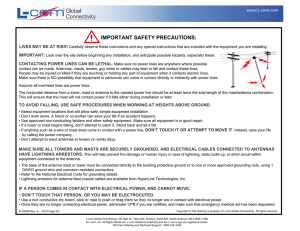
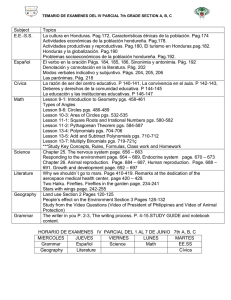
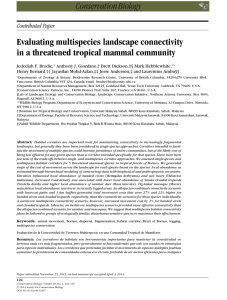
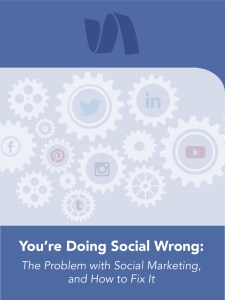
British Journal of Neurosurgery ISSN: 0268-8697 (Print) 1360-046X (Online) Journal homepage: www.tandfonline.com/journals/ibjn20 Individualised connectomic-guided radiosurgical thalamotomy for chronic pain Eduardo Lovo, Flavia Venetucci Gouveia, Jurgen Germann, William Omar Contreras, Eduardo Joaquim Lopes Alho, Claudia Cruz & Luis BermúdezGuzmán To cite this article: Eduardo Lovo, Flavia Venetucci Gouveia, Jurgen Germann, William Omar Contreras, Eduardo Joaquim Lopes Alho, Claudia Cruz & Luis Bermúdez-Guzmán (08 Sep 2025): Individualised connectomic-guided radiosurgical thalamotomy for chronic pain, British Journal of Neurosurgery, DOI: 10.1080/02688697.2025.2557210 To link to this article: https://doi.org/10.1080/02688697.2025.2557210 © 2025 The Author(s). Published by Informa UK Limited, trading as Taylor & Francis Group. Published online: 08 Sep 2025. Submit your article to this journal Article views: 383 View related articles View Crossmark data Full Terms & Conditions of access and use can be found at https://www.tandfonline.com/action/journalInformation?journalCode=ibjn20 BRITISH JOURNAL OF NEUROSURGERY https://doi.org/10.1080/02688697.2025.2557210 SHORT REPORT Individualised connectomic-guided radiosurgical thalamotomy for chronic pain Eduardo Lovoa, Flavia Venetucci Gouveiab, Jurgen Germannc, William Omar Contrerasd, Eduardo Joaquim �dez-Guzm�ang,h Lopes Alhoe, Claudia Cruzf, and Luis Bermu a Neurosurgery, Gamma Knife Program, International Cancer Center, Diagnostic Hospital, San Salvador, El Salvador; bNeuroscience and Mental Health, Hospital for Sick Children, Toronto, Canada; cCenter for Advancing Neurotechnological Innovation to Application (CRANIA), Krembil Brain Institute, Toronto, Canada; dInternational Neuromodulation Center-NEMOD, UNAB University, Bucaramanga, Colombia; eNeurocirurgia, Cl�ınica de Dor e Funcional, S~ao Paulo, Brazil; fAlgology, Pain Management Program, International Cancer Center, Diagnostic Hospital, San Salvador, El Salvador; gCancer Research UK Cambridge Institute, University of Cambridge, Cambridge, UK; hRobotic Radiosurgery Center, Costa Rican Oncology Center, San Jos�e, Costa Rica ABSTRACT ARTICLE HISTORY Introduction: Radiosurgery targeting the thalamus has long been used to treat refractory pain, with medial thalamotomy as a key approach. Traditionally, targeting relied on indirect methods based on anatomical atlases, which do not account for individual variations in brain connectivity. Recent advances in connectomic-guided stereotactic radiosurgery have improved precision in the treatment of movement disorders, but their application to pain management remains underexplored. This study evaluates the feasibility of connectomicguided radiosurgery for refractory pain using Brainlab Elements, integrating autosegmentation and manual contouring for patient-specific planning. Methods: We analysed the thalamic target’s structural and functional connectivity using the FMRIB Software Library and Advanced Normalisation Tools. The region of interest (ROI) was mapped using diffusion tensor imaging and functional magnetic resonance imaging to assess connectivity with pain-processing structures, including the periventricular grey (PVG) and ventroposteromedial (VPM) nucleus. Connectivity analysis was performed with Brainlab Elements and validated against independent connectomic studies. Dose-volume relation­ ships for PVG and VPM were retrospectively assessed in patients treated with radiosurgery for chronic pain. Results: Connectivity analysis showed that fibres within the ROI extend to primary motor (M1) and sensory (S1) cortices, while descending fibres reach the periaqueductal gray (PAG). Functional connectivity linked the ROI to key pain-processing regions, including the pre­ frontal cortex, insula, amygdala, and cerebellum. Retrospective dose-volume (DVs) analysis revealed clear differences between the volumes receiving more than 20 Gy in the original vs connectomic-based target. . The integration of Brainlab Elements facilitated connectomicguided targeting, enabling a patient-specific approach to radiosurgery. Conclusion: Connectomic-guided radiosurgery is a feasible approach that enables precise, patient-specific targeting pain management. Auto-segmentation of PVG and VPM allows dose-volume assessment, potentially correlating with clinical outcomes. Standardising connectomic-guided planning may enhance radiosurgical precision and support future clin­ ical research in refractory pain. Received 13 May 2025 Revised 22 July 2025 Accepted 2 September 2025 Introduction Radiosurgical thalamic targeting for refractory pain dates back to Lars Leksell’s development of the Gamma Knife.1 Traditional medial thalamotomy, typ­ ically involving the centromedian and parafascicular CONTACT Luis Berm�udez-Guzm�an Costa Rica [email protected] KEYWORDS Connectomic-guided radio­ surgery; thalamotomy; refractory pain; diffusion tensor imaging (DTI) complex, has been well-documented and used both unilaterally and bilaterally for managing oncological and non-oncological pain. Recently, its application has expanded to include refractory trigeminal neuralgia, chronic facial pain, and other neuropathic pain syn­ dromes, although the outcomes vary.2–9 Robotic Radiosurgery Center, Costa Rican Oncology Center, San Jos�e, � 2025 The Author(s). Published by Informa UK Limited, trading as Taylor & Francis Group. