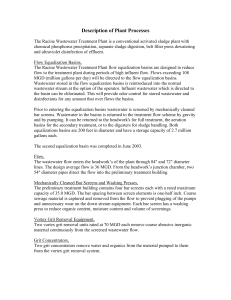
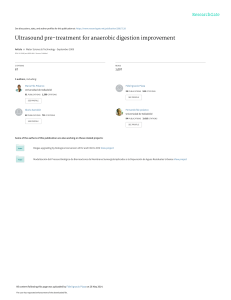
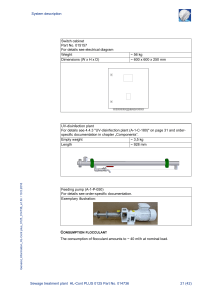
MEDICALLY USED RADIONUCLIDES IN S E W A G E S L U D G E B. ERLANDSSON* and S. MATTSSON Technical Department, Personnel Health Care, City of MalmO, S-220 02 MalmO, Sweden. and Department of Radiation Physics, MalmO General Hospital, S-214 O1MalmO, Sweden (Received 17 May, 1977; revised 25 August, 1977) Abstract. The concentration of medically used radionuclides has been studied in sludge from the sewage treatment plant serving the borough of Malta0. In this area all nuclear medicine procedures are carried out in one hospital and almost all patients live in the borough. Therefore, the input of medically used radionuclides into the sewage system can be estimated with good accuracy. Samples of digested sludge have been tal(en once or twice a week during half a year. Iodine-131 (physical half life (T) = R.05 d) was detected in all samples. The 13q-activity concentration due to medical use varied between (0.034-0.01) and (0.124-0.02) nCi kg -1. The ratio between the total output of 13tI via the sludge and an adherent input of the radionuclide into the sewage system was determined to (2.6 + 0.6) × 10-3, which is equivalent to a ratio of (2 + 1) × 10-2 for stable I. Occasionally measurable activities of 198Au (T= 2.7 d) and 201T1(T= 3.1 d) have been found. The radioactivity concentration of medically used radionuclides in the sludge is low and constitutes no health problems for the persons involved. The sludge however has proved to be a very sensitive and suitable integrator of radioactive material released from a large urban area. 1. Introduction The use of radionuclides in medicine leads to the release of radioactivity in the wastes from different hospital laboratories and from the excreta of patients inside and outside the hospital. The need to control excreta from patients who have received therapeutic activities of radionuclides, e.g., 10 to 100 mCi of 13xI, has long been recognized, but very few direct measurements in sewage systems have been made (Moss, 1973; Sodd et al., 1975). During the last years, there has been a large increase in the number of patients who have been investigated with the widening range of radiopharmaceuticals clinically available. The activities used can be of the order of 15 mCi 99Tcm for brain and sceletal scintigraphy as well as for circulation studies, 2 to 3 mCi 99Tcm for liver and lung scintigraphy, and 2 mCi 2°1T1for myocard studies, etc. The concentration of various medically used radionuclides in the sewage system and in the recipient has hitherto mainly been estimated according to very rough theoretical models, and there is a growing need to control such estimates by measurements. The borough of Malm0 has unique features for such a study. All nuclear medicine *Present address: Department of Nuclear Physics, University of Lund and Lund Institute of Technology, S-223 62 Lund, Sweden. Water, Air, and Soil Pollution 9 (1978) 199-206. All Rights Reserved Copyright © 1978 by D. ReideI Publishing Company, Dordrecht, Holland 200 B.ERLANDSSONANDS. MATTSSON procedures are carried out in one hospital and almost all patients live in the borough, which has one main sewage treatment plant. Thus the excreta from the patients reach the same treatment plant both when they are in hospital and in their homes. Thus we have good information about the input of medically used radionuclides in the Sewage system. 2. Description of the Sewage System The sewage from about 225 000 of the 250 000 inhabitants of the borough of MalmO is treated at SjOlunda in the northern part of MalmO at the Sound (Figure 1), and only 10% of the sewage, from about 25 000 inhabitants, is treated at a smaller plant. To the SjOlunda plant is also connected the sewage system of the boroughs of Lomma and BurlOv, and parts of Staffanstorp (totally 25 000 inhabitants). The total serviced area is 134 km 2, but only parts of this area are overbuilt and certain parts are serviced by a duplicate system in which rainwater passes directly into the sea without passing the sewage treatment plant. The overbuilt area from which the rainwater passes through the SjOlunda plant is therefore only about 28 km 2. The sewage treatment plant is constructed to give partial biological cleaning. The Fig. 1. M a p over M a l m 0 with neighbourhood and the collecting area of Sj01unda sewage treatment plant. 