International Journal of Gynecology and Obstetrics (2005) 89, 236 — 241
www.elsevier.com/locate/ijgo
REVIEW ARTICLE
The B-Lynch and other uterine compression suture
techniques
M.S. Allama,T, C. B-Lynchb
a
Department of Obstetrics and Gynaecology, South Glasgow University Hospitals, Glasgow, UK
Department of Obstetrics and Gynaecology, Milton Keynes General Hospital, Oxford Deanery, UK
b
Received 5 January 2005; received in revised form 28 January 2005; accepted 4 February 2005
KEYWORDS
B-Lynch;
Uterine compression
sutures
Abstract
Background: Postpartum hemorrhage (PPH) remains among the 5 main causes of
maternal death in developing and developed countries, and uterine atony is the most
common cause (75—90%) of primary PPH. Uterine compression sutures running
through the full thickness of both uterine walls (posterior as well as anterior) have
recently been described for surgical management of atonic PPH. Christopher B-Lynch
was the first to highlight this revolutionary principle, and other uterine compression
suture techniques have since been described by Hayman and Cho.
Objectives: Step-by-step description of the B-Lynch brace suture and discussion of
the current compression suture techniques.
Conclusions: The different uterine suture techniques have proved to be valuable and
safe alternatives to hysterectomy in the control of massive PPH, and the present review
can make the surgeon better aware of their effective use and the risks they may entail.
D 2005 International Federation of Gynecology and Obstetrics. Published by Elsevier
Ireland Ltd. All rights reserved.
1. Introduction
A blood loss in excess of 1000 mL following delivery,
together with the rapidity of the loss, is used as a
T Corresponding author. 8 Lanfine road, Ralston, PA1 3NL,
Scotland, UK. Tel.: +44 1415612644.
E-mail address: [email protected] (M.S. Allam).
clinical diagnostic tool for major postpartum hemorrhage (PPH). Major PPH occurs in approximately
4% of vaginal and 6% of cesarean deliveries [1]. In a
study of 48,865 women who were delivered
between 1997 and 1999 in the London area in
England, severe PPH was diagnosed in 6.7 per 1000
deliveries [2]; the World Health Organization
estimated at 20 million the annual number of
maternal complications of PPH [3]; and in the
0020-7292/$ - see front matter D 2005 International Federation of Gynecology and Obstetrics. Published by Elsevier Ireland Ltd.
All rights reserved.
doi:10.1016/j.ijgo.2005.02.014
The B-Lynch and other compression suture techniques
developing world death from PPH, which occurs in
approximately 1 per 1000 deliveries [1], accounts
for up to 4% of all maternal deaths in the United
States [4]. Moreover, PPH was determined by the
2000—2002 triennial Confidential Enquiry Into
Maternal Deaths to have played a significant role
in 17 deaths in the United Kingdom [5] and it
remains among the 5 main causes of maternal
death in developing and developed countries [6].
Uterine atony accounts for 75—90% of primary PPH
[1].
Different uterine compression sutures have
recently been described to control PPH, including
a suture that runs through the full thickness of both
anterior and posterior uterine walls. Christopher BLynch was the first to highlight this technique [7].
The present review emphasises the special features
of the B-Lynch brace suture and provides a comparative discussion of the current compression
suture techniques [7—9].
237
In the case of coagulopathy, if diffused bleeding
is controlled by compression, it will also be
controlled by the suture. However, application of
the B-Lynch suture is not a substitute for the
medical treatment of coagulopathy.
If the criteria for the B-Lynch suture are met, the
uterus remains exteriorized until the suture is
completed. The assistant performs uterine compression with both hands throughout suture placement the by the main surgeon.
