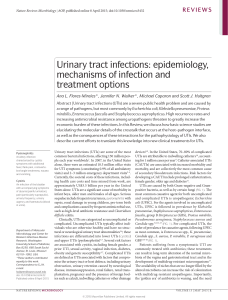
Pediatr Nephrol (2016) 31:1253–1265 DOI 10.1007/s00467-015-3168-5 EDUCATIONAL REVIEW Acute pyelonephritis in children William Morello 1 & Claudio La Scola 1 & Irene Alberici 1 & Giovanni Montini 2 Received: 12 November 2014 / Revised: 22 June 2015 / Accepted: 30 June 2015 / Published online: 4 August 2015 # IPNA 2015 Abstract Acute pyelonephritis is one of the most serious bacterial illnesses during childhood. Escherichia coli is responsible in most cases, however other organisms including Klebsiella, Enterococcus, Enterobacter, Proteus, and Pseudomonas species are being more frequently isolated. In infants, who are at major risk of complications such as sepsis and meningitis, symptoms are ambiguous and fever is not always useful in identifying those at high risk. A diagnosis of acute pyelonephritis is initially made on the basis of urinalysis; dipstick tests for nitrites and/or leukocyte esterase are the most accurate indicators of infection. Collecting a viable urine Key summary points (1) Very young children with acute pyelonephritis have ambiguous symptoms and are at major risk of complications. The presence of fever is not helpful in identifying high-risk infants. (2) Collecting a correct urine sample for urine culture using clean voided methods is reliable and effective, even in infants. (3) Oral antibiotic treatment is recommended in well-appearing children, while hospital admission and intravenous therapy are suggested for children in bad clinical condition and for newborns. (4) The usefulness of a full imaging work-up after a first fUTI is questioned. The new guidelines suggest less aggressive imaging strategies, to reduce radiation exposure and costs. (5) The efficacy of antibiotic prophylaxis in preventing recurrence is still a matter of debate, even in patients with VUR. It seems to reduce the rate of recurrence, but with no influence on the appearance of kidney scarring. The risk of antibiotic resistance is a warning against its routine use. * Giovanni Montini [email protected] 1 Nephrology and Dialysis Unit, Department of Pediatrics, Azienda Ospedaliero Universitaria Sant’Orsola-Malpighi, Via Massarenti 11, 40138 Bologna, Italy 2 Pediatric Nephrology and Dialysis Unit, Department of Clinical Sciences and Community Health, University of Milan Fondazione IRCCS Cà Granda -Ospedale Maggiore Policlinico Via della Commenda, 9 20122 Milano, Italy sample for urine culture using clean voided methods is feasible, even in young children. No gold standard antibiotic treatment exists. In children appearing well, oral therapy and outpatient care is possible. New guidelines suggest less aggressive imaging strategies after a first infection, reducing radiation exposure and costs. The efficacy of antibiotic prophylaxis in preventing recurrence is still a matter of debate and the risk of antibiotic resistance is a warning against its widespread use. Well-performed randomized controlled trials are required in order to better define both the imaging strategies and medical options aimed at preserving long-term renal function. Keywords Urinary tract infections . Acute pyelonephritis . Vesicoureteral reflux . Guidelines . Antibiotic prophylaxis . Antibiotic resistance Abbreviations AAP American Academy of Pediatrics AP Acute pyelonephritis CKD Chronic kidney disease DMSA Dimercaptosuccinic acid E. coli Escherichia coli fUTI Febrile urinary tract infections ISPN Italian Society of Pediatric Nephrology LUTI Lower urinary tract infections NICE National Institute for Clinical Excellence PCT Procalcitonin RCT Randomized controlled trial SPA Suprapubic bladder aspiration TDA Top-down approach U-CATH Urethral catheterization UPEC Uropathogenic E. coli US Ultrasound UTI Urinary tract infections 1254 VCUG VUR Pediatr Nephrol (2016) 31:1253–1265 Voiding cystourethrography Vesicoureteral reflux Introduction Acute pyelonephritis (AP) is an infection involving the renal parenchyma, which is generally associated with systemic signs of inflammation. As the presence of fever is usually an indicator of renal involvement, the terms febrile urinary tract infection (fUTI) and AP are often used interchangeably and will be used synonymously in this paper. AP is considered to be one of the most serious bacterial illnesses during childhood. These concerns are warranted by the high risk of sepsis in young children in the acute phase [1] and the potential risk of renal scarring with possible long-term morbidity. In the past, a great effort was made to try to minimize these consequences through the aggressive treatment of the acute infection, an intensive imaging work-up in order to discover possible anatomical defects, and the use of antibiotic prophylaxis to prevent recurrences. Over the last three decades, however, it has become apparent that congenital bilateral renal hypodysplasia is the main reason for renal damage in the children who progress towards the need for dialysis and kidney transplantation [2], even in the absence of a history of AP and/or vesicoureteral reflux (VUR). Therefore, a less intensive approach in the management of children following a AP has been suggested by the most recent guidelines. However, a number of major concerns still remain, especially regarding diagnosis, the need to perform imaging in order to diagnose reflux and scarring, and the role of antibiotic prophylaxis. Here we summarize the state of the art, focusing on the most controversial topics. Etiology/physiopathology The kidneys and urinary tract are usually germ-free. Most