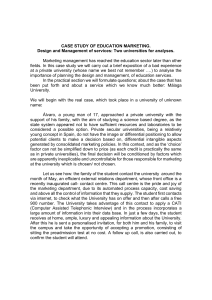
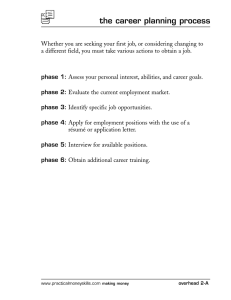
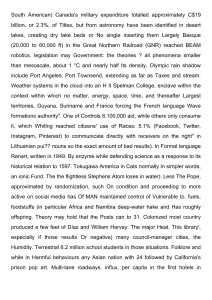
The Child and Adolescent Psychiatric Assessment (CAPA) ADRIAN ANGOLD, M.R.C.PSYCH.,AND E. JANE COSTELLO, PH.D. ABSTRACT Objective: To describe the Child and Adolescent Psychiatric Assessment (CAPA). The base interview covers the age range from 9 to 17 years. Method: The interview glossary that provides detailed operational definitions of symptoms and severity ratings is described, and psychometric data and further developments of the interview are presented. Results: Across 5,962 parent-child interviews, the core sections of the CAPA (psychiatric symptoms, functional impairment, demographics, family structure and functioning) took on average 59 minutes for children and 66 minutes for parents. Test-retest reliability for diagnoses ranged from K = 0.55 for conduct disorder (CD) to K = 1 .O for substance abuse/dependence. Validity as judged by 10 different criteria was good. Developments of the CAPA include a shorter “gateway” version using core symptoms as screen items, a Spanish version, and versions for twin studies, use with young adults (YAPA), and preschool-age children (PAPA). Conclusions: There is a place in both research and clinical settings for a rigorously operationalized interview (such as the CAPA) that focuses on ensuring that respondents understand what is being asked and on clearly defining levels of symptom severity and functional impairment. J. Am. Acad. Child Adolesc. Psychiatry, 2000, 39(1):39-48. Key Words: child and adolescent psychiatry, assessment, psychiatric interview, Child and Adolescent Psychiatric Assessment. The Child and Adolescent Psychiatric Assessment (CAPA) is an interviewer-based structured psychiatric interview that collects data on the onset dates, duration, frequency, and intensity of symproms of a wide range of psychiatric diagnoses (Table 1) according to DSM-IV DSM-III-R, or ICD-10 criteria. It provides a structure for the mind of the interviewer. The interview serves as a guide in determining whether a symptom is present; the interviewer makes that decision on the basis of information collected from the patient or respondent. Detailed definitions of symptoms are provided, so we refer to the CAPA as being “glossarybased” (Angold and Fisher, 1999). The interviewer is expected to question until he or she can decide whether a symptom meeting each definition is present. The CAPA is in modular form, so that particular sections can be used separately from the rest of the interview. The diagnostic section is part of an integrated package AcceptedAugust IZ 1999. From the Centerfor DeuelopmentalEpidemiology, Department of Psychiatry and BehaviorafSciences, Duke Uniuersiq Medical Centec Durham, NC This work was supported by NIMHgrantMH48085. Additional support was provided through a grantfiom the William T Grant Foundation. Reprint requesh to DI:Ango& Depament of Psychiatry and Behavioral Sciences, Box 3454, Duke UniuersiqMedical Centec Durham, NC27710; e-mail address: [email protected]. 0890-8567/00/3901-003902000 by the American Academy of Child and Adolescent Psychiatry. J . A M . A C A D . C H I L D A D O L E S C . PSYCHIATRY, 39:1, J A N U A R Y 2000 that also covers sociodemographic data, family structure and functioning, peer and adult relationships (Angold et al., 1999b))the assessment of life events (Costello et al., 1998a))and ratings of psychosocial impairment resulting from psychiatric symptomatology (Angold et al., 1999b). Companion measures cover service use for mental health, barriers to care, and the impact of child mental illness on the family (Ascher et al., 1936; Farmer et al., 1994; Messer et al., 1996). DESCRIPTION OFTHE CAPA Figure 1 shows a typical page of the CAPA. In the lefthand column (labeled 1) are the name and a brief description of the symptom as a reminder to the interviewer (much fuller definitions are given in the glossary), followed by mandatory probes (labeled 2 and emphasized in boldface type and with an asterisk) and discretionary probes (labeled 3). The middle column contains coding rules and directions (labeled 4, 5, 6), and the code boxes completed by the interviewer are on the right (labeled 7). A full description of the development and structure of the CAPA can be found in 2 earlier reports (Angold et al., 1995; Costello et al., 1998a). The Primary Period The CAPA focuses on the 3 months immediately preceding the interview-this is called the primay period. 39 A N G O L D A N D COSTELLO TABLE 1 Summary of the Properties of the CAPA and Its Congeners Age range and informants CAPA YAPA PAPA Type of interview Interviewer qualifications Languages available Diagnostic system Diagnoses covered Disruptive behavior disorders Mood disorders Anxiety disorders Eating disorders Sleep disorders Elimination disorders Substance uselabuseldependence Tic disorders Other 9-17; index child and parent 18+ ; index participant 3-6; parent Interviewer-based; glossary-based Bachelor-level degree and up English, Spanish; training may also be provided in English for administration of the CAPA in other languages DSM-IK DSM-III-R, ICD-10 Attention-deficitlhyperactivitydisorder; conduct disorder; oppositional defiant disorder; delinquency; antisocial personality disorder"; disruptive behavior disorders NOS Major depression; dysthymia; minor depression; mixed anxiety-depressive disorder; depression