2.3. Suture application in the case of a low
transverse hysterotomy wound
2.3.1. Placement of first stitch relative to low
transverse cesarean section wound
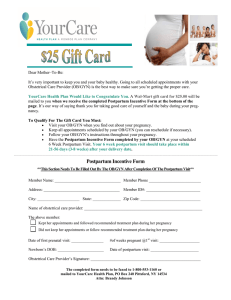
With the bladder displaced inferiorly, the first
stitch is placed 3 cm below the hysterotomy
incision on the patient’s right side and threaded
through the uterine cavity to emerge anteriorly 3
cm above the upper-incision margin, approximately
4 cm from the lateral border of the uterus (Fig. 1).
2. Methods
The procedure was first performed in 1989 by one
of the authors (C.B-L.) in a patient who was
experiencing massive PPH but refused hysterectomy. The suture aims to exert continuous
vertical vascular compression [7,10,11].
2.1. Surgeon’s position
It is assumed that the surgeon is right-handed and
standing on the right side of the patient.
2.2. Test for the potential efficacy of the
B-Lynch suture before performing the
procedure
The patient is placed in the Lloyd Davies or
lithotomy position. Once laparotomy is performed, an assistant standing between the
patient’s legs intermittently swabs her vagina to
determine the presence and extent of bleeding.
After the uterus is exteriorized, bimanual compression is applied. To do this, the bladder
peritoneum is first reflected inferiorly below
the cervix; then, the whole uterus is compressed
by placing one hand posteriorly with the ends of
the fingers at the level of the cervix and the
other hand anteriorly just below the bladder that
has been displaced inferiorly. If bleeding stops
with compression, there is a good chance that
the B-Lynch suture will also cause the bleeding to
stop.
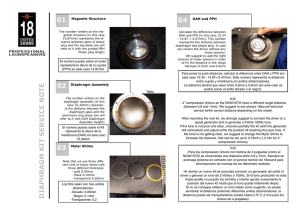
2.3.2. Fundus
The suture material is now carried over the top of
the uterus to the posterior side. The suture
material should be more or less vertical over the
fundus, i.e., lay about 4 cm from the horn (Fig. 2).
It does not tend to slip laterally toward the broad
ligament because the suture material has been
pulled through and the uterus is being compressed,
which ensure that proper placement is achieved
and maintained (Fig. 2).
2.3.3. Posterior wall
The spot on the posterior aspect of the uterus
where the suture should be pulled through the
uterine wall is easy to determine. It is, on the
horizontal plane, at the level of the uterine incision
at the insertion of the uterosacral ligament (Fig. 2).
The assistant keeps compressing the uterus
manually as the suture material is fed through the
posterior wall into the cavity. This helps the
surgeon pull it through without breakage and allows
for maximum compression at the end of the
procedure. Furthermore, it minimizes the risk of
suture slipping and uterine trauma. The suture
material now lies horizontally on the cavity side of
the posterior uterine wall (Fig. 2).
2.3.4. Fundus
The suture material is pulled again through to the
posterior wall (serosal wall), brought over the top
of the fundus posteriorly, and then down the
anterior left side of the uterus. The needle is now
238
M.S. Allam, C. B-Lynch
Figure 1
The B-Lynch suture, anterior view [10].
placed in a position symmetrical to that in which it
first entered the right side (i.e., 3 cm above the
upper lip of the incision and 4 cm from the lateral
side of the uterus), pushed into the uterine cavity
and then again through the lower segment, 3 cm
below the lower incision margin (Fig. 2).
The assistant maintains compression as the
suture material is pulled through its different
points of entry in a way that ensures uniform
tension and no slipping. The 2 ends of the suture
are tied with a double throw knot to maintain
tension after the lower segment incision had been
closed by either the 1- or 2-layer method (Fig. 2).
2.3.5. Relation to the hysterotomy incision
Even tension on the 2 ends of the suture material
can be manually maintained while the lower-seg-
Figure 2
ment incision is closed; alternatively, the 2 ends
can be tied before closure and both options works
equally well. If the latter is chosen, however, it is
essential that the corners of the hysterotomy
incision be identified and stay sutures placed
before the knot is tied. This ensures that when
the lower segment is closed, the corners of the
incision are not missed. It is important to identify
the corners of the uterine incision to ensure that no
bleeding points are left unsecured, particularly
because most of the patients undergoing the
procedure are hypotensive. Because the knot is
low on the lower segment, there is room for wound
closure.