cases of AP result from the ascension of fecally derived organisms through the urethra and periurethral tissues into the bladder, with subsequent invasion of the kidney. Usually, urine flow prevents infection, washing out the bacteria penetrating into the urinary tract [3]. When bacteria colonize the urinary tract, some children will develop asymptomatic bacteriuria or lower urinary tract infections (LUTIs), while only a minority will experience AP, with systemic symptoms secondary to immune system activation. A variety of host factors or germ characteristics contribute to the risk of AP in early childhood. Regarding the host, the most important condition associated with AP is the presence of anatomical, renal, and urinary tract abnormalities, such as VUR, obstructive megaureter, or neurogenic bladder, in relation to urine stasis. Other host factors could include dysfunctional bladder emptying [4], detrusor instability [5], constipation, and fecal soiling. On the other hand, germ virulence also plays a central role in the pathogenesis of AP. Escherichia coli (E. coli) is the most frequent bacteria, with a prevalence of about 80–90 % [6–8]. The primary reservoir of E. coli is the human gut, where this germ is a normal commensal. The anatomical proximity to the urethral orifice increases the risk of colonization of the urinary tract. The isolate responsible for AP in a given individual often matches rectal isolates from that same person [9]. Among the different strains of E. coli, uropathogenic E. coli (UPEC) are characterized both by additional virulence mechanisms that facilitate their invasion of the urinary tract and kidneys and their resistance to innate immune responses. UPECs are equipped with fimbriae (or pili) that facilitate uroepithelial adherence, even in the presence of adequate urine flow. Their ability to bind to host tissues is essential for the colonization of the urinary tract, against the flow of urine. Type 1 and type P pili are the two best-known types, type P being more frequently associated with AP than LUTI [10]. Other types of pili have also been described. The switch in the expression of different types of pili seems to be influenced by the environment (a process known as phase variation) [11]. These processes increase the likelihood of adherence to host tissue [10]. Other UPEC characteristics that confer a survival advantage are virulent capsule antigens, iron acquisition systems, and toxin secretion [10, 12]. Moreover, the presence of plasmids can contribute to antibiotic resistance [13]. UPECs act as opportunistic intracellular pathogens. Once UPECs invade the uroepithelium, the formation of an intracellular biofilm, containing thousands of rapidly multiplying organisms, can protect themselves from the host immune system. From the bladder, bacteria ascend to the kidney, especially in the presence of anatomical factors such as VUR or major dilation with obstruction. The host’s inflammatory response to colonization by UPECs is characterized by cytokine production, neutrophil influx, exfoliation of infected bladder epithelial cells, and the generation of reactive nitrogen and oxygen species [14]. A prolonged inflammatory state could result in scarring, although the exact underlying mechanisms are still unknown (Fig. 1). The remaining 10–20 % cases of AP are caused by a variety of other organisms including Klebsiella, Enterococcus, Enterobacter, Proteus, and Pseudomonas species. A recent report by pediatric nephrologists from 18 units in ten European countries focused on the causative organisms detected in 4745 positive urine cultures between July 2010 and June 2012 from both hospitalized and non-hospitalized infants under 24 months of age. E. coli was the most frequent bacterium isolated from the urine cultures. However, in 10/16 hospitals and in 6/15 community settings, E. coli was isolated in less than 50 % of the total positive urine cultures. Other isolated Pediatr Nephrol (2016) 31:1253–1265 1255 Fig. 1 Pathogenesis of acute pyelonephritis: E. coli invades uroepithelium, facilitated by the presence of fimbriae. The lipopolysaccharide binds CD14 and activate Toll-like receptors (TLR). As a consequence, nuclear factor κB (NF-κB) migrates into the cell nucleus, stimulating the transcription of inflammatory factors that will mediate fever, neutrophil recruitment, and vascular permeability. The same mechanism can also be responsible for kidney scarring (modified from Montini et al. [4] with permission from Massachusetts Medical Society) bacterial strains were Klebsiella, Enterococcus, Proteus, and Pseudomonas, not only from hospital settings. This underlines the fact that E. coli is the most common organism causing UTIs in infants, however other bacterial strains are now being isolated more frequently than in the past [15]. Clinical manifestations Symptomatology of AP in pediatric patients is variable and influenced by the age of the child, the virulence of the organism, and the inflammatory immune response. Fever (38.5 °C and over) is commonly considered a marker of renal parenchyma involvement, while localized symptoms such as dysuria, frequency, malodorous urine, and urinary incontinence are associated with urethra and bladder involvement. However, symptoms are often non-specific in very young children (<2–3 months): labile temperature, slow feeding and poor weight gain, irritability, lethargy, hypotony, abdominal pain, nausea, and vomiting. These children with ambiguous symptoms have been reported to be at higher risk of complications, such as