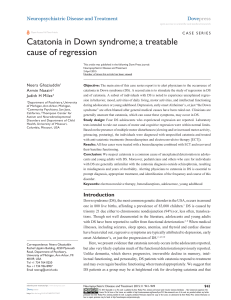
Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie, 41 (1), 2013, 69–74 Z. Kinder-Jugendpsychiatr. F. Häßler Psychother. et al.: Catatonia 41 (1) © 2013 in a 14-Year-Old Verlag Hans Huber, Girl with Hogrefe Schizoph AG , renia Bern http://econtent.hogrefe.com/doi/pdf/10.1024/1422-4917/a000211 - Tuesday, October 04, 2016 8:46:08 PM - IP Address:181.170.215.116 Kasuistik A Case of Catatonia in a 14-Year-Old Girl with Schizophrenia Treated with Electroconvulsive Therapy Frank Häßler1, Olaf Reis1, Steffen Weirich1, Jacqueline Höppner2, Birgit Pohl3, and Johannes Buchmann1 1 Clinic for Child and Adolescent Psychiatry, Neurology and Psychotherapy, University of Rostock, Germany, 2Clinic for Psychiatry and Psychotherapy, University of Rostock, Germany, 3 Clinic for Anaesthesiology, University of Rostock, Germany Abstract. This article presents a case of a 14-year-old female twin with schizophrenia who developed severe catatonia following treatment with olanzapine. Under a combined treatment with amantadine, electroconvulsive therapy (ECT), and (currently) ziprasidone alone she improved markedly. Severity and course of catatonia including treatment response were evaluated with the Bush-Francis Catatonia Rating Scale (BFCRS). This case report emphasizes the benefit of ECT in the treatment of catatonic symptoms in an adolescent patient with schizophrenic illness. Keywords: catatonia, schizophrenia, adolescence, ECT Der Einsatz von EKT bei einer 14-jähigen schizophrenen Patientin mit Katatonie Zusammenfassung. Es wird über den Fall einer 14jährigen schizophrenen Patientin berichtet, die nach der Behandlung mit Olanzapin eine schwere Katatonie entwickelte. Unter einer kombinierten Therapie aus Amantadin, Elektrokrampftherapie (EKT) und gegenwärtig Ziprasidon verbesserte sich ihr Zustand merklich. Schwere und Verlauf der Katatonie wurden mit der Bush-Francis Catatonia Rating Scale (BFCRS) gemessen. Der Fallbericht betont die Nützlichkeit von EKT bei der Behandlung von katatonen Symptomen bei einer adoleszenten schizophrenen Patientin. Schlüsselwörter: Catatonia, Schizophrenie, Adoleszenz, EKT Introduction Despite the first description of catatonia by Kahlbaum in 1874, our knowledge about the phenomenology, diagnosis, etiology, and treatment of catatonia in childhood and adolescence is still scarce. One reason for this scarcity is that in the past catatonia was frequently diagnosed under other labels, such as catalepsy, stupor, and encephalitis lethargica (Shorter, 2012). For adults, catatonia is a well-described syndrome that appears to be underdiagnosed (Fink & Taylor, 2009). Both classification systems, DSM-IV (295.20) and ICD-10 (F 20.2), acknowledge the association of catatonia with schizophrenia. In the upcoming version of DSM5 the direct tie between catatonia and schizophrenia is to be eliminated. The DSM-5 consideration of a fifth digit for a catatonia specifier might be an improvement. The addition of specifiers of this kind, however, has been criticized DOI 10.1024/1422-4917/a000211 in the past (Fink, 2011). The DSM-5 classification acknowledges catatonia as an independent entity for the first time (Fink, Shorter & Taylor, 2010). The current version of DSM (DSM-IV) allows for a classification of catatonia only as derived from affective, other psychiatric, or toxic disorders as well as from organic diseases. Organic diseases as causes of catatonia are mentioned in ICD-10 (F06.1) as well. Symptoms of catatonia vary from positive motoric symptoms, such as excitement, to negative motoric symptoms, such as immobility or stupor. More than 50% of all patients suffering from catatonia display a combination of immobility, mutism, withdrawal, negativism, posturing, grimacing, and rigidity (Rosebush & Mazurek, 2010). Frequencies of catatonia among young patients admitted to psychiatric facilities seem to be lower (0.6–17%) than rates found in adults (7.6–38%) (Cornic, Consoli & Cohen, Z. Kinder-Jugendpsychiatr. Psychother. 