Because the uterus undergoes its maximum
involutionary process in the first week after vaginal
or cesarean delivery, the suture probably will have
The B-Lynch suture, front view, back view, and knot [10].
The B-Lynch and other compression suture techniques
lost some tension after about 24—48 h. Yet, enough
hemostasis will have been achieved and there is no
need to delay closing the abdomen after the suture
placement. The assistant swabbing the vagina can
verify that the bleeding has been controlled.
2.4. Suture placement after vaginal delivery
If laparotomy is required for the management of
atonic PPH, hysterotomy is warranted before placement of the B-Lynch suture. The blind application
of the suture can cause obliteration of the cervical
and/or uterine lumens and lead to pyometra and
morbidity [12]. Moreover, B-Lynch suture application without confirmation that the uterine cavity is
completely empty is less likely to be successful. By
the time laparotomy begins, even if uterine exploration has been performed, blood clots are likely to
have collected within the uterine cavity. Hysterotomy allows to explore the uterine cavity and
remove blood clots, retained products of conception, and an abnormally placed placenta. Hysterotomy thus makes proper application of the suture
possible, and therefore also maximum, even, and
simultaneous compression to both sides of the
uterus [11].
2.5. Application for abnormal placentation
The B-Lynch suture may be beneficial in cases of
placenta accreta, percreta, and increta. In a
patient with placenta praevia, a figure-of-eight or
transverse compression suture of the lower segment anteriorly, posteriorly, or both, is applied to
control bleeding. If it does not control bleeding,
the B-Lynch suture may be placed in addition for
hemostasis [11].
3. Discussion
At the time of writing there were 10 reports
involving a total of 38 women who had been treated
with the B-Lynch surgical technique for severe PPH,
with 36 successes and 2 failures [7,13—21]. More
than 1000 procedures have been performed worldwide, with only 7 failures reported [10]. The
reported causes of failure varied from placenta
percreta and uncontrolled disseminated intravascular coagulopathy to lack of suture tension or
improper suture application [10].
Three patients underwent laparoscopy at various
time intervals postoperatively for sterilisation,
suspected pelvic inflammatory disease, and appendicitis. One patient with ileostomy underwent
239
laparotomy for suspected intestinal obstruction 10
days after receiving a B-Lynch suture (unpublished
data). Magnetic resonance imaging and hysterosalpingography performed in 1 patient revealed no
intraperitoneal or uterine sequelae [17]. No complications have been observed in the 5 patients of
the first published series, who have all experienced
further pregnancy and delivery [7,10].
The prophylactic application of the B-Lynch
suture was performed after cesarean delivery in
15 patients significantly at risk for PPH, and there
were no reported complications. All patients were
fully counseled about the procedure and its benefits, risks, and implications. Informed consent was
signed before surgery (unpublished data).
The B-Lynch surgical technique can preserve life
and fertility [7], and it has been recommended by
various authorities worldwide [5,22—24]. The chances for success of this simple, inexpensive, and
quick procedure are uniquely tested immediately
before and after its performance, and the procedure can be performed by surgeons with average
surgical skills at units with limited resources.
Furthermore, with the B-Lynch suture, an even
pressure can be achieved at the same time to both
sides of the uterine body. With more than 1000
procedures performed worldwide by surgeons of
various experience at units receiving widely different financial and clinical support, it is the most
frequently used surgical technique for uterine
compression. Tied or untied, the suture provides
even compression, and thus provides enough space
to comfortably close the uterine incision without
disturbing the anatomy. A new, user-friendly material is currently used by the authors (Ethiguard
blunt needle, half circle, 70-mm in length, with a
90-cm suture [available in violet, code W3709];
Ethicon, Somerville, NJ, USA). The suture material
is a poliglecaprone 25 monofilament (Monocryl;
Ethicon) whose absorption profile is 60%, 20%, and
0% of the original strength at 7, 14, and 21 days.
