo lo que describe su dolor) O Constant (Constante) O Occasional (Ocasional) O Burning (Ardiente) (Fecha de nacimiento) Where is your pain today? (Dónde está dolor de hoy?) (Blando) O Stabbing O Numbness (Punsante) (entumecimiento) O Dull/ Aching O Pressure (Inexplicable) (Tensión) O Sharp O Tingling (Agudo) (Hormigueo) O Shooting O Nagging (Punzante) (persistente) O Throbbing O Cramping (Palpitante) (Calambres) (farmacia) O Tender O Electric (Electrico) Is your pain Better / Worse / Unchanged ? (Es tu dolor Mejor/Peor/Igual) What is your usual level of pain? Have You Had an Injection since your las visit? Yes No (Has tenido alguna injección desde tu ultima visita?) (Usualmente cual es tu nivel de dolor) Percentage of relief from Injection ____________% ¿Cual es el porcentaje de alivio de la injección? Are medications helping with your pain? ¿ Los medicamentos te están ayudando con el dolor? Well (bien) Fairly (bastante) Not Very Well (no mucho) Poorly (poco) Percentage of relief taking pain medications_________% Pain is WORSE with: Pain is BETTER with: (Porcentaje de Alivio tamando medicamentos) (Tu dolor es peor con:) O Activity (actividad) (Tu dolor es mejor con:) O Resting (descansando) Current functional level with medication: O Walking (caminando) O Lying Down (acostado) O Standing (de pie) O Turning on other side O Sitting (sentado) O Bending (doblando) O Lying Flat (acostandose) (girando el cuerpo) O Lying on recliner (nivel functional actual sin medicación) O Better O Much Improved O Very Poor O Worse O Unchanged (mejor) (Mucho mejor) (Bien poco) Fair (Peor) (ningun cambio) Quality of sleep : Good Poor (La calidad del sueño) (Bien) (razonable) (pobre) (sentadonse en un reclinable) O Driving (manejando) O Ice/ Heat (frio/caliente) Any side effects of prescribed medication? O Coughing (tosiendo) O Massage (masage) (Alguna reacción de los medicamentos recetados) O Turning Side to Side O Injections (inyecciónes) _______________________________________________ O Lifting (levantando) O Medications (medicamentos) Describe your mood: Good Fair Poor Depressed O Weather Changes (cambio de tiempo) O Going Up Stairs (subiendo escaleras) (Describe tu estado de ánimo) (Bien) (Razonable) (Deprimido) O Nothing (nada) CONTINUE TO BACK Please Circle: General: Eyes: HEENT: Psychological: (Psicologico) Fatigue (fatigado) Changes in Vision Headaches (Dolor de cabeza) Depression (Depresión) Weight Loss (Cambios en la vision) Loss of Hearing (Pérdida de audición) Anxiety (Ansiedad) Sinus Problems Difficulty Thinking (Problemas de sinusitis) (Dificultad de pensar) (Ojos) (Pérdida de peso) Respiratory Cardiovascular: Gastrointestinal: Shortness of Breath High Blood Pressure (Alta Presión) Abdominal Pain (Dolor Abdominal) Incontinence (Incontinencia) Asthma (Asma) Chest Pain (Dolor de pecho) COPD/ Emphysema Poor Circulation (Pobre circulación)Nausea/ Vomiting (Nauseas/Vomitos)Inability to Control Urine Sleep Apnea Irregular Heart Beat Heartburn (Acidez) (Dificultad de dormir) (Latidos irregulares del corazón) Constipation (Estreñimiento) Reflux (Reflujo) Urological: Kidney Stones (problemas renales) (Incapacidad de controlar la orina) Stomach Ulcer (Ulcera estomacal) Musculoskeletal: Neurological: Endocrine: Hematologic: Muscle Cramps(calambres)Trouble Concentrating Thyroid Problem (Problemas toroides)Bleeding Disorder (Sangrado) Neck Pain (Dolor de cuello) Gait Disturbance(Manchas) Diabetes Anemia Shoulder Pain (Dolor del hombre) Stroke (Ataque fulminante) Hepatitis Easy Bruising (Hematomas fácilmente) Back Pain(Dolor de espalda) Weakness (Debilidad) Blood Transfusion Joint Pain (Dolor en las articulaciones) Seizures (Ataques epilépticos) (Transfución de sangre) Joint (Articilación) Swelling (Hinchazón) Morning Stiffness (Rigidez matutina) ANY NEW ISSUES? (Algún problema nuevo) ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ OFFICE USE ONLY: (Uso de oficina solamente) VITALS: HEIGHT_____________ TEMP______________ BP_____________ RESP.____________