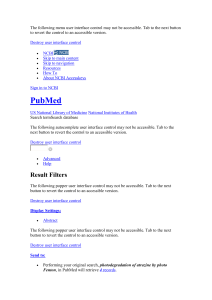
ARTHRITIS & RHEUMATISM Vol. 52, No. 1, January 2005, pp 128–135 DOI 10.1002/art.20776 © 2005, American College of Rheumatology Role of Interleukin-1 and Tumor Necrosis Factor ␣ in Matrix Degradation of Human Osteoarthritic Cartilage Masahiko Kobayashi,1 Ginette R. Squires,1 Aisha Mousa,1 Michael Tanzer,2 David J. Zukor,3 John Antoniou,3 Ulrich Feige,4 and A. Robin Poole1 Objective. To determine whether interleukin-1 (IL-1) or tumor necrosis factor ␣ (TNF␣), or both, plays a role in the excessive degradation that is observed in cultured osteoarthritic (OA) articular cartilage. Methods. Antagonists of IL-1 and TNF␣, namely, IL-1 receptor antagonist and the PEGylated soluble TNF␣ receptor I, respectively, were added at different concentrations to explant cultures of nonarthritic (5 obtained at autopsy) and OA (15 obtained at arthroplasty) articular cartilage. The cleavage of type II collagen (CII) by collagenase was measured by an immunoassay in cartilage and culture media. Proteoglycan (mainly aggrecan) content and degradation were measured by a colorimetric assay for glycosaminoglycan (GAG) content in cartilage and culture media. Reverse transcriptase–polymerase chain reaction was used to analyze gene expression of matrix metalloproteases (MMPs) 1, 3, and 13, CII, aggrecan, IL-1, and TNF␣. Results. Antagonists of IL-1 and TNF␣ inhibited the increase in CII cleavage by collagenase as well as the increase in GAG release observed in OA cartilage compared with normal cartilage. Inhibition was significant in tissue from some patients but not from others, although significant inhibition was observed when all the results were analyzed together. An increase in the GAG content in cartilage was seen in 4 of 15 cases. However, this increase was not significant when all the data were combined. Preliminary results indicated no effect of these antagonists on nonarthritic cartilage from 3 different donors. Independent analyses of gene expression in cultured cartilage from 9 other OA patients revealed that IL-1 or TNF␣ blockade, either alone and/or in combination, frequently down-regulated MMP-1, MMP-3, and MMP-13 expression. Expression of IL-1 and TNF␣ was inhibited by either antagonist or by the combination in essentially half the cases. The combined blockade up-regulated aggrecan and CII gene expression in approximately half the cases. Conclusion. These results suggest that the autocrine/paracrine activities of TNF␣ and IL-1 in articular cartilage may play important roles in cartilage matrix degradation in OA patients but not in all patients. Inhibition of either or both of these cytokines may offer a useful therapeutic approach to the management of OA by reducing gene expression of MMPs involved in cartilage matrix degradation and favoring its repair. Dr. Poole’s work was supported by Shriners Hospitals for Children, Amgen, the Canadian Institutes of Health Research, the Canadian Arthritis Network, and the National Institute on Aging, NIH. 1 Masahiko Kobayashi, MD, PhD (current address: Kyoto City Rehabilitation Hospital, Kyoto, Japan), Ginette R. Squires, PhD, Aisha Mousa, MSc, A. Robin Poole, PhD, DSc: Shriners Hospital for Children, Montreal, Quebec, Canada; 2Michael Tanzer, MD: Montreal General Hospital, McGill University, Montreal, Quebec, Canada; 3 David J. Zukor, MD, John Antoniou, MD: Jewish General Hospital, McGill University, Montreal, Quebec, Canada; 4Ulrich Feige, PhD: Amgen, Thousand Oaks, California. Address correspondence and reprint requests to A. Robin Poole, PhD, DSc, Joint Diseases Laboratory, Shriners Hospitals for Children, Departments of Surgery and Medicine, McGill University, 1529 Cedar Avenue, Montreal, Quebec H3G 1A6, Canada. E-mail: [email protected]. Submitted for publication February 11, 2004; accepted in revised form October 8, 2004. Osteoarthritis (OA) is a slowly progressive degenerative disease characterized by early loss of the tensile strength of articular cartilage (1), which is produced by a fibrillar network composed of type II collagen (CII) (1,2). Excessive degradation of CII (3,4), such as that induced by collagenase, is a feature of OA (5–7) and rheumatoid arthritic (3) articular cartilage. The compressive stiffness of joint cartilage depends on the swelling pressure achieved by hydration of proteoglycan (1). Thus, the net loss of proteoglycan that occurs in the early stage of OA results in reduced stiffness of the cartilage (1,6). Damage to collagen is eventually accompanied by loss of the proteoglycans aggrecan, biglycan, 128 IL-1 AND TNF␣ IN CARTILAGE DEGRADATION and decorin (1,8,9). These changes first occur at, and close to, the articular surface (9,10). Proinflammatory cytokines, such as interleukin-1 (IL-1) and tumor necrosis factor ␣ (TNF␣), are suspected of causing damage to OA cartilage by inducing matrix metalloproteinase (MMP) expression in chondrocytes in an autocrine/paracrine manner (11–13). Both cytokines activate synthesis and release of MMPs, which leads to matrix breakdown (1,6,13). Elevated levels of IL-1 are found in OA synovial fluid, and gene expression of IL-1 is up-regulated in OA cartilage (6). Two receptors for IL-1 have