Mass absorption is complete at 90—120 days. The
long blunt needle allows for safe handling and
placement. The suture material can be easily and
safely adjusted and tightened against the uterine
wall. The length of the suture is very convenient for
the assistant to maintain a persistent, even compression on both sides of the uterine body while the
lower segment incision is being closed by the main
surgeon. No adverse effects of the Monocryl
filament have been reported, but its long-term
effects are not yet clear. The postprocedure
patency of the uterine and cervical lumens has
been tested [17], and no known postoperative
mortality related to the B-Lynch suture has been
reported [5]. Furthermore, as it was first applied
240
M.S. Allam, C. B-Lynch
in 1989, the B-Lynch suture technique has data
from a longer follow-up time than the other
uterine compression techniques [10]. As it is now
applied at a much lower threshold of suspicion
than in the first published series [7], and sometimes prophylacticaly in patients at high risk,
competence for its performance will increase.
The cost-effectiveness of this procedure may
continue to encourage developing countries to
consider it for both prophylactic and therapeutic
purposes. It is easy to perform after cesarean
deliveries and can be used, if necessary, after
vaginal deliveries followed by PPH if laparotomy is
warranted.
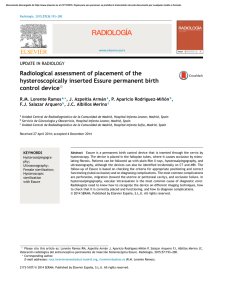
4. Other uterine compression suture
procedures
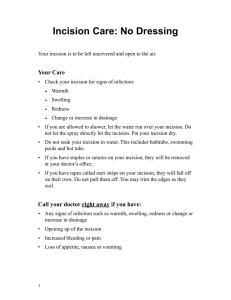
Other techniques, such as that described by Hayman et al [8] and the Cho [9] technique of multiple
square sutures, were developed to oppose the
anterior and posterior uterine walls (Figs. 3 and
4). The Hayman technique is probably quicker to
apply than the cho or B-Lynch techniques in cases
of atonic PPH following spontaneous vaginal delivery, as the lower uterine segment is not opened,
nor the uterine cavity explored. The Hayman
technique, however, runs the risk of allowing blood
to be trapped within the uterine cavity instead of
being expelled freely through the cervix [25]. And
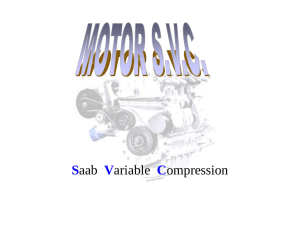
the Cho technique, which pierces the atonic
Figure 4 The Cho multiple-square sutures compressing
anterior to posterior uterine walls [9].
bleeding uterus up to 32 times, may also run the
risk of returning the patient to the operating
theatre. Moreover, by bracing multiple areas of
the uterine body, it could interfere with physiologic
uterine involution and may result in blood-filled
pockets inside the uterine cavity. The Cho technique has been reported to be associated with
pyometra and subsequent hysterectomy [12]. With
these 2 techniques, it is not clear how an even
compression can be applied to both sides of the
uterine body during the procedure. As both techniques are relatively new, worldwide feedback data
about safety, efficacy, and subsequent fertility are
still limited.
5. Conclusions
Postpartum hemorrhage can have diverse causes,
but uterine compression suture techniques have
proved to be valuable in the control of massive PPH
as an alternative to hysterectomy. This review can
make the surgeon aware of their effective application, and of the risks and potential complications
that they may entail.
References
Figure 3 The Hayman uterine compression suture
without opening the uterine cavity [8].
[1] Mousa H, Alffirevic Z. Treatment for primary postpartum
haemorrhage (Cochrane Review). The Cochrane Library,
vol. 1. Oxford7 Update Software; 2003.
