I
TORSTEN DECKERT
Physicochemically, NPH and lente insulins differ in size of crystals, content of protamine and zinc, and
often in species composition, since lente always contains beef insulin. The duration of the hypoglycemic
effect of lente insulin seems to be longer than 24 h, whereas that of NPH insulin does not exceed 24 h
when given in amounts of 0.2-0.3 U/kg body wt. Moreover, NPH and lente insulins differ in their
ability to form stable mixtures with neutral insulin solutions, since only NPH insulin can be mixed with
regular insulin without changing the specific course of effect of regular insulin. Highly purified porcine
NPH and the lente-like porcine insulin preparation, Monotard, do not seem to differ regarding side
effects (lipoatrophy, immunogenicity). However, highly purified lente insulin (containing beef insulin)
seems to be more immunogenic than highly purified porcine NPH insulin, DIABETES CARE 3- 623-626,
SEPTEMBER-OCTOBER 1980.
T
he most widely used intermediate-acting insulin
preparations are NPH and lente insulins. It is
often asked whether there is any difference between them in their course of action, reproducibility of resorption, mixability with regular insulin, and side effects, particularly immunogenicity. To answer these questions, the known characteristics of these two insulin preparations are briefly reviewed.
HISTORICAL BACKGROUND
NPH (neutral protamine Hagedom) insulin is a further development of Hagedorn's protamine insulin1 made by
Krayenbiihl and Rosenberg at Nordisk Insulinlaboratorium,
Denmark, in 1946.2 They found that insulin and protamine
brought together in isophane proportions (the condition in
which neither insulin nor protamine is found in excess) at
neutral pH, in the presence of small amounts of zinc and
phenol and/or cresol, will precipitate in oblong tetragonal
crystals without leaving any regular insulin in the supernatant.
Lente insulin (zinc insulin preparation) was invented by
Hallas-Mtfller et al. in 1952 at the Novo company, also in
Denmark.3 The prolongation of effect is based on the fact
that the solubility of insulin at neutral pH in acetate buffer
can be reduced by a surplus of zinc. Furthermore, it can be
modified by the physical state of zinc insulin and by proper
usage of the solubility characteristics of beef insulin.
PHYSICOCHEMICAL CHARACTERISTICS
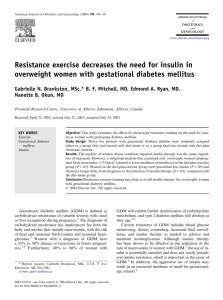
NPH insulin preparations are suspensions of small insulin
protamine crystals of the same size (Figure 1). The volume of
the crystals may vary between 1 and 20 fim3. The crystals are
suspended in a phosphate buffer at neutral pH. The lente insulin preparations are suspensions of about 70% large rhombohedral beef zinc insulin crystals (ultralente) and 30%
amorphous porcine zinc insulin particles (semilente). The
volume of the ultralente crystals is about 200- 1000 fxm3.
The mixture is suspended in acetate buffer at neutral pH
containing a surplus of zinc.
Bottles containing NPH as lente insulin have to be inverted several times before the preparation is drawn up into
the syringes before injection. However, because the zinc insulin crystals are larger and heavier than the NPH crystals,
lente insulin will sedimentate faster than NPH insulin after
shaking the suspension, which might have some practical
importance. The content of protamine and zinc in NPH and
lente insulins is given in Table 1.