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives License (http://creativecommons.org/licenses/bync-nd/4.0/), which permits non-commercial re-use, distribution, and reproduction in any medium, provided the original work is properly cited, and is not altered, transformed, or built upon in any way. The terms on which this article has been published allow the posting of the Accepted Manuscript in a repository by the author(s) or with their consent. 2 E. LOVO ET AL. Despite these advances, all of these procedures have relied on indirect anatomical targeting, localising structures based on standard atlases, predefined stereotactic coordinates, or anatomical landmarks. This method does not account for interindividual ana­ tomical variability and does not incorporate functional connectivity data, limiting its precision. Unlike inva­ sive procedures such as deep-brain stimulation or high-intensity focused ultrasound, radiosurgery does not allow for real-time physiological validation. A more patient-specific targeting strategy is therefore essential to improve precision and clinical efficacy. Recent advances in functional and structural neuro­ imaging now permit the use of each patient’s unique brain-connectivity maps to guide stereotactic plan­ ning. One pioneering application (recently introduced for tremor treatment) retrospectively identified an optimal lesion ‘sweet spot’ by correlating clinical out­ comes with connectivity to the primary motor cortex.10 While connectivity-based targeting is gaining traction in movement disorders, its potential applica­ tion in pain management remains largely unexplored. In our previous work, we evaluated the outcomes of unilateral radiosurgical thalamotomy using indirect targeting in a cohort of 14 patients with refractory pain, reporting a long-term success rate of 50%.2 That study also generated three-dimensional models of the target region (using the S~ao Paulo-W€ urzburg Atlas of the Human Brain) to suggest an initial coordinate set (X: 4–4.5 mm, Y: 4 mm, Z: þ4 mm relative to the anterior commissure-posterior commissure line). While this provided a useful starting framework, it did not leverage patient-specific connectivity data to refine the target further. Building on that foundation and our later observa­ tions that the 20 Gy isodose can overlap with the med­ ial dorsal parvocellular nucleus (MDpc) (which may modulate the affective/cognitive dimensions of pain),5 we refined our targeting by lowering the Z coordinate by 2 mm, optimising coverage of the centromedianparafascicular (CM-Pf) complex, which aligns approxi­ mately with the 0 mm Z-axis (relative to the anterior commissure-posterior commissure line). This refine­ ment was guided by the concept of a neuromodulatory ‘area of influence’, corresponding to the 20 Gy isodose line.11 This threshold was selected based on preclinical studies demonstrating neuronal spiking and metabolic activity alterations at subnecrotic radiation doses,12 as well as empirical clinical observations.13 More recently, we have integrated Brainlab Elements (Brainlab, Munich, Germany) into our Gamma Knife workflow to enable automated PVG/PAG and VPM segmentation, as well as fibre-tracking within the ROI. Critically, the connectomic analyses presented here con­ firmed that the irradiated thalamic region projects not only to the primary motor (M1) and sensory (S1) corti­ ces via the corticospinal tract, but also to descending pathways targeting the periaqueductal and periventricu­ lar grey. In addition, projections were observed to a broad corticolimbic network, including the somatosen­ sory and premotor cortices, prefrontal regions, insula, temporo-occipital junction, and posterior cingulate, highlighting the PVG/PAG as a key node in pain modulation. This technical report details the incorporation of connectomic data into the refinement of thalamic radiosurgical targeting for pain, describing our current patient workflow, connectivity analyses, and updated targeting methodology. Additionally, we provide retro­ spective dose-volume comparisons for target struc­ tures, with radiation doses ranging from 100 to 140 Gy, which have demonstrated clinical efficacy2,5,6 in various forms of refractory pain, hopefully provid­ ing preliminary reference points for future target adjustments based on such parameters. Methods Structural connectivity analysis ROI segmentation and normalisation Starting from the post-operative MRI of a patient treated with a 140 Gy thalamotomy for pain, we first segmented the contrast-enhancing lesion (the target ROI) using FMRIB Software Library tools. This ROI was then normalised to standard space (ICBM 2009b