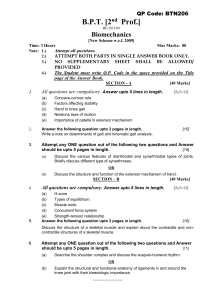
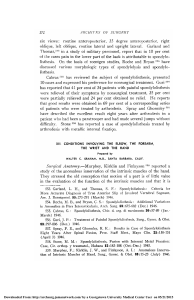
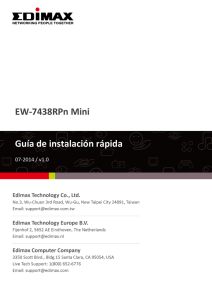
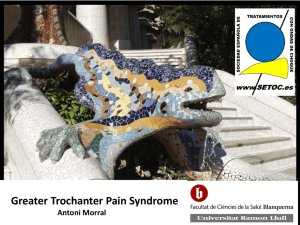
HAND/PERIPHERAL NERVE Outcomes and Complications of Tendon Transfers to Address Pinch and Grasp Weakness: A Systematic Review of the Operative Management of Ulnar Nerve Paralysis Downloaded from https://journals.lww.com/plasreconsurg by HfrIkaGAojkMSJGF5yDN1i8ch8wwE0fXdujRZV8lmytvQuQ+j/FfXobpYmJ5FPNTDArd6iscQpUjprG4tYVhHrQFtSgGl2nbt8zBCU4Q5tupTP3tStWYs+uzeAHRZ0kV on 07/19/2021 Christine V. Schaeffer, M.D. Heather A. McMahon, M.D. Eric R. Wagner, M.S., M.D. Brent R. DeGeorge, Jr., M.D., Ph.D. Charlottesville, Va.; and Atlanta, Ga. Background: Patients with ulnar nerve paralysis note difficulties performing activities of daily living because of weakness of pinch and altered grasp mechanism. This review investigates outcomes of tendon transfers for ulnar nerve paralysis to assist in shared decision-making with patients during preoperative counseling and to inform operative choices. Methods: A systematic review was conducted to identify studies reporting outcomes following tendon transfer for ulnar nerve palsy. Studies were screened according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, and inclusion and exclusion criteria were applied. Primary outcome measures included postoperative pinch strength and mechanism of grasp. Results: A total of 26 studies (687 patients) met criteria for inclusion. After pooled analysis, the flexor digitorum superficialis lasso procedure yielded the highest rate of complete correction of claw deformity (60.6 percent), followed by flexor digitorum superficialis four-tail operation (31.4 percent). The extensor carpi radialis longus four-tail operation yielded the greatest improvement in grip strength (3.8 kg). The extensor carpi radialis brevis four-tail operation resulted in the best open hand assessment and mechanism of closing scores; however, these studies did not objectively evaluate grip strength. The greatest increase in pinch strength was following tendon transfer to adductor pollicis alone. Conclusions: Despite the heterogeneous data, if the primary goal is improvement in the appearance of claw deformity, the evidence supports flexor digitorum superficialis lasso transfer. However, if the primary concern is grip strength, the data favor extensor carpi radialis longus four-tail transfer. When pinch strength is functionally limiting, adductorplasty alone is most effective. These data will assist providers in appropriately informing patients of common risks and complications and setting realistic expectations following tendon transfer procedures. (Plast. Reconstr. Surg. 148: 109, 2021.) I n the hand, the ulnar nerve characteristically innervates the adductor pollicis, deep head of the flexor pollicis brevis, all the interossei, the lumbricals of the ring and small fingers, and the hypothenar muscles—although anatomical variations of innervation have been documented.1,2 Ulnar nerve paralysis manifests clinically as weakness, deformity, asynchronous motion, and loss From the Department of Plastic Surgery, University of Virginia; and the Department of Orthopedic Surgery, Emory University School of Medicine. Received for publication March 17, 2020; accepted January 15, 2021. Copyright © 2021 by the American Society of Plastic Surgeons DOI: 10.1097/PRS.0000000000008052 of abduction/adduction control.1 The adductor pollicis and first dorsal interosseous muscles provide up to 75 percent of the adduction force of the thumb, and the intrinsic muscles of the hand account for approximately 50 percent of grip strength.3 Consequently, following ulnar nerve injury a reduction in pinch strength by up to 83 Disclosure: The authors have no financial interest to declare in relation to the content of this article. No funding was received for this work. Related digital media are available in the full-text version of the article on www.PRSJournal.com. www.PRSJournal.com 109 Copyright © 2021 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited. Plastic and Reconstructive Surgery • July 2021 percent and grip strength up to 85 percent has been observed.2,4,5 Finger deformities in ulnar paralysis occur because of the role of the intrinsic muscles in coordination of synchronous motion of the metacarpophalangeal and interphalangeal joints. Loss of intrinsic function of the ring and small fingers results in unopposed metacarpophalangeal extension by extensor digitorum communis and interphalangeal joint flexion by flexor digitorum superficialis and profundus with development of the characteristic claw deformity.1 In patients with ulnar nerve paralysis, the interphalangeal joints must be fully flexed before the extrinsic finger flexors can produce metacarpophalangeal flexion—causing significant limitations in grasp of both large and small objects.1,6 Functionally, these patients primarily complain of problems with grasping, lifting, and holding small objects; eating; and fine motor tasks.7 The most common functional deficits in ulnar nerve paralysis are a direct result of pinch weakness and finger deformities, resulting in an altered grasp mechanism. To treat these deficits in the chronic setting, there are multiple tendon transfers described to restore pinch strength and to improve grasp function by means of correction of the claw deformity. The reconstructive plan for these patients is based on numerous factors, including deficits on examination, patient goals, concomitant nerve/tissue injuries, and available tendons for transfer.6 However, there remains a paucity of comparison data on the outcomes of these tendon transfers (Fig. 1 and Table 1). Therefore, the goal of this review is to provide an evidence-based analysis of functional outcomes following tendon transfer, assist in preoperative counseling and shared decision-making, and inform operative choices. F1,T1 PATIENTS AND METHODS Data Collection We performed a systematic review in accordance with the 2009 Preferred Reporting Items for Fig. 