sepsis and meningitis [1]. The identification of the children at higher risk for complications represents a clinical challenge: in a recent report by Averbuch et al. involving 81 infants with UTI aged 0–2 months, the risk of bacteremia was associated with a blood creatinine level above the 50th percentile for age, however, this risk was not associated with the presence of fever [16]. Furthermore, a recent retrospective study conducted on 350 infants between 29 and 90 days of age with UTI showed a similar rate of bacteraemia in afebrile and febrile infants, while well-appearing young infants with a procalcitonin (PCT) value <0.7 ng/ml were at very low risk of bacteremia [17]. In a large, multicenter, retrospective study of 1895 patients aged 29–60 days with culture-proven fUTI, infants not clinically ill on emergency department examination and without a high-risk past medical history were at very low risk for adverse events such as death, shock, bacterial meningitis, intensive care unit admission, or need for ventilator 1256 Pediatr Nephrol (2016) 31:1253–1265 support. In the same study, the presence of bacteremia was associated with a higher frequency of complications [18]. Similar data has also been reported in a smaller cohort of 140 children [19]. The emission of malodorous urine can be reported by parents or caregivers, but as shown in a recent study by Gauthier et al. [20], its presence is neither specific nor sensitive enough to rule in or rule out a diagnosis of AP. Macroscopic analysis may also reveal cloudy urine. In older children, recurrent AP may result from voiding disturbances, including hyperactivity and dysfunctional bladder emptying. A precise history of voiding modality including incontinence, enuresis, frequency of micturition, urgency and bowel habits are useful in this setting. In conclusion, a diagnosis of AP has to be taken in consideration in all infants with fever and no signs of localization. Diagnosis The diagnosis of AP is initially made on the basis of urinalysis results and the presence of clinical symptoms due to the fact that urine culture results take 24–48 h to obtain. If AP is strongly suspected, particularly in the case of clinically ill young children, empirical antibiotic treatment should be started, always in consideration of local drug-sensitivity patterns. While waiting for urine culture results, the diagnosis of AP can be supported by the presence of white blood cells or bacteria on microscopic examination of an uncentrifuged urine sample. Manual microscopy is accurate, but can be time consuming, while automated urine microscopy is faster and less costly. In a recent prospective study, both techniques gave comparable results in terms of the detection of pyuria, while automated analysis is less sensitive and specific for bacteriuria than Gram-stained smears [21]. A urine dipstick, a chemically sensitive strip of paper that can identify one or more constituents of urine by immersion, provides a rapid, easy and costeffective way of guiding initial diagnosis and management. When more abnormalities are found together, this increases the likelihood of AP. A positive leukocyte esterase test results from the presence of white blood cells, but it may be related to infections other than AP or to non-steroidal anti-inflammatory agents as well. Leukocyte esterase is also present when lysed leucocytes are not visible on microscopy. A positive nitrite test indicates bacteriuria; most uropathogens can indeed convert nitrate to nitrite. Generating sufficient nitrite for a positive test can take up to 4 h, so in the case of urine frequency (infants), the possibility of false negatives should be considered. Therefore, leukocyte esterase has a good sensitivity but a lower specificity than nitrite; a combination of both tests can be helpful in guiding interpretation [22, 23]. A systematic review published by Whiting et al. in 2006 [24] showed that the combination of results of leukocyte esterase and nitrite on a urine dipstick is a reliable test both for ruling in or out UTI. A subsequent meta-analysis carried out in 2010 evaluated the effect of age on the performance of dipstick and compared this test to microscopy [25]. Of the six studies included in the analysis, only two compared the performance of dipstick in younger and older children. When both nitrites and leukocyte esterase are considered, the ability of dipstick to rule bacteriuria both in and out was good in children over 2 years, but the performance was significantly less reliable in younger children. However, in a recent retrospective study [26] comparing the performance of urine dipstick and urine microscopy as screening tests for AP in 6394 febrile infants aged 1 to 90 days, the dipstick had a greater positive predictive value (PPV) than combined urinalysis (66.8 vs. 51.2 %; p<0.001) or microscopic urinalysis (66.8 vs. 58.6 %; p<0.001) and a negative predictive value (NPV) of 98.7 %. The addition of microscopy would slightly increase the NPV to 99.2 %, but resulting in eight false-positives for every missed AP. More recently, Velasco et al. [27] focusing on the leukocyte esterase test only showed that dipstick use has the same accuracy in young febrile infants as in older children. In conclusion, we believe that urine dipstick represents a useful and rapid screening tool for AP. A practical approach for the interpretation of results is summarized in Table 1. Diagnosis of renal parenchymal involvement The differentiation of AP from LUTIs can be a challenge, especially in younger