NLIN asymmetric) using transformations derived from rigid post-to-pre-operative image alignment and full non-linear pre-operative to Montreal Neurological Institute (MNI) space registration with Advanced Normalisation Tools. Tractography and fibre density mapping Brain-wide structural connectivity was examined using a 12 million-fibre whole-brain tractography template. All streamlines intersecting the ROI were identified, and fibre density maps were generated and compared to the XTRACT Human Connectome Project Probabilistic Tract Atlas. Functional connectivity analysis Resting-State fMRI processing Functional connectivity was assessed via resting-state fMRI by analysing blood oxygen level-dependent BRITISH JOURNAL OF NEUROSURGERY (BOLD) signal correlations between the ROI and other brain voxels. A whole-brain r-map was produced, con­ verted into a t-map using the known p-distribution, and corrected for multiple comparisons (p < 0.05, whole-brain voxel-wise Bonferroni correction). Alternative connectivity analysis approach ROI definition and ellipsoid generation Based on the same data set from the MRI used for structural connectivity analysis, the ROIs were defined in MNI space by transforming stereotactic coordinates into MNI (ICBM 152) coordinates (x ¼ ±4 mm, y ¼ −20 mm, z ¼ þ2 mm). A customised Python script was used to generate ellipsoid ROIs based on the diameters of the 50% isodose curve of the prescription dose and the isodose line corresponding to 20 Gy. These ROI masks were imported into DSI Studio soft­ ware (https://dsi-studio.labsolver.org/), where a group connectome template, constructed from 1021 subjects, was used for analysis. Data acquisition and reconstruction A multishell diffusion scheme was implemented with b-values of 990/1985/2980 s/mm2, each with 90 diffu­ sion sampling directions. Imaging was acquired at an in-plane resolution and slice thickness of 1.25 mm. Diffusion data were reconstructed in MNI space using q-space diffeomorphic reconstruction to obtain the spin distribution function, employing a diffusion sam­ pling length ratio of 2.5 and an output resolution of 1 mm. Deterministic fibre-tracking A deterministic fibre-tracking algorithm, incorporating augmented tracking strategies, was used to enhance reproducibility. Parameters included a randomly selected anisotropy threshold between 0.5 and 0.7 (Otsu threshold) and an angular threshold between 45� and 90� . Tracks shorter than 30 mm or longer than 200 mm were excluded, with a total of 1,000,000 seed points placed for tractography. Connectivity-based treatment planning & workflow Pre-treatment imaging One day before treatment, patients underwent axial T1weighted gadolinium-enhanced MRI (1 mm slice thick­ ness, no spacing), diffusion tensor imaging (DTI), and a 1-mm axial T2-weighted sequence covering the thalamic region (from the corpus callosum to the trigeminal 3 nerve). Imaging was performed using a 1.5 Tesla Siemens Avanto MRI scanner (Siemens, Erlangen, Germany). A standard diagnostic computed tomography (CT) scan of the head is also acquired with 1 mm slice thickness. Segmentation and co-registration Connectivity planning using Brainlab Elements (https:// www.brainlab.com/) enabled clinical verification of the ROI with patient-specific connectomics based on DTI tract reconstruction. This process included automatic segmentation of key anatomical structures such as the PVG/PAG, VPM, M1, S1, amygdala, and cerebellum, as well as manual contouring of the insular lobes. Image fusion and distortion correction On the day of treatment, we first aligned the planning MRI and CT using Elements Image Fusion. We then co-registered the DTI to the T1-weighted MRI and ran Elements Distortion Correction Cranial, which compares the MRI against the CT to flag any geomet­ ric distortions greater than 1 mm within the thalamic volume. Although distortions above this threshold were detected, we did not apply the correction, opting instead to use the T1-weighted MRI as our distortionfree reference for all DTI and diffusion-weighted sequences used in subsequent fibre tracking. Treatment setup and verification Using Elements Trajectory Planning, all images were aligned to the anterior commissure-posterior commis­ sure (AC-PC) line. In the Elements Basal Ganglia Atlas, auto-segmented structures (including the PVG/ PAG, VPM, M1, S1, amygdalae, and cerebellum) were selected. Additional regions of interest (ROIs), such as the insula, orbitofrontal cortex (OFC), and superior frontal gyrus (SFG), were manually contoured. Small ROIs were then placed bilaterally between the PVG and VPM at 2 mm above the AC-PC line. These were labelled as the left and right planning target volumes (PTVs), although no specific volumes were defined at this stage, as these ROIs served solely as connectivity seeds. In Elements FiberTracking, specific ROI combina­ tions were used to generate distinct connectivity maps: OFC þ PVG, representing the descending pain pathway; PVG alone, showing projections to the OFC and M1; SFG þ ipsilateral PTV, or SFG alone, illus­ trating the medial pain pathway; M1 þ S1 þ VPM, highlighting the lateral spinothalamocortical pathway; PVG þ PTV þ VPM, providing a comprehensive con­ nectivity map of the target region. 