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram outlining study selection for inclusion in review. 110 Copyright © 2021 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited. Volume 148, Number 1 • Restoration of Pinch and Grasp Table 1. Reported Tendon Transfer Procedures in the Literature for Ulnar Nerve Palsy Targeted Deformity Function Tendon Transfer Grasp Static correction of claw deformity ECU ECRL Tendon grafts Four-tail approach ECRL ECRB FCR FDS PL Lasso procedure ECRL FDS PL ECRB ECRL FDS FPB Split EDM APL EIP EBP PL Split EDM Dynamic correction of claw deformity Pinch Thumb adduction (transfer to AP) Index finger abduction (transfer to first DI) ECU, extensor carpi ulnaris; ECRL, extensor carpi radialis longus; ECRB, extensor carpi radialis brevis; FCR, flexor carpi radialis; FDS, flexor digitorum superficialis; PL, palmaris longus; AP, adductor pollicis; EDM, extensor digiti minimi; APL, adductor pollicis longus; EIP, extensor indicis proprius; DI, dorsal interosseous; EPB, extensor pollicis brevis. Systematic Reviews and Meta-Analyses guidelines.8 A systematic review of the literature regarding the use of tendon transfers to address functional deficits as a result of ulnar nerve paralysis was conducted using PubMed (1965 to 2018), Ovid MEDLINE (1948 to 2018), and Cochrane Database of Systematic Reviews; the queries were performed in April of 2018. The specific search strategies were devised in conjunction with a health sciences librarian with expertise in systematic review search methodology. We used the following search terms for each of the databases: ulnar nerve*; tendon transfer*. Detailed search strategies are outlined in Appendix 1. (See Appendix, Supplemental Digital Content 1, which shows the search strategy used for systematic review, http://links.lww.com/PRS/ E478.) In addition, we assessed the reference lists of included studies or pertinent reviews identified through the initial search to ensure inclusion of all relevant publications. No study design or date limits were imposed on the search. Inclusion criteria consisted of studies in the English language, written on the treatment of ulnar nerve paralysis with tendon transfers in human subjects. The exclusion criteria were studies without outcome data, studies that did not report outcomes stratified by procedure performed, and studies reporting outcomes following nerve transfers for ulnar nerve paralysis. Participants of any age with ulnar nerve paralysis were considered. No minimum length of followup criteria were required. We included studies evaluating patients with a combination of ulnar and median nerve paralysis if data for restoration of ulnar nerve function were reported. The authors screened the titles and abstracts yielded by the search against the eligibility criteria described above. Full articles were obtained for all titles that appeared to meet the inclusion criteria. The full-text reports were then reviewed to determine whether inclusion criteria were met. Data were extracted from each full text, including study characteristics (year, level of evidence, patient demographics), surgical technique, total duration of follow-up, clinical outcomes, and postoperative complications. Level of evidence for data were assigned using the criteria outlined by the Oxford Centre for Evidence Based Medicine, The Journal of Hand Surgery, and The Journal of Bone and Joint Surgery. Missing data elements were documented as “not reported.” To facilitate analysis of these treatment methods despite heterogeneity of selected outcome metrics, all available data were abstracted and categorized as objective (improvement of key pinch strength, grip strength, or grasp) and subjective (functional improvement, patient satisfaction). Subjective data most frequently consisted of either surgeon or patient-rated outcomes data and were reported as the total number of patients achieving a good or excellent result. Statistical Analysis We included studies representing the highest level of evidence available; however, the existing data are from retrospective cohorts or case series (Level III and IV). For articles that included individual patient information tables, data were collected and pooled estimates were measured. If individual patient information was not available, the reported overall mean values were used. Our reported outcomes focused on recovery of key pinch and grasp. Descriptive statistics with weighted means were calculated to report data given variability in sample size between studies. The