children. However, the confirmation of renal parenchymal involvement can be useful for the Table 1 Practical approach for urinary tract infection (UTI) diagnosis on the base of urinalysis (modified from Ammenti et al. [23] with permission from John Wiley and Sons) Nitrite Leucocyte esterase Likelihood of urinary tract infection (UTI) Action Positive Positive Positive Negative UTI very likely UTI very likely Perform urine culture and start antibiotic on an empiric basis Perform urine culture and start antibiotic on an empiric basis Negative Negative Positive Negative UTI likely UTI unlikely Perform urine culture and start antibiotic on an empiric basis Search for alternative diagnosis Repeat urine dipstick if fever persists Pediatr Nephrol (2016) 31:1253–1265 identification of children at major risk for complications, renal scarring, and long-term sequelae. Technetium-99 m– dimercaptosuccinic acid (DMSA) scanning is considered the reference standard for the confirmation of AP [28, 29], but its routine use is not generally recommended due to the radiation dose and several practical issues related to the availability of the test. Therefore, clinical signs, laboratory tests, and other imaging techniques have been considered as surrogates for the diagnosis of AP. Ultrasound (US) has been found to be a poor test for the localization of UTI [24]. Fever higher than 38.5 °C is commonly considered as a marker of renal parenchymal involvement even if specificity and sensitivity are low [24, 30, 31] . Moreover, as mentioned previously, fever can be absent in infants under 90 days. Regarding laboratory markers, the elevation of C-reactive protein levels and white blood cell count can suggest the presence of renal involvement, but sensitivity and specificity are low [32]. PCT, a precursor of calcitonin, produced by the thyroid gland and released during bacterial infections, is a new promising marker of renal parenchymal involvement [33], and also in very young children [34]. A meta-analysis of 18 studies involving 1011 patients evaluated the role of PCT as a predictor of both AP and scarring in children with UTI [32]. PCT was associated with AP and scarring and demonstrated a significantly higher area under the curve than either C-reactive protein or white blood cell count. A value ≥0.5 ng/ml predicted early and late (scar) renal parenchymal involvement [32]. This cut-off provided an odds ratio of 7.9 for the identification of AP with a sensitivity of 71 % and specificity of 72 %. Sensitivity was 79 % for late scarring with a lower specificity of 50 %. Even if PCT cannot replace the DMSA scan as the gold standard for parenchymal involvement, it can be used as an available biomarker to discriminate between LUTIs and AP and identify children who would benefit from a late DMSA scan [32, 34]. This has been confirmed by a recent Cochrane review [35]. We believe that in well-appearing children with AP blood tests and DMSA scans are not necessary in the majority of cases; in selective cases or in hospitalized children, PCT represents a useful marker of renal parenchymal involvement. Collection of urine samples for microbiological diagnosis The diagnosis of AP is confirmed by the culture of a single strain of bacteria in significant numbers from an appropriately collected urine specimen. Particular efforts have been made to better understand how to avoid false-positive tests due to contamination during collection. Whether the child can control his/her bladder must be taken into account when selecting the appropriate method of collection, and the best method for urine sample collection is still a matter of debate in non- 1257 toilet trained children. Methods can be either invasive or noninvasive. The cut-off point necessary for the positivity of a urine culture test differs according to the collection technique; the decreased risk of contamination associated with invasive methods allows for a lower cut-off of positivity. Invasive techniques are suprapubic bladder aspiration (SPA) and urethral catheterization (U-CATH), while non-invasive methods include mainly the clean-voided method (mid-stream and clean catch) and the sterile bag. There is some concern regarding the low specificity of noninvasive techniques due to the contamination rate. Sensitivity can be lower in very young infants (<90 days) with both methods [36]. Some authors suggest that every bag-obtained positive-result urinalysis should be confirmed with a more reliable method before therapy [37]. However, even invasive methods can fail to collect a viable urine sample for culture; the success rate of invasive methods varies from 20 to 90 % for SPA, while it is reported to be between 72 and 100 % for U-CATH [31, 38, 39]. Moreover, both methods are associated with pain and discomfort for both the child and caregivers [40]. The clean voided mid-stream method is the best for toilettrained children. Performing a thorough perineal/genital cleaning with soap before collection significantly reduces the rate of contamination, which is described as around 20 % [41]. Collecting a clean sample from non toilet-trained children can be more difficult. Fernández et al. [42] recently described a technique for successfully obtaining clean-catch specimens from very young infants. It consists of three steps: (1) feed the baby and clean the genitals 25 min after feeding; (2) stimulate the bladder by tapping the suprapubic area at a frequency of 100 taps per minute for 30 s, while someone holds the baby under their armpits with their legs dangling; (3) massage