41 (1) © 2013 Verlag Hans Huber, Hogrefe AG, Bern 70 F. Häßler et al.: Catatonia in a 14-Year-Old Girl with Schizophrenia Table 1 Similarities and differences of catatonia and NMS http://econtent.hogrefe.com/doi/pdf/10.1024/1422-4917/a000211 - Tuesday, October 04, 2016 8:46:08 PM - IP Address:181.170.215.116 Similarities Differences Catatonia NMS Motor symptoms hypokinesia/akinesia bizarre additional symptoms: posturing, automatisms, negativism, rarely hyperkinesia (stereotypies) only hypokinesia, rigidity, no major behavioral abnormalities Affective symptoms anxieties strong, intense and uncontrollable anxiety less intense and more controllable anxiety Onset slower onset sudden start of mental changes, motor rigidity, fever, and autonomous dysregulation Pathophysiology of motor symptoms right posterior parietal cortical dysfunction blockade of D-2 receptors in striatum with consecutive dysregulation of subcorticalcortical connections in the “motor loop” Pathophysiology of affective symptoms deficits in medial orbitofrontal cortical ac- emotional reaction to akinesia with abnortivity mal subcortical-cortical modulation Treatment first choice: benzodiazepines (BZP), e.g., Lorazepam 1–2 mg up to 20 mg/day second choice in case of nonresponding to BZPs or in case of fever more than 39 °C: ECT third choice – if comorbid with schizophre- no neuroleptics nia: neuroleptics, predominantly atypical neuroleptics while maintaining BZPs – if comorbid with affective disorders: no neuroleptics 2007). For childhood and adolescence, Wing and Shah (2000) described five essential features of catatonia (1–5) and three behavioral abnormalities (6–8): 1. Increased slowness affecting movement and verbal responses 2. Difficulties in initiating and completing actions 3. Increased reliance on physical or verbal prompting by others 4. Increased passivity and apparent lack of motivation 5. Day-night reversal 6. Parkinsonian features 7. Excitement and agitation 8. Repetitive, ritualistic behavior. To evaluate the severity and course of catatonia, including treatment response, in adolescents, the Bush-Francis Catatonia Rating Scale (BFCRS) (Bush, Fink, Petrides, Dowling & Francis, 1996) is seen as the gold standard (Wong, Ungvari, Leung & Tang, 2007). The BFCRS consists of 23 items with 17 items scored on a scale ranging from 0 to 3 and 6 symptoms being scored as either absent or present. The BFCRS is well established in research and practice (Takaoka & Takata, 2003). Nevertheless, the definition of catatonia lacks coherence and clarity. Benzodiazepines are the widely recommended first choice of drugs for the treatment of catatonia (Francis, 2010; Ungvari, Caroff & Gerevich, 2010); second and third choices for treatment are described in Table 1. Treatment differs in third choices according to the comorbid disorder of catatonic symptoms. In case a catatonia is associated with a schizophrenic disorder, a cave has to be avoided, because neuroleptics themselves have been shown to trigger catatonia. The so-called neuroleptic malignant syn- drome (NMS) largely resembles catatonia and was extensively discussed in its relationship to catatonia. The most commonly held opinion is that catatonia and NMS are two entities on the same spectrum (Fink, 1996; Fink & Taylor, 2001). There are now five different hypotheses concerning the nature of the link between the two diagnoses (Vesperini, Papetti & Pringuey, 2010): 1. NMS is a drug-induced form of catatonia. 2. NMS is a drug-induced form of malignant catatonia. 3. NMS and malignant catatonia are the same. 4. Catatonia is a risk factor for NMS. 5. NMS is a heterogeneous syndrome that includes both catatonic and noncatatonic responses to antipsychotic drugs. For a clinician, it becomes difficult to distinguish between these two conditions because many diagnostic criteria overlap. In a retrospective investigation of clozapine, catatonia was diagnosed in 7.4% of patients while in a trial of risperidone 5% of patients showed catatonic symptoms (Ungvari et al., 2010). Both studies did not differentiate between catatonia and NMS, a fact that might explain the high rates of catatonic symptoms observed. About 20 cases of NMS induced by olanzapine have been published (Srivastava, Borkar & Chandak, 2009). Confusion rises if aripiprazole is recommended for the treatment of catatonia (Viktor & Tamas, 2010), which is also known to trigger catatonic symptoms (Shepherd, Garza & De Leon, 2009). For the clinician, the question often arises how to differentiate between symptoms induced by neuroleptics and noninduced symptoms, usually comorbid with an affective or schizophrenic disorder. Table 1 gives an overview of some characteristics we found in the literature (Lee, 2010; Nort- Z. Kinder-Jugendpsychiatr. Psychother. 