collected data were divided into two categories: (1) the effect of tendon transfer on grasp (Table 2) and (2) the effect of tendon transfer on key pinch (Table 3). Surgical outcomes to evaluate improvement of grasp are summarized in Appendix 2 (see Appendix, Supplemental Digital Content 2, which shows surgical outcomes used to evaluate improvement in grasp. PIP, proximal 111 Copyright © 2021 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited. Plastic and Reconstructive Surgery • July 2021 Table 2. Summary of Data for Grasp Operations Lasso FDS ECRL Four-Tail PL FDS ECRL ECRB PL FCR Sample size No. of studies 10 1 1 7 4 2 1 1 No. of patients 277 (6–70) 12 18 112 (3–54) 106 (1–54) 75 25 4 digits (range) (21–54) Outcomes % of patients 61 (0–83) — — 31 (21–68) 13 (12–18) 29 25 — with complete correction of claw (range) OHA 61 — — 61 61 76 70 — CFA 89 — — 75 61 80 70 — MOC 77 — — 77 67 81 70 — Change in grip −4.2 — — 1.8 3.8 — — — strength (kg) (−10.7 to 4.4) Change in grip 4.2% — — 4.0% 15% — — — strength (% (−21 to 20%) unaffected hand) Complications Swan-neck 6% — — 30% 7%† — 6%† — deformity (2 to 17%)* (29 to 32%)* Checkrein 11% — — — — — — — deformity (6 to 14%)* Altered finger range of motion PIP 6%* — 4% of digits* — 9.5%† — — hyperextension Limited finger 6% † 5.5%† (PL and — 6% (extension)† — 5% (extension)† — ROM ECRL lasso) 11% (flexion)† 10% (flexion)† PIP stiffness 8% (6 to 20%)† — — — — — — — Recurrent claw 29%† — — 18% of digits† — 9.5%† — — deformity Adhesions — 17% (distal palm; PL 9% of digits† — — — — and ECRL lasso) Injury to — 8% 5.5% — — — — — median nerve FDS, flexor digitorum superficialis; ECRL, extensor carpi radialis longus; PL, palmaris longus; ECRB, extensor carpi radialis brevis; FCR, flexor carpi radialis; OHA, open hand assessment; CFA, closed fist analysis; MOC, mechanism of closing; PIP, proximal interphalangeal; ROM, range of motion. *Donor finger deformity. †Recipient finger deformity. interphalangeal; MRI, mean rate of improvement, http://links.lww.com/PRS/E479), and the Functional Hand Assessment scoring criteria are summarized in Appendix 3 (see Appendix, Supplemental Digital Content 4, which shows a summary of Functional Hand Assessment scoring criteria based on Brand’s criteria. PIP, proximal interphalangeal; MCP, metacarpophalangeal; IP, interphalangeal; DIP, proximal interphalangeal, http://links.lww.com/PRS/E480.)9 RESULTS Study Retrieval and Characteristics Figure 1 outlines our Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram of the selection process. After title and abstract search, 26 articles encompassing 687 patients met the inclusion and exclusion criteria. The causes of ulnar nerve paralysis included leprosy (eight studies, 307 patients), posttraumatic (13 studies, 161 patients), nerve compression/ severe cubital tunnel syndrome (six studies, 63 patients), and not reported (four studies). Two articles were prospective and 24 were retrospective. Twenty-three studies provided Level IV evidence, whereas three studies provided Level III evidence. Tendon Transfer for Grasp For the management of grasp, there are two generally accepted treatment approaches: static or dynamic tendon transfers. The Bouvier test is used to assess the integrity of the extensor apparatus and therefore determine complexity of the ulnar claw. A positive test is present if the patient can actively extend the interphalangeal joint when metacarpophalangeal joint extension is blocked. 112 Copyright © 2021 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited. X X — — — 5.5%, cramping — 17%, causing tenodesis — — — — Forearm symptoms Adhesions 64.6% 14%, PIP flexion contracture — Decreased thumb ROM No significant complications X X 72.8% 2.3% — 3.8 38.5% AP, adductor pollicis; DI, dorsal interosseous; FDS, flexor digitorum superficialis; FPB, flexor pollicis brevis; AbPL, abductor pollicis longus; EPB, extensor pollicis brevis; PL, palmaris longus; EIP, extensor indicis pollicis; EPB, extensor pollicis brevis; ECRL, extensor carpi radialis longus; ECRB, extensor carpi radialis brevis; EDM, extensor digiti minimi; MCP, metacarpophalangeal; ROM, range of motion. — 13%, abduction deficit 7%, De Quervain 7%, postoperative synovitis 22%, abduction deficit; 11%, MCP extensor lag 11%, intersection syndrome — — — 54.9% 2.9% 27.3% 11%, index adduction deficit 17%, extension deficit fifth MCP; 17%, flexion deficit fifth MCP — 1 6 1 6 1 8 1 9 2 29 (11–18) 1 6 2 1 36 (18–18) 15 2 40 (18–20) 1 4 PL FDS FPB AbPL EPB Sample size No. of studies No. of patients (range) Outcomes Change in pinch strength, kg Change in pinch strength, % unaffected hand Postoperative pinch strength, % unaffected hand Complications Donor deformity Transfer to AP Table 3. Summary of Data for Pinch Operations Transfer to First DI EIP (AP) EBP (First DI) Transfer to AP plus First DI ECRB (AP) EIP ECRL (AP) (First DI) OR EDM (AP) EDM AbPL (First DI) AbPL (First DI) (First DI) EDM (AP) EIP (First DI) Volume 148, Number 1 • Restoration of Pinch and Grasp A negative Bouvier test indicates a complex claw deformity, which requires an operation to address both metacarpophalangeal hyperextension and weak interphalangeal extension.6,10,11 The application of the Bouvier test for surgical decisionmaking is discussed in only two of the included