been identified, IL-1 receptor type I (IL-1RI) and IL-1RII, which mediate the biologic activation of cells by IL-1 (14). TNF␣, as well as IL-1, can induce cartilage degradation (1,6,11,13). TNF␣ content is elevated in the synovial fluid of OA joints. There are 2 cell surface receptors for TNF␣ (TNFR) namely, p55 (TNFRI) and p75 (TNFRII) (15–17). TNF␣ exerts its biologic effect following intracellular signaling with the high-affinity TNFRI under in vivo conditions. Expression of TNFRI has been localized in cells at sites of focal loss of proteoglycans in OA cartilage (18). TNF␣ and TNFRs I and II are upregulated in OA cartilage (1,6,13). IL-1 is regulated by a naturally occurring soluble IL-1 receptor antagonist (IL-1Ra), a 22-kd glycosylated protein that is a natural inhibitor of IL-1 (19–22). In IL-1Ra–deficient mice, a destructive and inflammatory arthropathy similar to human RA develops spontaneously (23), suggesting that endogenous IL-1Ra functions to suppress inflammation in mice. The administration of IL-1Ra suppresses joint erosion in human RA (24). Moreover, intraarticular injections of IL-1Ra or transfection of IL-1Ra gene can ameliorate the progression of experimental OA in animal models (25). The soluble TNF receptors sTNFRI and sTNFRII are shed by proteolytic cleavage of the extracellular domain of TNFRI and TNFRII (26). The shed receptors retain their ability to bind TNF␣. TNFRI is regarded as a dominant receptor for intracellular signaling because the primary inflammatory responses to soluble TNF␣ are mediated by TNFRI signaling in vivo. Studies using either a neutralizing chimeric (mouse– human) TNF␣-specific monoclonal antibody (27) or an sTNFRII:Fc fusion protein (28) have resulted in significant benefit in RA patients. More recently, PEGylated sTNFRI has been developed. It is well tolerated, nonimmunogenic, and has a long half-life, and preliminary evidence of efficacy has been shown in RA patients (29). The triple-helical cleavage of CII is mediated primarily by collagenases that belong to the MMP family 129 (1,6,30). Three of the known human collagenases, collagenase 1 (MMP-1), collagenase 2 (MMP-8), and collagenase 3 (MMP-13), have been shown to cleave triplehelical CII between residues 775 (glycine) and 776 (leucine). Each of these collagenases produces the characteristic large TCA (three-quarter–length) and smaller TCB (one-quarter–length) cleavage products of the constituent ␣-chain (5). Recently, we developed an antibody that recognizes the carboxy-terminal neoepitope (Col23/4Cshort) of the TCA fragment. It has been used in an immunoassay to provide the first direct evidence that there is increased CII cleavage in OA cartilage (5,7) in association with increased collagenase expression and content (31,32). This activity probably mainly involves MMP-1 and MMP-13 (7). Degradation of the proteoglycan aggrecan in OA involves the activation of MMPs and aggrecanases (30,31,33), which cleave the core protein at different sites in both the interglobular domain and the chondroitin sulfate–rich region (30,34). There is a general consensus that MMPs contribute to chondrocyte-mediated matrix degeneration of OA cartilage. However, as yet, the relative importance of each of the MMPs and the factors responsible for their expression are not fully understood, and the importance and involvement of IL-1 and TNF␣ in the resorption of articular cartilage seen in OA remain unclear. This is mainly because of the lack of any direct evidence that inhibition of the activity of either or both of these cytokines would reduce matrix degradation in articular cartilage in OA. The purpose of this study was to determine if the up-regulation of chondrocyte-derived TNF␣ and IL-1 that is seen in OA may contribute to the increased matrix degradation in articular cartilage observed in this disease. We report the first direct evidence that the excessive CII cleavage by collagenases and proteoglycan degradation (measured as release from cartilage) can be arrested in some cases by TNF␣ or IL-1 blockade using PEGylated sTNFRI and/or IL-1Ra (anakinra) or combinations thereof. Evidence for matrix regeneration is also presented. These observations implicate these cytokines in cartilage degeneration in OA and suggest that blockade of either or both of these cytokines may be a valuable therapeutic strategy in the management of OA in a group of patients with this disease. MATERIALS AND METHODS Anticytokines. Recombinant human IL-1Ra (anakinra) (21,22) and PEGylated sTNFRI, comprising a high molecular weight polyethylene glycol molecule attached at the 130 N-terminus (29), were both prepared by Amgen (Thousand Oaks, CA) and stored at ⫺80°C. Cartilage. Human femoral condylar cartilage was obtained at the time of total knee arthroplasty from 32 patients with OA, which was diagnosed according to the criteria of the American College of Rheumatology (35). Cartilage from 15 patients (4 men and 11 women; mean ⫾ SD age 67.3 ⫾ 20.1 years) was used for explant culture, cartilage from 8 patients (2 men and 6 women; mean ⫾ SD age 69.3 ⫾ 8.3 years) was used for RNA extraction without culture, and cartilage from 9 patients (1 man and 8 women; mean ⫾ SD age 