201 M E D I C A L L Y U S E D R A D I O N U C L I D E S IN SEWAGE S L U D G E SEWAGE WATER SEDIMENTATION SLUDGE ~3] SLUDGE SLUDGE~ SLUDGE 0.5-1 d,m~RESERVOIRS 4-7 °/odin. DIGESTER ~/o / / WATER / / / BC O ILL IG AL EO AG NN IC WATER DIGESTEDsLuDGE l =4%d'm' //SLUDGE I PRESS DIGESTED SLUDGE =z, °/o " d.m.1 ESERVOIR DIGESTED SLUDGE 2 0 - 2 5 % d.m. d.m. = dry m a t e r i a l Fig,2. Block diagram of the Sj01undasewagetreatment plant. main part of the sewage passes through the plant in about 5 h. Figure 2 shows schematically how the sewage water is processed. During a month about 3.2 × 106 m 3 of the waste water reaches the plant. The sewage sludge is pumped from the sedimentation reservoir (1) to a reservoir (2) where some of the water is separated and then to the sludge digesters. These consist of two parallel blocks of chambers (3) with a total volume of 11 300 m 3. When the volume of digested sludge increases, part of it is pumped to a tank with a volume of 5 000 m 3 (4) and from this tank, part of the sludge is removed periodically. This sludge is compressed (5) so that the content of dry substance increases to 20 to 25%, with a mean value of 23%, and is then transported to different users. A mean volume of 1 320 m 3 of digested sludge leaves the plant every month. In this work we have studied the radioactivity concentration in this final f o r m of digested sludge. 3. Radionuclide Sources The most important source for radionuclides found in the Sj 01unda sewage treatment plant is together with artificial- and natural fall-out the effluent from Malm0 General Hospital. The activity of various radionuclides, which during one year are administered to patients for radiotherapy and diagnostic procedures, is given in Table I. The radionuclides 90y and 198Au are normally injected into body cavities to produce a local 202 B. ERLANDSSON AND S. MATTSSON TABLE I Activity of radionuclides which were administered to patients during one year (1976) For radiotherapy Radionuclide For diagnostics (in vivo procedures) T Activity per year Radionuclide T Activity per year 32p 14.3 d 0.04 Ci (1 GBq) 85Sr 65.1 d 0.03 Ci (1 GBq) 9oy 1311 198Au 2.67 d 8.05 d 2.70 d 0.06 Ci (2 GBq) 1.3 Ci (0.05 TBq) 0.3 Ci (0.01 TBq) 99Tcm* 131I 133Xe 6.03 h 8.05 d 5.27 d 32 Ci (1.2 TBq) 0.03 Ci (1 GBq) 3 Ci (0.1 TBq) 2°iT1 73.5 h 0.2 Ci (7 GBq) *As radionuclide impurities 0.008 Ci 188Re (16.8 h), 0.001 Ci 99Mo (66.7 h), 0.003 Ci 186Re (88.9 h), etc. For in vitro diagnostics: 0.4 Ci 125I (60.2 d). irradiation and the leakage from these cavities is normally very small. Therefore these radionuclides are expected to be found in measurable amounts in the sewage water only in connection with accidents and post-mortem examinations of treated patients. The medically used radionuclide which is supposedto be easily detected in the present study is 1311.Normally about two thirds of the orally given activity is excreted via the urine of the treated patients in the first 24 h and smaller fractions subsequently. Concerning the radionuclides used for nuclear diagnostics 99Tcm and 2°1T1 might be found in various parts of the sewage system. Because of the short physical halflife of 99TCm, this radionuclide is not supposed to appear in detectable concentrations in the digested sewage sludge. 4. Sample Collection and Measurement Samples of digested sludge were collected once a week from the beginning of July 1976 to the end of January 1977. From mid-October to mid-December the sludge was collected twice a week. The sludge was packed in a 2 000 ml cylindrical plastic can (~b= 116 mm, height = 190 mm), which was filled up. The can was placed with its central axis perpendicular to the central axis of a 46 cm 3 Ge(Li)-detector. The distance between the center of the sample and the detector end window was 9 cm. The Ge(Li)-spectrometer provided a good energy resolution (FWHM = 1.99 keV at 1.33 MeV). The detector and the sample were housed in a lead cave with 8 cm thick walls. The detection efficiency for photons of various energies was determined from measurements on water solutions containing known activities of 22Na, 57Co (The Radiochemical Centre, Amersham, England), and 152Eu (Laboratoire de Metrologie des Rayonnements Ionisants, Gif-sur-Yvette, France) in the same plastic cans as the sludge samples. The counting time was normally 54 000 s (15 h) or 80 000 s ( ~, 22.2 h) MEDICALLYUSEDRADIONUCLIDESIN SEWAGESLUDGE 203 per sample. The minimum detectable activity (ICRU, 1972) of 131Iin a typical sewage sludge sample was with these counting times about 28 pCi and 23 pCi respectively. 