41 (1) © 2013 Verlag Hans Huber, Hogrefe AG, Bern http://econtent.hogrefe.com/doi/pdf/10.1024/1422-4917/a000211 - Tuesday, October 04, 2016 8:46:08 PM - IP Address:181.170.215.116 F. Häßler et al.: Catatonia in a 14-Year-Old Girl with Schizophrenia hoff, 1996, 2002; Rosebush & Mazurek, 2010), which can help to differentiate between the two forms of catatonia. Comprehensive reviews concerning this issue were given by several authors (Lee, 2010; Takaoka & Takata, 2003; Ungvari et al., 2010) with varying results. Studies such as the one by Carroll, Kennedy, and Goforth (2000) failed to discriminate between catatonia and NMS. Characteristics like those listed in Table 1 might provide a first guideline, although the differentiation between drug-induced and noninduced catatonia remains an open question in our view. In case a catatonia is diagnosed for a patient also suffering from schizophrenia, some issues should be considered (Fink et al., 2010; Kruger, Bagby, Hoffler & Braunig, 2003). First, the association of schizophrenia and catatonia appears only to be moderate: Among adult catatonic patients about 28% were also diagnosed with schizophrenia (Caroff, Mann, Campbell & Sullivan, 2004). In younger patients this association appears to be even weaker. In 89 cases of children and adolescents with catatonia analyzed by Takaoka and Takata (2003), schizophrenia was present in 16.9%. Second, patients with schizophrenic catatonia do not respond well to the treatment with benzodiazepines. A study by Ungvari et al. (2010) reported response rates of 20–30% for schizophrenic patients, while more than 80% of catatonic patients suffering from affective disorders reacted positively to benzodiazepines (Rosebush & Mazurek, 2010). Third, other beneficial medical treatment options were reported for schizophrenic patients, such as antiepileptic drugs or bromocriptine (dopamine agonist). Amantadine (antagonist of the NMDA type glutamate receptor) was also reported to be beneficial (Lee, 2010; Rosebush & Mazurek, 2010; Takaoka & Takata, 2003). In case schizophrenic children or adolescents do not respond to medical treatment, or show a refractory to psychotropic medications, electroconvulsive therapy (ECT) is considered to be an effective treatment alternative (Takaoka & Takata, 2003; Wachtel, Dhossche & Kellner, 2011). Recently, an overview was published regarding responses to ECT in catatonic adult patients (Caroff, Ungvari, Bhati, Datto & O’Reardon, 2007). The authors concluded that acute hypokinetic catatonia is extremely sensitive to ECT, achieving response rates of 67% to 100%. Sienaert, Vansteelandt, Demyttenaere, and Peuskens (2010) found no evidence of a deleterious effect of ultrabrief bifrontal or unilateral ECT on cognitive functioning. A study by Rey and Walter (1997) on children and adolescents found overall efficacy rates of 80% for ECT. For ECT in younger patients it is important to recognize that, compared to adults, children show lower seizure thresholds while ECT seizures last longer (Rey & Walter, 1997). Case Report The patient we report about is a 14-year-old female twin (IQ 53) who at age 12 started to experience visual, haptic, 71 and imperative acoustic hallucinations. Since then she felt anxious and observed, she shook herself and trembled over her whole body. The patient’s thinking was confused, and her thoughts were incoherent. Neurological status, laboratory findings, liquor cerebrospinalis, video-EEG, and cranial MRI remained normal. All findings failed to provide evidence for an organic background to the psychotic symptoms. Developmental disorders were excluded by two experienced psychiatrists. Under combined treatment with behavioral psychotherapy