70.7 ⫾ 9.2 years) was used for RNA extraction after culture. Cartilage from 8 nonarthritic joints was obtained at autopsy (within 16 hours of death) from site-matched regions with no evidence of macroscopic articular degeneration. Of these, cartilage from 5 persons (2 men and 3 women; mean ⫾ SD age 54.4 ⫾ 20.1 years) was cultured as explants without anticytokines to establish normal controls. Cartilage from 3 others (3 women; mean ⫾ SD age 62.3 ⫾ 1.2 years) was cultured as explants with the anticytokines. None of the persons without arthritis had diabetes or had received chemotherapy prior to death. Cartilage preparation. Cartilage was prepared as previously described (36). Briefly, the cartilage samples were washed 3 times with medium A, containing Dulbecco’s modified Eagle’s medium (Gibco BRL, Grand Island, NY) with 20 mM HEPES buffer (pH 7.4) (Gibco BRL), 45 mM NaHCO3, 100 units/ml penicillin, 100 g/ml streptomycin, and 150 g/ml gentamicin sulfate. Full-depth cartilage slices from a single area, ⬃20 mm ⫻ 20 mm, were cut vertical to the articular surface and then into cubes of ⬃2 mm ⫻ 2 mm (5–7 cubes were randomly obtained, and wet weights ⬃60 mg per well were determined). These were placed in culture wells (48-well Costar 3548 plate; Corning, Corning, NY). Samples were held in preculture conditions for 24–48 hours at 37°C in 1 ml of medium A supplemented with 50 g/ml L-ascorbic acid (Gibco BRL), 0.1 mg/ml bovine serum albumin (Sigma, St. Louis, MO), and 5.0 g/ml insulin, 5.0 g/ml transferrin, and 5.0 ng/ml sodium selenite (ITS; Boehringer Mannheim, Dorval, Quebec, Canada) (medium B). Cartilage explant culture. The media were changed on day 0. Thereafter, media were replaced every 4 days. PEGylated sTNFRI at 100 ng/ml, 500 ng/ml, or 1,000 ng/ml; IL-1Ra (anakinra) at 20 ng/ml or 100 ng/ml; or PEGylated sTNFRI at 100 ng/ml plus IL-1Ra at 20 ng/ml, PEGylated sTNFRI at 500 ng/ml plus IL-1Ra at 100 ng/ml, or PEGylated sTNFRI at 1,000 ng/ml plus IL-1Ra at 100 ng/ml were freshly added to medium B from day 0 at each medium change. In view of limitations imposed by cartilage availability, not all these concentrations could always be used in any one study. Hence, selected concentrations were examined for each donor. This ensured that a range of concentrations could be examined for the complete study of all donors. Protein controls were not used in these studies since we had no access to what we considered acceptable control proteins for IL-1Ra and PEGylated sTNFRI. Cartilage (triplicate cultures for each analytical point) was cultured for up to 16 days. The conditioned media were collected at each medium change from day 4 to day 16 and stored at ⫺20°C until further analyzed. Cartilage explants were also harvested and stored at ⫺20°C until analyzed. The KOBAYASHI ET AL availability of articular cartilage in each OA patient determined the number of additions that could be studied. Extraction and assay of cartilage explants and media for collagenase-cleaved, denatured, and total CII content. OA cartilage explants from day 16 of culture were digested for extraction of collagenase-cleaved (5), denatured, and total CII (4), as previously described. The conditioned media were assayed for the cleavage neoepitope, and the cumulative neoepitope in the conditioned media was calculated by totaling the data from each medium change day. Total cleavage neoepitope in cartilage and media was calculated by summing the cartilage and culture media data, expressed as pmoles of peptide/mg wet weight of cartilage, based on the molecular weight of the standard peptide epitope of 608. Determination of proteoglycan content and release. The content and release of proteoglycan were determined in cartilage extract and conditioned culture media as sulfated glycosaminoglycan (GAG), which is primarily a measure of proteoglycan aggrecan content, using a modification of the colorimetric dimethylmethylene blue dye-binding assay (37). Cumulative proteoglycan release (GAG in the media) and its content in cartilage (GAG in the cartilage) were expressed as g GAG/mg wet weight of cartilage. GAG release into medium was represented as a percentage of the total cumulative GAG in the cartilage plus cumulative GAG release into medium. This provides a more accurate presentation of release, accounting for the marked variation in cartilage GAG content (7,8). Total RNA extraction and isolation. Total RNA was isolated directly from cartilage without culture or from cartilage explants after culture by the acid guanidinium isothiocyanate procedure according to the method of Chomczynski and Sacchi (38), with some modifications. OA cartilage specimens from 8 patients (in which matrix degradation was not studied due to limited amounts of tissue) were subjected to RNA extraction without culture. OA cartilage explants from 9 patients were cultured with or without IL-1Ra (anakinra) at 100 ng/ml, or PEGylated sTNFRI at 1,000 ng/ml, or a combination of the 2 over 24 hours. After that, the explants were harvested and subjected to RNA extraction. Briefly, cartilage tissue (200–300 mg) was homogenized in solution D (4M guanidinium isothiocyanate, 20 mM sodium acetate, pH 5.2, containing 