MIE vs. Open Esophagectomy for Esophageal Cancer: A Population Study
Anuncio

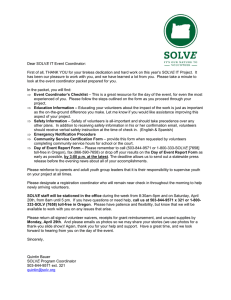
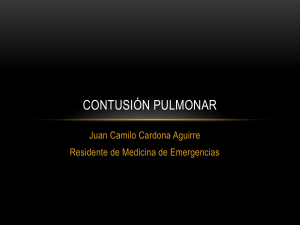
Minimally Invasive Versus Open Esophagectomy for Esophageal Cancer: A Population-Based Analysis Babatunde A. Yerokun, MD, Zhifei Sun, MD, Chi-Fu Jeffrey Yang, MD, Brian C. Gulack, MD, Paul J. Speicher, MD, Mohamed A. Adam, MD, Thomas A. D’Amico, MD, Mark W. Onaitis, MD, David H. Harpole, MD, Mark F. Berry, MD, and Matthew G. Hartwig, MD Department of Surgery, Duke University Medical Center, Durham, North Carolina; Department of Surgery, Division of Cardiovascular and Thoracic Surgery, Duke University Medical Center, Durham, North Carolina; and Department of Cardiothoracic Surgery, Stanford University, Stanford, California Background. The objective of this study was to evaluate outcomes of minimally invasive approaches to esophagectomy using population-level data. Methods. Multivariable regression modeling was used to determine predictors associated with the use of minimally invasive approaches for patients in the National Cancer Data Base who underwent resection of middle and distal clinical T13N03M0 esophageal cancers from 2010 to 2012. Perioperative outcomes and 3-year survival were compared between propensitymatched groups of patients with esophageal cancer who underwent minimally invasive esophagectomy (MIE) or open esophagectomy (OE). A subgroup analysis was performed to evaluate the impact of using robotic-assisted operations as part of the minimally invasive approach. Results. Among 4,266 patients included, 1,308 (30.6%) underwent MIE. It was more likely to be used in patients treated at academic (adjusted odds ratio [OR], 10.1; 95% confidence interval [CI], 4.2–33.1) or comprehensive cancer facilities (adjusted OR, 6.4; 95% CI, 2.6–21.1). Compared with propensity-matched patients who underwent OE, patients who underwent MIE had significantly more lymph nodes examined (15 versus 13; p [ 0.016) and shorter hospital lengths of stay (10 days versus 11 days; p [ 0.046) but similar resection margin positivity, readmission, and 30-day mortality (all p > 0.05). Survival was similar between the matched groups at 3 years for both adenocarcinoma and squamous cell carcinoma (p > 0.05). Compared with MIE without robotic assistance, use of a robotic approach was not associated with any significant differences in perioperative outcomes (p > 0.05). Conclusions. The use of minimally invasive techniques to perform esophagectomy for esophageal cancer is associated with modestly improved perioperative outcomes without compromising survival. O the technical difficulties encountered in laparoscopic resections, but data comparing RAMIE versus standard MIE without robotic assistance (SMIE) are lacking. The only study comparing RAMIE versus SMIE found no differences in operative time, blood loss, number of resected lymph nodes, postoperative complications, days of mechanical ventilation, length of intensive care unit stay, or length of hospital stay [4]. Despite the ongoing adoption of MIE, data regarding the oncologic acceptability of using a minimally invasive approach in esophageal cancer is extremely limited. Most comparative effectiveness studies are single highvolume institutional experiences that lack generalizability [5–8]. The Traditional Invasive Versus Minimally Invasive Esophagectomy (TIME) trial is the only ver the past decade, minimally invasive esophagectomy (MIE) has been used increasingly for the treatment of esophageal cancer [1]. Currently, MIE can be performed through the laparoscopic transhiatal, the laparoscopic-thoracoscopic McKeown, or the laparoscopicthoracoscopic Ivor Lewis approach [2]. Although there are differences in the specific operative approach, supporters