4 E. LOVO ET AL. The connectomic-defined target was identified at the thickest and most central portion of the medial spinothalamic tract, and its coordinates were recorded for treatment planning. Once all imaging data and segmentations were transferred to GammaPlan (GP), the left and right PTVs, PVG/PAG, and VPM were registered to the patient’s profile. The AC-PC line was marked in GP, and functional targets were incorpo­ rated using the coordinates derived from Elements software. Dose prescription varied by clinical indication: 140 Gy (unilateral) or 120 Gy (bilateral) for benign conditions such as chronic facial or neuropathic pain, and 90 Gy (under a triple-strategy protocol) for onco­ logical pain, ensuring that the 20 Gy isodose line encompassed part of both the PVG and VPM. After final approval, the patient is positioned in the GK suite, and a ‘time-out’ is conducted to confirm identity, pathology, treatment team, and correct place­ ment of the Vantage frame (Elekta, Stockholm, Sweden) under local anaesthesia. The patient is positioned at a 90� angle in the trunnion, and High-Definition Motion Management is activated to halt treatment in the event of frame slippage or cranial movement >1 mm. A cone-beam CT scan is acquired and co-registered to the planning CT. The neurosurgeon, radiation oncologist, and physicist verify alignment before treat­ ment initiation. Following treatment, the frame is removed, and patients are discharged with instructions to take paracetamol (500 mg-1 g every 8 hours) for any discomfort at pain sites. Patients maintain their base­ line pain medications and are followed daily for 15 days, then every 15 days thereafter to assess treatment response. somatosensory and premotor cortices, medial and dorsolateral prefrontal cortices, insula, temporo-occipital junction, and posterior cingulate cortex (Figure 1(C)). These connectivity patterns align with our radiosurgi­ cal targeting strategy, which focuses on the parvocellular section of the VPM nucleus and the centromedianparafascicular (CM-Pf) complex in the medial thalamus, both implicated in relaying sensory signals related to pain perception. We ensure that these regions receive radiation doses exceeding 20 Gy within the treatment zone, aiming to modulate thalamic activity and relieve chronic pain. The convergence of anatomical, functional, and treatment-planning data reinforces the ROI as a therapeutically relevant target for pain management. To further validate the targeting accuracy and net­ work engagement, we conducted a complementary tractography-based analysis using the 20 Gy isodose line volume as a seed. This analysis identified a total of 1483 fibre tracts (Figure 2), with the majority pro­ jecting to the superior frontal gyrus (SFG; 669 tracts), followed by the lateral orbital cortex (217 tracts), pars orbitalis (60 tracts), pars triangularis (49 tracts), and pre-central gyrus (M1) (26 tracts). Notably, no fibres reached the post-central gyrus (S1). A more stringent analysis using the inner 50% isodose level of 140 Gy yielded 772 tracts, again showing dominant connectiv­ ity to the SFG (306 tracts), with additional projections to the lateral orbital cortex (129 tracts) and pars orbi­ talis (39 tracts). These findings provide additional sup­ port for the functional integration of the target ROI within pain-relevant cortical networks. Results Building on these anatomical and tractographic findings, we translated connectivity insights into the clinical work­ flow through connectivity-guided treatment planning and dose-volume analysis. One day before radiosurgery, patients underwent axial T1-weighted gadoliniumenhanced MRI (1 mm slice thickness, no spacing), diffu­ sion tensor imaging (DTI), and a 1-mm axial T2weighted sequence covering the thalamic region (from the corpus callosum to the trigeminal nerve). Integration of Brainlab Elements into the clinical pipeline enabled patient-specific connectomic validation of the ROI using DTI-based tract reconstruction. Key pain-related struc­ tures (including the PVG/PAG, ventral posteromedial nucleus (VPM), M1, S1, amygdala, and cerebellum) were automatically segmented, with manual contouring per­ formed for additional regions such as the insula, orbito­ frontal cortex (OFC), and superior frontal gyrus (SFG). Structural and functional connectivity analysis Structural and functional connectivity mapping in stand­ ard space revealed that fibres originating from the target region of interest (ROI) consistently extended to both the primary motor cortex (M1) and primary sensory cortex (S1) via the corticospinal tract (Figure 1(A)). Additionally, descending projections, particularly M1, were observed reaching the periaqueductal grey (PAG) through the periventricular grey (PVG). Fibre density maps (Figure 1(B)) confirmed strong white matter con­ nectivity with these regions, supporting the anatomical relevance of the selected ROI in pain modulation. Functional connectivity