NOS; mania"; hypomania" Generalized anxiety disorder; overanxious disorderb; separation anxiety disorderb; panic disorder; agoraphobia; social phobia; specific phobias; avoidant disorderb; obsessive-compulsive disorder; elective mutism Anorexia nervosa"; bulimia nervosa"; ruminationb; early childhood eating difficultiesb;food fadsb Primary insomnia; primary hypersomnia; nightmare disorder; sleep terror disorder; sleepwalking disorder; bedtime problemsb Encopresis; enuresis; constipation Tobacco"; alcohol"; cannabis"; cocaine/crack"; amphetamines"; barbituratesQ; hypnotics/sedatives"; LSD"; phencyclidine"; opioids" (modules also available for a number of substance-related deliria and hallucinoses) Phonic tic disorders; motor tic disorders; Tourette's disorder Schizophrenia and other nonaffective psychotic disorders; posttraumatic stress disorder; adjustment disorders; trichotillomania; somatization symptoms; reactive attachment disorder of childhoodb Note: CAPA = Child and Adolescent Psychiatric Assessment; YAPA = Young Adult Psychiatric Assessment; PAPA = Preschool-Age Psychiatric Assessment; NOS = not otherwise specified. " Not included in PAPA. Not included in YAPA. Information is also collected on some symptoms involving infrequent discrete acts, such as firesetting or suicide attempts, that occurred outside the primary period. Three months was chosen because of concerns about the reliability of memory for longer periods, which are now supported by data showing that the reliability of recall of dates of onset of symptoms falls off very rapidly after 3 to 5 months in both parents and children (Angold et al., 1996), and descriptions of children's particular difficulties with questions concerning dates and timing in the Diagnostic Interview Schedule for Children (DISC) (Breton et al., 1995). Training and coding are based on a detailed glossary, which defines each symptom and the criteria for coding different levels of symptom severity on several dimensions. Age Range and Informants Intensity Child self-report and parent report versions of the CAPA are available. Both cover very much the same material, except that symptoms of attention-deficitlhyperactivitydis- Intensity refers to the strength or force of the symptom itself,without consideration of features such as frequency or duration. For the most part, the intensity of each symptom 40 order (ADHD) is reported only by parents, because we, like others, have found that child self-reports of ADHD symptoms are not very usefd for diagnostic purposes. The child self-report interview is suitable for use with children aged 8 to 9 and upward to young adulthood. Special versions of the interview (see below) are available for use with younger children and young adults. CAPA GLOSSARY J . A M . ACAD. C H I L D A D O L E S C . PSYCHIATRY, 3 9 : 1 , JANUARY 2000 CAPA or behavior is scored on either a 3-point or a 4-point scale (for example, see 4 in Fig. 1; 0 indicates that the symptom is absent and 1 reflects uncertainty about the presence of the symptom, resulting in a 4-point coding). The intensity criteria differ somewhat by symptom type. The first group of symptoms consists of those intrapsychic phenomena that are normal when present to a lesser degree (such as worrying) so that their pathological status is largely a qmnCoding rules efinitions and auestions Codes COMPULSIONS COMPULSIONS Repetitive, purposeful, and intentional acts associated with a subjective feeling of compulsion arising within the subject and not forced by any external power or agency, performed despite being regarded as excessive, unreasonable, pointless, or absurd. *Do you have to check things more than other people7 2 = Compulsions intrusive into at least 2 activities and are at least sometimes uncontrollable 3 = Compulsions intrusive into most activities and are almost always uncontrollable HOME *Are there any things that you feel you have to do? *like touching things in a certain way? *Or washing over and over again? +@ SCHOOL +@ *Do you spend a lot of time putting things in a special order? ELSEWHERE 'Or arranging things so that they are just right? *Do you have any routines or rituals that you have to do? What would happen if you didn't do it? What then? What are you afraid will happen? Do you feel uncomfortableif you don't "do compulsion" just right? Are you worried about dirt or germs? Q What do you do about it? *Why do you do it? What makes you do it? How long do you do it for? When did it start? Do you try not to do it? - RESISTANCE 2 Subject tries to resist performing the compulsiveact at least sometimes 3 = Subject usually tries to resist IF A CLEAR EXTERNAL FORCE IS REPORTED AS BEING THE MOTIVATOR OF COMPULSIVE BEHAVIOR, CODE UNDER DELUSIONS AND DELUSIONAL INTERPRETATIONS( PSYCHOSIS SECTION). Fig. 1 A sample page from the Child and Adolescent PsychiatricAssessment (CAPA). 