of MIE have cited reduced perioperative morbidity, shortened hospital stay, and improved patient satisfaction when compared with traditional open esophagectomy (OE) [3]. More recently, robotic-assisted minimally invasive esophagectomy (RAMIE) has been introduced to address Accepted for publication Feb 16, 2016. Presented at the Forty-first Annual Meeting of the Western Thoracic Surgery Association, Whistler, British Columbia, Canada, June 24– 27, 2015. Address correspondence to Dr Hartwig, Duke University Medical Center, Box 3863, Durham, NC 27710; email: [email protected]. Ó 2016 by The Society of Thoracic Surgeons Published by Elsevier (Ann Thorac Surg 2016;-:-–-) Ó 2016 by The Society of Thoracic Surgeons Dr D’Amico discloses a financial relationship with Scanlan. 0003-4975/$36.00 http://dx.doi.org/10.1016/j.athoracsur.2016.02.078 2 YEROKUN ET AL MIE VERSUS OE FOR ESOPHAGEAL CANCER Abbreviations and Acronyms CI MIE OE RAMIE SMIE = = = = confidence interval minimally invasive esophagectomy open esophagectomy robotic assisted minimally invasive esophagectomy = standard minimally invasive esophagectomy without robotic assistance multicenter randomized study comparing open esophagectomy versus MIE, but it lacks power to detect any oncologic difference [9]. Moreover, although 1 population study analyzed short-term outcomes between MIE and OE in the United Kingdom [10], no study to date has examined survival differences between MIE and OE on a national level in the United States. Therefore the purpose of this study was to compare perioperative outcomes and survival in patients who underwent MIE versus traditional OE using population-level data. Furthermore, we aimed to assess any differences in using a robotic-assisted minimally invasive approach over the standard MIE approach. The primary hypothesis was that surgical approach would not be associated with perioperative outcomes or 3-year survival. Patients and Methods The Duke University Institutional Review Board approved this retrospective review of the National Cancer Data Base. The National Cancer Data Base is jointly administered by the American College of Surgeons and the American Cancer Society and collects data from greater than 1,500 cancer institutions. The database currently contains records of 30 million patient records and approximately 70% of newly diagnosed cancer cases in the United States. Patients with clinical T1-3any NM0 esophageal cancers located in the middle and distal esophagus who underwent esophagectomy from 2010 to 2012 were included in the study. MIE was defined by intent-to-treat criteria as any operation involving either thoracoscopy or laparoscopy, including any hybrid or robotic-assisted approach. Patients with nonmalignant pathologic conditions or missing surgical approach data were excluded. The primary end point of our study was 3-year survival. Secondary end points included positive surgical margins, lymph nodes examined, hospital length of stay, 30-day unplanned readmissions, 30-day mortality, and adjuvant therapy use. Baseline characteristics between all cases of OE and MIE were compared using the Kruskal-Wallis and Pearson’s c2 tests for continuous variable and categorical variables, respectively. Multivariable logistic regression models were developed to identify factors independently associated with the use of OE versus MIE; a backward variable elimination method was used to produce the Ann Thorac Surg 2016;-:-–- most parsimonious model based on the lowest Akaike information criterion. To adjust for potential selection bias between the comparison of OE and MIE, we developed propensity scores, defined as the conditional probability of undergoing MIE. Patients were matched using a 1:1 nearest-neighbor algorithm, using the following