THE JOURNAL OF PROSTHETIC DENTISTRY
GALINDO, SOLTYS, AND GRASER
DENTAL TECHNOLOGY
Kenneth D. Rudd
Long-term reinforced fixed provisional restorations
Daniel Galindo, DDS,a James L. Soltys, DDS,b and Gerald N. Graser, DDS, MSc
University of Rochester Eastman Dental Center, Rochester, N.Y.
Extensive prosthodontic treatment often requires fabrication of long-term provisional restorations.
Numerous materials and techniques have been described for prolonged insertion of interim restorations. This article describes a procedure for fabrication of long-term reinforced heat-processed
provisional restorations based on a diagnostic wax-up. Reinforced heat-processed provisional
restorations reduced flexure, which minimizes progressive loss of cement and diminished the
possibility of recurrent decay. Occlusal stability and vertical dimension were maintained because of
greater wear resistance. Occlusion, tooth contours, and pontic design developed in the provisional
restoration were duplicated in the definitive restoration. The use of a matrix from a diagnostic waxup facilitated fabrication of the prosthesis, and made the procedure less time-consuming and more
predictable. (J Prosthet Dent 1998;79:698-701.)
E
xtensive prosthodontic treatment often requires
fabrication of long-term provisional restorations. Fixed
provisional restorations are also indicated for partially
edentulous patients undergoing implant therapy when
teeth adjacent to the edentulous area are restored with
complete crowns. In these cases, fixed provisional restorations prevent loading of submerged implants or tissue grafts during the healing phase, which is likely to
occur with transitional removable partial dentures.
Provisional restorations are indicated to protect the
dental pulp, protect periodontal tissues, prevent tooth
movement, aid in positional stability, and allow proper
mastication and esthetics.1,2 In many instances, provisional restorations are also helpful as a guide for construction of the final restoration. Esthetics and appearance are evaluated by dentist and patient during this
phase.3
Autopolymerizing acrylic resin is usually the biomaterial in provisional restorations. However, when longterm provisional fixed restorations replace several teeth,
the strength and stability of the prosthesis is critical.
Heat-processed acrylic resin has greater strength, wear
resistance, color stability, and resistance to fracture than
autopolymerizing resins.4 However, in long-span edentulous situations, fractures may still occur.
Provisional restorations may be reinforced with various materials to avoid fracture. Tylman5 described fabrication of acrylic fixed partial dentures (FPDs) supported by an internal metal framework with ferrule-type
retainers cast in hard gold alloy. Youdelis and Faucher6
reported a technique that used stainless steel wire to reinforce autopolymerizing acrylic resin provisional restorations. Binkley and Irvin7 described heat-processed
a
Resident, Department of Prosthodontics.
Clinical Assistant Professor, Department of Prosthodontics.
c
Professor and Postgraduate Program Director, Department of Prosthodontics.
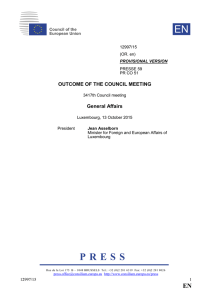
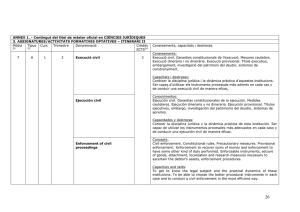
Fig. 1. Pretreatment of patient. Bone augmentation has been
performed in maxillary left quadrant before implant placement. Healing is progressing.
provisional restorations reinforced with a 16- or 18gauge cast metal framework. Hazelton and Brudvik8
suggested reinforcement of autopolymerized provisional
restorations with stainless steel orthodontic band material.
This article describes a procedure for fabricating reinforced, heat-processed, acrylic resin provisional restorations based on a diagnostic wax-up. A base metal framework with complete copings was waxed on a stone cast
of the actual tooth preparations. The framework was then
opaqued and incorporated in the final wax-up. The waxup was fabricated by using a silicone matrix of a diagnostic wax-up or cast and injected base plate wax. After
the occlusion and contours were established, the structure was processed.
PROCEDURE
b
698
THE JOURNAL OF PROSTHETIC DENTISTRY
1. Formulate a diagnostic wax-up on casts mounted
with a semiadjustable articulator. Establish tooth
VOLUME 79 NUMBER 6
GALINDO, SOLTYS, AND GRASER
THE JOURNAL OF PROSTHETIC DENTISTRY
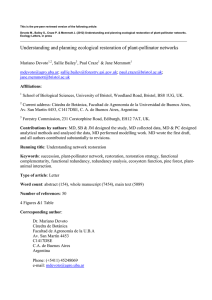
Fig. 2. Diagnostic wax-up. Patient will receive three-unit implant-supported FPD in maxillary left quadrant.