studies.11,12 Fifteen studies including 531 patients described procedures, performed with the intent of restoring grasp by improving claw deformity, with a sample size per study ranging from four to 70 patients (see Table 2 for sample size by procedure).11–24 The mean patient age was 28 years (range, 7 to 60 years). The predominant cause of ulnar nerve paralysis was leprosy (301 patients), followed by trauma (92 patients). Patients with isolated ulnar nerve paralysis were evaluated in seven studies—the remaining eight studies included patients with median and ulnar nerve paralysis or did not specify. The mean duration of ulnar nerve paralysis was 45 months (range, 1 to 360 months), and the mean duration of total postoperative follow-up was 31 months (range, 3 to 150 months). Weighted surgical outcomes and postoperative complications are summarized in Table 2 and Figures 2 through 4 because of variability in study size. F2 –F4 I. Static Procedures: Claw Deformity Static procedures prevent metacarpophalangeal hyperextension and can be used in patients with “simple” claw deformities (positive Bouvier test) to improve grasp cascade and in patients who lack functional donor tendons for transfer.6,10,11 The described use of static tenodesis procedures (e.g., Riordan static tenodesis, Smith sling tenodesis, Srinivasan tenodesis) in the literature is largely limited to tetraplegic patients and therefore were not captured in the literature review.25–30 II. Dynamic Procedures: Claw Deformity In “complex” claw deformities (negative Bouvier test), dynamic tendon transfers are typically required to address weak interphalangeal extension caused by intrinsic muscle paralysis. Dynamic procedures also have the added benefit of increasing grip strength.6,10,11 Techniques used for dynamic tendon transfer to restore grasp include the lasso procedure and the fourtail approach, though many variations have been described in the literature. In the lasso procedure, the donor tendon is transferred by means of a volar route adjacent to the lumbrical muscle, looped through and around the A1 pulley, then sutured proximally to itself.17 Lasso procedures using flexor digitorum superficialis, 113 Copyright © 2021 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited. Plastic and Reconstructive Surgery • July 2021 Fig. 2. Weighted outcomes of rate of claw deformity resolution in patients undergoing procedures to improve grasp, accounting for differences in study size. FDS, flexor digitorum longus; 4-T, four-tail; ECRL, extensor carpi radialis longus; ECRB, extensor carpi radialis longus; PL, palmaris longus. extensor carpi radialis longus, and palmaris longus donor tendons were included in this review.11,12,15–17,19–22,31 The four-tail approach, also referred to in the literature as the modified Stiles-Bunnell procedure, requires splitting the donor tendon longitudinally into four equal tails, which are then passed through the lumbrical canal of each finger and attached to the radial lateral bands of the long, ring, and small fingers and the ulnar lateral band of the index finger.32,33 Alternative insertion sites have been described, including donor tendon insertion on the radial lateral bands of index, long, ring, and small fingers (Warren)34 and insertion on the radial aspect of proximal phalanx of the involved fingers (Burkhalter and Strait).13 Fourtail procedures using flexor digitorum superficialis, extensor carpi radialis longus, extensor carpi radialis brevis, palmaris longus, and flexor carpi radialis donor tendons were included in this rev iew.11–14,22–24,34 Burkhalter and Strait compared grip strength between tendon transfers (flexor digitorum superficialis four-tail, extensor carpi radialis longus four-tail, extensor carpi radialis brevis fourtail, and brachioradialis four-tail surgery) and reported that patients had “considerable increase in grip strength” following extensor carpi radialis longus four-tail and extensor carpi radialis brevis four-tail surgery, particularly when compared to patients who underwent flexor digitorum superficialis four-tail surgery.13 Tendon Transfer for Pinch Thirteen studies in this review described surgical procedures with the intent of restoring pinch function following ulnar nerve paralysis.23,24,35–45 The total number of patients included was 166, with sample size ranging from four to 22 patients (see Table 3 for sample size by procedure). The mean age of patients was 40 years (range, 9 to 77 years) and the predominant cause of ulnar nerve paralysis was trauma (eight studies, 85 patients), followed by cubital tunnel syndrome/ulnar nerve compression (five studies, 57 patients). One hundred four patients had isolated ulnar nerve paralysis; the remaining studies included patients with median and ulnar nerve paralysis (51 patients).23,24,35,37–41,45 The mean duration of ulnar nerve paralysis was 24.5 months (range, 3 to 192 months), and the mean duration of total postoperative follow-up was 29 months (range, 1 to 144 months). To restore pinch function, various tendons were transferred to the adductor pollicis alone, the first dorsal interosseous muscle alone, or a combination of the two procedures. The donor tendons described in this series include the extensor indicis proprius, flexor digitorum superficialis, abductor pollicis longus, extensor pollicis brevis, 114 Copyright © 2021 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited. Volume 148, Number 1 • Restoration of Pinch and Grasp Fig. 3. Open hand assessment, closed fist analysis, and mechanism of closing weighted outcomes of procedures performed to improve grasp, accounting for differences in study size. FDS, flexor digitorum longus; 4-T, four-tail; ECRL, extensor carpi radialis longus; ECRB, extensor carpi radialis longus; PL, palmaris longus. 