variables: age, sex, race, insurance status, Charlson-Deyo comorbidity score, treatment facility type (community, comprehensive, or academic), location of the primary lesion (middle or lower third of the esophagus), American Joint Committee on Cancer clinical T and N stages, tumor size, and use of simultaneous neoadjuvant chemotherapy and radiotherapy. Outcomes were compared in propensity-matched groups. Survival was plotted using the Kaplan-Meier method. To assess the effect of robotic assistance in MIE, a subgroup analysis was performed in a similar fashion comparing RAMIE versus SMIE. This method was repeated for both adenocarcinoma and squamous cell carcinoma. For all analyses, p values less than 0.05 were considered to indicate statistical significance. All analyses were performed using R, version 3.0.1 (The R Foundation for Statistical Computing, Vienna, Austria). Results Among 4,266 total patients identified, 2,958 (69.3%) underwent OE, whereas 1,308 (30.7%) underwent MIE. Among patients who received MIE, 231 (17.6%) underwent RAMIE. Unadjusted baseline characteristics of patients who underwent OE and MIE are shown in Table 1. Patients who underwent MIE were more likely to be treated at an academic facility (p < 0.001), to have a lower clinical T stage (p ¼ 0.029), to have a lower pathologic T stage (p ¼ 0.041), and to have a smaller tumor size (p ¼ 0.007) when compared with patients undergoing OE. Conversion to an open procedure within the entire MIE group was 11.6%. The use of MIE increased from 27.1% in 2010 to 37.5% in 2012. The median number of esophagectomies per center was 2. After accounting for patient, tumor, and hospital factors, we found that treatment at either a comprehensive facility (odds ratio [OR], 7.32, 95% confidence interval [CI], 2.28–23.47; p ¼ 0.001) or an academic facility (OR, 11.24; 95% CI, 3.52–35.90; p < 0.001) was predictive of a patient undergoing MIE (Fig 1). Independent predictors of OE included the presence of a clinical stage T2 tumor (OR, 0.74; 95% CI, 0.58–0.96; p ¼ 0.023) or a clinical stage T3 tumor (OR, 0.72; 95% CI, 0.56–0.93; p ¼ 0.011), when compared with clinical stage T1 disease (Fig 1). After propensity matching, no substantial differences in covariates remained between groups (Table 2). Within matched groups, we found that margin positivity, unplanned readmission, and 30-day mortality rates were not significantly different between OE and MIE groups (all p > 0.05). However, the MIE group was associated with a higher number of lymph nodes harvested (15 versus 13; p ¼ 0.016) and a modest decrease in hospital length of stay (10 days versus 11 days; p ¼ 0.046) (Table 3). Ann Thorac Surg 2016;-:-–- 3 YEROKUN ET AL MIE VERSUS OE FOR ESOPHAGEAL CANCER Table 1. Baseline Characteristics of OE Versus MIE and SMIE Versus RAMIE Groups Variable Age (y) Sex Male Female Race White Black Other Insurance status None Private Government Charlson-Deyo comorbidity index 0 1 2 Year of diagnosis 2010 2011 2012 Hospital location Northeast Midwest South West Facility type Community Comprehensive Academic Primary tumor site Lower third of esophagus Middle third of esophagus Histologic type Squamous cell Adenocarcinoma Clinical T stage T1 T2 T3 Clinical N stage N0 N1 N2 N3 Pathologic T stage T0/in situ T1 T2 T3 T4 OE (n ¼ 2,958) MIE (n ¼ 1,308) 57/64/70 57/64/70 83.6% (2,474) 16.4% (484) 84.1% (1,100) 15.9% (208) 93.7% (2,741) 4.5% (131) 1.8% (54) 94.8% (1,233) 3.8% (50) 1.3% (17) 2.0% (59) 45.0% (1,301) 53.0% (1,533) 1.9% (25) 47.9% (619) 50.2% (649) 70.7% (2,090) 23.3% (690) 6.0% (178) 70.9% (927) 23.5% (308) 5.6% (73) 35.6% (1,054) 32.3% (954) 32.1% (950) 27.1% (354) 35.4% (463) 37.5% (491) 20.6% 34.3% 32.9% 12.2% 28.2% 25.4% 30.5% 15.9% p Value 0.596 0.707 SMIE (n ¼ 1077) RAMIE (n ¼ 231) 