5. Result and Discussion 5.1. IODINE-131 Figure 3 shows the 1311activity concentration (nCi kg "1) in the digested sludge ("~ 23 % dry substance) together with the estimated release of 131I (mCi) into the sewage system. For each treated patient the release has been calculated from information on activity administered and from earlier determined individual values on the urinary excretion of 131I. At the beginning of December 1976 minor activities from patients treated at the university hospital in Lund were released into the system. This has been accounted for. The curve shows two peaks which can be connected with known release of 131I into the system. The first one occurs around 20 August arising from a single input of about 36 mCi during the first days of the month. The maximum activity of 131I is measured about 2 to 3 weeks after the release. The other peak around 26 October [(0.42+0.01)nCi kg -1] is probably due to a nuclear weapon test in the atmosphere 131I-coneentration in digested sludge nCi.kg -1 0.5 I r I I "China 09 26 . I . . . TT I I China 11 17" I 0.4 0.3 131I-activity in e x c r e t a from rnCi (staptes) patients ~ 30 0.2 20 0.1 10 0 August 1976 Fig. 3. September October November December January 1977 131I-activity concentration in digested sludge (left ordinate) and estimated daily release of 131I from patients (right ordinate) during the period August 1976 to January 1977. B. ERLANDSSONAND S. MATTSSON 204 over the western parts of the People's Republic of China on 26 September, 1976. Short lived fission products were first registered in surface air over Sweden during the week 4-11 October (DeGeer, 1976). A third bump occured in December. Because no increase of other fission products than 131I is seen from another Chinese nuclear weapon test on 17 November, (Erlandsson and Mattsson, 1978), the 131I-peak in December might be explained by the release of 1311caused by medical use. For 131Iit is now possible to calculate the ratio between the output to the digested sludge and the input to the sewage system. The output data have been compared with input data 18 d earlier to account for the dwelling time in the sludge digester. The results are presented in Table II. The second part of this table refers to the bomb fall-out. In situ deposition measurements at Barseb~ick 20 km north of Malmt~ on 1976-10-29 gave the value (1.1+0.2)nCi m -2, (Finck et al., 1977). With a collecting area of 28 km 2 and complete run off this gives an input of 208 mCi (this activity value refer to 1976-10-07). When the output was calculated, a constant 'hospital' background of 0.06 kg -1 was subtracted. The background was estimated using the input from the General Hospital during the period 1976-09-20 to 1976-10-20, the output of digested sludge and an output-input factor of 2.6 × 10-3. This gives a factor of 1.6 × 10 -3 between output and input of 1311from the China bomb which is in good agreement with the mean value for the release from the hospital, which is (2.6+0.6) × 10 -3. The mass ratio of outcoming sludge and the incoming sewage water to Sj01unda is 4.1 × 10-4. Thus the ratio between 131I concentration in the digested sludge and in the input sewage water is about 6. If we assume that all I behaves in the same way, the data for 1311can be used to estimate the situation for other I isotopes by correcting for the different physical half-life and thus the different residence time in the sludge digesters. If 1251is released into the sewage system 1.5 % of the activity will leave the sewage plant via the sludge, TABLE I1 The ratio between output and inl~ut (18 days earlier) of 1311 in the Sj01unda sewage treatment plant Time period Input (mCi) Release from the hospital: 760715-760915 760802-761003 87.0 761112~770101 761130-770118 O u t p u t (mCi) Output/input 2.0 x 10 -3 0.174 47.1 3.1 × 10 -3 0.145 M e a n value 2.6 x 10 -3 B o m b fallout 761005-761029 761017-761119 224 0.365 1.6)< 10 -3 MEDICALLY USED RADIONUCLIDES IN SEWAGE SLUDGE 205 which has its maximum 125I concentration after around 20 days. If 129I or stable I is released, about 2°7o will be found in the sludge with maximum concentration after around 28 days. The ratio between 1291 or stable I concentration in the digested sludge and in the input sewage water is about 50. In the work by Sodd et al. (1975) there was a remarkable discrepancy between the activity administered to the patients (10 to 20 mCi per week) and the activity found in the effluent from the sewage treatment plant (93 mCi per week). This discrepancy was explained as arising from outlets from other radionuclide users in the area. This explanation would call for a release 4 to 5 times greater than the medical. In view of our results a possible explanation could be that this increased activity is partly due to fall-out from a nuclear weapon test over the People's Republic of China on 27 June, 1973. 