Abstracts
[2576] Figure 3. Terminal ileum biopsy showing small bowel mucosa with chronic active inflammation, crypt architectural distortion, colonic crypts containing eosinophils and neutrophils.
[2577]
Figure 3. Push enteroscopy identifying an oozing mass, found in the jejunum, that was
consistent with peritoneal mesothelioma.
[2577] Figure 1. CT displaying a lymph node inseparable from a loop of proximal small bowel
measuring 7.3 3 2.4 cm; correlating with an intensely FDG avid lymph node on PET/CT in image
2.
[2578]
[2577]
Figure 2. PET/CT showing FDG avidity of the small bowel.
2578
Meckel’s Diverticulum: A Diverticulum Like No Other
Mira Alsheikh, MD1, Fady Haddad, MD2, Stephen Mulrooney, MD3.
1
2
Staten Island University Hospital, Staten Island, NY; Northwell Health Staten Island University
3
Hospital, Staten Island, NY; Staten Island University Hospital, Northwell Health, Staten Island, NY.
INTRODUCTION: Meckel’s diverticulum (MD) is a relatively uncommon cause of gastrointestinal
(GI) bleeding in adults. “Often looked for and seldom found,” MD is challenging to diagnose despite
the various imaging modalities available. Herein, we present the case of a young man who presented
with lower GI hemorrhage and negative endoscopy, bleeding scan, and angiography. Meckel’s diverticulum was later diagnosed via scintigraphy scan. We review the noninvasive diagnostic imaging
for Meckel’s diverticulum, mainly technetium-99m (Tc 99m) pertechnetate scan, and bleeding scan.
© 2019 by The American College of Gastroenterology
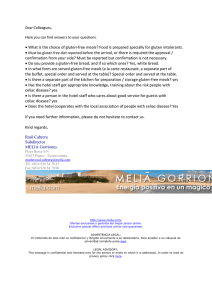
Figure 1. Meckel’s diverticulum, macroscopic view.
CASE DESCRIPTION/METHODS: A 26-year-old man presented with multiple episodes of
melena. He had acute onset anemia. Workup, including upper endoscopy, colonoscopy, and push
enteroscopy were not able to identify the site of bleeding even after repeat procedures. A computed
tomography scan with intravenous contrast and mesenteric angiography were also unrevealing. A
Technetium 99m bleeding scan was read as negative. Persistent bleeding necessitated recurrent
transfusions. Capsule endoscopy was deployed. A Meckel’s scan (Tc 99m Pertechnetate scan)
revealed an abnormal focus of uptake in the right lower abdomen suggesting the diagnosis of
Meckel’s diverticulum. The patient underwent laparoscopic resection of the diverticulum and was
discharged home (Figures 1 and 2). A retrospective review of the bleeding scan revealed isolated
uptake in the location of the Meckel’s Diverticulum. Review of the capsule endoscopy revealed
a diverticulum in the small bowel in the right lower quadrant without active bleeding (Figure 3).
DISCUSSION: Bleeding Meckel’s diverticulum is easier to diagnose than MD presenting with other
symptoms, but still an outstanding challenge. High suspicion for MD should be sought in the
evaluation of a young patient presenting with GI bleeding; the gold standard for diagnosis is the
technetium-99m pertechnetate scan or so-called Meckel’s scan. Bleeding scan is another noninvasive
imaging modality that helps to detect a bleeding MD. Although both scans use Tc 99m, the
mechanism is different. Meckel’s scan uses Tc 99m, which is secreted by parietal cells in the mucus,
thus detecting gastric cells within MD. On the other hand, the bleeding scan works via identifying Tc
99m that is bound to hemoglobin, therefore identifying a bleeding MD. Both scans are noninvasive
and safe. The use of either one should be tailored according to the clinical presentation.
The American Journal of GASTROENTEROLOGY
Copyright © 2019 by The American College of Gastroenterology. Unauthorized reproduction of this article is prohibited.
S1417
S1418
Abstracts
decreasing the absorption of fat-soluble vitamins K & Vitamin D. The parathyroids release more PTH
in an attempt to maintain serum calcium levels through increasing osteoclastic activity. Other
mechanisms active in celiac disease also increases bone resorption (See Figure 2). Bisphosphonates
are a standard treatment for preventing osteoporotic fractures, by reducing osteoclastic activity. In
this patient with active celiac disease, with low availability of dietary calcium, this resulted in hypocalcemia. This can be mitigated with closer observation and adjustment of doses of vitamin D and
calcium supplementation when administering bisphosphonates.