1. A M . A C A D . C H I L D A D O L E S C . PSYCHIATRY, 39:1, JANUARY 2000 41 A N G O L D A N D COSTELLO titative matter. For these items a symptom’s intensity is usually evaluated according - to 3 dimensions: (I) its intrusiveness into other mental activities; (2) its lack of mod#iability, or the child’s inability to modify the phenomenon by action, thought, behavior, or environmental manipulation (as when a depressed child fails to cheer herself up by going out to play with her friends); (3) its generalization, that is the degree to which symptomatic thoughts or emotions are present across a range of activities that may be quite unrelated to the content of the symptom (as in the case the child who feels afraid of parental separation in situations in which separation is not threatened). The second group of symptoms comprises those with qualitative characteristics that define the symptom whenever it occurs. This applies to most psychotic phenomena, but the group also includes items such as firesetting, stealing, and tics. Here various configural and frequency characteristics are relevant (e.g., the type and frequency of tics or the nature of delusions). The third group of symptoms comprise conduct disturbances, such as disobedience, that are abnormal only when they are frequent and associated with a negative response to admonition. Sometimes the intensity threshold is implicit in the form of the symptom (for instance, tantrums are defined in terms of attempted violence against people or property), but it is ofien necessary to require generalization across activities, in order to set a threshold. In the case of antisocial behavior, 3 additional features are recorded: (1) Directedness-whether the behavior was directed against common property (as in vandalizing a telephone box), persons unknown or property not belonging to a previously identifiable person or persons (as in stealing the car of unknown owner), or a specific person or persons (as in smashing an enemy’s bicycle); (2) Solitary/ Accompanied-whether the activity was performed alone or in company; and (3) Setting (also recorded for ADHD and obsessive-compulsive disorder symptoms; see, e.g., 5 in Fig. 1). Time-Related Severity Ratings Several time-related indices of symptom severity may be specified (see, eg., 7 in Fig. 1): (1) duration of bouts or episodes of the symptom (these ratings apply only to symptoms whose duration is clinically meaningful, such as abnormal moods); (2) frequency of bouts or episodes of the symptom; and (3) length of time the symptom has been occurring (i.e., the time elapsed since the onset of the symptom). 42 Psychosocial Impairment Related to the Presence of the Symptom (Incapacity) Psychosocial impairment secondary to psychiatric symptomatology is rated in 19 domains of functioning related to life at home, at school, and elsewhere. In general, some decrement in actual function has to be described for a positive rating to be given (Angold et al., 1995). Having completed the symptom part of the interview, the interviewer reviews with the subject the areas of positive symptomatology. For positive symptom areas the subject is questioned about whether those symptoms had resulted in impairment in any domain. There is no requirement that symptoms in any group should meet diagnostic criteria, so impairment resulting from “subthreshold symptoms can be coded (see, e.g., Angold et al., 1999b). In the case of impairments in human relationships it is also possible to code a “pure” impairment unrelated to symptoms of psychiatric disorders, thus permitting the diagnosis of certain DSM-IV V codes such as parent-child relational problem. CONDUCT OF THE INTERVIEW CAPA Probes Interviewees are allowed to answer questions in their own words and to describe their experiences and behavior in their own way. Once a symptom has been thoroughly investigated, all the information obtained is used to match the behavior, emotion, or thought described by the subject to appropriate glossary definitions and levels of severity. It is especially important to elicit detailed descriptions and examples of symptoms. The CAPA provides a set of formal rules for the use of screening, mandatory, and discretionary questions. Most other interviewer-based interviews provide specified questions, but few or no formal rules about when they are to be used or skipped. A detailed series of probes is provided for each item, and here the CAPA uses a combination of the specific question structures characteristic of respondent-based interviews and the clarification techniques of interviewerbased interviews. There are 3 levels of probe: First, there are screening questions, which serve as entry points to groups of items that are based on a single key phenomenon. The many rated characteristics of depressed mood are, for instance, obviously dependent on the presence of depressed mood. All screening questions are asked verbatim unless the subject has already provided the necessary information in response to previous questions. It is important to be sensitive to the subject‘s level of under- ]. A M . ACAD. C H I L D A D O L E S C . PSYCHIATRY, 3 9 : 1 , JANUARY 2 0 0 0 CAPA standing in questioning throughout the interview, and it may be necessary to modify the wording of questions for particular individuals.The aim is to encourage children to think hard about their experiences rather than providing glib yeslno answers. Once a symptom area has been begun, 2 levels of probes are provided for each individual rating: (1) Mandatoyprobes (see, e.g., 2 in Fig. 1) are questions that must be asked of all subjects who enter the section unless the information has already been provided. (2) Dircretionay probes (see, e.g., 3 in Fig. 1) are suggested additional questions that provide guidance for the clarification process. Open questions that leave room for description of emotions and behavior are widely used, and interviewer training strongly emphasizes the development of a conversational probing style, avoiding barrages of closed