analysis further demonstrated robust connections between the ROI and several cortical and subcortical structures, including the cerebellum, Connectivity-guided treatment planning and dosevolume analysis BRITISH JOURNAL OF NEUROSURGERY 5 Figure 1. ROI and Structural and Functional Connectivity Analyses. (A) The target ROI (red) is shown in axial, coronal, and sagittal views. (B) Structural connectivity analysis reveals fibres extending from the ROI (blue), travelling via the corticospinal tract, and reaching the PAG. (C) Functional connectivity analysis identifies the cerebellum and multiple cortical areas as functionally con­ nected to the ROI. The lesion ROI and connectivity maps are overlaid on a high-resolution MRI template in MNI space. Abbreviations: ROI: region of interest; PAG: periaqueductal grey; mPFC: medial prefrontal cortex; dlPFC: dorsolateral prefrontal cor­ tex; MNI: Montreal Neurological Institute. PVG/PAG segmentation enabled dose-volume quantifica­ tion of the radiosurgical shot, while delineation of other structures contributed critical data for refining treatment parameters using the Gamma Knife Icon system and GammaPlan. To guide targeting within functionally relevant pain networks, connectivity maps were generated to iden­ tify three principal pathways: the descending pain pathway (PVG ¼ OFC þ M1), the lateral pain pathway (M1 þ S1 þ VPM), and the medial pain pathway (SFG þ ipsilateral planning target volume), providing a comprehensive, patient-specific connectivity map to support precise dose delivery (Figure 3). To further enhance treatment precision, we refined the initial target coordinates based on connectivity data. Anatomically, the refined target aligns with the thickest and most central portion of the medial spinothalamic tract bundle, anchoring the isocentre coordinates used during treatment (Figure 4(A)). After image acquisition and segmentation, all relevant struc­ tures, including the left and right planning target vol­ umes (PTV), PVG/PAG, and VPM, are transferred and registered within the GammaPlan system under the patient’s profile. The anterior commissureposterior commissure line is defined, and functional targets are added using connectomic-based coordinates derived from Brainlab Elements (Figure 4(B)). Dose prescription is adapted to clinical indication: for benign conditions such as chronic facial or neuro­ pathic pain, a unilateral dose of 140 Gy or a bilateral dose of 120 Gy is used; for oncological pain, a triplestrategy protocol of 90 Gy is applied. In all cases, the 20 Gy isodose line is shaped to encompass key struc­ tures within the PVG and VPM, ensuring optimal 6 E. LOVO ET AL. Figure 2. A 3D Connectivity Analysis of the Radiosurgical Shot. (A) The shot is represented as a sphere from which fibres emanate, with the SFG hidden to reveal connectivity to the OFC (pink). (B) The left pars orbitalis (light green) is included. (C) The SFG is dis­ played separately as the primary connectivity site. (D) All cortical connections related to the shot are visualised. Abbreviations: 3D: three-dimensional; SFG: superior frontal gyrus; OFC: orbitofrontal cortex. engagement of pain-modulating pathways (Figure 4(C,D)). Retrospective dose-volume analysis of a patient treated for cancer pain revealed that this refine­ ment significantly increases the volume of the periaque­ ductal and periventricular grey (PVG/PAG) receiving >20 Gy (Table 1). After final approval, patients were positioned in the Gamma Knife (GK) suite for treatment delivery (Figure 5). A standardised ‘time-out’ procedure was per­ formed to confirm patient identity, pathology, and correct placement of the Vantage frame (Elekta, Stockholm, Sweden), applied under local anaesthesia. Patients were aligned at a 90� angle within the trunnion, and High-Definition Motion Management (HDMM) was activated to automatically pause treatment in the event of frame slippage or cranial motion exceeding 1 mm. A cone-beam CT scan was acquired and coregistered to the planning CT, allowing the neurosur­ geon, radiation oncologist, and physicist to verify align­ ment before treatment initiation. Following the BRITISH JOURNAL OF NEUROSURGERY 7 Figure 3. Pathway generation in brainlab elements. (A) The OFC is manually delineated, while the PVG/PAG is auto-segmented. These structures are added to the ‘Include Regions’ section, generating the descending pain pathway. (B) Lateral Spinothalamic Tract Generation. The precentral and postcentral gyri (M1, S1) and the VPM are auto-segmented and selected in ‘Include Regions’, automatically generating the lateral spinothalamic tract. (C) Medial Pain Pathway Generation. The SFG and a small region of inter­ est (PTV left) at 2 mm above the AC-PC line are manually drawn. The PVG/PAG and VPM are auto-segmented. These structures are added to ‘Include Regions’, generating the medial pain pathway. D-E) Global connectivity from the ROI. Lateral 3D view of all fibres extending from the ROI, which corresponds to a 5.6 mm diameter region at 2 mm above the AC-PC line, matching the 50% iso­ dose line (left). The same lateral view is