Besides these major differences, the chemical differences
depend on the species and the purity of the insulin used. The
insulin used in manufacturing NPH insulin is beef or pork
insulin or a mixture of both. Lente insulin is always a mixture of beef and pork insulin, since the ultralente part of
lente insulin is made from beef insulin and the semilente part
of lente insulin is made from porcine insulin. Porcine lentelike insulin is available as Monotard insulin (Novo, Copen-
DIABETES CARE, VOL. 3 NO. 5, SEPTEMBER-OCTOBER 1980
623
Downloaded from http://diabetesjournals.org/care/article-pdf/3/5/623/464446/3-5-623.pdf by guest on 12 December 2024
ntermediate-acting Insulin Preparations:
NPH and Lente
INTERMEDIATE-ACTING INSULIN: NPH AND LENTE/TORSTEN DECKERT
(a)
Downloaded from http://diabetesjournals.org/care/article-pdf/3/5/623/464446/3-5-623.pdf by guest on 12 December 2024
(b)
FIG. I. Photomicrograph of (a) NPH suspension and (b) lente insulin suspension at room temperature. 1.0 cm =20
hagen, Denmark). The species specificity seems to play a role
in the immunogenicity of insulin, since insulin preparations
containing beef insulin have been shown to induce insulin
antibodies more easily than insulin preparations containing
only porcine insulin.11
The purity of the insulin component varies over a wide
range. During the last years there has been a development
toward insulin preparations of higher purity, since it has
been shown that several side effects (for example, lipoatrophy, insulin resistance, insulin allergy, and the development of several humoral antibodies) depend largely on the
purity of the insulin preparation.4*5 The purity of NPH as
624
/u,m.
well as lente insulin preparations is expressed in suffix as single peak, single component, monocomponent (MC), or rare
immunogenic (RI). Single peak means that insulin has been
isolated by gel filtration, which separates molecules according to their size (i.e., insulin, arginine insulin, desamidoinsulin, ethylester insulin, and small amounts of other polypeptides). Single component, monocomponent, and rare
immunogenum (RI) means that insulin has been further
purified by chromatography, which also separates molecules
of the same molecular size and therefore contains less impurities. As well, NPH made from porcine insulin as lente insulin of highly purified quality is available. However, for docu-
DIABETES CARE, VOL. 3 NO. 5, SEPTEMBER-OCTOBER 1980
INTERMEDIATE-ACTING INSULIN: NPH AND LENTE/TORSTEN DECKERT
TABLE 1
Content of protamine and zinc in NPH and lente insulins
NPH
Lente
Physical state
pH
Zn (mg/100 U)
Protamine
(mg/100 U)
Crystalline
70% crystalline
30% amorphous
7.3
7.3
0.02
0.20
0.3-0.4
0
ABSORPTION FROM SUBCUTANEOUS TISSUE
COURSE OF ACTION
The time curve of the blood glucose lowering action of NPH
and lente insulins (as given by Nordisk Insulinlaboratorium
and the Novo Company in 1978) is shown in Table 3. However, randomized crossover experiments against placebo in
fasting diabetic subjects have only been done by K^lendorf et
al. with NPH insulin.6 They found that the starting action
began 120 min after the injection, and that the maximal action occurred 5.5 h after the injection, 30 min after the
maximal plasma insulin concentration had been reached.
From Rasmussen et al.'s experiments in nonfasting diabetic
subjects, it seems that the maximal effect after lente was first
achieved after 10 h. 9
The porcine lente-like preparation Monotard appears to
have a shorter effect than lente insulin. Our crossover experiments on maturity-onset diabetic subjects using highly
purified porcine NPH insulin and the highly purified porcine
lente-like preparation Monotard did not indicate differences
in the blood glucose lowering effects between these two preparations (Figure 2). Reproducibility of the blood glucose
lowering effect of NPH insulin in maturity-onset diabetes
was shown to be excellent.6
It can be concluded from resorption studies, studies of
plasma insulin concentration after subcutaneous injection,
and studies of the blood glucose lowering effects of NPH and
lente that lente has a more protracted action than NPH insulin.
bsorption studies with NPH and lente insulins have
been done either by following the disappearance
of radioactivity from subcutaneous tissue after
the injection of labeled NPH or lente insulin or
by following the plasma insulin concentration after subcutaneous injection of these preparations in patients with only
minor or no endogenous insulin secretion. However, the
same techniques have not been used and the results therefore
are not strictly comparable.