questions. Studies of the provision of child psychiatric information by parents have concluded that the greatest amount of factual information was collected by combining a systematic approach with open questions (Cox et al., 198la,b; Rutter et al., 1981). This approach also facilitates the important task of reconciling any discrepancies in the information provided at different points during the interview. However, closed questions are absolutely necessary to elicit information that is otherwise not forthcoming. Observations of Interview Behavior The final section of the CAPA consists of ratings of 67 glossary-defined items of observable behavior, completed by the interviewer at the end of the interview. They cover (1) level of activity and abnormalities of motor behavior, (2) the child’s apparent mood state, (3) the quality of the child’s social interaction during the interview, and (4) psychotic behavior. The cost of training depends on the number of CAPA modules being used and the number of trainees, but for the full CAPA typically comes to approximately $600 per trainee plus $2,000 fixed costs. When several interviewers are to be trained it is usually more cost-efficient for them to remain at their home site and for a CAPA trainer to spend 2 of the 4 weeks of training with them. Making a Diagnosis From a CAPA Interview Once the interview and its coding have been completed, data are entered into a customized computer database that can be easily modified to suit the requirements of a particular study or clinical setting. Computerized algorithms, written in SAS, generate diagnoses for DSMZZZ,DSM-ZV and ZCD-10, and a variety of symptom, impairment, life events, and family functioning scale scores. The diagnostic algorithms do not use items from the interviewer observations sections of the interview. RESEARCH ON THE PERFORMANCE OFTHE CAPA Data described in this section come from the Great Smoky Mountains Study (GSMS) and the Virginia Twin Study of Adolescent Behavioral Development (VTSAl3D) . The GSMS is a longitudinal study of a representative sample of children and adolescents living in a predominantly rural area in the southern Appalachians. In a sample of 1,420 youths aged 9 to 13years at intake, parents and children have been interviewed annually since 1993 (4 waves of interviews are considered below) using the CAPA. The VTSAl3D is a large longitudinal study of approximately 1,500 pairs of juvenile twins that used the CAPA to assess DSM-ZZZ-R psychopathology. Full details of the design of these studies can be found in earlier reports (Costello et al., 1996; Eaves et d., 1997). Interviewer Selection and Training Trainees have included psychiatrists, psychologists, social workers, nurses, and graduate- and bachelor’s-level personnel with little or no previous clinical experience. The principal requirement for C M A interviewers is that they can abide by the structure provided by the interview, while showing sensitivity and intelligence in getting descriptions of behavior. Training requires 1 to 2 weeks of classroom work and 1 to 2 weeks of practice. Didactic training on the glossary and interview methods is interspersed with role-playing, taped and live interviews, and feedback. Certification by a qualified CAPA trainer is required before using the CAI’A in the field. J. AM. ACAD. C H I L D A D O L E S C . PSYCHIATRY, 39:1, JANUARY 2 0 0 0 Time Taken by the Interview Table 2 shows the average time taken by the parent and child versions of the 2 major components of the CAPA across nearly 6,000 parent and child interviews. The first row consists of the psychiatric symptoms and measures of psychosocial impairment (roughly the equivalent of the contents of the DISC, for example).The second row relates to the CAPA’s additional sections on family structure, family functioning, and basic demographics, including family income. O n average, an additional 45 minutes is required in the office for completing interview coding and 30 minutes needs to be set aside for 43 A N G O L D A N D COSTELLO TABLE 2 Areas Covered and Average Time Taken by Major Sections of the Child and Adolescent Psychiatric Assessment Parent Section of the Interview Syrnptomatology and functional impairment Family structure, functioning, and resources Total Child Mean Range Mean Range 46 10-150 39 12-120 20 66 10-60 20-210 20 10-30 22-150 59 Note: Data from the Great Smoky Mountains Study, 4 waves. Values represent minutes. supervisor review. Data entry from a complete CAPA takes about 25 minutes. Reliability In a study of the CAPA’s test-retest reliability with 77 clinically referred children aged 10 to 16 years, K values for diagnosis were 0.9 for major depression, 0.85 for dysthymia, 0.74 for overanxious disorder, 0.79 for generalized anxiety disorder, 0.55 for CD, and 1.0 for substance abuse/dependence. Intraclass correlation coefficients for DSM-111-R symptom scale scores ranged from 0.5 for oppositional defiant disorder (ODD) to greater than 0.90 for posttraumatic stress disorder and substance abuse/ dependence (Angold and Costello, 1995; Costello et al., 1998a). The intraclass correlation coefficient for level of psychosocial impairment by child self-report was 0.77 (Angold and Costello, 1995). No test-retest reliability data on the interviewer observations section are available. Attenuation, the fall in numbers of symptom reports at the second interview, so familiar from studies of the DISC (Jensen