the paravertebral lumbar area with light circular movements for 30 s. More recently, this method was validated as safe, quick, and effective in a randomized controlled trial (RCT) involving 127 term newborns performed by Altuntas et al. [43]. The success rate of midstream urine sample collection was 78 % for children assigned to the experimental group (bladder stimulation and lumbar massage) and 33 % for the control group (p<0.001) with a median time of 60 s versus 300 s in the control group. Presently, there is no consensus regarding the best method to use in non-toilet-trained children and different guidelines recommend different approaches (Table 2). The American Academy of Pediatrics (AAP) guidelines [31] recommend the use of invasive methods only. The National Institute for Clinical Excellence (NICE) [30] and the Italian Society of Pediatric Nephrology (ISPN) guidelines [23] recommend a less aggressive approach, using invasive techniques only in specific clinical situations, for example, for a febrile child in poor general health or severely ill in appearance. 1258 Table 2 Pediatr Nephrol (2016) 31:1253–1265 Urine collection methods in non-toilet-trained children according to the most recent guidelines Guidelines Suprapubic bladder aspiration (SPA) National Institute for Clinical Excellence (NICE) [30] American Academy of Pediatrics (AAP) [31] Italian Society of Pediatric Nephrology (ISPN) [23] Clean catch Sterile bag Second option* First choice Not recommended** First choice Not considered No First choice Second choice*** Not considered Urethral catheterization (U-CATH) In case of bad clinical conditions *If other non-invasive methods are not possible **If clean catch is not possible, other non-invasive methods (pads) are recommended ***In case of good clinical condition A recent survey [44] on current practice in primary care of children aged 1–36 months, performed in 26 European countries, identified bag as the most frequently used method in Europe, with a significant difference being seen in children <3 months vs. older. The study showed major differences among countries: in Poland, the bag is hardly ever used, while in Germany, the bag is preferred even for children under 3 months old. Similar data emerged from a survey of general practitioners in the West of Ireland aimed at evaluating the implementation of the NICE UTI guidelines in children. Eighty percent of responders stated a preference for the use of a bag to collect a urine sample from a child older than 1 year of age while only 20 % would use the clean-catch method [45]. In conclusion, contamination by bacteria not present in the bladder is possible for all urine collection methods. In our opinion, clean voided methods should be the first choice as they are relatively easy to perform, reliable, cost-effective and acceptable to children, parents, and caregivers. The use of invasive methods should be reserved for children in poor general health. The sterile bag, one of the most widely used methods, especially in primary care, is often preferred by parents for home collection. This method should be used for a dipstick only. In the case of positivity for leucocyte esterase or nitrites, a urine culture should be collected using a different method. Treatment and hospitalization Historically, children with AP have been managed with hospitalization and intravenous therapy. Nevertheless, short courses of intravenous antibiotics (up to 4 days) followed by oral therapy are as effective as longer courses of intravenous treatment (7–14 days) [46–50]. Recent evidence [6, 7, 51–53], moreover, suggests that oral antibiotic treatment alone is as effective as initial parenteral treatment followed by oral antibiotics. A Cochrane review update on antibiotic treatment for AP performed in 2014 [51] found four studies [6, 7, 52, 53] involving 1131 children comparing oral antibiotics for 10 to 14 days with intravenous followed by oral antibiotics. Time to resolution of fever and the number of children with persistent AP at 72 h after the start of therapy did not differ significantly between groups. No significant difference in the mean levels of laboratory biomarkers were found in one study [6]. The number of children with kidney parenchymal damage on DMSA scan at follow-up did not differ significantly between groups. On the basis of these data, the most recent guidelines [23, 30, 31] for the treatment of childhood AP, recommend oral antibiotics for the treatment of children >2 months of age, unless the child is seriously ill and/or unable to tolerate oral antibiotics. To date, no data from RCTs are available to determine the optimal total duration of antibiotic therapy for AP. Oral antibiotic administration is therefore recommended in the outpatient setting. Hospital admission for intravenous therapy is suggested for children in bad clinical condition, if they are vomiting, or if poor compliance is suspected [23, 30]. There is no gold standard empirical antibiotic treatment; resistance patterns can be very different between countries, as demonstrated by the above-mentioned recent European survey [15], which evaluated the resistance patterns of E. coli. A high rate of resistance to amoxicillin was reported by almost all the centers. Data on co-amoxiclavulanate and oral cephalosporin showed a large geographic variability, while a high prevalence of trimethoprim-resistant E. coli was found, probably due to its widespread use as a prophylactic antibiotic. Nitrofurantoin showed a good rate of efficacy, with some isolated but