and an oral final dose of 600 mg quetiapine retard, the symptoms of schizophrenia decreased significantly, allowing the patient to be discharged from the hospital. At age 13 psychopathological symptoms slowly returned. Especially acoustic hallucinations and symptoms of anxiety cropped up. At the beginning of 2011, at age 14, our patient had to be treated again as an inpatient. At this point in time, we were confronted with pronounced mood variations and a distinctive affective instability with ambitendencies. An increase of the quetiapine dose (maximum 1200 mg) failed to provide substantial effects. Therefore, we started to change medication to olanzapine interleavingly. One day after the last application of quetiapine (300 mg) and under 20 mg olanzapine the girl became suddenly stiff showing a distinctive rigidity of the extremities and the trunk, also developing a captocormia. Our patient showed severe states of uncontrollable anxiety, restlessness, drivenness, echolalia, verbigerations, excitement, iterations, stereotypies, and a resistance to passive movements. Her thinking and speaking were completely confused and incoherent. Eventually, within 2 days, she developed a catatonic stupor with a waxy flexibility (flexibilitas cerea). The creatinine kinase (CK) increased within these 2 days to 1071 U/l (reference < 109 U/l), myoglobine increased to 171 ng/ml (reference 25–58 ng/ml). Other laboratory findings remained unchanged (liquor cerebrospinalis, parameters of coagulation and inflammation, liver enzymes, potassium, sodium, chloride), just as did temperature, blood pressure, respiratory rate, diaphoresis, and other vegetative parameters. However, a constant trembling of the whole body was remarkable. A repetition of EEG and cMRI did not provide any new results. An intravasal application of biperidene to evaluate extrapyramidal side effects provided no results. At this time, the hypothesis of an NMS was built, despite the fact that an increase of the CK does not provide a valid indicator (Lee, 2010). With the differential diagnosis of a NMS, all neuroleptics were removed Table 2 Sum scores of the BFRCS during the catatonic stupor state of the girl, starting with the first day of the rigidity (minimal 0, maximum 66); b = biperidene, d = diazepam, l = lorazepam, h = haloperidol Day BFRCS 1 30 2 (b) 42 3 (d) 45 5 (l) 51 7 (l + h) 40 10 12 45 48 Z. Kinder-Jugendpsychiatr. Psychother. 41 (1) © 2013 Verlag Hans Huber, Hogrefe AG, Bern 72 F. Häßler et al.: Catatonia in a 14-Year-Old Girl with Schizophrenia http://econtent.hogrefe.com/doi/pdf/10.1024/1422-4917/a000211 - Tuesday, October 04, 2016 8:46:08 PM - IP Address:181.170.215.116 Table 3 Course during treatment with ECT Date ECT bitemporal 08.02.2011 Energy set 10% Charge delivered 49.3 mC Current 0. 90 A Stimulus duration 5.6 s Pulse width 0.50 ms Frequency 10 Hz 09.02.2011 Epileptic seizure/duration Bush-Francis Catatonia Rating Scale Remarks/medication 84 s 37 Lorazepam 2 × 2 mg Haloperidol 3 × 5 mg i.v., Clexane 20 mg s.c. No changes 121 s 36 No changes 10.02.2011 No changes 29 s 37 + Antibiotics and Iron 11.02.2011 No changes 20 s 35 Moving to pediatric emergency unit, Amantadine 600 mg/day 14.02.2011 Energy set 15% Charge delivered 75.4 mC Current 0.90 A Stimulus duration 5.6 s Pulse width 0.50 ms Frequency 20 Hz 250 s 36 Amantadine 900 mg/day 16.02.2011 No changes 108 s 26 No changes 18.02.2011 No changes 152 s 24 No changes 21.02.2011 No changes 210 s 25 No changes 23.02.2011 No changes 145 s 21 No changes 25.02.2011 Energy set 10% Charge delivered 49.3 mC Current 0. 90 A Stimulus duration 5.6 s Pulse width 0.25 ms Frequency 10 Hz 51 s 01.03.2011 No changes 32 s 19 Lorazepam 3 × 0.5 mg Amantadine 2× 200 mg/day In days with ECT without morning doses of any drugs. 04.03.2011 No changes 54 s 19 No changes 08.03.2011 No changes 32 s 8 11.03.2011 Energy set 15% Charge delivered 75.4 mC Current 0. 90 A Stimulus duration 5.6 s Pulse width 0.50 ms Frequency 20 Hz 97 s 12 No changes 16.03.2011 Energy set 15% Charge delivered 75.4 mC Current 0. 90 A Stimulus duration 4.2 s Pulse width 0.50 ms Frequency 20 Hz 183 12 Lorazepam 3 × 0.5 mg, Ziprasidone 2 × 20 mg/day on days with ECT without morning doses. 