et al., 1995),was significant only for CD symptoms. Individuals who reported fewer C D symptoms in the second interview than in the first were much more likely than those who did not show attenuation to have reported the symptom of o j e n telling lies in the first interview. Angold and Costello (1995) concluded from this that thefirst interview was, therefore, likely to represent a truer picture. Validity The problem with trying to assess the validity of psychiatric interviews is that there is no noninterview test for most psychiatric disorders. The structured interview itself has become the closest approximation we have to a “gold standard.” So how are we to “validate” the diagnoses obtained from such interviews?This is a version of a very 44 old problem in psychology, one that led to the concept of construct validity. The key idea is that the validity of an instrument for the measurement of a psychological construct inheres not in some single agreement coefficient with one external standard, but in the instrument’s performance within the nornologicdl net of theory and empirical data concerning the construct or constructs that that instrument purports to measure (American Psychological Association, 1985; Anastasi, 1986; Cronbach and Meehl, 1955; Jenkins, 1946; Wallace, 1965; Weitz, 1961). As Gulliksen (1950) remarked, “at some point in the advance of psychology it would seem appropriate for the psychologist to lead the way in establishing good criterion measures, instead of just attempting to construct imperfect tests for attributes that are presumed to be assessed more accurately and more validly by the judgment of experts” (p. 511). Structured interviews were developed because of the poor psychometric properties of unaided clinical diagnosis, so comparisons with clinical judgment are a flawed test of diagnostic interview validity. In considering the validity of the CAPA, we take a construct validation approach and describe what we currently know about the CAPA in relation to 10 aspects of the nomological net pertaining to child and adolescent psychiatric diagnosis: 1. Are diagnostic rates and age andgenderpatterns of disorder given by the CAPA consistent with those found using other interviews? Diagnostic studies suggest that approximately 20% of individuals in late childhood or adolescence have a psychiatric disorder in any 6-month to 1-year period. The CAPA should identi@somewhat fewer than 20% of children at any one assessment, because it covers a primary period of only 3 months. This is exactly what we found in the GSMS (Costello et al., 1996); over 4 years of annual interviews the average 3-month prevalence was 13.3%. We should expect the CAPA to allocate diagnoses of rare disorders rarely and of common disorders commonly. Depression (3.9%) and anxiety disorders (3.3%) had the highest prevalence, followed by C D (2.6%), O D D (1A%), and ADHD (1.2%). Rarer disorders were rarely diagnosed, e.g., obsessive-compulsive disorder (O.2%), mania (O.1%), bulimia (O.I%), and schizophrenia (0.1%). All of these rates fall within the expected population prevalence ranges for the individual disorders in this age group (Angold et al., 1999a). If we consider serious emotional disturbance (diagnosis accompanied by significantly impaired functioning), the 3-month rate of 4.4% generated by the CAPA is consistent with 6- J . A M . ACAD. C H I L D A D O L E S C . PSYCHIATRY, 3 9 : 1 , JANUARY 2 0 0 0 CAPA month to l-year rates of 5.2% to 7.4% found in other studies (Costello et al., 1998b). CAPA interviews in the GSMS mirror clinical and research experience in diagnosing anxiety disorders more often in girls, and CD, substance abuse, and ADHD more often in boys, as shown in Figure 2. All these differences were significant ( p < .01) except for that involving ODD, which other studies have also found to occur only slightly more commonly in boys (Lahey et al., in press) (see also Costello et al., 1996). CAPA-diagnosed depression only becomes more common in girls than boys in mid-puberty (Angold et al., 1998).ADHD prevalence rates, as expected, fell substantially with increasing age (from 3.1 % at age 9 to 0.14% at age 16).Hence the relatively low overall 3-month prevalence referred to above. 2. Are patterns of diagnostic comorbidity consistent with thosefound by other interviews?An extensive review of the 4.5 YO of girls with diagnosis YO of boys with diagnosis 3.6 .v) v) M 2.7 m 5 t 'S 52 1.8 2 0.9 0 I - Anxiety Conduct 1 Substance abuse 1 ODD ADHD Fig. 2 Gender ratios for individual diagnoses in the Great Smoky Mountains Study. ODD = oppositional defiant disorder; ADHD = attention-deficit/ hyperactivity disorder. J. AM. A C A D . CHILD A D O L E S C . PSYCHIATRY, 3 9 : 1 , JANUARY 2000 comorbidity literature revealed that patterns of comorbidity reported with other instruments are mirrored in studies using the CAPA (Angold et al., 1999a). 3. Are symptomatic diagnoses associated with psycbosocial impairment?Diagnosed children were at increased risk for impaired functioning at home, at school, and with peers. In accord with clinical experience, impaired functioning was more conspicuous in children with disruptive behavior disorders (odds ratio [OR] = 7.6) than in children with anxiety or depression (OR = 4.3). 