The B-Lynch and other compression suture techniques
[2] Mousa H, Walkinshaw S. Major postpartum haemorrhage.
Curr Opin Obstet Gynecol 2001;13:595 – 603.
[3] WHO report of technical working group. The prevention and
management of postpartum haemorrhage. Geneva: World
Health Organisation (1999) WHO/MCH/90-97.
[4] Pahlavan P, Nezhat C, Nezhat C. Hemorrhage in obstetrics and gynecology. Curr Opin Obstet Gynecol 2001;13:
419 – 24.
[5] Department of Health. Why mothers die: report on
confidential enquiries into maternal deaths in the United
Kingdom 2000—2002. London, England7 RCOG Press; 2004.
p. 86 – 93.
[6] Dildy G. Postpartum hemorrhage: new management options.
Clin Obstet Gynaecol 2002;45:330 – 44.
[7] B-Lynch C, Coker A, Lawal A, Abu J, Cowen M. The B-Lynch
surgical technique for the control of massive postpartum
hemorrhage: an alternative to hysterectomy? Five cases
reported. Br J Obstet Gynaecol 1997;104:372 – 5.
[8] Hayman R, Arulkumaran S, Steer P. Uterine compression
sutures: surgical management of postpartum hemorrhage.
Obstet Gynecol 2002;99:502 – 6.
[9] Cho J, Jun H, Lee C. Hemostatic suturing technique for
uterine bleeding during cesarean delivery. Obstet Gynecol
2000;96:129 – 31.
[10] B-Lynch C. B-Lynch brace suture (technical details). Available at: http://www.cblynch.com/HTML/technique.html.
Accessed September 25, 2003.
[11] Chez R, B-Lynch C. The B-Lynch suture for control of
massive postpartum hemorrhage. Contemp Obstet Gynaecol 1998;43:93 – 8.
[12] Ochoa M, Allaire A, Stitely M. Pyometria after hemostatic
square suture technique. Obstet Gynecol 2002;99:506 – 9.
241
[13] Smith K, Baskett T. Uterine compression sutures as an
alternative to hysterectomy for severe postpartum hemorrhage. J Obstet Gynaecol Can 2003;25:197 – 200.
[14] Mazhar S. Management of massive postpartum hemorrhage
by bB-LYNCHQ brace suture. J Coll Phys Surg Pak 2003;13:
51 – 2.
[15] Wergeland H. Use of the B-Lynch suture technique in
postpartum hemorrhage. Tidsskr Nor Laegeforen 2002;
122:370 – 2.
[16] Vangsgaard K. bB-Lynch sutureQ in uterine atony. Ugeskr
Laeger 2000;162:3468.
[17] Ferguson J. B-Lynch suture for postpartum hemorrhage.
Obstet Gynecol 2000;95(6 Pt. 2):1020 – 2.
[18] Dacus J. Surgical treatment of uterine atony employing the
B-Lynch technique. J Matern-Fetal Med 2000;9:194 – 6.
[19] Danso D, Reginald P. Combined B-lynch suture with intrauterine balloon catheter triumphs over massive postpartum
haemorrhage. Br J Obstet Gynaecol 2002;109:963.
[20] Steer P. Correspondence. Br J Obstet Gynaecol 1999;106:286.
[21] Roman A, Rebarber A. Seven ways to control postpartum
haemorrhage. Contemp Obstet Gynecol 2003;48:34 – 53.
[22] Department of Health. Why mothers die: report on
confidential enquiries into maternal deaths in the United
Kingdom 1997—1999. London, England7 RCOG press; 2001.
p. 94 – 103.
[23] Royal College of Obstetricians and Gynaecologists. Placenta
praevia: diagnosis and management. Guideline, vol. 27.
London, England7 RCOG Press; 2001.
[24] Farrell E. Obstetric haemorrhage management guidelines.
J Healthc Prof 2002;6:1 – 7.
[25] B-Lynch C. Correspondence. Br J Obstet Gynaecol 2005;
112:126.
 0
0