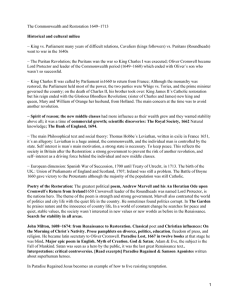
Fig. 4. Wax copings and pattern made with 10-gauge sprue
wax. Large beads were glued to waxed framework.
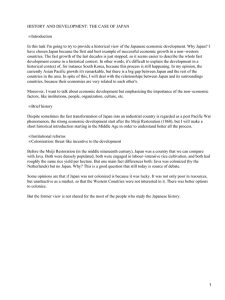
Fig. 3. Wax copings end 2 mm coronal to finish line because
margin will be covered entirely with acrylic resin in case modifications of preparation are needed.
Fig. 5. Cast metal framework was opaqued with liquid opaquer.
contour and occlusion according to clinical situations (Figs. 1 and 2).
2. Make a full arch impression of the prepared teeth
with reversible or irreversible hydrocolloid. Record
a face-bow transfer and centric relation. Select the
appropriate shade and cast the impression using type
IV dental stone.
3. Make two matrices of the waxed teeth with use of
laboratory putty (Sil-Tech, Williams Ivoclar North
America, Inc., Amherst, N.Y.), and include adjacent
teeth to index the matrix. The first matrix is sectioned and is used to evaluate space available for
acrylic resin around the framework. On the second
matrix, make 2 mm wide access holes with a round
bur preserving the occlusal anatomy.
4. Apply die spacer (Zahn Die Spacer, Zahn Dental
Company Inc., Port Washington, N.Y.) over the
abutments of the working cast, 2 mm coronal to
the finish line.
5. Wax copings over abutments and connect them with
JUNE 1998
10-gauge sprue wax (Kerr Manufacturing Co.,
Emeryville, Calif.). Extension of copings is 2 mm
coronal to finish line because the margin will be
covered entirely with acrylic resin in case modifications of the preparation are needed (Fig. 3). Check
space for acrylic resin around the waxed framework
with the first matrix and adjust.
6. Add Rêten large beads (Lang Dental Manufacturing
Co., Chicago, Ill.) to the waxed framework (Fig. 4).
7. Cast the framework using a base metal alloy and
seat the casting.
8. Apply Biolon liquid opaquer (Dentsply Trubyte,
York, Pa.) to the framework (Fig. 5).
9. Place the second matrix over the cast and seal the
edges of the matrix with utility wax strips (Hygienic
Corporation, Akron, Ohio) (Fig. 6).
10. Heat baseplate wax (Neo Wax, Dentsply Trubyte,
York, Pa.) until it melts and inject wax through the
holes of the matrix with the use of a glass eye dropper previously warmed. Wax flows until the available space is full. Allow wax to cool for 5 to 10
minutes.
699
THE JOURNAL OF PROSTHETIC DENTISTRY
GALINDO, SOLTYS, AND GRASER
Fig. 6. Second matrix was placed on working cast with metal
framework and edges sealed with utility wax.
Fig. 8. Final restoration after processing, finishing, and polishing.
Fig. 7. Wax was injected through holes with glass eye dropper. Wax was directed through remaining holes indicating that
space is now full. After wax has hardened, remove matrix and
check completeness of wax-up, tooth contours, and occlusion.
Fig. 9. Restoration cemented with temporary luting cement
(mirror image).
11. Remove matrix and check for completeness of the
wax-up and occlusion. Make adjustments in contours and occlusion (Fig. 7). Size of embrasure
spaces was predicted with the initial diagnostic waxup.
12. Invest wax-up on the cast in a denture flask.
13. Boil out the wax and secure position of framework
on the cast. Pack dentin colored acrylic resin (Biolon,
Dentsply Trubyte) covering framework. Close the
flasks and trial pack.
14. Open flasks, remove excess, and cut back dentincolored resin in incisal and cervical aspects. Place
incisal and cervical colored resin. Staining can be
added at this stage using the Kayon synthetic resins
denture stain kit (Kay See Dental Manufacturing
Co., Kansas City, Mo.). Close the flasks and heat
process.
15. Finish and polish provisional restoration (Fig. 8).
700
16. Seat the restorations intraorally. If necessary, reline
margins with autopolymerizing resin; allow to cure,
then refine margins and repolish restorations.
17. Cement provisional restoration with an interim luting agent (Fig. 9).
DISCUSSION
Heat-processed provisional restorations with metal
reinforcement based on a diagnostic wax-up as a guide
offered several advantages compared with other techniques, including predictable contours, stable occlusion,
esthetics, patient acceptance, strength, and durability.
The patient can perform oral hygiene procedures easier
because embrasure spaces may be wider without compromising strength. If teeth are contoured appropriately,
periodontal tissues are healthier.