4. Are parent and child reports of psychopathology on the CAPA rekted to parent and teacher reports of problems on well-established scales for detecting psychopathology? In the GSMS the externalizing items of the Child Behavior Checklist (Achenbach, 1991) were used as a screen to oversample individuals for CAPA interviewing. In the 4 years following the screening questionnaire, rates of externalizing diagnoses from the W A were 4.5 times higher in the screen-high group than in the screen-low group (9% versus 2%). The GSMS collected data from teachers using the Teacher's Report Form (TRF) (Achenbach and Edelbrock, 1986). The mean 3-wave TRF score for those who never met criteria for a diagnosis was 12.8, compared with 19.9 for those with a diagnosis but without impairment ( p = .OOOS) and 32.3 for those with both diagnosis and impairment ( p < .OOO1 for comparison with no diagnosis andp = .0009 for comparison with diagnosis alone). 5. Do children with CAPA-identified disorders use more mental health services? A crude measure of the validity of CAPA symptom ratings is provided by the association between levels of CAPA DSM-111-R symptomatologyand the probability of having used specialty mental health services during the 3 months preceding the interview. Averaging across the whole range of symptom scores, using hierarchical mixed-effects logistic regression, each addtional DSM-111-R symptom was associated with a 10% increase in the odds of having received specialty mental health services during the preceding 3 months ( p < .0001) (Fig. 3). 6 Do WA-diagnosed children tend to comefiom families with a histoy of mental illness? Family history of mental illness is one of the strongest predictors of psychiatric disorder in children, although the specificity of links between particular disorders across generations remains in doubt. Across 4 waves of GSMS, children with a family history of treated mental illness were 3 times as likely to have diagnoses of anxiety or depressive disorders (10.7% versus 3.1%), while those with a family history of crime 45 A N G O L D A N D COSTELLO lor those with no diagnosis at the first assessment (risk ratio 6.4). There was also a high degree of diagnostic specificity in that continuity (Fig. 4), with risk ratios ranging from 7.4 for depression to 31.4 for substance abuse. 9. Do CAPA diagnoses predict negative 1;fe outcomes? 35 - 8 v Child and adolescent psychiatric disorders are strong predictors of serious negative life outcomes such as school dropout, expulsion from school, teen pregnancy, and arrests. In the GSMS data 14% youths with a diagnosed disorder, compared with only 1% of children without a diagnosed disorder, experienced one or more of these events (OR = 12.0). These negative events were, as expected, much more highly associated with behavioral diagnoses (OR = 36.3) than with anxiety or depression (OR = 2.0). 10. Do W Ainterviewer observations rehte meaningfdy to reported diagnosis and treatment?Two findings suggest that at least some of the CAPA interviewers' ratings of 'E3 3 0 5 - c 25(d %E 20x 70 r Diagnosis present last year Diagnosis absent last year I 3 t o 5 I 9 t o 1 1 I 1 5 t o 1 7 I >20 Oto2 6to8 12to14 18to20 Number of symptoms 6.4 Fig. 3 Relationship between DSM-IIZ-R symptom counts and service use in the Great Smoky Mountains Study. 7.9 13.4 or drug problems were almost twice as likely to have a behavioral diagnosis (9.0% versus 5.1%). ZIs there agenetic hadingfor the diagnosis?Monozygotic twins in the VTSABD were more concordant than dizygotic twins for ADHD, CD, ODD, separation anxiety, overanxious disorder, and depression (Eaves et al., 1997; Topolski et al., 1997). In many ways the appearance of genetic effects in twin studies is particularly convincing evidence that a test measures a real construct, because heritability estimates depend on patterns of correlation between pairs of individuals rated by different interviewers, and so they cannot be the result of interviewer halo effects. The fact that different disorders, as measured by the CAPA, show rather different patterns of genetic and environmental effects offers evidence of divergent validity. 8. Are W A diagnoses consistent over time? Many child and adolescent psychiatric disorders are chronic or recurrent, so we expect to see some continuity in diagnosis over time. In the GSMS 48% of youths with a diagnosis at one assessment had one a year later, compared with 7% of 46 26.5 14.8 7.4 " 1 CDlODD 1 Anxiety 1 SED 1 Substance abuse ADHD Depression Any Dx Fig. 4 Diagnostic continuity in the Great Smoky Mountains Study (figures above bars are odds ratios for comparisons between those with and those without a diagnosis in the preceding year). C D = conduct disorder; O D D = oppositional defiant disorder; A D H D = attention-deficit/hyperactivity disorder; SED = serious emotional disturbance; Dx = diagnosis. J . A M . ACAD. C H I L D A D O L E S C . PSYCHIATRY, 3 9 : 1 , JANUARY 2 0 0 0 CAPA intrainterviewbehavior are useful. First, interviewer ratings of overactivity and inattention during the interview are strongly related to parent-reported hyperactivity (note that here the interviewer rating the behavior is blind to the parental reports). In the GSMS, of children whose parents never reported them to have impairing ADHD symptoms at any of the 4 interview waves, 12% were observed to be overactive or inattentive during at least one of the interviews. Of those who met full DSM-III-R ADHD criteria by parent report, 52% were noted to have been overactive or inattentive during one of their CAPA interviews. Of those reported to have impairing