115 Copyright © 2021 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited. Plastic and Reconstructive Surgery • July 2021 Fig. 4. Change in grip strength preoperatively and postoperatively in kilograms after procedures performed to improve grasp, weighted to account for differences in study size. FDS, flexor digitorum longus; 4-T, four-tail; ECRL, extensor carpi radialis longus. extensor digiti minimi, extensor carpi radialis longus, extensor carpi radialis brevis, palmaris longus, and flexor pollicis brevis. Weighted outcomes of the above studies are illustrated in Figure 5 and summarized in Table 3. DISCUSSION Regardless of cause, ulnar nerve paralysis results in significant functional impairment, with weakness of pinch and altered grasp.46,47 Based on the data, the flexor digitorum superficialis lasso procedure resulted in the highest rate of correction of claw deformity (60.6 percent), followed by the flexor digitorum superficialis fourtail approach (31.4 percent). The functional hand assessment instrument was used to evaluate postoperative results, and extensor carpi radialis brevis four-tail surgery resulted in the best open hand assessment and mechanism of closing Fig. 5. Change in key pinch strength preoperatively and postoperatively in kilograms after procedures performed to improve pinch, weighted to account for differences in study size. AP, adductor pollicis; DI, dorsal interosseous. 116 Copyright © 2021 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited. Volume 148, Number 1 • Restoration of Pinch and Grasp scores.9,48 The flexor digitorum superficialis lasso procedure gave the best closed fist analysis results. However, the functional hand assessment was performed in two separate studies for flexor digitorum superficialis lasso, flexor digitorum superficialis four-tail, and extensor carpi radialis longus four-tail operations and only one study for extensor carpi radialis brevis four-tail and palmaris longus four-tail surgery. The weighted averages for the former operations, represented in Figures 2 through 4, demonstrate a more representative postoperative result than the outcomes reported from small, individual studies. Dynamic procedures completely corrected claw deformity in 35 percent of patients and resulted in a net increase in strength of 6.4 percent from preoperatively to postoperatively (62.7 percent of the normal, unaffected side). For pinch procedures, the average restoration of pinch strength was 60 percent of the unaffected hand. The greatest improvement of grip based on weighted average results was seen following the extensor carpi radialis longus four-tail operation, with a 3.8-kg increase in grip and 15 percent net increase in strength from preoperative to postoperative measurement (49 percent of unaffected hand grip strength) (Table 2). In addition, the use of a wrist extensor (extensor carpi radialis longus and brevis) for tendon transfer biomechanically introduces a new motor power into the hand and maintains tension during wrist flexion because of its dorsal location.16,17,49 Hastings and Davidson11 and Hastings and McCollam17 reported grip strength results following flexor digitorum superficialis lasso in 1988 and 1994. In 1988, this group noted an increase in grip strength of 7.8 kg following the flexor digitorum superficialis lasso procedure at 40 months postoperatively; however, this study included grip strength measurements for only nine patients, and grip at 8 months decreased by 10.7 kg compared to preoperative measurements. In 1994, a 21 percent decrease in grip strength was noted following the flexor digitorum superficialis lasso procedure.11,17 Consequently, the authors attributed the increase in grip strength at 40 months in their initial study to “extremity conditioning,” and recommended against using the flexor digitorum superficialis lasso to increase grip. Özkan et al. noted superior results following the flexor digitorum superficialis lasso procedure for grip compared to the extensor carpi radialis longus four-tail procedure— increase in grip strength of 4.4 kg and 16 percent increase in strength (versus 3.8 kg and 15 percent, respectively, after the extensor carpi radialis longus four-tail procedure). They attributed these results to tendon transfers to all four digits, instead of only clawed digits.12 Interpretation of absolute increase in grip strength measured in kilograms is limited, as only two studies [56 patients (Hastings and McCollam, and Özkan et al.)] reported this outcome.12,17 The greatest increase in pinch was seen following transfer to the adductor pollicis alone. However, only one of three studies evaluating adductorplasty alone measured pinch. The individual tendon transfers that resulted in the most significant increase in pinch strength were extensor