57/64/70 56/64/70 84.0% (905) 16.0% (172) 84.4% (195) 15.6% (36) 95.1% (1019) 3.7% (40) 1.1% (12) 93.4% (214) 4.4% (10) 2.2% (5) 1.9% (20) 47.8% (509) 50.3% (535) 2.2% (5) 48.0% (110) 49.8% (114) 70.3% (757) 24.0% (258) 5.8% (62) 73.6% (170) 21.6% (50) 4.8% (11) 29.4% (317) 35.3% (380) 35.3% (380) 16.0% (37) 35.9% (83) 48.1% (111) 29.9% 25.3% 27.5% 17.3% 20.3% 25.5% 44.6% 9.5% 0.284 0.951 0.853 0.588 <0.001 <0.001 <0.001 (369) (332) (399) (208) <0.001 (322) (273) (296) (186) (47) (59) (103) (22) <0.001 2.7% (81) 35.3% (1,041) 61.9% (1,825) 0.3% (4) 26.5% (347) 73.2% (957) 89.0% (2,634) 11.0% (324) 89.2% (1,167) 10.8% (141) 22.1% (653) 77.9% (2,305) 20.0% (261) 80.0% (1,047) 11.4% (299) 25.7% (673) 62.9% (1,645) 14.5% (167) 25.6% (296) 59.9% (692) 51.0% 39.1% 8.5% 1.4% (1,492) (1,145) (248) (42) 52.6% 40.1% 6.4% 0.9% (680) (519) (83) (12) 18.9% 31.1% 17.0% 32.6% 0.5% (494) (812) (443) (852) (12) 20.3% 34.9% 14.9% 29.3% 0.6% (246) (422) (180) (354) (7) 0.649 0.884 0.39 0.22 (608) (1,016) (974) (360) p Value 0.148 0.4% (4) 27.5% (296) 72.1% (777) 0.0% (0) 22.1% (51) 77.9% (180) 88.9% (957) 11.1% (120) 90.9% (210) 9.1% (21) 20.1% (216) 79.9% (861) 19.5% (45) 80.5% (186) 14.1% (132) 26.5% (248) 59.4% (555) 15.9% (35) 21.8% (48) 62.3% (137) 53.0% 40.2% 6.1% 0.8% (564) (428) (65) (8) 50.7% 39.7% 7.9% 1.7% (116) (91) (18) (4) 19.6% 35.4% 15.1% 29.4% 0.6% (194) (350) (149) (291) (6) 23.7% 32.9% 14.2% 28.8% 0.5% (52) (72) (31) (63) (1) 0.867 0.362 0.119 0.843 0.029 0.335 0.063 0.373 0.041 0.732 (Continued) 4 YEROKUN ET AL MIE VERSUS OE FOR ESOPHAGEAL CANCER Ann Thorac Surg 2016;-:-–- Table 1. Continued Variable Pathologic N stage N0 N1 N2 N3 Pathologic M stage M0 M1 Tumor size (mm) Neoadjuvant chemoradiotherapy Conversion to open operation OE (n ¼ 2,958) MIE (n ¼ 1,308) p Value SMIE (n ¼ 1077) RAMIE (n ¼ 231) 0.874 67.1% 20.8% 8.4% 3.7% (1,774) (549) (223) (97) 66.6% 20.3% 9.1% 3.9% (812) (248) (111) (48) 0.778 66.3% 20.2% 9.5% 4.0% (664) (202) (95) (40) 67.9% 21.1% 7.3% 3.7% (148) (46) (16) (8) 0.111 99.3% (2,937) 0.7% (21) 20/35/50 62.3% (1,837) ... 99.7% (1,304) 0.3% (4) 19/30/50 61.3% (800) 11.6% (152) 0.007 0.504 ... p Value 0.354 99.6% (1,073) 0.4% (4) 19/30/50 59.8% (643) 13.0% (139) 100.0% (231) 0.0% (0) 20/30/50 68.0% (157) 12.1% (28) 0.657 0.021 0.727 Data are represented as percent (n) for categorical variables and Q1/median/Q3 for continuous variables unless otherwise specified. MIE ¼ minimally invasive esophagectomy; OE ¼ open esophagectomy; Q1 ¼ first quartile; minimally invasive esophagectomy; SMIE ¼ standard minimally invasive esophagectomy. When stratified by histologic type, 3-year survival was similar between OE and MIE. For patients with adenocarcinoma, 3-year survival was 49.4% versus 56.7% for OE and MIE, respectively (p ¼ 0.206) (Fig 2A). For patients with squamous cell carcinoma, 3-year survival was 56.3% versus 54.7% for OE and MIE, respectively (p ¼ 0.870) (Fig 2C). Robotic Versus Standard MIE Subgroup Analysis When comparing MIE performed with or without robotic assistance, patients treated with robotic MIE were more likely to have received neoadjuvant chemoradiotherapy (68.0% versus 59.8%; p ¼ 0.021) but otherwise were not significantly different, including the rate of conversion to open operations (Table 1). After propensity matching, no substantial differences remained between the 2 groups, likely meaning that these differences were center specific (Table 2). Within matched groups, we found no differences between RAMIE and SMIE in Fig 1. Forest plot of factors associated with use of minimally invasive esophagectomy (MIE). Black squares represent odds ratios for the independent association of each factor with using MIE; 95% confidence interval bounds are represented by the corresponding horizontal lines. Factors