0.1M 2-mercaptoethanol and 0.5% N-lauroylsarcosine). One volume of isopropanol was added to the mixture, and all proteins and nucleic acids were precipitated at ⫺20°C overnight. After centrifugation at 4°C, the pellet was digested with 1 mg/ml proteinase K (molecular biology grade; Gibco BRL) at 65°C for 2 hours. After digestion, the mixture was extracted with 1 volume of phenol and 0.1 volume of chloroform/alcohol (49:1). The aqueous phase was recovered after centrifugation at 4°C and precipitated with 1 volume of ethanol at ⫺80°C overnight. After centrifugation, the pellet was washed with 70% ethanol to remove any excess salt. The total RNA pellet was resuspended in diethyl pyrocarbonate–treated water, and the amount of total RNA was quantitated by measuring the optical density at 260 nm. Reverse transcription and polymerase chain reaction (PCR). Solution (1 l) from reverse transcription was incubated in 50 l reaction mixture containing 2.5 units of AmpliTaq DNA polymerase (Applied Biosystems, Branchburg, NJ) in 50 mM KCl, 1.5 mM MgCl2, 10 mM Tris HCl, pH 8.3, 200 IL-1 AND TNF␣ IN CARTILAGE DEGRADATION 131 Table 1. Primer sets used for polymerase chain reaction* MMP-1 MMP-13 MMP-3 IL-1 TNF␣ COL2A1 Aggrecan GAPDH Forward Reverse 5⬘-AAAGGGAATAAGTACTGGG-3⬘ 5⬘-GATAAAGACTATCCGAGAC-3⬘ 5⬘-TGCGTGGCAGTTTGCTCAGCC-3⬘ 5⬘-GTCTCCTACCAGACCAAG-3⬘ 5⬘-GTCTCCTACCAGACCAAG-3⬘ 5⬘-GAACCCAGAACAACACAATCC-3⬘ 5⬘-TGAGGAGGGCTGGAACAAGTACC-3⬘ 5⬘-GCTCTCCAGAACATCATCCCTGCC-3⬘ 5⬘-GTTTTTCCAGTGTTTTCCTCAG-3⬘ 5⬘-CGAACAATACGGTTACTC-3⬘ 5⬘-GAATGTGAGTGGAGTCACCTC-3⬘ 5⬘-GAAGTCAGTTATATCCTGGC-3⬘ 5⬘-CAAAGTAGACCTGCCCAGACTC-3⬘ 5⬘-AGAGGGGAGAAAAGTCCGAAC-3⬘ 5⬘-GGAGGTGGTAATTGCAGGGAACA-3⬘ 5⬘-CGTTGTCATACCAGGAAATGAGCTT-3⬘ * MMP ⫽ matrix metalloproteinase; IL-1 ⫽ interleukin-1; TNF␣ ⫽ tumor necrosis factor ␣. M dNTP mixture, and 0.4 mole each of the oligonucleotide primer pairs. The final PCR protocols were as follows: 30 cycles of denaturation at 95°C for 1 minute, annealing at 50–56°C for 1 minute, and extension at 72°C for 5 minutes, followed by a 10-minute postextension at 72°C. Prior analyses showed that this number of cycles at a given sample dilution ensured that the product was generated in a manner proportional to the sample messenger RNA (mRNA) content. The primers for MMP-1, MMP-13, IL-1, TNF␣, COL2A1, aggrecan, and GAPDH are listed in Table 1. The annealing temperature was 50°C for MMP-1, MMP-13, IL-1, and GAPDH, and 56°C for TNF␣, COL2A1, and aggrecan. PCR product sizes were verified by electrophoresis in 1.5% agarose gel. GAPDH was used as a reference to demonstrate equal gel loading. The analyses were conducted in the previously described manner (39), whereby each analysis was performed at least 3 times at different dilutions of each sample of the original complementary DNA to ensure the accuracy of the results. The band intensities were determined to be below saturation by dilution and cycle variation. Other details are as previously described (39). The digital images of each PCR product were analyzed in relationship to GAPDH using image analysis software (NIH Image 1.60; National Institutes of Health, Bethesda, MD; online at http://rsb.info.nih.gov/nihimage/) to evaluate the relative pixel intensity of the band of PCR products. The autobackground subtraction was used to control for the background signal. Statistical analysis. Data were expressed as the mean ⫾ SD. Cultures and assays were performed at least in triplicate. To analyze treatment effects on a group study, mean values for individual patient cartilage were determined first. These were then expressed as the mean ⫾ SD for each group. A one-way analysis of variance was used employing Dunnett’s correction and Prism software (GraphPad Software, San Diego, CA). Spearman’s rank correlations were used to compare the effects on collagen and proteoglycan degradation and of TNF␣ with IL-1 inhibition. P values less than 0.05 were considered statistically significant. RESULTS Effects of PEGylated sTNFRI and IL-1Ra (anakinra) on CII cleavage by collagenase and proteoglycan degradation. Cleavage of CII was increased in OA cartilage over that observed in normal cartilage (Figure 1). In individual studies, significant inhibition was observed in 7 of 15 cases; in others, nonsignificant reductions were commonly observed (data not shown). When analyzed together, the addition of IL-1Ra and/or PEGylated sTNFRI to cultures of OA articular cartilage was found to significantly reduce this cleavage of CII (Figure 1). Cleavage was reduced by PEGylated sTNFRI at 500 ng/ml and by 2 of the 3 combinations tested with IL-1Ra. Both concentrations of IL-1Ra tested were equally active (Figure 1). Inhibition of the excessive release of GAG in OA cartilage was significant in 5 of 15 cases, with nonsignificant reductions noted in other cartilage (data not shown). When all cartilage was analyzed together, a significant inhibition of GAG release was also observed at 500 ng/ml PEGylated sTNFRI, by both concentrations Figure 1. Inhibition of type II collagen (CII) cleavage in osteoarthritic (OA) cartilage explants (number of samples shown in parentheses) by interleukin-1 receptor antagonist (IL-1Ra) and tumor necrosis factor ␣ (TNF␣) at the indicated concentrations. Nonarthritic normal cartilage cultured without these additives is shown for comparison. Values are the mean and SD number of CII cleavage epitopes generated by collagenase (Col2-3/4Cshort or C1,2assay) in cartilage and medium over 16 days of culture with or without PEGylated soluble TNF␣ receptor I (sTNFRI) and/or IL-1Ra. ⴱ ⫽ P ⬍ 0.05 versus control OA culture. 