insurance demographic information form
Anuncio

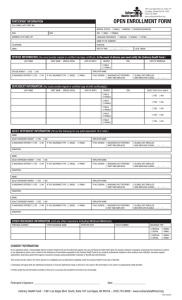
Houston Methodist Wellness Services INSURANCE DEMOGRAPHIC INFORMATION FORM *Please provide a COPY front and back of your insurance card at the time of your appointment* *Por favor proporcione una copia del frente y el dorso de la tarjeta del seguro medico en su primera cita* Your name as it appears on insurance card: Su nombre tal como aparece en la tarjeta de seguro: First Name Last Name Primer nombre Apellido Current Mailing Address and Telephone: Dirección actual y teléfono: Street or P.O. Box Calle o Apartado Postal City State Zip Code Telephone Ciudad Estado Código postal Teléfono Gender: Date of Birth MM DD YYYY F M Social Security Number Sexo Fecha de cumpleaños Número de la seguro social Insurance Information: Información de Seguros Insurance Carrier Insurance P.O. Box Address Compania Aseguradora apartado postal de seguro Policy Number/ Member ID Group Number Número de Póliza / identificación de miembro Número de grupo CPT Code: 90661 CPT Administration: 90471 Diagnosis Code: Z 23 The information cited on the form above is correct and complete. I understand that I am responsible for any portion of my bill not covered through my insurance plan, I authorize The Methodist Hospital physician Organization to act as an agent in obtaining payments from my insurance company. I authorize the release of medical information to all parties involved in my care. I agree to allow copies of this authorization to be used in place of an original. I authorize the use of “signature on file” to be used in insurance claim submissions which authorizes payment to be sent directly to the physician. I understand that I am responsible for notifying the office of any pre-certification or referral requirements my insurance company may have. Signature of patient or authorized agent Firma del paciente o agente autorizado Date Fecha