shown, displaying all relevant structures involved in pain perception and regulation (right). Abbreviations: M1: primary motor cortex; S1: primary sensory cortex; VPM: ventroposteromedial nucleus; 3D: three-dimensional. OFC: orbitofrontal cortex; PVG: periventricular grey; PAG: periaqueductal grey. SFG: superior frontal gyrus; PTV: planning target vol­ ume; VPM: ventroposteromedial nucleus; AC-PC: anterior commissure-posterior commissure; ROI: region of interest. procedure, the frame was removed, and patients were discharged. This patient-specific workflow enabled integration of anatomical and connectivity data directly into the treat­ ment planning algorithm, refining coordinates for a fully connectomic-driven targeting approach. Importantly, the incorporation of PVG segmentation allowed for quantifi­ cation of dose-volume delivery to these key painmodulatory regions, an advancement not previously feasible with standard radiosurgical protocols. Verification of the clinical workflow showed that pretreatment imaging (MRI, DTI, CT) was successfully fused and aligned to the AC-PC line, with geometric distortion correction and co-registration ensuring accur­ ate spatial localisation. Intra-procedural assessments con­ firmed proper frame placement and minimal cranial movement (<0.5 mm), validating the implementation of refined target coordinates during GK treatment. Collectively, both structural and functional connectivity analyses confirmed that the region of interest (ROI) 8 E. LOVO ET AL. Figure 4. Target Refinement in Brainlab Elements Trajectory Planning and GammaPlan Integration. (A) The refined target corre­ sponds to the thickest fibre bundle of the medial pain pathway (green), marked with an orange trajectory in sagittal and coronal views, showing its relationship to the VPM and PVG. The tract is turned off to clearly visualise the coordinates before exporting to GammaPlan (bottom part). (B) GammaPlan Integration. Axial, coronal, and sagittal screenshots of GammaPlan displaying AC-PC alignment (green boxes) and imported elements from Brainlab software: VPM (red, lateral), PVG (blue, medial), and the expected 50% and 20 Gy isodose lines for a bilateral 4 mm, 90 Gy shot. Functional target selection in GammaPlan, with Brainlab-derived coordinates marked by green crosshairs bilaterally, is also shown (bottom part). (C) Dose prescription Variations in gammaPlan. Bilateral 4 mm shots prescribing 90 Gy DMax and Bilateral 4 mm shots prescribing 120 Gy DMax. (D) Unilateral shots prescribing 100 Gy and 120 Gy DMax, respectively. In all images, the outermost isodose line represents the 20 Gy threshold. Abbreviations: VPM: ventroposteromedial nucleus; PVG: periventricular grey; AC-PC: anterior commissure-posterior commissure; PVG: periventricular grey; DMax: maximum dose. BRITISH JOURNAL OF NEUROSURGERY 9 Table 1. Retrospective calculation of dose-volume effects from connectomic target refinement in a patient treated with tripletarget radiosurgery for cancer pain. Dose (Gy) 140 140 120 120 100 100 Coordinate Original Connectomic-based Original Connectomic-based Original Connectomic-based PVG volume receving >20 Gy (cc) 0.012 0.023 0.009 0.021 0.007 0.018 % PVG receving >20 Gy 50 96 39 89 27 76 Dmax 62.6 94 53.7 80.6 26 67 Median D 23 42 9 36 7.5 30 VPM volume receving >20 Gy (cc) 0.012 0.016 0.006 0.012 0.002 0.008 % VPM receiving >20 Gy 12 15 6 11 2 7 Dmax 39 83 33.6 71 36.6 60 Median D 14 13.5 12.1 11.6 7.8 9.6 Abbreviations: PVG: Periventricular Gray; Dmax: Maximum dose; Median D: Median dose; VPM: Ventral posteromedial nucleus. Figure 5. Patient positioning and motion tracking in gamma knife radiosurgery. (A) Frontal view of the patient with the Vantage frame fixed to the skull and coupled to the trunnion at a 90� angle, with a CBCT scan in progress. A fiducial marker for HDMM is placed on the patient’s nose. (B) Lateral view showing the Vantage frame, trunnion, and motion tracker. HDMM ensures movement remains below 1 mm, typically <0.5 mm, throughout treatment. Abbreviations: CBCT: cone-beam computed tomography; HDMM: high-definition motion monitoring. maintains robust connections to pain-processing areas, with the superior frontal gyrus (SFG) emerging as a pre­ dominant node. The connectivity-guided adjustment of the Z coordinate improved dose distribution to the PVG/ PAG, enhancing modulation of pain pathways. The revised, patient-specific workflow (incorporating advanced segmentation, connectivity mapping, and dose-volume quantification) underscores the potential clinical value of a connectomic-guided radiosurgical strategy for chronic pain management. Discussion Radiosurgical refinement in essential tremor has demon­ strated the value of combining anatomy with tractogra­ phy.12,14,15 Yet, thalamic radiosurgery for pain has remained dependent on atlas-based, indirect targeting. Pain engages a far more distributed and multilayered network than tremor, and consensus on optimal radio­ surgical targets remains elusive. Most existing approaches continue to rely on indirect atlas measurements, such as the Schaltenbrand-Wahren microseries.2,3,7,8 