132 Figure 2. Inhibition of glycosaminoglycan (GAG) degradation in OA cartilage explants (number of samples shown in parentheses) by IL-1Ra and TNF␣ at the indicated concentrations. Values are the mean and SD percentage release of total GAG into medium over 16 days of culture. ⴱ ⫽ P ⬍ 0.05 versus control OA culture. See Figure 1 for other definitions. of IL-1Ra and by all 3 combinations of these antagonists (Figure 2). An increase in GAG content was observed in 4 of 15 cases (Figure 3). For the group as a whole, the combined analyses failed to reveal any effects of either or both antagonists together on total GAG content (data not shown). Correlations between degradation of CII and proteoglycan and their inhibition. When all results were examined using Spearman’s rank analyses for correlations between the collagenase-generated cleavage and the percentage of GAG release into the medium, there was a significant positive correlation (rs ⫽ 0.559, P ⬍ 0.0001). But when collagen cleavage was compared with the GAG content in the cartilage, there was a significant negative correlation (rs ⫽ ⫺0.533, P ⬍ 0.0001). A negative correlation between GAG release and GAG content (rs ⫽ ⫺0.863, P ⬍ 0.0001) was also observed. Although not always apparent in individual analyses, studies of all patients revealed that total CII cleavage epitope (rs ⫽ 0.953, P ⬍ 0.0001), GAG release (rs ⫽ 0.959, P ⬍ 0.0001), and GAG content (rs ⫽ 0.971, P ⬍ 0.0001) in IL-1Ra–treated specimens were each positively correlated with comparable results for PEGylated sTNFRI–treated specimens. However, when we examined within a patient the inhibitory effects of either cytokine antagonist on collagen cleavage versus inhibition of GAG release and increase in GAG content, there was very little evidence for combined inhibition of both collagen and GAG release and an increase in GAG content. Thus, in 3 of 15 cases, collagenase activity alone was arrested, with no effect on GAG release or content. KOBAYASHI ET AL In 2 of 15 cases, collagen cleavage, as well as GAG release, was inhibited. Collagenase inhibition was observed, with an increase in GAG content (no effect on release) in 1 of 15 cases. In no instance was there an inhibition of collagen cleavage with an inhibition of GAG release and an increase in GAG content. Thus, it is clear that inhibition of GAG degradation and an increase in content are usually not observed together. Neither is there evidence for any consistent linkage between inhibition of collagenase activity and inhibition of proteoglycan degradation with an increase in content. Effects of PEGylated sTNFRI and IL-1Ra (anakinra) on matrix degradation in normal cartilage explants. Preliminary studies revealed that neither IL1Ra, PEGylated sTNFRI, nor their combination had a significant effect on CII cleavage, GAG release, or GAG content in nonarthritic cartilage from 3 donors (data not shown). Figure 3. Increase in glycosaminoglycan (GAG) content in 4 OA cartilage samples (each from a different patient) due to cytokine inhibition. Media additions were PEGylated sTNFRI at 100 ng/ml (T1), 500 ng/ml (T2), or 1,000 ng/ml (T3); IL-1Ra (anakinra) at 20 ng/ml (I1) or 100 ng/ml (I2); or PEGylated sTNFRI at 100 ng/ml plus IL-1Ra at 20 ng/ml (T1I1), PEGylated sTNFRI at 500 ng/ml plus IL-1Ra at 100 ng/ml (T2I2), or PEGylated sTNFRI at 1,000 ng/ml plus IL-1Ra at 100 ng/ml (T3I2). OA represents the control culture with no additions. Values are the mean and SD GAG content in OA cartilage cultured for 16 days with PEGylated sTNFRI and/or IL-1Ra. ⴱ ⫽ P ⬍ 0.05 versus control OA culture. See Figure 1 for other definitions. IL-1 AND TNF␣ IN CARTILAGE DEGRADATION 133 In 3 of these 6 cases, PEGylated sTNFRI suppressed MMP-1 expression. IL-1Ra treatment or the combination suppressed MMP-13 expression in 3 of 7 cases, and PEGylated sTNFRI inhibited expression in 1 of 7 cases. The combination suppressed MMP-1 expression in 7 of 9 cases and MMP-13 in 6 of 7 cases. MMP-3 expression was effectively inhibited by these cytokine antagonists. MMP-3 was down-regulated by IL-1Ra in 6 of 9 cases and by PEGylated sTNFRI in 5 of 9; the combination suppressed expression in all 9 cases. In 4 of 9 cases, IL-1 gene expression was suppressed by IL-1Ra and in 3 of these 4, by PEGylated sTNFRI as well. Gene expression of TNF␣ was suppressed in 4 of 8 cases by IL-1Ra and in 6 cases (4 of 4 in which IL-1Ra inhibition occurred) by PEGylated sTNFRI. The combination suppressed IL-1 expression in 3 of 9 cases, whereas TNF␣ expression was suppressed in 5 of 8 cases. COL2A1 expression was enhanced in 1 of 8 cases by IL-1Ra, in 3 of 8 cases by PEGylated sTNFRI, and in 3 of 8 cases by the combination. Aggrecan expression was up-regulated in 4 of 9 cases by IL-1Ra, in 3 of 9 cases by PEGylated sTNFRI, and in 5 of 9 cases