to the right of the vertical line at 1.0 are independently associated with using MIE. Patients receiving care at an academic or comprehensive institution are associated with use of minimally invasive esophagectomies, whereas patients with cT2 and cT3 tumors were associated with use of open esophagectomy (OE). Q3 ¼ third quartile; RAMIE ¼ robotic-assisted positive resection margin, lymph nodes harvested, hospital length of stay, 30-day readmission, or 30-day mortality (all p > 0.05) (Table 3). After stratification by histologic type, there were no significant differences in 3-year survival between SMIE and RAMIE for patients with adenocarcinoma (p ¼ 0.783) (Fig 2B). However, patients with squamous cell carcinoma who underwent RAMIE had statistically superior survival (84% versus 56% at 2 years; p ¼ 0.034) (Fig 2D). Comment In this population-level analysis of a minimally invasive approach to esophagectomy for esophageal cancer, we observed significantly higher odds of MIE use in academic centers, suggesting that adoption of MIE remains predominantly confined to academic and teaching institutions in the United States. Additionally, MIE is associated with modest improvements in lymph node Ann Thorac Surg 2016;-:-–- 5 YEROKUN ET AL MIE VERSUS OE FOR ESOPHAGEAL CANCER Table 2. Baseline Characteristics of OE Versus MIE and Laparoscopic Versus RAMIE Groups After Propensity Matching Variable Age (y) Sex Male Female Race White Black Other Charlson-Deyo comorbidity index 0 1 2 Facility type Community Comprehensive Academic Tumor size (mm) Clinical T stage T1 T2 T3 Clinical N stage N0 N1 N2 N3 Primary tumor site Lower third of esophagus Middle third of esophagus Neoadjuvant chemoradiotherapy OE (n ¼ 928) MIE (n ¼ 928) StDiff SMIE (n ¼ 170) RAMIE (n ¼ 170) StDiff 57/64/71 57/64/70 0.9% 56/63/69 56/64/70 8.9% 84.3% (782) 15.7% (146) 83.5% (775) 16.5% (153) 2.0% 2.0% 84.1% (143) 15.9% (27) 83.5% (142) 16.5% (28) 1.6% 1.6% 94.0% (872) 4.4% (41) 1.6% (15) 94.0% (872) 4.7% (44) 1.3% (12) 0 1.5% 2.9% 89.4% (152) 7.6% (13) 2.9% (5) 91.2% (155) 5.9% (10) 2.9% (5) 6.9% 7.5% 0 72.7% (675) 22.4% (208) 4.8% (45) 72.4% (672) 22.8% (212) 4.7% (44) 0.8% 1.0% 0.5% 75.3% (128) 19.4% (33) 5.3% (9) 75.9% (129) 20.0% (34) 4.1% (7) 1.5% 1.5% 5.9% 0.2% (2) 26.8% (249) 73.0% (677) 20/35/50 0.2% (2) 26.8% (249) 73.0% (677) 20/35/50 0 0 0 2.6% 0.0% (0) 22.9% (39) 77.1% (131) 22.5/35.0/50.0 0.0% (0) 22.9% (39) 77.1% (131) 20.0/35.0/50.0 0 0 0 3.2% 16.4% (152) 25.1% (233) 58.5% (543) 15.7% (146) 26.1% (242) 58.2% (540) 1.6% 2.2% 0.7% 14.1% (24) 25.9% (44) 60.0% (102) 16.5% (28) 22.9% (39) 60.6% (103) 5.6% 7.0% 1.2% 51.5% 41.7% 6.1% 0.6% 50.1% 42.5% 6.8% 0.6% (465) (394) (63) (6) 2.9% 1.5% 2.6% 0 51.2% 40.0% 8.2% 0.6% 50.6% 40.6% 8.2% 0.6% 1.2% 1.2% 0 0 90.5% (840) 9.5% (88) 63.7% (591) 4.4% 4.4% 1.6% 94.1% (160) 5.9% (10) 70.6% (120) (478) (387) (57) (6) 89.2% (828) 10.8% (100) 62.9% (584) (87) (68) (14) (1) (86) (69) (14) (1) 91.8% (156) 8.2% (14) 70.6% (120) 8.5% 8.5% 0 Data are represented as percent (n) for categorical variables and Q1/median/Q3 for continuous variables unless otherwise specified. Groups with standardized differences (StDiff) less than 10% were considered similar. MIE ¼ minimally invasive esophagectomy; OE ¼ open esophagectomy; Q1 ¼ first quartile; minimally invasive esophagectomy; SMIE ¼ standard minimally invasive esophagectomy. harvesting and hospital length of stay without compromising long-term survival. Finally, robotic assistance is not associated with improved perioperative outcomes over standard minimally invasive methods. Regarding MIE, the current literature highlights outcomes when confined to high-volume experienced Q3 ¼ third quartile; RAMIE ¼ robotic-assisted surgeons and establishes the efficacy of MIE in the management