carpi radialis longus to adductor pollicis and abductor pollicis longus to the first dorsal interosseous.38,40,41,44 Postoperative pinch as a percentage of the unaffected hand was highest following transfer to the first dorsal interosseous alone— transfer of abductor pollicis longus to the first dorsal interosseous resulted in 75 percent of unaffected hand pinch strength. As a group, transfer to adductor pollicis alone resulted in the greatest increase in pinch strength as a percentage of normal hand pinch strength. However, both flexor digitorum superficialis to adductor pollicis and combined transfer of extensor digiti minimi to adductor pollicis/extensor indicis proprius to the first dorsal interosseous resulted in a 41 percent increase. In general, complication reporting in these studies was inconsistent and sparse. However, swan-neck deformity was a commonly noted postoperative donor finger deformity following the flexor digitorum superficialis four-tail procedure (30 percent). Several authors hypothesize that this deformity relates to unopposed pull of the central slip on the middle phalanx, removal of the primary proximal interphalangeal joint flexor, attachment of the donor tendon slip to the extensor mechanism (by means of the lateral bands in the classic four-tail approach), preoperative laxity of the proximal interphalangeal joint volar plate, and surgical technique.6,50 Swan-neck deformities were noted with increased frequency following four-tail approaches (Table 2) and not reported following extensor carpi radialis longus/palmaris longus lasso procedures. This finding may be attributable to the donor tendon slip not attaching to the extensor mechanism with the lasso approach and therefore not increasing extension torque.51 Theoretical increased risk of swan-neck deformity has also been suggested with tendon transfer to the extensor mechanism in patients with a positive preoperative Bouvier test.6 Tendon transfers using a wrist extensor (extensor carpi 117 Copyright © 2021 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited. Plastic and Reconstructive Surgery • July 2021 radialis longus/brevis) or palmaris longus typically require lengthening by tendon grafts (palmaris or plantaris tendon, tensor fascia lata graft) to reach the insertion target on the digit.15 The use of tendon grafts theoretically increases the morbidity of the procedure and is thought to increase rate of adhesions (Table 2). Adhesions were noted as a postoperative complication in one study following palmaris longus transfer to the first dorsal interosseous [one patient (16.7 percent)]. One case of intersection syndrome requiring tenolysis was noted following combined tendon transfer of extensor carpi radialis longus to adductor pollicis and abductor pollicis longus to the first dorsal interosseous. Limited thumb abduction was noted in extensor carpi radialis brevis [two of 15 patients (13 percent)] and extensor carpi radialis longus [two of nine patients (22 percent)] transfer to the adductor pollicis.4,41 Some debate exists in the literature regarding adhesion formation after the use of wrist tendon as donors; however, in these studies, no evidence of significant limitations in wrist range of motion were noted.41,44 Recurrence of or incomplete correction of claw deformity were reported only following flexor digitorum superficialis lasso (29 percent), flexor digitorum superficialis four-tail (18 percent), and extensor carpi radialis brevis four-tail (9.5 percent) tendon transfers. Interestingly, the highest rates of resolution of claw deformity were also reported following flexor digitorum superficialis lasso (61 percent; range, 0 to 81 percent) and flexor digitorum superficialis four-tail (31 percent; range, 21 to 68 percent) procedures. The present study has several limitations. Of the 26 studies, three presented Level III evidence and the remainder were Level IV. As a result, a formal meta-analysis could not be performed, and we were limited in the conclusions and the strength of recommendations that could be made. Significant variability in outcomes reporting also limited our ability to directly compare studies. We focused primarily on the most common and consistently reported outcomes (see Appendix, Supplemental Digital Content 2, http://links.lww.com/PRS/ E479). For studies evaluating grasp, outcomes were grouped based on donor tendon used, yet there were significant differences in methodology between authors. Sample size of individual studies was also a significant limitation. Three of the larger studies—Brandsma et al.50 (100 patients), Brand9 (150 patients), and Solonen and Bakalim52 Fig. 6. Algorithm for evidence-based management of grasp and pinch deficits with ulnar nerve palsy. *Bouvier test: a positive test is present if the patient can actively extend the interphalangeal joints when metacarpophalangeal joint extension is blocked, whereas a negative Bouvier test indicates a complex claw deformity, which requires an operation to address metacarpophalangeal joint hyperextension and weak interphalangeal extension. FDS, flexor digitorum superficialis; ECRL, extensor carpi radialis longus; AP, adductor pollicis. 