by the combination (Figure 4). These effects on the expression of collagen and aggrecan matrix molecules were not correlated. DISCUSSION Figure 4. Effects of IL-1Ra at 100 ng/ml and sTNFRI at 100 ng/ml or their combination on gene expression. OA cartilage specimens from 9 patients were cultured for 24 hours with and without 100 ng/ml IL-1Ra (ILA), 100 ng/ml sTNFRI (STR), or their combination (Comb). GAPDH is used as the loading reference. MMP ⫽ matrix metalloproteinase; IL-1 ⫽ interleukin-1. See Figure 1 for other definitions. Alterations of gene expression in OA cartilage explants by PEGylated sTNFRI and/or IL-1Ra, analyzed by nonquantitative reverse transcription–PCR. Since it was not possible to conduct studies of matrix degradation and gene expression on the same samples due to lack of sufficient tissue obtained at arthroplasty, cartilage specimens from other patients were cultured for 24 hours with or without IL-1Ra (anakinra) at 100 ng/ml, PEGylated sTNFRI at 1,000 ng/ml, or their combination and were examined (Figure 4). Where detectable, gene expression of MMP-1, MMP-13, and MMP-3 was suppressed by either antagonist or by the combination in the specimen examined. In 6 of 9 cases, IL-1Ra and the combination down-regulated MMP-1 gene expression. When OA cartilage degeneration is examined in culture, it is apparent that there is excessive and continuous degradation of CII and proteoglycan, as shown here and as shown previously for CII (5,7). Although the mechanism responsible for this progressive pathologic degradation is not understood, IL-1 and/or TNF␣ have been hypothesized to be involved. Here, we show that the degradation of CII and proteoglycan in OA cartilage can be arrested to varying degrees (some of which are significant) in individual patients by blockade of IL-1 and/or TNF␣ activity and that these inhibitions are also significant when all analyses are examined together. The inhibitory effects of these cytokine antagonists on CII versus proteoglycan degradation were clearly not interrelated, although a direct correlation was observed between collagen cleavage and proteoglycan release, irrespective of treatment. Moreover, the more collagen cleavage and GAG release we observed, the less proteoglycan was present in the cartilage. In most cases involving an arrest of CII cleavage, we observed inhibition with each cytokine antagonist alone and with both in combination. In one case, the combination had no effect, whereas the individual an- 134 tagonists were inhibitory. In another case, IL-1Ra was inhibitory but not the combination (data not shown). Such differences no doubt reflect the heterogeneity of the tissue from patient to patient in terms of responsiveness and our inability to adequately ensure the preparation of completely “homogeneous” aliquots of the chopped cartilage from a given joint. While the decreases in MMP mRNA seen in some patients is consistent with the inhibition in CII degradation, it was not possible to determine whether there was a correlation between these effects in individual patients since the matrix and mRNA analyses had to be conducted on separate patients in view of limitations in the amount of tissue available at arthroplasty. IL-1 or TNF␣ blockade caused a suppression of the expression of these same cytokines in a number of cases, further pointing to the autocrine/paracrine role of these chondrocyte-derived cytokines in this degradation process. Moreover, blockade of IL-1 expression also often resulted in suppression of TNF␣ expression and vice versa. These observations provide important evidence to indicate linkages in the functional activities of these cytokines generated by chondrocytes. Soluble IL1RII has been shown to inhibit IL-1–induced nitric oxide and/or prostaglandin E2 production in chondrocytes (41). Using gene array analysis, a recent study has shown that OA cartilage lacks mRNA expression of IL-1Ra and decoy IL-1RII, which may allow IL-1 to drive pathologic change (40). The role of TNF␣ in OA cartilage degradation has been regarded as being less clear than that of IL-1. However, our results indicate that TNF␣ blockade can be chondroprotective in cultured OA cartilage and as effective as IL-1Ra in the control of collagen cleavage. Previously, it was reported that there is increased production of both TNF␣ and its converting enzyme, TACE, in human OA cartilage (41), combined with enhanced expression of signaltransducing TNFRI in isolated OA chondrocytes (42). Other candidates for TNF␣ blockade would be TACE inhibitors, anti-TNF␣ antibodies, sTNFRI, or sTNFRII. The ability of IL-1 or TNF␣ blockade to enhance expression of CII and aggrecan in cartilage from some patients and, in a few cases, to increase aggrecan content is of interest in view of the demonstrated inhibitory effects of these cytokines on the synthesis of these matrix molecules (1,6,43). These observations suggest that in some cases, these antagonists may also have the potential to promote cartilage repair. The reasons why in some patients, no responses were observed in the presence of either cytokine antagonist and why different results were obtained in different patients suggest that KOBAYASHI ET