2580
Nothing but NET: A Case of Neuroendocrine Tumor in the Duodenal Bulb
Michelle Baliss, DO1, Mohammad Bilal, MD1, Sheharyar Merwat, MD2.
2
The University of Texas Medical Branch, Galveston, TX; University of Texas Medical Branch,
Galveston, TX.
1
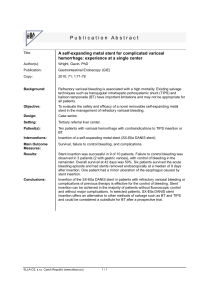
[2578] Figure 2. Microscopic examination with hematoxylin-eosin stain shows the margin of
Meckel’s diverticulum with the normal intestinal mucosa. Notice the ectopic gastric mucosa with
mucous and parietal cells.
INTRODUCTION: Neuroendocrine tumors (NETs) are rare neoplasms that comprise approximately 2% of all malignant tumors in the gastrointestinal system. The ileum remains the most
common site of NETs in the small intestine, making up .70% of small bowel NETs. Duodenal NETs
are exceedingly rare, comprising 2-3% of all gastrointestinal NETs and 1-3% of all duodenal tumors.
We present a rare case of a patient diagnosed with a duodenal bulb NET.
CASE DESCRIPTION/METHODS: A 66-year-old male with a past history of gastroesophageal
reflux disease and hypertension presented to the gastroenterology clinic with a chief complaint of
intermittent halitosis for the past year. The symptoms were unrelated to food intake. His recent
dental examination was normal. He did not have a family history of gastrointestinal malignancies.
His physical examination was unremarkable. Laboratory data including Helicobacter pylori antigen
was unremarkable. He underwent esophagogastroduodenoscopy which demonstrated a 15 mm
nodule in the duodenal bulb (Figure 1). Histopathological examination of the nodule showed a welldifferentiated neuroendocrine tumor. Neuroendocrine immunohistochemical stains were positive for
chromogranin and synaptophysin. Ki-67 was positive in 1% of tumor cells. CT scan of the abdomen
revealed a 1.2 3 0.8 3 0.7 cm well-defined hyperattenuating structure in the posterior wall of the
duodenal bulb (Figure 2). On endoscopic ultrasound, the lesion appeared to be located within the
deep mucosa and submucosa without invasion of adjacent structures (Figure 3). The patient has been
referred to medical oncology.
DISCUSSION: The duodenum is an uncommon location for NETs. Duodenal NETs are typically
small, single-lesion neoplasms, the majority of which are non-functional and diagnosed during
the 6th decade of life. Unlike NETs of the jejunum and ileum that lack a gender preference,
duodenal NETs carry a slight male predominance. Metastasis to regional lymph nodes is seen in
;60% of cases and to the liver in less than 10% of cases. The absence of neuroendocrine clinical
syndromes in .90% of duodenal NETs coupled with the rarity of this malignancy creates
a noteworthy diagnostic challenge. It is therefore not surprising that the majority of these cases
are diagnosed incidentally during work-up for other symptoms. With a rising annual incidence of
NETs, it is important for gastroenterologists to keep this diagnosis in mind as a differential for any
nodule in the duodenum.
2581
Acute Lymphoblastic Leukemia Presenting With Mesenteric Ischemia
[2578]
Figure 3. Videocapsule endoscopy: Meckel diverticulum.
2579
Calcium Disorders in Celiac Disease
Usman Naseer, MBBS1, Ali Wazir, MBBS1, Raina A. Patel, MD2, Haider Rahman, MD1,
Jae Chung, DO1, Mackenzie LaPorte, MBA, BS3, Elise Malecki, MD, PhD3.
1
2
3
Albany Medical Center, Albany, NY; Stratton Veteran Affairs Medical Center, Albany, NY; Albany
Medical College, Albany, NY.
INTRODUCTION: Celiac disease is known to affect calcium homeostasis in various ways leading to
osteoporosis and osteopenia. We present a case of active celiac disease complicated by hypocalcemia
and osteoporosis.