important exceptions. Therefore, pediatricians should be aware of the local resistance patterns in order to better define the initial therapy; the antibiotic can be subsequently modified according to antibiogram results. Regarding the prompt initiation of therapy after the onset of symptoms, a retrospective analysis involving 287 children with AP did not show an increased risk of scarring related to the delay in antibiotic treatment [54]. Further evidence is needed to confirm this initial observation. However, as mentioned above, empirical antibiotic treatment should be started soon after AP is suspected (urinalysis and symptoms), particularly in young children. The association of steroid therapy, during the acute phase, has been proposed for the prevention Pediatr Nephrol (2016) 31:1253–1265 1259 of subsequent scarring. A randomized trial of oral methylprednisolone compared with placebo in 84 children with a first episode of AP on DMSA scan, demonstrated a significant reduction in scarring at 6 months (33 vs. 60 %; p < 0.05) in those given steroids [55]. As mentioned above, a subgroup of children that require special attention and rapid hospitalization are newborns who present unwell with unstable temperature. These children need intravenous antibiotics after appropriate cultures, including blood and urine cultures. Imaging In the past, children were subjected to extensive diagnostic imaging procedures after a first AP, which involved US, voiding cystourethrography (VCUG), and DMSA scanning [56]. This approach was aimed at detecting scarring and identifying VUR of any grade, with the intention of preventing “reflux nephropathy” and its long-term sequelae (hypertension and renal failure) [57]. It was believed that early detection of VUR and scars would permit the prompt initiation of antibiotic prophylaxis and/or surgical correction of the reflux, with the intent of reducing AP recurrence and the appearance of renal scarring. The true benefit of this approach has been reconsidered over time [23, 31, 58]. Data from pediatric registries for chronic kidney disease (CKD) together with the improvement and diffusion of antenatal US has shown that renal damage, which was previously associated with acquired pyelonephritic scarring, is very often congenital in nature, caused by alterations in kidney development, particularly hypodysplasia [59, 60], and can be associated with urinary tract anomalies, such as obstruction or high-grade VUR. In Table 3 effect, distinguishing between congenital damage and APrelated renal scarring is quite impossible with the available diagnostic tools (renal US and DMSA scan). Furthermore, recent publications have highlighted a low correlation between AP and its long-term sequelae. In a systematic review by Toffolo et al. it was observed that of the 1029 children evaluated in prospective studies with normal renal function at the time of the fUTI, only 0.4 % showed a deterioration in renal function during the follow-up period [61]. Salo et al. reported that the etiologic fraction of recurrent childhood fUTIs as a main cause of CKD was, at most, 0.3 % in the absence of structural kidney abnormalities evident in imaging studies after the first childhood fUTI [62]. The usefulness of a complete imaging work-up in children with confirmed AP has never been proved, while a systematic review showed no evidence of a reduction in the recurrence of infection or renal scarring [63]. The role of surgery [58, 64, 65] and antibiotic prophylaxis [65–70] in children with VUR has also been recently reevaluated. In light of these new emerging data, the current guidelines for the management of a first fUTI in children have been modified, favoring less aggressive imaging strategies (Table 3). However, there is no agreement regarding the best screening test, the nature of malformations or the degree of reflux or damage that merits detection [2]. The AAP guidelines suggest performing a routine renal and bladder US after a first fUTI, while VCUG is recommended only if hydronephrosis, scarring, or other anomalies are detected at US [31] or in the presence of “other atypical or complex clinical circumstances”, not specified in detail. DMSA scanning is not recommended. NICE [30] and ISPN [23] integrate the results of US with the presence of risk factors for the identification of children in need of further Imaging strategies after a first febrile urinary tract infection (fUTI) according to the different guidelines National Institute for Clinical Excellence (NICE) [30] American Academy of Pediatrics (AAP) [31] Italian Society of Pediatric Nephrology (ISPN) [23] Top-down approach (TDA) [28] <6 months >6 months US Yes If atypical UTIa Yes Yes No VCUG If abnormal US and/or atypical UTIa If risk factorsb If abnormal US Acute DMSA No Late DMSA If atypical UTIa No If atypical UTIa No No If abnormal US and/or risk factorsc No If abnormal US and/or VUR If positive acute DMSA Yes If positive acute DMSA UTI urinary tract infection, US ultrasound, VCUG voiding cystourethrography, DMSA dimercaptosuccinic acid a Seriously ill, poor urine flow, abdominal or bladder mass, raised creatinine, septicemia, failure to respond to correct antibiotic treatment within 48 h, infection with non-E. coli organisms b c Dilatation on US, poor urine flow, non-E. coli infection, family history of VUR Abnormal prenatal US of the urinary tract, family history of VUR, septicemia, renal failure, age<6 months in a male infant, likely non-compliance of the family, abnormal bladder emptying, no clinical response to