23.03.2011 No changes 222 9 Lorazepam 3 × 0.5 mg, Ziprasidone 60 mg/day, Amantadine 2 × 200 mg/day on days with ECT without morning doses of any drugs. No changes Z. Kinder-Jugendpsychiatr. Psychother. 41 (1) © 2013 Verlag Hans Huber, Hogrefe AG, Bern No changes in medication, transfer back to the clinic for child and adolescent neuropsychiatry http://econtent.hogrefe.com/doi/pdf/10.1024/1422-4917/a000211 - Tuesday, October 04, 2016 8:46:08 PM - IP Address:181.170.215.116 F. Häßler et al.: Catatonia in a 14-Year-Old Girl with Schizophrenia and the girl was treated solely with benzodiazepines (3 × 10 mg diazepam). Within two days, the CK returned to a normal degree, but the catatonic stupor and a significant impairment of vigilance and communication abilities with a pronounced staring remained. At this point, the diagnosis was rechanged to catatonic schizophrenic stupor because catatonia had started as a mix of behavioral symptoms, not only as hypokinesia (see Table 1). Neither diazepam nor lorazepam (3 × 2 mg) improved the status markedly. Because of the primary schizophrenia we started a reattempt with haloperidol (3 × 10 mg) as an ultima ratio, but failed again. Table 2 shows the daily total scores of the BFCRS during this time. On day 16 after the beginning of the rigidity, we commenced bitemporal ECT (Thymatron® System IV with GenieTM IV EEG analysis software) with a cluster of daily treatments over 4 days. To reduce side effects, especially cognitive dysfunctions, we used ECT treatment techniques that in adults have proved to result in smaller short- or long-term memory deficits (Sackeim et al., 2007). In particular, we stimulated her with brief pulse form. An individual electrical dosage titration was done at the beginning of the first ECT session. There were no major effects, but an acute exacerbation of schizophrenic symptoms was seen at the beginning of ECT. For that reason, we started with an accompanying amantadine therapy (3 × 200 mg). With this add-on we aimed at a beneficial effect as reported by Carroll, Goforth, and Thomas (2007). After the patient started to show signs of malnutrition and a beginning pneumonia with light to moderate febrile temperature, she was transferred temporarily to a pediatric emergency unit where antibiotics were added to the treatment. No autonomic abnormalities appeared further on. Bitemporal ECT was continued three times a week for the next six treatment episodes, then twice a week for another four treatment episodes, and finally once per week for two maintaining treatment episodes. Lorazepam and amantadine treatment was continued over this time period with the patient showing slow improvement of the motor and the psychopathological state. After 12 treatments, the girl showed significant improvement; she started to move (answered with little movement or tone) and became more verbal. ECT was finished after 16 treatments. Catatonic symptoms were no longer evident, though the visual, haptic, and imperative acoustic hallucinations returned, again associated with marked fear. After careful consideration we decided to start again with a neuroleptic therapy. With a dose of 40 mg (2 × 20 mg) ziprasidone we saw an intermediate elevation of the CK, with a maximum of up to 496 U/l. Under a dose of 20–40 mg ziprasidone our patient no longer hallucinated, showing a markedly reduced anxiety with psychopathological and motor status being almost normal. Table 3 shows the course during treatment with ECT inclusive technical parameters. 