118 Copyright © 2021 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited. Volume 148, Number 1 • Restoration of Pinch and Grasp (34 patients)—were excluded from this review, as results were not categorized based on procedure performed. For studies evaluating pinch, there was significant variability in donor tendons used for transfer. Therefore, outcomes were grouped based on tendon transfer target(s). The majority of tendon transfer approaches for pinch outlined here were described in only a single study (eight of 13 studies), with a maximum of two studies per group evaluating the same transfer(s). Lastly, given the limited number of studies available, a minimum duration of follow-up was not selected as an exclusion criterion. The minimum follow-up of the studies included was 6 months, which may be an insufficient amount of time to accurately assess postoperative results and complications. Ultimately, we were able to identify several key conclusions, which can help to inform the joint decision-making process (summarized in Fig. 6). The Bouvier test should be performed preoperatively to assess the integrity of the extensor mechanism and to guide the decision to perform static versus dynamic procedures for grasp. Based on the available evidence, if the primary goal is to improve appearance of the claw deformity with a dynamic procedure, a flexor digitorum superficialis lasso procedure should be considered. If the patient’s primary concern is grip strength, the extensor carpi radialis longus four-tail tendon transfer should be considered. When pinch strength is functionally limiting, adductorplasty alone is the most successful procedure in the available literature. We anticipate that this review will assist providers in counseling their patients regarding postoperative expectations and summarizes the risks of these procedures. In addition, we recommend future efforts to standardize preoperative and postoperative assessments, including objective grip and range-of-motion data and patient-reported outcomes questionnaires.53 Brent R. DeGeorge, Jr., M.D., Ph.D. Department of Plastic Surgery University of Virginia 1215 Lee Street Charlottesville, Va. 22903 [email protected] ACKNOWLEDGMENT The authors would like to thank the staff at the University of Virginia Health Sciences Library for their assistance with the compilation of the systematic review. REFERENCES 1. Dell PC, Sforzo CR. Ulnar intrinsic anatomy and dysfunction. J Hand Ther. 2005;18:198–207. 2. Mannerfelt L. Studies on the hand in ulnar nerve paralysis: A clinical-experimental investigation in normal and anomalous innervation. Acta Orthop Scand. 1966;37(Suppl 87):3–176. 3. Cook S, Gaston RG, Lourie GM. Ulnar nerve tendon transfers for pinch. Hand Clin. 2016;32:369–376. 4. Smith RJ. Tendon Transfers of the Hand and Forearm. 1st ed. Boston: Little Brown; 1987. 5. Kozin SH, Porter S, Clark P, Thoder JJ. The contribution of the intrinsic muscles to grip and pinch strength. J Hand Surg Am. 1999;24:64–72. 6. Diaz-Garcia RJ, Chung KC. A comprehensive guide on restoring grasp using tendon transfer procedures for ulnar nerve palsy. Hand Clin. 2016;32:361–368. 7. McCormick CA, Rath S, Patra PN, Pereira J, Wilkinson M. A qualitative study of common functional problems experienced by people with complete ulnar nerve paralysis. Lepr Rev. 2008;79:154–161. 8. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and metaanalyses: The PRISMA statement. PLoS Med. 2009;6:e1000097. 9. Brand P. Paralytic claw hand; with special reference to paralysis in leprosy and treatment by the sublimis transfer of Stiles and Bunnell. J Bone Jointt Surg Br. 1958;40:618–632. 10. Sammer DM, Chung KC. Tendon transfers: Part II. Transfers for ulnar nerve palsy and median nerve palsy. Plast Reconstr Surg. 2009;124:212e–221e. 11. Hastings H, Davidson S. Tendon transfers for ulnar nerve palsy: Evaluation of results and practical treatment considerations. Hand Clin. 1988;4:167–178. 12. Özkan T, Özer K, Gülgönen A. Three tendon transfer methods in reconstruction of ulnar nerve palsy. J Hand Surg Am. 2003;28:35–43. 13. Burkhalter WE, Strait JL. Metacarpophalangeal flexor replacement for intrinsic-muscle paralysis. J Bone Joint Surg Am. 1973;55:1667–1676. 14. Taylor NL, Raj AD, Dick HM, Solomon S. The correction of ulnar claw fingers: A follow-up study comparing the extensorto-flexor with the palmaris longus 4-tailed tendon transfer in patients with leprosy. J Hand Surg Am. 2004;29:595–604. 15. Narayanakumar TS. Claw-finger correction in leprosy using half of the flexor digitorum superficialis. J Hand Surg Eur Vol. 2008;33:494–500. 16. Malaviya GN. Comparative evaluation of effectiveness of different motor muscles in modified lasso procedure for correction of finger clawing. J Hand Surg Br. 2003;28:597–601. 17. Hastings H II, McCollam SM. Flexor digitorum superficialis lasso tendon transfer in isolated ulnar nerve palsy: A functional evaluation. J Hand Surg Am. 1994;19:275–280. 18. Patond KR, Betal BD, Gautam V. Results of thumb correction in leprosy using different techniques. Indian J Lepr. 1999;71:155–166. 19. Shah A. Correction of ulnar claw hand by a loop of flexor digitorum superficialis motor for lumbrical replacement. J Hand Surg Br. 1984;9:131–133. 20. Rath S. Split flexor pollicis longus tendon transfer to A1 pulley for correction of paralytic Z deformity of the thumb. J Hand Surg Am. 2013;38:1172–1180. 