correct antibiotic treatment within 72 h, non-E. coli infection 1260 imaging (VCUG and/or DMSA scan). However, in clinical practice, it is common to perform an initial DMSA scan in children with a first fUTI, during the acute phase, only performing VCUG in those with a renal involvement (topdown approach, TDA) [28]. Recently, Nelson et al. [71] analyzed data from 2259 patients under 60 months of age who underwent VCUG and US for a history of UTI in order to assess the sensitivity, specificity, and predictive values of US for VCUG abnormalities. The authors concluded that in children with a history of UTI, US is a poor screening test for genitourinary abnormalities, with low sensitivity and specificity and that sonography and cystography should be considered complimentary. However, in the same paper, among the 1203 children aged 2 to 24 months who underwent imaging after a first fUTI, the negative predictive value was 72–74 % for VUR grade II and 95–96 % for VUR grade>III, even though the likelihood ratio is not available for the interpretation of the data. This interesting finding suggests that with a normal renal and bladder US we can confidently exclude those refluxes at higher risk of recurrent fUTIs and therefore possible renal damage. Further diagnostic procedures should be limited to those children who have recurrent febrile infections or documented renal developmental anomalies (e.g., hypodysplasia) that represent an independent risk factor for the development of chronic kidney disease. In a recent study [72], the authors retrospectively simulated the application of these different guidelines to a cohort of 304 children aged 2 to 36 months enrolled in the Italian Renal Infection Study 1 [6], comparing the efficacy of exclusive oral with initial parenteral antibiotic treatment, after a first fUTI. The results of US, VCUG, acute and late DMSA scans were available for all the recruited children. The missed rate of reflux grades III–V was 27 % for ISPN, 50 % for NICE, 61 % for AAP and 15 % for the TDA, while the rate of missed scars was 53 % for ISPN, 62 % for NICE and 100 % for AAP. Clearly, the TDA would have detected the presence of all scars. All the above-mentioned imaging approaches, apart from the TDA, showed low sensitivity and failed to identify a good proportion of patients with VUR and scars. Consequently, all three diagnostic algorithms are unable to rule children with high-grade VUR or scarring either in or out. On the other hand, a less aggressive imaging work-up allows for a substantial reduction in economic costs and radiation exposure. A recent study associated the exposure to diagnostic radiography in early infancy with an increased risk of lymphoma (odds ratio, 5.14; 95 % CI, 1.27–20.78) [73]. Although the results referred to a small number and must be confirmed by means of further studies, the radiation risks connected to radiographic and scintigraphic imaging should not be underestimated. Moreover, the clinical significance of missing some children with VUR or scars is still unclear regarding the long-term consequences. Pediatr Nephrol (2016) 31:1253–1265 Another interesting approach is reported in a recent metaanalysis in which Shaik et al. [8] evaluated data from published studies of children (0–18 years old) with a first UTI who underwent a DMSA scan at least 5 months after the index episode and tested three prediction models to identify children at major risk of scarring. The authors identified nine studies that met the criteria and for which data was available, six were observational and three were RCTs. Data on the primary outcome was available for a total of 1280 children. Renal scarring was present in 199 children (15.5 %) and 100 of these (50.3 %) had VUR. The presence of scars was associated, in decreasing order, with: grade IV–V VUR; abnormal US findings; grade III VUR; C-reactive protein level; temperature; organism other than E. coli; polymorphonuclear cell count; grade I–II VUR. Age, sex, and duration of fever did not influence the presence of scars at late DMSA scan. They also developed a prediction model that combines US finding + clinical information (temperature + organism other than E. coli) that can identify children at higher risk of scarring. The other two models studied, which included inflammatory markers (model 2) and presence and grade of VUR (model 3), appeared less robust in terms of sensitivity, specificity, PPV, NPV, positive and negative likelihood ratios. Screening all children after a first fUTI would reveal a low prevalence of VUR (20–30 %), above all for grades IV–V (1– 4 %) [6, 8, 31]. Furthermore, only 15 % of children present scarring at late DMSA scan after a first fUTI [8]. As children with recurrent infections have an increased risk of VUR and scars [8], a complete imaging work-up is usually required for recurrent infections, therefore VUR or scars would be correctly identified at this point. In conclusion, we believe that, in light of current knowledge, a less aggressive diagnostic approach should be adopted after a first fUTI. Therefore, we suggest performing an US, conversely we discourage the routine execution of VCUG and DMSA scans, considering the high rate of spontaneous resolution of VUR with age and the good renal outcome for patients with scarring but without major congenital renal abnormalities. Identifying the high risk population for which a full imaging work-up is necessary allows for a reduction in the number of unnecessary imaging tests, psychological stress and economic and radiation costs. Outcome