AL these contrasting responses may be due to differences in the pathobiology, which remain to be determined. It was, however, clearly apparent that by examining inhibition of degradation and GAG content increases in individual cases, there was no evidence for a consistent linkage between the effects on CII cleavage, proteoglycan release, and content. In conclusion, this is the first study to demonstrate that TNF␣ and IL-1 present in OA cartilage are involved in collagenase-mediated cleavage of CII, aggrecan degradation, and the inhibition of gene expression of matrix molecules. Although the ability of these antagonists to regulate this degradation varies considerably according to the patient, the group analyses suggest that PEGylated sTNFRI and/or IL-1Ra (anakinra) may offer opportunities to control cartilage damage in some patients with OA by inhibiting the degradation of extracellular matrix by suppressing the expression of MMP genes involved in cartilage degradation. This may help in cartilage repair. REFERENCES 1. Poole AR. Cartilage in health and disease. In: Koopman WJ, editor. Arthritis and allied conditions: a textbook of rheumatology. 14th ed. Philadelphia: Lippincott Williams & Wilkins; 2001. p. 226–84. 2. Kempson GE, Muir H, Pollard C, Tuke M. The tensile properties of the cartilage of human femoral condyles related to the content of collagen and glycosaminoglycans. Biochim Biophys Acta 1973; 297:456–72. 3. Dodge GR, Poole AR. Immunohistochemical detection and immunochemical analysis of type II collagen degradation in human normal, rheumatoid, and osteoarthritic articular cartilages and in explants of bovine articular cartilage cultured with interleukin 1. J Clin Invest 1989;83:647–61. 4. Hollander AP, Heathfield TF, Webber C, Iwata Y, Bourne R, Rorabeck C, et al. Increased damage to type II collagen in osteoarthritic articular cartilage detected by a new immunoassay. J Clin Invest 1994;93:1722–32. 5. Billinghurst RC, Dahlberg L, Ionescu M, Reiner A, Bourne R, Rorabeck C, et al. Enhanced cleavage of type II collagen by collagenases in osteoarthritic articular cartilage. J Clin Invest 1997;99:1534–45. 6. Poole AR, Howell DS. Etiopathogenesis of osteoarthritis. In: Moskowitz RW, Howell DS, Altman RD, Buckwalter JA, Goldberg VM, editors. Osteoarthritis: diagnosis/surgical management. 3rd ed. Philadelphia: WB Saunders; 2001. p. 29–47. 7. Dahlberg L, Billinghurst RC, Manner P, Nelson F, Webb G, Ionescu M, et al. Selective enhancement of collagenase-mediated cleavage of resident type II collagen in cultured osteoarthritic cartilage and arrest with a synthetic inhibitor that spares collagenase 1 (matrix metalloproteinase 1). Arthritis Rheum 2000;43: 673–82. 8. Rizkalla G, Reiner A, Bogoch E, Poole AR. Studies of the articular cartilage proteoglycan aggrecan in health and arthritis: evidence for molecular heterogeneity and extensive molecular changes in disease. J Clin Invest 1992;90:2268–77. 9. Poole AR, Rosenberg LC, Reiner A, Ionescu M, Bogoch E, Roughley PJ. Contents and distributions of the proteoglycans IL-1 AND TNF␣ IN CARTILAGE DEGRADATION decorin and biglycan in normal and osteoarthritic human articular cartilage. J Orthop Res 1996;14:681–9. 10. Hollander AP, Pidoux I, Reiner A, Rorabeck C, Bourne R, Poole AR. Damage to type II collagen in aging and osteoarthritis starts at the articular surface, originates around chondrocytes, and extends into the cartilage with progressive degeneration. J Clin Invest 1995;96:2859–69. 11. Poole AR, Alini M, Hollander AR. Cellular biology of cartilage degradation. In: Henderson B, Edwards JC, Pettipher ER, editors. Mechanisms and models in rheumatoid arthritis. London: Academic Press; 1997. p. 163–204. 12. Borden P, Solymar D, Sucharczuk A, Lindman B, Cannon P, Heller RA. Cytokine control of interstitial collagenase and collagenase-3 gene expression in human chondrocytes [published erratum in J Biol Chem 1996;271:33706]. J Biol Chem 1996;271: 23577–81. 13. Goldring MB. The role of the chondrocyte in osteoarthritis [review]. Arthritis Rheum 2000;43:1916–26. 14. Slack J, McMahan CJ, Waugh S, Schooley K, Spriggs MK, Sims JE, et al. Independent binding of interleukin-1␣ and interleukin-1 to type I and type II interleukin-1 receptors. J Biol Chem 1993;268:2513–24. 15. Loetscher H, Pan YC, Lahm HW, Gentz R, Brockhaus M, Tabuchi H, et al. Molecular cloning and expression of the human 55 kd tumor necrosis factor receptor. Cell 1990;61:351–9. 16. Schall TJ, Lewis M, Koller KJ, Lee A, Rice GC, Wong GH, et al. Molecular cloning and expression of a receptor for human tumor necrosis factor. Cell 1990;61:361–70. 17. Suda T, Takahashi T, Golstein P, Nagata S. Molecular cloning and expression of the Fas ligand, a novel member of the tumor necrosis factor family. Cell 1993;75:1169–78. 18. Webb GR, Westacott CI, Elson CJ. Chondrocyte tumor necrosis factor receptors and focal loss of cartilage in osteoarthritis. Osteoarthritis Cartilage 1997;5:427–37. 19. Seckinger P, Lowenthal JW, Williamson K, Dayer JM, MacDonald HR. A urine inhibitor of interleukin 1 activity that blocks ligand binding. J Immunol 1987;139:1546–9. 