Historically, our own planning followed this convention, using sagittal and axial placements derived from stereotactic atlases. The functional and connectomic analyses presented here, however, represent a pivotal shift: by mapping each patient’s network, Brainlab Elements enables a move from one-size-fits-all planning to truly individualised treatment. This shift is especially relevant in the context of multiple-site targeting, a strategy increasingly explored in pain radiosurgery. The principle first appeared in post-herpetic trigeminal neuralgia, where three patients received Gamma Knife treatment at two sites: 60–80 Gy to the trigeminal nerve and 120–140 Gy to the centro­ median nucleus.4 Though preliminary, this series 10 E. LOVO ET AL. illustrated that engaging both peripheral and central nodes may enhance analgesia more effectively than single-target approaches. Our own experience supports this model. In a cohort of 21 patients with chronic facial pain, we observed rapid (>50% within seven days), dose-dependent relief when the thalamus received 140 Gy, significantly out­ performing 120 Gy or lower, whereas trigeminal nerve dosing showed no such correlation.6 This dual-target strategy suggests that higher thalamic doses may more effectively engage descending and lateral pain pathways within the 20 Gy isodose ‘area of influence’. In contrast, our recent triple-target approach for intractable cancer pain used lower radiation doses (90 Gy) across the pitu­ itary and bilateral thalami, achieving substantial reduc­ tions in VAS scores and medication requirements, with minimal side effects and improved quality of life.16 These findings highlight a critical insight: robust anal­ gesia may result from either higher doses to select nodes or synergistic modulation across multiple circuits, even at non-ablative levels. These observations raise fundamental questions: which target, or combination of targets, drives the greatest clinical benefit? Does efficacy arise from a dominant node, or concurrent modulation of several interconnected structures? Prospective, comparative tri­ als that incorporate each patient’s connectome will be essential to answer these questions and advance a truly circuit-based intervention for pain. Our current meth­ odology suggests that connectomic-guided targeting can increase the volume of the PVG and VPM receiv­ ing �20 Gy, potentially resulting in better outcomes. The PVG/PAG is a well-established component of the descending pain pathway17 while the VPM nucleus of the thalamus is critical for relaying somatosensory information, particularly from the face and head.18 Our approach also provided insights into prefrontal con­ nectivity with the PVG/PAG, hippocampus, thalamus, insula, and amygdala, regions integral to pain process­ ing and regulation.19 Ascending nociceptive afferents pass through the PVG/PAG to the thalamus, while descending modulation regulates dorsal horn activation in response to peripheral stimuli. The thalamic region between the PVG and VPM, where the shot is typically centred, is also linked to the CM-Pf complex and the medial pain pathway, which mediates the affectiveemotional dimensions of pain.2,5,20 While our current treatment algorithm does not expli­ citly target the PVG or VPM, the ability to retrospect­ ively assess dose-volume relationships and potentially correlate them with clinical outcomes could represent an important step towards refining connectomic-based targeting. Reporting these values across various strategies and doses provides a foundational dataset for future opti­ misation. Prospective validation using patient-specific, connectivity-guided planning remains a critical direction for future research. Conclusions Connectomic-based radiosurgery for pain is feasible using the commercially available Brainlab Elements software. Auto-segmentation and manual contouring of brain regions enable patient-specific treatment planning. We successfully correlated and validated our current patient planning workflow with independent functional connectomic studies, leading to its adoption at our centre. The ability to auto-segment the PVG and VPM nucleus also allows for volume and dose measure­ ments, which may facilitate future correlations with clinical outcomes. A key contribution of this technical report is the establishment of a more standardised approach to treatment planning and delivery, which could help unify target selection across the radiosurgi­ cal community. This standardisation may, in turn, stimulate further clinical research and trials on refrac­ tory oncological and non-oncological pain. Current limitations include the restricted number of thalamic structures that can be auto-segmented for pain treatment. The addition of the CM-Pf complex would be a valuable enhancement. Further research is also needed to explore additional potential radiosur­ gery targets and determine the optimal radiation doses for maximum therapeutic effectiveness. Acknowledgements We acknowledge and deeply appreciate Bogdam Valcu and Rebecca Ljungqvist from Brainlab Elements for their critical guidance on optimising the operation of the software Elements. Disclosure statement No potential conflict of interest was reported by the author(s). Ethical approval Written informed consent was obtained from the patients for their anonymised information to be published in this article. Ethical approval to report this series was obtained from a local research ethics committee (Comit�e Nacional de Etica de la Investigaci� on en Salud - CNEIS/2022/10). BRITISH JOURNAL OF NEUROSURGERY References 11. 