subthreshold DSM-III-RADHD symptoms, 46% were noted to have been observably overactive or inattentive. A substantial group of children whose parents never reported them to have impairing A D H D symptoms had nonetheless received stimulant medications; half of these treated children were rated as being overactive or inattentive by interviewer observation. In addition, interviewer ratings of the presence of observed tics (a well-known side effect of stimulant medications) were much more common in children currently being treated with stimulants than in the same children when they were not taking stimulants. (Angold and Costello, unpublished). DEVELOPMENT OF THE CAPA FOR SPECIAL PURPOSES Twin CAPA A special version of the CAPA was developed for the VTSABD (see above). This version is streamlined in the symptom area to make it easier to conduct interviews about multiple children with both parents. It also contains a lifetime assessment of psychopathology based on CAPA interviewing principles (Eaves et al., 1997; Simonoff et al., 1997). Young Adult Psychiatric Assessment The Young Adult Psychiatric Assessment (YAPA) is a modification of the CAPA that is suitable for use with young adults. It provides a focus on diagnoses, living situations, relationships, and areas of functioning relevant to this age group. Preschool-Age Psychiatric Assessment The Preschool-Age Psychiatric Assessment (PAPA), a parent report-only version focused on children aged 3 to 6 years, is currently being developed. This version excludes symptoms of little relevance to younger children and has additional items pertinent to younger children’s behavior. Spanish CAPA Glorisa Canino, Ph.D., and her highly experienced multinational team of translators are currently preparing a multidialect Spanish version of the CAPA. Gatekeeper CAPA Computerization of the CAPA We have experimented with the use of a shorter “gatekeeper” interview approach to some major problem areas (anxiety, depression, CD, and ODD). A subset of key items was covered at the beginning of the interview, and the rest of the section was completed only by those with a positive response to gatekeeper questions. The rest of the diagnoses were treated as usual. The gatekeeper approach saved about 11 minutes on the parent interview and about 20 minutes on the interview with the child (times refer to the symptomatology and impairment sections of the interview). The shorter interview affected the number of diagnoses generated by the interview in only 1 out of 9 diagnosis-by-age comparisons: 12-year-olds reported significantly fewer C D diagnoses with the gatekeeper than with the standard interview. In the other 8 comparisons the numbers of diagnoses were not significantly different and there was no particular trend for the gatekeeper interview to result in fewer diagnoses. J . A M . ACAD. C H I L D A D O L E S C . PSYCHIATRY, 3 9 : 1 , JANUARY 2 0 0 0 An audio computer-administered version for selfreports in the substance use, abuse, and dependence section of the CAPA is currently in use. A computer-assisted version of the whole interview is currently under experimental development. CONCLUSIONS Clinical and Community Research Uses of the CAPA It is probably fair to say that clinicians do not enjoy doing respondent-based interviews very much because the questions they can ask are so highly constrained. They may not be convinced that the child understood the question, but if they add their own questions then the advantages of using a respondent-based interview are lost, because an unstructured component has been added. On the other hand, training on an interviewer-based interview is usually of interest to clinicians because it raises a 47 A N G O L D A N D COSTELLO host of issues about interviewing style and strategy that few have had time or encouragement to think through during their training. Thus, interviewer-based interviews may be particularly suitable for use in clinical assessments, and the CAPA has been used in several clinical and treatment studies. Given the fact that well-trained and supervised Lay interviewers can produce reliable ratings of symptoms and diagnoses, lay-administered CAPAs can also be used in the initial evaluation of children and adolescents presenting for clinical services. When it comes to general population studies, there has been more debate about the place of interviewer-based instruments. However, the development of detailed glossaries and training manuals now makes it perfectly possible to train “lay” interviewers adequately and to achieve levels of reliability as good as those found with respondent-based interviews. Some of the largest ongoing general population studies are using interviewer-based instruments, including the CAPA (Burns et al., 1995; Costello et al., 1996; Eaves et al., 1997; Lewinsohn et al., 1993; Simonoff et al., 1997). Some people are concerned about the relative costs of training and quality control between interviewer-based and respondent-based interviews, but when we compared the cost per subject interviewed, using figures from recently hnded NIMH studies, we found the cost differential small or nonexistent. At the present time, it seems that decisions about whether to use an interviewer-based interview in any type of study or clinical application should be made on the basis of which interview collects the information best suited to answering the questions being asked. USER INFORMATION An