20. Hannum CH, Wilcox CJ, Arend WP, Joslin FG, Dripps DJ, Heimdal PL, et al. Interleukin-1 receptor antagonist activity of a human interleukin-1 inhibitor. Nature 1990;343:336–40. 21. Eisenberg SP, Evans RJ, Arend WP, Verderber E, Brewer MT, Hannum CH, et al. Primary structure and functional expression from complementary DNA of a human interleukin-1 receptor antagonist. Nature 1990;343:341–6. 22. Carter DB, Deibel MR Jr, Dunn CJ, Tomich CS, Laborde AL, Slightom JL, et al. Purification, cloning, expression and biological characterization of an interleukin-1 receptor antagonist protein. Nature 1990;344:633–8. 23. Horai R, Saijo S, Tanioka H, Nakae S, Sudo K, Okahara A, et al. Development of chronic inflammatory arthropathy resembling rheumatoid arthritis in interleukin 1 receptor antagonist-deficient mice. J Exp Med 2000;191:313–20. 24. Campion GV, Lebsack ME, Lookabaugh J, Gordon G, Catalano M, and the IL-1Ra Arthritis Study Group. Dose-range and dosefrequency study of recombinant human interleukin-1 receptor antagonist in patients with rheumatiod arthritis. Arthritis Rheum 1996;39:1092–101. 25. Fernandes J, Tardif G, Martel-Pelletier J, Lascau-Coman V, Dupuis M, Moldovan F, et al. In vivo transfer of interleukin-1 receptor antagonist gene in osteoarthritic rabbit knee joints: prevention of osteoarthritis progression. Am J Pathol 1999;154: 1159–69. 26. Higuchi M, Aggarwal BB. TNF induces internalization of the p60 receptor and shedding of the p80 receptor. J Immunol 1994;152: 3550–8. 135 27. Elliott MJ, Maini RN, Feldmann M, Long-Fox A, Charles P, Bijl H, et al. Repeated therapy with monoclonal antibody to tumour necrosis factor ␣ (cA2) in patients with rheumatoid arthritis. Lancet 1994;344:1125–7. 28. Moreland LW, Baumgartner SW, Schiff MH, Tindall EA, Fleischmann RM, Weaver AL, et al. Treatment of rheumatoid arthritis with a recombinant human tumor necrosis factor (p75)-Fc fusion protein. N Engl J Med 1997;337:141–7. 29. Caldwell JR, Davis MW, Jelaca-Maxwell K, Wang A, Wason S, Chase W, et al. A phase I study of pegylated tumor necrosis factor receptor type I (PEG sTNF-R1[p55]) in subjects with rheumatoid arthritis (RA) [abstract]. Arthritis Rheum 1999;42 Suppl 9:S236. 30. Nagase H. Matrix metalloproteinases. In: Hooper N, editor. Zinc metalloproteinases in health and disease. Bristol (UK): Taylor and Francis; 1996. p. 153–204. 31. Mitchell PG, Magna HA, Reeves LM, Lopresti-Morrow LL, Yocum SA, Rosner PJ, et al. Cloning, expression, and type II collagenolytic activity of matrix metalloproteinase-13 from human osteoarthritic cartilage. J Clin Invest 1996;97:761–8. 32. Shlopov BV, Lie WR, Mainardi CL, Cole AA, Chubinskaya S, Hasty KA. Osteoarthritic lesions: involvement of three different collagenases. Arthritis Rheum 1997;40:2065–74. 33. Lark MW, Bayne EK, Flanagan J, Harper CF, Hoerrner LA, Hutchinson NI, et al. Aggrecan degradation in human cartilage: evidence for both matrix metalloproteinase and aggrecanase activity in normal, osteoarthritic, and rheumatoid joints. J Clin Invest 1997;100:93–106. 34. Mort JS, Poole AR. Mediators of inflammation: tissue destruction and repair. D. Proteinases and their inhibitors. In: Klippel JL, Crofford LJ, Stone JH, Weyand CM, editors. Primer on the rheumatic diseases. 12th ed. Atlanta: Arthritis Foundation; 2001. p. 72–81. 35. Altman R, Asch E, Bloch D, Bole G, Borenstein D, Brandt K, et al. Development of criteria for the classification and reporting of osteoarthritis: classification of osteoarthritis of the knee. Arthritis Rheum 1986;29:1039–49. 36. Billinghurst RC, Wu W, Ionescu M, Reiner A, Dahlberg L, Chen J, et al. Comparison of the degradation of type II collagen and proteoglycan in nasal and articular cartilages induced by interleukin-1 and the selective inhibition of type II collagen cleavage by collagenase. Arthritis Rheum 2000;43:664–72. 37. Farndale RW, Buttle DJ, Barrett AJ. Improved quantitation and discrimination of sulphated glycosaminoglycans by use of dimethylmethylene blue. Biochim Biophys Acta 1986;883:173–7. 38. Chomczynski P, Sacchi N. Single-step method of RNA isolation by acid guanidinium thiocyanate-phenol-chloroform extraction. Anal Biochem 1987;162:156–9. 39. Tchetina E, Mwale F, Poole AR. Distinct phases of coordinated early and late gene expression in growth plate chondrocytes in relationship to cell proliferation, matrix assembly, remodeling and cell differentiation. J Bone Miner Res 2003;18:844–51. 40. Attur MG, Dave M, Cipolletta C, Kang P, Goldring MB, Patel IR, et al. Reversal of autocrine and paracrine effects of interleukin 1 (IL-1) in human arthritis by type II IL-1 decoy receptor: potential for pharmacological intervention. J Biol Chem 2000;275:40307–15. 41. Amin AR. Regulation of tumor necrosis factor-␣ and tumor necrosis factor converting enzyme in human osteoarthritis. Osteoarthritis Cartilage 1999;7:392–4. 42. Westacott CI, Atkins RM, Dieppe PA, Elson CJ. Tumor necrosis factor-␣ receptor expression on chondrocytes isolated from human articular cartilage. J Rheumatol 1994;21:1710–5. 43. Goldring MB, Birkhead J, Sandell LJ, Kimura T, Krane SM. Interleukin 1 suppresses expression of cartilage-specific type II and IX collagens and increases type I and III collagens in human chondrocytes. J Clin Invest 1988;82:2026–37.