of esophageal pathologic conditions. However, our study attempts to establish the present-day application of MIE and determine how effectively it is being used. In the setting of academic institutions, Parameswaran and colleagues [11] and Schoppmann and Table 3. Study Outcomes in Propensity-Matched OE Versus MIE and Laparoscopic Versus RAMIE Groups Outcomes Positive resection margin Lymph nodes harvested (number) Hospital length of stay (d) 30-d readmission 30-d mortality rate OE (n ¼ 928) MIE (n ¼ 928) p Value SMIE (n ¼ 170) RAMIE (n ¼ 170) p Value 5.5% (50) 8/13/20 8/11/16 6.7% (62) 3.7% (23) 7.0% (65) 9/15/21 8/10/14 7.0% (65) 3.0% (17) 0.176 0.016 0.046 0.792 0.497 4.1% (7) 11/16/22 8/10/13 8.9% (15) 2.7% (3) 6.5% (11) 11/16/21 8/10/14 5.9% (10) 3.7% (3) 0.333 0.954 0.835 0.292 0.677 Matched variables included age, sex, race, insurance status, Charlson-Deyo comorbidity score, treatment facility type, location of the primary tumor, histologic type, American Joint Committee on Cancer clinical stage, tumor size, and use of neoadjuvant chemoradiotherapy. Data are represented as percent (n) for categorical variables and Q1/median/Q3 for continuous variables unless otherwise specified. MIE ¼ minimally invasive esophagectomy; OE ¼ open esophagectomy; Q1 ¼ first quartile; minimally invasive esophagectomy; SMIE ¼ standard minimally invasive esophagectomy. Q3 ¼ third quartile; RAMIE ¼ robotic-assisted 6 YEROKUN ET AL MIE VERSUS OE FOR ESOPHAGEAL CANCER Ann Thorac Surg 2016;-:-–- Fig 2. Survival of open esophagectomy (OE) versus minimally invasive esophagectomy (MIE) and standard minimally invasive esophagectomy (SMIE) versus robotic-assisted minimally invasive esophagectomy (RAMIE), stratified by histologic type. (A) Adenocarcinoma: OE versus MIE; (B) adenocarcinoma: SMIE versus RAMIE; (C) squamous cell carcinoma: OE versus MIE; (D) squamous cell carcinoma: SMIE versus RAMIE. colleagues [12] both reported similar short-term outcomes between OE and MIE in Europe. Similarly, Luketich and associates [5] demonstrated that MIE is an efficacious and safe operation in the United States. In 1,033 consecutive patients at a high-volume center, the authors reported an exceptionally low mortality rate of 0.9%, with a median hospital stay of 8 days. On a population level, Mamidanna and coworkers [10] analyzed 7,502 patients who underwent OE and MIE (n ¼ 1,155) in the United Kingdom and found no differences in 30-day morbidity and mortality. Overall, there is consistent evidence that MIE can be performed by high-volume experts in the field safely and without additional risk to the patient. In this study, even with a median number of esophagectomies per center of only 2 per year, the outcomes again were similar and even slightly favored MIE when comparing perioperative outcomes. Conversely, comparative oncologic data in the literature are limited and inconclusive. Regarding lymph node harvesting, several institutions report improved nodal retrieval with MIE [11, 13, 14], with other studies showing no significant differences [12, 15]. For long-term outcomes, Palazzo and colleagues [6] reported 5-year mortality data from 168 patients treated in a high-volume academic institution and found a 2-fold survival advantage in patients treated with MIE (hazard ratio, 2.0). Although the authors accounted for several important patient and tumor variables, concerns were raised regarding the reproducibility of the significant outcome differences in these groups. Moreover, because of the small sample sizes in previous institutional studies, any disparities may be attributed to inadequate adjustment, including hospital-level factors. Our study improves on these limitations by analyzing data on a population level, attenuating the effect of outliers in center