The most extensive studies with radioactive-labeled NPH
insulin have been done by Ktflendorf et al.6 and with labeled
lente insulin by Binder et al.7'8 The differences between
NPH and lente insulin, according to their results, are shown
in Table 2. Twenty-four hours after injection in the femoral
region, remarkably more radioactivity is found at the injection site after lente insulin compared with NPH insulin.
The disappearance of radioactivity at the injection site
after NPH insulin followed first-order kinetics,6 whereas
lente was absorbed in a biphasic curve,7 probably because
lente insulin is a mixture of amorphous and crystalline zinc
insulin.
The reproducibility of day-to-day absorption in the same
patient, measured as the variation coefficient of the time MIXABILITY
until 40-50% of the maximal radioactivity disappeared, was
26% for NPH insulin6 and about 35% for lente insulin.7 Regular insulin can be mixed with NPH or lente insulin in
Thus, the reproducibility of the resorption of both insulin the same syringe in every ratio. However, the course of effect
will change with lente/regular mixtures depending on the
TABLE 2
TABLE 3
Time curve of action of NPH and lente insulins
Differences in absorption between NPH and lente insulins
Percent of injected insulin at injection site after:
NPH
Lente
10 h
24 h
36 h
40
70
10
40
0
25
Data from K0lendorf et al.6 and Binder.7
Course of effect (h)
NPH
Lente
Onset
Maximum
End
1*4
2Vi
4-12
24
24 Vi
Data from Nordisk Insulinlaboratorium and Novo Company, 1978.
DIABETES CARE, VOL. 3 NO. 5, SEPTEMBER-OCTOBER 1980
625
Downloaded from http://diabetesjournals.org/care/article-pdf/3/5/623/464446/3-5-623.pdf by guest on 12 December 2024
menting purity, techniques such as gel filtration and
chromatography are insufficient. The purity of insulin should
be further specified by radioimmunologic determination of
the relevant contaminants [i.e., a-components, proinsulin,
glucagon-like materials, pancreatic polypeptide (PP), vasoactive intestinal peptide (VIP), somatostatin] by well-documented techniques. Also, the purity of protamine, zinc, and
other additives should be stated. Otherwise, the purity of
NPH and lente insulins cannot be compared.
preparations seems to be in the same range. It must, however, be mentioned that the experiments with lente insulin
were\done with non-highly purified insulins.
After subcutaneous injection of NPH insulin in reasonable
doses, plasma insulin concentration increases significantly
after 2 h and is maximal after 5 h. 6 After lente insulin in
comparable amounts, the time for significant initial increments to occur is not known. The maximal plasma insulin
concentration seems to be reached 7 h after the injection of
lente insulin.9 Twenty-four hours after the injection of NPH
insulin, the plasma insulin concentration is not higher than
before the injection. Twenty-four hours after lente insulin,
plasma insulin still seems to be elevated.10
INTERMEDIATE-ACTING INSULIN: NPH AND LENTE/TORSTEN DECKERT
per cent of initial
blood glucose (m* SEM )
x NPH (Retard R I ® )
o Lente like (Monotard®)
100-
n= 12
8060-
^N-f+Hnu-——-—Hi
40T injection
13
15
17
19
21
TIME
ratio between lente and regular insulin in the syringe,10 presumably because the surplus of zinc in the supernatant of
lente insulin will react with regular insulin and change it to a
semilente-like preparation. This is not the case when mixing
regular insulin with NPH. Stable mixtures of regular and intermediate-acting insulin can only be prepared with NPH insulin.6
IMMUNOGENICITY
T
he immunogenicity of NPH and lente insulin depends largely on the purity and species of the insulin used. Preparations containing beef insulin are
more immunogenic than insulin preparations
made of porcine insulin of comparable purity.11 However, by
using lente insulin of monocomponent purity (lente prepared
from highly purified beef and highly purified porcine insulin), formation of antibodies can be avoided in some instances,4 but not to the same extent as with highly purified
porcine insulin.11 Highly purified porcine NPH insulin Leo
Retard RI (Nordisk) and the highly purified porcine lentelike insulin preparation Monotard (Novo) are of very low
immunogenicity. Antibody formation against proinsulin,12
glucagon, VIP, PP, and probably somatostatin can be
avoided.13 Antibodies against protamine have not been described, but in a few patients with insulin allergy, positive
cutaneous reactions were seen against highly purified insulin
as well as protamine.14 It is not known whether the insulin
preparation plays a role in the development of late diabetic
complications; probably this cannot be substantiated.