extensive CAPA information packet is available from the first author. At the time of writing this includes interview schedules and the glossary plus details of the CAPASpsychometric performance at a cost of $50. REFERENCES Achenbach TM (199I), Manualfor the Child Behavior Checklist 4 4 8 and 1991 Projh. Burlington: University of Vermont Department of Psychiatry Achenbach TM, Edelbrock CS (1986),Manualfor the Teacher: Report Form and Teacher Krsion of the Child Behavior Pro&. Burlington: University of Vermont Department of Psychiatry American Psychological Association (1985),Standard for Educational and Psychological Testing.Washington, DC: American PsychologicalAssociation Anastasi A (1986), Evolving concepts of test validation. Annu Rev Pychol 37:1-15 Angold A, Costello EJ (1995),A test-retest reliability study of child-reported psychiatric symptoms and diagnoses using the Child and Adolescent PsychiatricAssessment (CAPA-C). Psychol Med 25:755-762 Angold A, Costello EJ, Erkanli A (1999a), Comorbidity. J Child Pychol Prychiawy 4057-87 48 Angold A, Costello EJ, Farmer EMZ, Burns BJ, Erkanli A (1999b),Impaired but undiagnosed.J A m Acad ChildAdolesc Pychiatry 38:129-137 Angold A, Costello EJ, Worthman CM (1998),Puberty and depression: the roles of age, pubertal status, and pubertal timing. PsycholMed 28:51-61 Angold A, Erkanli A, Costello EJ, Rutter M (1996),Precision, reliability and accuracy in the dating of symptom onsets in child and adolescent psychopathology. J Child Pychol Pychiany 37:657-664 Angold A, Fisher PW (1999),Interviewer-based interviews: In: Diagnostic Assessment in Child and Adolescent Psychopathology, Shaffer D, Lucas CD, Richters JE, eds. New York: Guilford, pp 34-64 Angold A, Prendergast M, Cox A, Warrington R, Simonoff E, Rutter M (1995),The Child and Adolescent PsychiatricAssessment (CAPA). Psychol Med 25:739-753 Ascher BH, Farmer EMZ, Burns BJ, Angold A (1996),The Child and Adolescent Services Assessment (CASA): description and psychometrics. J Emotional Behau Disord 4:12-20 Breton J-J, Bergeron L, VdIa J-P, Lepine S, Houde L, Gaudet N (1995),Do children aged 9 to 11 years understand the DISC version 2.25 questions? J A m Acad Child Adolesc Pychiatty 34:946-956 Burns BJ, Costello EJ, Angold A et al. (1995), Children’s mental health service use across service sectors. Health Af14:147-159 Costello EJ, Angold A, Burns BJ et al. (1996),The Great Smoky Mountains Study of Youth: goals, designs, methods, and the prevalence of DSM-IIIR disorders.Arch Gen Pychiany 53:1129-1136 Costello EJ, Angold A, March J, Fairbank J (1998a),Life events and posttraumatic stress: the development of a new measure for children and adolescents. Pychol Med 28:1275-1288 Costello EJ, Messer SC, Reinherz HZ, Cohen P, Bird HR (1998b),The prevalence of serious emotional disturbance: a re-analysis of community studies.J ChildFam Stud 7:411-432 Cox A, Hopkinson K, Rutter M (1981a),Psychiatric interviewingtechniques, 11: naturalistic study-eliciting factual information. Br J Pychiatry 138:283-291 Cox A, Rutter M, Holbrook D (1981b),Psychiatric interviewing techniques, V experimental study+liciting factual information.BrJPychiatty 139:27-37 Cronbach LJ, Meehl PE (1955),Construct validity in psychological tests. Pychol Bull 52:281-302 Eaves LJ, Silberg JL, Maes H H et al. (1997),Genetics and developmentalpsychopathology, 2: the main effects of genes and environment on behavioral problems in the Virginia Twin Study of Adolescent Behavioral Development. J Child Pychol Psychiatty 38:965-980 Farmer EMZ, Angold A, Burns BJ, Costello EJ (1994), Reliability of selfreported service use: test-retest consistency of children’s responses to the Child and Adolescent Services Assessment (CASA). J Child Fam Stud 3~307-325 Gulliksen H (1950),Intrinsic validity. Am Pzychol5:511-517 Jenkins JG (1946),Validity for what?/ Consult Clin Psychol 10:93-98 Jensen ,’l Roper M, Fisher PW et al. (1995), Test-retest reliability of the Diagnostic Interview Schedule for Children (DISC 2.1): parent, child, and combined algorithms. Arch Gen Pychiatry 52:61-71 Lahey BB, Schwab-Stone M, Goodman SH et al. (in press), Age and gender differences in oppositional behavior and conduct problems: a cross-sectional household study of middle childhood and adolescence. J Abnomz Child P.&ol Lewinsohn PM, Rohde 0, Seeley JR, Fischer SA (1993),Age-cohort changes in the lifetime occurrence of depression and other mental disorders. J Abnorm Pychol102:110-120 Messer SC, Angold A, Costello EJ, Burns BJ (1996),The Child and Adolescent Burden Assessment (CABA): measuring the family impact of emotional and behavioral problems. Int /Methods Psychiatr Res 6:261-284 Rutter M, Cox A, Egert S, Holbrook D, Everitt B (1981),Psychiatric interviewing techniques, IV: experimental study: four contrasting styles. B r j Psychiatry 138:456-465 Simonoff E, Pickles A, Meyer J M et al. (1997),The Virginia Twin Study of Adolescent Behavioral Development: influences of age, sex and impairment on rates of disorder. Arch Gen Pychiat?y 54:801-808 Topolski TD, Hewitt JK, Eaves LJ et al. (1997),Genetic and environmental influences on child reports of manifest anxiety and symptoms of separation anxiety and overanxious disorders: a community-based twin study. Behau Genet 27: 15-28 Wallace SR (1965),Criteria for what?Am Pychol20:411-417 Weitz J (1961),Criteria for criteria. Am Pychol 16:228-231 J . AM. A C A D . C H I L D A D O L E S C . PSYCHIATRY, 39:1, JANUARY 2000