73 Discussion The patient reported here was a female adolescent with mild mental retardation who exhibited severe catatonia. She was successfully treated with amantadine HCL, ECT, and is currently being treated solely with ziprasidone. Improvement was noted after 12 ECT episodes. In sum, she received a total of 16 ECT episodes. Our case report is in line with the investigation by Girish and Gill (2003). In their study 14 patients with nonaffective, nonorganic catatonia who did not respond to benzodiazepines improved rapidly under ECT. Catatonic symptoms in this study, however, disappeared more quickly than in our case. We observed a catatonic status with a prominent stupor combined with waxy flexibility persisting over 7 weeks. Alterations of excitement were first seen after the 12th ECT episode. With regard to the young age of our patient initial seizure thresholds (IST) were set at a lower level (49.3 mC and 75.4 mC), compared to IST in bilateral ECT in adults (111.6 mC) as reported by Waarde, Verwey, and Mast (2009). The treatment with antipsychotics is in line with more recent strategies reported by Caroff et al. (2007) and Rosebush and Mazurek (2010). However, the role of antipsychotic drugs in catatonia remains unclear to date and has been studied insufficiently. We argue here that antipsychotics may be effective in some cases. They should, however, be handled with greatest care because they may rechallenge catatonic episodes (Lee, 2010). We agree with Francis (2010), who proposed a cautious trial of these agents and careful monitoring for catatonic symptoms. Unfortunately, schizophrenic catatonia proves to be a severe condition in young people, with 10% mortality at 4year follow-up (Cornic et al., 2007), caused by either suicide (n = 2) or by medical conditions (n = 1). In other words, the course of our patient remains uncertain, despite the marked reduction of psychopathology and catatonic symptoms. For severe cases of schizophrenic catatonic stupor refractory to pharmacological treatment, we suggest an intensive and, if necessary, long-lasting ECT sequence – even in adolescents. In our case we saw no memory impairment as measured with the Working Memory Index of the Wechsler Scales for children. In sum, we regard ECT as a valuable second-choice treatment option (see Table 1) in adolescents with schizophrenic catatonic stupor. References Bush, G., Fink, M., Petrides, G., Dowling, F. & Francis, A. (1996). Catatonia. I. Rating scale and standardized examination. Acta Psychiatrica Scandinavica, 93, 129–136. Caroff, S. N., Mann, S. C., Campbell, E. C. & Sullivan, K. A. (2004). Epidemiology. In S. N. Caroff, S. C. Mann, A. Francis & G. L. Fricchione (Eds.), Catatonia: From psychopathology to neurobiology (pp. 12–23). Washington, DC: American Psychiatric Press. Z. Kinder-Jugendpsychiatr. Psychother. 41 (1) © 2013 Verlag Hans Huber, Hogrefe AG, Bern http://econtent.hogrefe.com/doi/pdf/10.1024/1422-4917/a000211 - Tuesday, October 04, 2016 8:46:08 PM - IP Address:181.170.215.116 74 F. Häßler et al.: Catatonia in a 14-Year-Old Girl with Schizophrenia Caroff, S. N., Ungvari, G. S., Bhati, M. T., Datto, C. J. & O’Reardon, J. P. (2007). Catatonia and prediction of response to electroconvulsive therapy. Psychiatric Annals, 37, 57–67. Carroll, B. T., Goforth, H. W. & Thomas, C. (2007). Review of adjunctive glutamate antagonist therapy in the treatment of catatonia syndromes. Journal of Neuropsychiatry and Clinical Neuroscience, 19, 406–412. Carroll, B. T., Kennedy, J. C. & Goforth, H. W. (2000). Catatonic signs in medical and psychiatric catatonias. CNS Spectrum, 5, 66–69. Cornic, F., Consoli, A. & Cohen, D. (2007). Catatonia in children and adolescents. Psychiatric Annals, 37, 19–26. Fink, M. (1996). Neuroleptic malignant syndrome and catatonia. One entity or two? Biological Psychiatry, 39, 1–4. Fink, M. (2011). Catatonia from its creation to DSM-5: Considerations for ICD. Indian Journal of Psychiatry, 53, 214–217. Fink, M., Shorter, E., & Taylor, M. A. (2010). Catatonia is not schizophrenia: Kraepelin’s error and the need to recognize catatonia as an independent syndrome in medical nomenclature. Schizophrenia Bulletin, 36, 314–320. Fink, M., & Taylor, M. A. (2001). The many varieties of catatonia. European Archives of Psychiatry and Clinical Neurosciences, 251 (Suppl. 