01. 12. 02. 03. 04. 05. 06. 07. 08. 09. 10. Leksell L, Meyerson BA, Forster DM. Radiosurgical thalamotomy for intractable pain. Confin Neurol 1972; 34:264. Lovo EE, Torres B, Campos F, et al. Stereotactic gamma ray radiosurgery to the centromedian and par­ afascicular complex of the thalamus for trigeminal neur­ algia and other complex pain syndromes. Cureus 2019; 11:e6421. PMID: 31886103; PMCID: PMC6925372. Franzini A, Ninatti G, Rossini Z, et al. Gamma knife central lateral thalamotomy for chronic neuropathic pain: a single-center, retrospective study. Neurosurgery 2023;92:363–9. Epub 2022 Nov 10. PMID: 36637271. Keep MF, DeMare PA, Ashby LS. Gamma knife sur­ gery for refractory postherpetic trigeminal neuralgia: targeting in one session both the retrogasserian trige­ minal nerve and the centromedian nucleus of the thalamus. J Neurosurg 2005;102 Suppl:276–82. PMID: 15662825. Lovo EE, Moreira A, Cruz C, et al. Radiomodulation in mixed, complex cancer pain by triple target irradiation in the brain: a preliminary experience. Cureus 2022;14: e25430. PMID: 35774662; PMCID: PMC9236678. Moreira A, Santos Hern�andez DA, Caceros V, et al. Dual-target radiosurgery for concomitant continuous pain presentation of trigeminal neuralgia: radiomodu­ lation effect and dose. Cureus 2024;16:e51602. PMID: 38313895; PMCID: PMC10836852. Lara-Almunia M, Martinez Moreno NE, Torres Diaz CV, Gutierrez Sarraga J, Martinez Alvarez R. Gamma knife radiosurgery, central lateral thalamotomy, and chronic neuropathic pain: a prospective single-center study with long-term follow-up. World Neurosurg 2025; 194:123445. Epub ahead of print. PMID: 39579928. Urgosik D, Liscak R. Medial Gamma Knife thalamot­ omy for intractable pain. J Neurosurg 2018;129:72–6. PMID: 30544296. Young RF, Vermeulen SS, Grimm P, et al. Gamma Knife thalamotomy for the treatment of persistent pain. Stereotact Funct Neurosurg 1995;64 Suppl 1:172– 81. PMID: 8584825. Middlebrooks EH, Patel V, Popple RA, et al. Connectomic-guided stereotactic radiosurgery thala­ motomy for tremor: a patient-specific approach to enhance outcomes. J Neurosurg 2025;143:53–62. Epub ahead of print. PMID: 39951712. 13. 14. 15. 16. 17. 18. 19. 20. 11 Ganz JC. Radiobiology. Prog Brain Res 2022;268:23– 48. Epub 2021 Dec 14. PMID: 35074083. Yeh C-I, Cheng M-F, Xiao F, et al. Effects of focal radiation on [18 F]-fluoro-D-glucose positron emission tomography in the brains of miniature pigs: prelimin­ ary findings on local metabolism. Neuromodulation 2021;24:863–9. Epub 2020 Apr 8. PMID: 32270579. R�egis J, Bartolomei F, Hayashi M, Chauvel P. Gamma Knife surgery, a neuromodulation therapy in epilepsy surgery!. Acta Neurochir Suppl 2002;84:37–47. PMID: 12379003. Gomes JGR, Gorgulho AA, de Oliveira L�opez A, et al. The role of diffusion tensor imaging tractography for Gamma Knife thalamotomy planning. J Neurosurg 2016;125:129–38. PMID: 27903188. Tsolaki E, Kashanian A, Chiu K, Bari A, Pouratian N. Connectivity-based segmentation of the thalamic motor region for deep brain stimulation in essential tremor: a comparison of deterministic and probabilistic tractog­ raphy. Neuroimage Clin 2024;41:103587. Epub 2024 Feb 27. PMID: 38422832; PMCID: PMC10944185. Del Cid P, Aquino L, Moreira A, et al. Triple-target radiosurgery for intractable cancer pain of mixed ori­ gin: two-centre experience in Central America. Br J Pain 2025;20494637251350331. https://journals.sagepub. com/doi/full/10.1177/20494637251350331. PMCID: PMC12176783 Luo H, Huang Y, Green AL, Aziz TZ, Xiao X, Wang S. Neurophysiological characteristics in the periven­ tricular/periaqueductal gray correlate with pain per­ ception, sensation, and affect in neuropathic pain patients. Neuroimage Clin 2021;32:102876. Du Y, Lin S-D, Wu X-Q, et al. Ventral posteromedial nucleus of the thalamus gates the spread of trigeminal neuropathic pain. J Headache Pain 2024;25:140. PMID: 39192198; PMCID: PMC11348609. Ong WY, Stohler CS, Herr DR. Role of the prefrontal cortex in pain processing. Mol Neurobiol 2019;56: 1137–66. Epub 2018 Jun 6. PMID: 29876878; PMCID: PMC6400876. Weigel R, Krauss JK. Center median-parafascicular complex and pain control. Review from a neurosurgi­ cal perspective. Stereotact Funct Neurosurg 2004;82: 115–26. Epub 2004 Jul 15. PMID: 15305084.
 0
0
Anuncio
Documentos relacionados


Descargar
Anuncio
Añadir este documento a la recogida (s)
Puede agregar este documento a su colección de estudio (s)
Iniciar sesión Disponible sólo para usuarios autorizadosAñadir a este documento guardado
Puede agregar este documento a su lista guardada
Iniciar sesión Disponible sólo para usuarios autorizados