outcomes. In 2012, Biere and associates [9] published results from the Traditional Invasive Versus Minimally Invasive Esophagectomy (TIME) trial, the only randomized study examining differences in outcomes between OE and MIE. In the TIME trial, 115 patients from the United Kingdom Ann Thorac Surg 2016;-:-–- were randomized to either an open or minimally invasive approach. Although the authors concluded that OE and MIE were equivalent except for a decrease in perioperative pulmonary complications, the TIME trial was powered to demonstrate only differences in short-term outcomes. It lacked the ability to look at other perioperative or oncologic outcomes. By examining patient outcomes on a population level, our study improves on the power to detect small differences in survival in a multivariable fashion. With respect to comparative differences in the newest robotic approaches to esophagectomies, data are limited as well. Weksler and coworkers [4] published an institutional experience of 43 patients who underwent MIE, including only 11 patients who underwent robotic esophagectomies. Although the authors rightfully concluded that in their hands, robotic and nonrobotic approaches were equivalent, the sample size was small, the results were unadjusted, and the study lacked any oncologic data. Although our study similarly suffers from this issue when analyzing robotic versus standard MIE resections, we were able to account for known confounders in reporting our results. Our study has several limitations that should be acknowledged. First, as a limitation of our data set, specific approaches to MIE (McKeown, Ivor-Lewis, transhiatal) could not be captured. However, previous data have shown similar oncologic outcomes from any of the 3 approaches despite differences in perioperative complications [16]. We were also unable to differentiate between patients undergoing a hybrid approach (ie, laparoscopy combined with a minithoracotomy) versus a complete MIE. The inability to account for these variables allows for the possible introduction of unknown interactions and confounders. Second, our data set does not capture specific complications, which precludes our study from comparing perioperative outcomes with more granularity and from comparing the rate of complications related to approach. However, we used hospital length of stay and readmission rates as surrogates, which previous studies have shown to be effective markers for clinically significant perioperative complications [17]. Finally, our analysis was retrospective in nature and thus subject to selection bias. Although we attempted to control for known clinical, socioeconomic, hospital, and tumor covariates through our propensity-matched analysis, inherent differences between comparison groups may still occur that would be best addressed with a sufficiently powered randomized trial. For example, 2 different clinical trials in progress randomizing patients between OE and MIE are the French MIRO (Oesophagectomie Pour Cancer par Voie Conventionnelle ou Coelio-Assist ee) trial [18] and the British ROMIO (Randomized Oesophagectomy: Minimally Invasive or Open) trial [19]. Nonetheless, our study is the largest comparative effectiveness study of MIE to date to examine long-term survival. In conclusion, MIE is associated with modestly improved perioperative outcomes without compromising survival. Our results support the ongoing adoption of YEROKUN ET AL MIE VERSUS OE FOR ESOPHAGEAL CANCER 7 minimally invasive technologies in the surgical management of esophageal cancer. Institutional funding was the study. In addition, this work Institutes of Health–funded Network (B.C.G. and M.G.H.), primary funding source for this was supported by the National Cardiothoracic Surgery Trials 5U01HL088953-05. References 1. Lazzarino AI, Nagpal K, Bottle A, Faiz O, Moorthy K, Aylin P. Open versus minimally invasive esophagectomy: trends of utilization and associated outcomes in England. Ann Surg 2010;252:292–8. 