1), 1/11–1/13. Fink, M., & Taylor, M. A. (2009). The catatonia syndrome. Forgotten but not done. Archives of General Psychiatry, 66, 1173–1177. Francis, A. (2010). Catatonia: Diagnosis, classification, and treatment. Current Psychiatry Report, 12, 180–185. Girish, K. & Gill, N. S. (2003). Electroconvulsive therapy in lorazepam nonresponsive catatonia. Indian Journal of Psychiatry, 45, 21–25. Kruger, S., Bagby, R. M., Hoffler, J. & Braunig, P. (2003). Factor analysis of the catatonia rating scale and catatonic symptom distribution across four diagnostic groups. Journal of Comprehensive Psychiatry, 44, 472–482. Lee, J. W. Y. (2010). Neuroleptic-induced catatonia. Clinical presentation, response to benzodiazepines, and relationship to Neuroleptic Malignant Syndrome. Journal of Clinical Psychopharmacology, 30, 3–10. Northoff, G. (1996). Neuroleptic malignant syndrome and catatonia: One entity or two? Biological Psychiatry, 40, 431–432. Northoff, G. (2002). Catatonia and neuroleptic malignant syndrome: psychopathology and pathophysiology. Journal of Neural Transmission, 109, 1453–1467. Rey, J. & Walter, G. (1997). Half a century of ECT use in young people. American Journal of Psychiatry, 154, 595–602. Rosebush, P. I. & Mazurek, M. F. (2010). Catatonia and its treatment. Schizophrenia Bulletin, 36, 239–242. Sackeim, H. A., Prudic, J., Fuller, R., Keilp, J., Lavori, P. W. & Olfson, M. (2007). The cognitive effects of electroconvulsive therapy in community settings. Neuropsychopharmacology, 32, 244–254. Shepherd, J., Garza, V. M. & De Leon, O. A. (2009). Waxing-and waning catatonia after intermittent exposure to aripiprazole in a case of autism and bipolar disorder (letter). Journal of Clinical Psychopharmacology, 29, 503–504. Shorter, E. (2012). Making childhood catatonia visible, separate from competing diagnoses. Acta Psychiatrica Scandinavica, 125, 3–10. Sienaert, P., Vansteelandt, K., Demyttenaere, K. & Peuskens, J. (2010). Randomized comparison of ultra-brief bifrontal and uni- lateral electroconvulsive therapy for major depression: Cognitive side effects. Journal of Affective Disorder, 122, 60–67. Srivastava, A., Borkar, H. A. & Chandak, S. (2009). Olanzapineinduced neuroleptic malignant syndrome in a patient with paranoid schizophrenia. Journal of Psychiatry and Clinical Neuroscience, 63, 119–121. Takaoka, K. & Takata, T. (2003). Catatonia in childhood and adolescence. Journal of Psychiatry and Clinical Neuroscience, 57, 129–137. Ungvari, G. S., Caroff, S. N. & Gerevich, J. (2010). The catatonia conundrum: Evidence of psychomotor phenomena as a syndrome dimension in psychotic disorders. Schizophrenia Bulletin, 36, 231–238. Vesperini, S., Papetti, F. & Pringuey, D. (2010). Are catatonia and neuroleptic malignant syndrome related conditions? Encephale, 36, 105–110. Viktor, V. & Tamas, T. (2010). The use of aripiprazole in the treatment of catatonia. Neuropsychopharmacologica Hungarica, 12, 373–376. Waarde, J. A. van, Verwey, B. & Mast, R. C. van (2009). Metaanalysis of initial seizure thresholds in electroconvulsive therapy. European Archives of Psychiatry and Clinical Neuroscience, 259, 467–474. Wachtel, L. E., Dhossche, D. M. & Kellner, C. H. (2011). When is electroconvulsive therapy appropriate for children and adolescents. Medical Hypotheses, 76, 395–399. Wing, L. & Shah, A. (2000). Catatonia in autistic spectrum disorders. British Journal of Psychiatry, 176, 357–336. Wong, E., Ungvari, G. S., Leung, S. K. & Tang, W. K. (2007). Rating catatonia in patients with chronic schizophrenia: Rasch analysis of the Bush-Francis Catatonia Rating Scale. International Journal of Methods in Psychiatric Research, 16, 161–170. Initial Date Submitted Date Revision Submitted January 23. 2012 May 3, 2012 Disclosures of interest of Dr. Häßler concern the following positions: Advisory Board for Eli Lilly GmbH Germany, Janssen-Cilag, Research Support from Novartis Pharmaceuticals, Bayer Vital, Travel Grants from Novartis Pharmaceuticals, AstraZeneca Pharmaceutical, Bayer Vital, consulting fees from Janssen-Cilag, Novartis Pharmaceuticals, Bayer Vital. All other authors declare that they have no conflicts of interest concerning financial or personal involvement with other people or organizations that could have had an interest in the outcome of the study. Dr. Olaf Reis Forschungsabteilung Klinik für Psychiatrie, Neurologie, Psychosomatik und Psychotherapie im Kindes- und Jugendalter der Universität Rostock Gehlsheimer Straße 20 18147 Rostock Deutschland [email protected] Z. Kinder-Jugendpsychiatr. Psychother. 41 (1) © 2013 Verlag Hans Huber, Hogrefe AG, Bern