The framework design included copings adapted over
the prepared abutments, which reduced flexure of the
provisional restorations. This increased retention of the
restoration, minimized flexure, progressive loss of cement, and diminished the possibility of recurrent deVOLUME 79 NUMBER 6
GALINDO, SOLTYS, AND GRASER
THE JOURNAL OF PROSTHETIC DENTISTRY
cay.5 The marginal area was relined with a minimal
amount of autopolymerizing resin that reduced the possibility of thermal damage to the dental pulp.9
Occlusal stability and vertical dimension were maintained because of greater wear resistance. The occlusion
developed in the provisional restoration was duplicated
in the definitive restoration, and tooth contours and
pontic design can also be monitored. After the patient
and dentist were satisfied, the definitive restoration resembled the provisional prosthesis.
In this procedure, the first silicone matrix was used to
evaluate available space for acrylic resin. The use of incisal, dentin body, and cervical acrylic resin enhanced
the patient’s acceptance of esthetics in the restoration.
The final wax-up for the provisional restoration was completed with use of the second silicone matrix. This saved
time during fabrication of the restoration and allowed
duplication of the contours and occlusion programmed
in the diagnostic wax-up.10
SUMMARY
This article described a procedure for the fabrication
of reinforced heat-processed fixed provisional restorations with use of a diagnostic wax-up. The increase in
rigidity provided by the metal framework incorporated
in the restoration addressed the problem of fracture. The
incidence of fractures have increased when provisional
FPDs were worn for prolonged periods and/or in longspan edentulous areas. The reduction of flexure in this
provisional prosthesis prevented loss of retention and
possible recurrent decay. The use of a previous diagnostic wax-up reduced laboratory time and ensured the success of the definitive restoration.
Adequate embrasure spaces and tooth contour also
developed in the initial wax-up were accurately duplicated in the provisional restoration, leading to healthy
periodontal tissue. Enough space was provided for the
bulk of acrylic resin with the use of a silicone matrix
indexed on adjacent teeth. This facilitated development
of esthetics that was used as a guide for fabrication of
the definitive restoration.
REFERENCES
1. Dykema RW, Goodacre CJ, Phillips RW. Johnston’s modern practice in fixed
prosthodontics. 4th ed. St Louis: WB Saunders; 1986. p. 77-90.
2. Amsterdam M, Fox L. Provisional splinting—principles and technics. Dent
Clin North Am 1959;1:73-9.
3. Rieder CE. The use of provisional restorations to develop and achieve esthetic expectations. Int J Periodont Rest Dent 1989;9:123-39.
4. Anusavice KJ. Phillips’ science of dental materials. 10th ed. Philadelphia:
WB Saunders; 1996. p. 237-71.
5. Tylman SD. Theory and practice of crown and bridge prosthodontics. 5th
ed. St Louis: CV Mosby; 1965. p. 1197-217.
6. Youdelis RA, Faucher R. Provisional restorations: an integrated approach to
periodontics and restorative dentistry. Dent Clin North Am 1980;24:285303.
7. Binkley CJ, Irvin PT. Reinforced heat-processed acrylic resin provisional restorations. J Prosthet Dent 1987;57:689-93.
8. Hazelton LR, Brudvik JS. A new procedure to reinforce fixed provisional
restorations. J Prosthet Dent 1995;74:110-3.
9. Tjan AH, Grant BE, Godfrey MF. Temperature rise in the pulp chamber
during fabrication of provisional crown. J Prosthet Dent 1989;62:622-6.
10. Morgan DW, Comella MC, Staffanou RS. A diagnostic wax-up technique. J
Prosthet Dent 1975;33:169-77.
Reprint requests to:
DR. DANIEL GALINDO
DEPARTMENT OF PROSTHODONTICS
UNIVERSITY OF ROCHESTER
EASTMAN DENTAL CENTER
625 ELMWOOD AVE.
ROCHESTER, NY 14620
Copyright © 1998 by The Editorial Council of The Journal of Prosthetic Dentistry.
0022-3913/98/$5.00 + 0. 10/1/89605
New product news
The January and July issues of the Journal carry information regarding new products of interest to prosthodontists. Product information should be sent 1 month prior to ad closing date to:
Dr. Glen P. McGivney, Editor, SUNY at Buffalo, School of Dental Medicine, 345 Squire Hall,
Buffalo, NY 14214. Product information may be accepted in whole or in part at the discretion of
the Editor and is subject to editing. A black-and-white glossy photo may be submitted to accompany product information.
Information and products reported are based on information provided by the manufacturer.
No endorsement is intended or implied by the Editorial Council of The Journal of Prosthetic
Dentistry, the editor, or the publisher.
JUNE 1998
701
 0
0