2. Mallipeddi MK, Onaitis MW. The contemporary role of minimally invasive esophagectomy in esophageal cancer. Curr Oncol Red 2014;16:1–8. 3. Luketich JD, Alvelo-Rivera M, Buenaventura PO, et al. Minimally invasive esophagectomy: outcomes in 222 patients. Ann Surg 2003;238:486. 4. Weksler B, Sharma P, Moudgill N, Chojnacki K, Rosato E. Robot-assisted minimally invasive esophagectomy is equivalent to thoracoscopic minimally invasive esophagectomy. Dis Esophagus 2012;25:403–9. 5. Luketich JD, Pennathur A, Awais O, et al. Outcomes after minimally invasive esophagectomy: review of over 1000 patients. Ann Surg 2012;256:95. 6. Palazzo F, Rosato EL, Chaudhary A, et al. Minimally invasive esophagectomy provides significant survival advantage compared to open or hybrid esophagectomy for patients with cancers of the esophagus and gastroesophageal junction. J Am Coll Surg 2015;220:672–9. 7. Pennathur A, Luketich JD. Minimally invasive esophagectomy: short-term outcomes appear comparable to open esophagectomy. Ann Surg 2012;255:206–7. 8. Sihag S, Wright CD, Wain JC, et al. Comparison of perioperative outcomes following open versus minimally invasive ivor lewis oesophagectomy at a single, high-volume centre. Eur J Cardiothorac Surg 2012;42:430–7. 9. Biere SS, van Berge Henegouwen MI, Maas KW, et al. Minimally invasive versus open oesophagectomy for patients with oesophageal cancer: a multicentre, open-label, randomised controlled trial. Lancet 2012;379:1887–92. 10. Mamidanna R, Bottle A, Aylin P, Faiz O, Hanna GB. Shortterm outcomes following open versus minimally invasive esophagectomy for cancer in England: a population-based national study. Ann Surg 2012;255:197–203. 11. Parameswaran R, Veeramootoo D, Krishnadas R, Cooper M, Berrisford R, Wajed S. Comparative experience of open and minimally invasive esophagogastric resection. World J Surg 2009;33:1868–75. 12. Schoppmann SF, Prager G, Langer FB, et al. Open versus minimally invasive esophagectomy: A single-center case controlled study. Surg Endosc 2010;24:3044–53. 13. Singh RK, Pham TH, Diggs BS, Perkins S, Hunter JG. Minimally invasive esophagectomy provides equivalent oncologic outcomes to open esophagectomy for locally advanced (stage II or III) esophageal carcinoma. Arch Surg 2011;146:711–4. 14. Berger AC, Bloomenthal A, Weksler B, et al. Oncologic efficacy is not compromised, and may be improved with minimally invasive esophagectomy. J Am Coll Surg 2011;212: 560–6. 15. Osugi H, Takemura M, Higashino M, Takada N, Lee S, Kinoshita H. A comparison of video-assisted thoracoscopic oesophagectomy and radical lymph node dissection for squamous cell cancer of the oesophagus with open operation. Br J Surg 2003;90:108–13. 16. Coit D. Surgical approaches to invasive adenocarcinoma of the gastroesophageal junction. Am Soc Clin Oncol 8 YEROKUN ET AL MIE VERSUS OE FOR ESOPHAGEAL CANCER Educ Book 2013: http://dx.doi.org/10.1200/EdBook_AM.2013. 33.e144. 17. Kassin MT, Owen RM, Perez SD, et al. Risk factors for 30-day hospital readmission among general surgery patients. J Am Coll Surg 2012;215:322–30. 18. Briez N, Piessen G, Bonnetain F, et al. Open versus laparoscopically-assisted oesophagectomy for cancer: a Ann Thorac Surg 2016;-:-–- multicentre randomised controlled phase III trial–the miro trial. BMC cancer 2011;11:310. 19. Avery KN, Metcalfe C, Berrisford R, et al. The feasibility of a randomized controlled trial of esophagectomy for esophageal cancer–the romio (randomized oesophagectomy: Minimally invasive or open) study: protocol for a randomized controlled trial. Trials 2014;15:200.