5.2. OTHER RADIONUCLIDES The presence of 6ther medically used radionuclides than 131I has been detected only occasionally. Normally, the activity concentration of 19SAuwas below the minimum detectable, which is 0.014 nCi kg"x(counting time: 8 × 104 s). On 27 August the sludge contained (0.069 + 0.005) nCi kg-1, and one week later on 3 September (0.030 + 0.004) nCi kg-1. After one more week 198Auwas not detectable. Our result indicates that there was a release of 198Au around 15 August. The most likely explanation to this release is a post-mortem examination on 18 August of a patient, who 7 days earlier had received 125 mCi of 198Au-colloid for therapy. Upon examination the body contained about 20 mCi of 19SAu. As the leakage of the radionuclide at the autopsy is very difficult to estimate, no sure output/input ratio can be given in this case. In one sample of digested sludge, from 17 January, 1977, measurable content of 2°lT1 (0.19 nCi kg-1) was registered. Both the 165 keV, and the Hg X-ray peaks appeared in the gamma-spectrum. Normally the 2°iT1 activity concentration was below the minimum detectable which is 0.15 nCi kg-1. As a mean around 0.7 mCi of SSSr is administered to patients every week. This gives an estimated weekly release of about 0.2 mCi to the sewage system. During certain periods much ihigher counting rates in the 514 keV peak than normally found have been recorded. This is difficult to explain because the input activity of 85Sr per week is almost constant which should cause a constant activity concentration in the sludge. An explanation is that other radionuclides also emitting 514 keV gamma-rays tempo r a r ily disturb the 85Sr measurements. Further investigations along this line are in progress (Erlandsson and Mattsson, 1978). 6. S u m m a r y and C o n c l u s i o n Iodine-131 was detected in all samples of digested sludge collected in Malm0 sewage treatment plant. Due to the medical use of the radionuclide the activity concentration 206 B. ERLANDSSON AND S. MATTSSON in the sludge varied between 0.03 and 0.12 nCi kg-1. A single 200 kton nuclear weapon test in China gave a maximum value of 0.42 nCi kg "1 about 40 days after the test. The ratio between the total output of 131I via the sludge and the input of 131I into the sewage system is (2.6+0.6) × 10-3, which is equivalent to a ratio of ( 2 + 1) × 10-2 for stable I. The 131I-content in the sludge due to medical use of the radionuclide is low and does not introduce any radiation protection problems for the persons working at the sewage treatment plant. At present the urine from patients receiving 100 mCi or more of 131I is stored for around 25 days in the hospital. Because the hospital staff has to handle the urine bags this storage will probably give a higher collective dose than if it was flushed into the sewage immediately. Therefore it is proposed that all urine from therapy patients is flushed into the sewage system without any storage. The small amount of other medically-used radionuclides found in the sludge is insignificant. This work however shows that digested sludge from a sewage treatment plant is a very sensitive and suitable integrator of reasonably longlived radioactivity released from a large urban area. Acknowledgments The authors acknowledge T. Bramst~ng, C. Pettersson, and B. Nosslin, MalmO General Hospital, for valuable information, fruitful discussions and support. They also appreciate the valuable information about the sewage system and the SjOlunda sewage treatment plant given by P. Ansner, L. Linde and A. Zimmergren. References DeGeer, L-E.: 1976, Private communication. The Research Institute of National Defence, Sundyberg, Sweden. Erlandsson, B. and Mattsson, S.: 1978, to be published. Finck, R., Lid6n, K., and Persson, R. B. R.: 1977, Paper presented at the IRPA IV Int. Congress, Paris, 24-30 April, 1977. International Commission on Radiation Units and Measurements: 1972, Measurement of Low-Level Radioactivity, Report 22, ICRU, Washington, D.C., U.S.A. Moss, C. E.: 1973, Health Phys. 25, 197. Sodd, V. J., Velten, R. J., and Saenger, E. L.: 1975, Health Phys. 28, 355.

![Tríptico del curso [PDF 450KB]](http://s2.studylib.es/store/data/006258131_1-103c5de49e5ed6e7b549fd7206c4fb9a-300x300.png)