21. Manivannan G, Das P, Karthikeyan G, John AS. Reconstructive surgery in children to correct ulnar claw hand deformity due to leprosy. Lepr Rev. 2014;85:74–80. 22. Ozkan T, Ozer K, Yukse A, Gulgonen A. Surgical reconstruction of irreversible ulnar nerve paralysis in leprosy. Lepr Rev. 2003;74:53–62. 23. Zweig J, Rosenthal S, Burns H. Transfer of the extensor digiti quinti to restore pinch in ulnar palsy of the hand. J Bone Joint Surg Am. 1972;54:51–59. 119 Copyright © 2021 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited. Plastic and Reconstructive Surgery • July 2021 24. Uraloğlu M, Orbay H, Açar HI, Sensöz O. Flexor pollicis brevis adductorplasty: An alternative method in ulnar nerve paralysis. Ann Plast Surg. 2006;57:110–114. 25. McCarthy CK, House JH, Van Heest A, Kawiecki JA, Dahl A, Hanson D. Intrinsic balancing in reconstruction of the tetraplegic hand. J Hand Surg Am. 1997;22:596–604. 26. Muzykewicz DA, Arnet U, Lieber RL, Fridén J. Intrinsic hand muscle function, part 2: Kinematic comparison of 2 reconstructive procedures. J Hand Surg Am. 2013;38:2100–2105.e1. 27. Fridén J, Reinholdt C, Gohritz A. The extensor pollicis longus-loop-knot (ELK) procedure for dynamic balance of the paralyzed thumb interphalangeal joint. Tech Hand Up Extrem Surg. 2013;17:184–186. 28. House JH. Reconstruction of the thumb in tetraplegia following spinal cord injury. Clin Orthop Relat Res. 1985;195:117–128. 29. Reinholdt C, Fridén J. Outcomes of single-stage griprelease reconstruction in tetraplegia. J Hand Surg Am. 2013;38:1137–1144. 30. Fridén J, Reinholdt C, Turcsányii I, Gohritz A. A single-stage operation for reconstruction of hand flexion, extension, and intrinsic function in tetraplegia: The alphabet procedure. Tech Hand Up Extrem Surg. 2011;15:230–235. 31. Patond KR, Betal BD, Gautam V. Results of thumb correction in leprosy using different techniques. Indian J Lepr. 1999;71:155–166. 32. Bunnell S. Surgery of the intrinsic muscles of the hand other than producing opposition of the thumb. J Bone Joint Surg. 1942;24:1–3. 33. Stiles JH, Forrester-Brown M. Treatment of Injuries of Peripheral Spinal Nerves. London: Henry Frowde & Hoddler & Stoughton; 1922. 34. Jamali AR, Bhatti A, Mehboob G. Transfer of extensor carpi radialis brevis as an extensor to extensor motor transfer (EEMT) in ulnar nerve palsy. J Pak Med Assoc. 2006;56:309–313. 35. Hamlin C, Littler JW. Restoration of power pinch. J Hand Surg Am. 1980;5:396–401. 36. Edgerton MT, Brand PW. Restoration of abduction and adduction to the unstable thumb in median and ulnar paralysis. Plast Reconstr Surg. 1965;36:150–164. 37. Nobuta S, Sato K, Kanazawa K, Hatori M, Itoi E. Effects of tendon transfer to restore index finger abduction for severe cubital tunnel syndrome. Ups J Med Sci. 2009;114:95–99. 38. Nemoto K, Arino H, Amako M, Kato N. Abductor pollicis longus transfer to restore index abduction in severe cases of cubital tunnel syndrome. J Hand Surg Eur Vol. 2007;32:296–301. 39. Hirayama T, Atsuta Y, Takemitsu Y. Palmaris longus transfer for replacement of the first dorsal interosseous. J Hand Surg Br. 1986;11:84–86. 40. Neviaser RJ, Wilson JN, Gardner MM. Abductor pollicis longus transfer for replacement of first dorsal interosseous. J Hand Surg Am. 1980;5:53–57. 41. Fischer T, Nagy L, Buechler U. Restoration of pinch grip in ulnar nerve paralysis: Extensor carpi radialis longus to adductor pollicis and abductor pollicis longus to first dorsal interosseus tendon transfers. J Hand Surg Br. 2003;28: 28–32. 42. Alnot JY, Masquelet A. Restoration of thumb-index pinch by a double tendon transfer following ulnar nerve paralysis (in English, French). Ann Chir Main 1983;2:202–210. 43. De Abreu LB. Early restoration of pinch grip after ulnar nerve repair and tendon transfer. J Hand Surg Br. 1989;14:309–314. 44. Smith RJ. Extensor carpi radialis brevis tendon transfer for thumb adduction: A study of power pinch. J Hand Surg Am. 1983;8:4–15. 45. Robinson D, Aghasi MK, Halperin N. Restoration of pinch in ulnar nerve palsy by transfer of split extensor digiti minimi and extensor indicis. J Hand Surg Br. 1992;17:622–624. 46. Lee SK, Wisser JR. Restoration of pinch in intrinsic muscles of the hand. Hand Clin. 2012;28:45–51. 47. McCormick CA, Rath S, Patra PN, Pereira J, Wilkinson M. A qualitative study of common functional problems experienced by people with complete ulnar nerve paralysis. Lepr Rev. 2008;79:154–161. 48. Brand PW. Tendon grafting. J Bone Joint Surg Br. 1961;43:444–453. 49. Sapienza A, Green S. Correction of the claw hand. Hand Clin. 2012;28:53–66. 50. Brandsma JW, Ottenhoff-De Jonge MW. Flexor digitorum superficialis tendon transfer for intrinsic replacement. Long-term results and the effect on donor fingers. J Hand Surg Br. 1992;17:625–628. 51. Hastings H II, McCollam SM. Flexor digitorum superficialis lasso tendon transfer in isolated ulnar nerve palsy: A functional evaluation. J Hand Surg Am. 1994;19:275–280. 52. Solonen KA, Bakalim GE. Restoration of pinch grip in traumatic ulnar palsy. Hand 1976;8:39–44. 53. Hudak PL, Amadio PC, Bombardier C. Development of an upper extremity outcome measure: The DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative Group (UECG). Am J Ind Med. 1996;29:602–608. 120 Copyright © 2021 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.