CASE DESCRIPTION/METHODS: The patient is a 74-year-old male with known Celiac disease
diagnosed 25 years ago. He had known hypocalcemia with secondary hyperparathyroidism treated
with calcium and calcitriol supplements to maintain calcium levels (Corrected Calcium: 8.5 mg/dl
with PTH of 89 pg/ml and 25-hydroxy Vitamin D of 80 ng/ml). The patient had a mechanical fall,
a few months ago and subsequent DEXA scan showed osteoporosis (Bone mineral density of L1-L4
vertebral bodies was 3.5 standard deviation below normal). The patient was treated with an infusion
of zoledronic acid. A week later the patient presented with malabsorptive diarrhea likely due to
reported non-compliance with a gluten-free diet. On admission labs, he was noted to have severe
hypocalcemia (ionized 0.8, corrected calcium was 6.7). Of note, his PTH had increased to 385.
Incidentally, his INR was also noted to be mildly elevated at 1.5. Despite this, he had no apparent
symptoms of hypocalcemia. During the admission, the patient had an EGD and biopsies were done
showing mucosal changes consistent with celiac disease confirming dietary non-adherence. Hypocalcemia was treated with IV infusion of Calcium and he was discharged on increased doses of
Calcitriol and calcium supplements with close follow-up with endocrinology.
DISCUSSION: Celiac disease affects the small intestine including duodenum, the primary site of
absorption of divalent ions including calcium. The intraluminal dietary fats bind to this calcium
The American Journal of GASTROENTEROLOGY
Michelle Baliss, DO1, Timothy Krill, MD1, Hamza Abdulla, MD1, Sreeram Parupudi, MD, FACG2.
1
2
The University of Texas Medical Branch, Galveston, TX; University of Texas Medical Branch,
Galveston, TX.
INTRODUCTION: Acute lymphoblastic leukemia (ALL) is a malignancy of B/T-cell lymphoid
precursors that predominantly affects the pediatric population. Presenting symptoms are usually
related to bone marrow and organ infiltration. Arterial thrombosis is extremely rare and seldom seen
as a presenting manifestation of acute leukemia. To our knowledge, we present the first case of
mesenteric ischemia due to complete occlusion of the superior mesenteric artery (SMA) as the first
manifestation of T-cell ALL.
CASE DESCRIPTION/METHODS: A 44-year-old male presented with severe upper abdominal
pain, vomiting and diarrhea for 1 day. Physical examination was notable for diffuse abdominal
tenderness and pain out of proportion to exam. Initial laboratory data showed WBC of 2.02 3
103/mL with 30% blasts. Lactic acid was within normal limits. CT of the abdomen revealed
a thrombus in the SMA resulting in complete occlusion (Figure 1). An emergent open SMA
thrombectomy was performed following failure of catheter-directed thrombolysis. Diffuse ischemic changes were visualized in the jejunum necessitating a partial small bowel resection
(Figure 2). Intraoperative transesophageal echocardiogram was negative for intracardiac thrombus or valvular pathology. A peripheral blood smear revealed a large population of immature cells
with fine chromatin and a high nuclear to cytoplasmic ratio (Figure 3). Flow cytometry showed
a large population of blasts constituting about 22% of cells, positive for CD5, CD7, and CD10. The
immunophenotypic appearance confirmed the diagnosis of T-ALL. He was referred to medical
oncology for bone marrow biopsy.
DISCUSSION: This is the first reported case of acute arterial occlusion in the SMA leading to
mesenteric ischemia as the initial manifestation of T-cell ALL. SMA thromboembolism typically
occurs in the setting of atherosclerosis or cardiac pathology, which were absent in this case.
Venous thromboembolism is a well-documented complication of acute leukemia that negatively
impacts mortality. The inhibition of anticoagulant proteins, production of prothrombotic factors,
alteration of the vascular endothelium, and increased vascular adhesion of leukemic cells are all
potential contributors. However, arterial occlusion is extremely unusual and almost exclusively
seen in acute promyelocytic leukemia (APL). This report illustrates that an unexplained arterial or
venous thrombotic event in a previously healthy patient could be a sign of an underlying
malignancy.
VOLUME 00 | SUPPLEMENT | MONTH 2019 www.amjgastro.com
Copyright © 2019 by The American College of Gastroenterology. Unauthorized reproduction of this article is prohibited.
 0
0