From Steno Memorial Hospital, DK-2820, Gentofte, Copenhagen, Denmark.
REFERENCES
1
Hagedorn, H. C , Jensen, B. N., Krarup, N. B., and Wodstrup, I.: Protamine insulinate. JAMA 106: 177-80, 1936.
626
2
Krayenbiihl, C., and Rosenberg, T.: Crystalline protamine insulin. Rep. Steno Hosp. (Kbh.) 1: 60-73, 1946.
3
Hallas-Mtfller, K., Jersild, M., Petersen, K., and Schlichtkrull,
J.: Zinc insulin preparations for single daily injection. JAMA 150:
1667-71, 1952.
4
Schlichtkrull, J., Pingel, M., Heding, L. G., Brange, J., and
J^rgensen, K. H.: Insulin preparations with prolonged effect. In Insulin II. Hasselblatt, A., and Bruchhausen, F. v., Eds. Berlin,
Springer-Verlag, 1975, pp. 729-77.
5
Deckert, T., Andersen, O. O., and Poulsen, J. E.: The clinical
significance of highly purified pig-insulin preparations. Diabetologia
10: 703-08, 1974.
6
K«ilendorf, K., Aaby, P., Westergaard, S., and Deckert, T.:
Resorption, effect and side effects of highly purified porcine NPHinsulin preparations (Leo®). Eur. J. Pharmacol. In press.
7
Binder, Chr.: Absorption of Injected Insulin. Copenhagen,
Munksgaard, 1969.
8
Faber, O. K., Lauritzen, T., Binder, Chr., Mouridsen, H. T.,
and V^lund, Aa.: Comparison of absorption and clinical effects of
Insulin Monotard® and Insulin Novo Lente®. Ugeskr. Laeg. 137:
2510-14, 1975.
9
Rasmussen, S. M., Heding, L. G., Parbst, E., and V«ilund,
Aa.: Serum IRI in insulin-treated diabetics during a 24/hour period.
Diabetologia JJ: 151-58, 1975.
10
Schlichtkrull, J.: The absorption of insulin. Acta Paediatr.
Scand. [Suppl.] 270: 97-102, 1977.
11
Chance, R. E., Root, M. A., and Galloway, J. A.: The immunogenicity of insulin preparations. Acta Endocrinol. (Kbh.)
Suppl. 205: 185-99, 1976.
12
Falling, I., Jerwell, J., Aagenaes, 0., and Aarseth, S.: Antibodies to insulin and proinsulin, metabolic control, and insulin
dose, in diabetics changing to highly purified insulins. Diabetologia
12: 390, 1976.
13
Bloom, S. R., West, A. M., Polak, J. M., Barnes, A. J., and
Adrian, T. E.: Hormonal Contaminants of Insulin from Gut Hormones. Bloom, S. R., Ed. Edinburgh, Churchill Livingstone, 1978,
pp. 318-22.
14
Rosenthal, A.: Genetic control of insulin antibody formation.
Juvenile Diabetes Foundation International Workshop on Insulin.
New York, 1978.
DIABETES CARE, VOL. 3 NO. 5, SEPTEMBER-OCTOBER 1980
Downloaded from http://diabetesjournals.org/care/article-pdf/3/5/623/464446/3-5-623.pdf by guest on 12 December 2024
20-
FIG. 2. Blood glucose lowering effect in percent
of initial capillary blood glucose (initial = mean
of blood glucose at 0700, 0800, and 0900 h)
after highly purified porcine N P H insulin (Retard RI) and the highly purified porcine Ientelike preparation (Monotard) given subcutaneous^ (at the arrow) in the femoral region.
Randomized crossover experiment.
 0
0