With the improvement of antibiotic therapies, acute infections usually resolve without sequelae. The long-term outcome of fUTIs is mostly related to the appearance of renal scarring. However, the frequency and severity of scarring as a consequence of AP, the time point at which it occurs and the longterm sequelae, such as the risk of consequent CKD, hypertension and pre-eclampsia, have been recently questioned. The diffusion of routine prenatal US over the past 20–30 years has Pediatr Nephrol (2016) 31:1253–1265 demonstrated that much of the renal damage previously attributed to AP is related to the congenital mal-development of the kidneys and is often associated with urinary tract abnormalities (high-grade VUR or obstruction). As a consequence, the role AP plays in renal scarring and its subsequent adverse outcome has been reconsidered [74]. Just a small minority of children (0.4 %) enrolled in prospective studies showed a deterioration of renal function to CKD after a fUTI on follow-up [61]. Conversely, virtually all the children with decreased renal function at the conclusion of studies had scarring or renal dysplasia at enrolment. The risk of hypertension is low [61]. The rate of hypertension only increased from 2.4 to 4.6 % in 713 children enrolled in five studies where blood pressure was measured at the beginning and end of followup (from 5 to 20 years). In the studies reporting a higher incidence of hypertension, up to 35 %, scarring and renal damage were almost always present at enrolment [61]. In contrast, one study [75] that followed two groups of children after a first UTI for 16 to 26 years found no significant differences in ambulatory blood pressure monitoring between the 53 individuals with scars when compared with 51 controls without scars. Childhood UTI has not been seen to influence growth or cause complications during pregnancy [61]. We believe that the long-term outcome of children following a single AP, in the absence of pre-existent renal damage, has to be considered good. Risk of recurrence and prevention While the prognosis of a single episode of AP is good, there are many concerns regarding the effect of recurrent fUTIs on scarring [76], renal function, and quality of life for children and caregivers. Identifying children at major risk could therefore allow for the implementation of preventive measures to reduce the risk of recurrences and preserve the final renal outcome in these children. There is a lack of solid evidence and some controversy regarding the risk factors predisposing recurrence. A major role for AP recurrence is played by dilating reflux, while grades I and II are not associated with frequent relapses, unless bladder dysfunction is also present. Panaretto et al., in a cohort of 290 children (aged up to 5 years) after a first fUTI, who developed 46 relapses, identified an age of less than 6 months at the time of the first UTI (OR 2.9) and grade III–V VUR (OR: 3.5) as independent risk factors for recurrence [76]. Conway et al. evaluated a cohort of 611 children under 6 years of age, recruited from a network of 27 pediatric primary care centers, 83 of whom developed recurrent UTI [77]. Factors associated with recurrences in multivariate analysis were white race, age between 3 and 4 years, age between 4 1261 and 5 years, and grade IV and V VUR. Sex, grade I–III VUR, and no circumcision did not influence the risk of recurrence. The role of circumcision in preventing AP in male infants is still a matter of debate. Two systematic reviews analyzed the role it plays with different conclusions; the first one performed by Sing-Grewal et al. [78] demonstrated that circumcision reduces the risk of UTI, but 111 circumcisions are required to prevent one infection in boys with no other risk factors. A lower number-needed-to-treat is necessary in case of recurrent UTI or high-grade VUR (11 and 4, respectively). Instead, a more recent meta-analysis by Morris et al. [79] reported lack of circumcision as an important risk factor for UTI during lifetime, irrespective of other risk factors. Moreover, a Cochrane review [80] failed to identify any randomized controlled study on the use of routine neonatal circumcision for the prevention of UTI in male infants. We believe that circumcision could be helpful in children with high-grade VUR and recurrent UTIs while on antibiotic prophylaxis. Other described risk factors relating to AP recurrence were family history of UTI, dysfunctional voiding syndrome, poor fluid intake, and functional stool retention. While some of the identified risk factors are not modifiable (age, white race, familiarity), others (presence of reflux, voiding habits, phimosis, bladder function, constipation, and fluid intake) can be modified through behavioral changes and/ or medical interventions. Historically, antibiotic prophylaxis has been used to prevent recurrence in children after fUTI, especially when VUR was detected. Antibiotic prophylaxis is the only preventive measure considered by the most recent guidelines, but none of these recommend its routine use [23, 31]. In a recent meta-analysis on the efficacy of antibiotic prophylaxis in children with VUR carried out by Wang et al. [81], the results of the eight RCTs that met the criteria were analyzed, and while the pooled results showed a reduced risk of recurrence in children undergoing antibiotic prophylaxis (pooled OR=0.63, 95 % CI=0.42–0.96), no differences were found in the appearance of new renal scars between the two groups. Furthermore, the number of renal scars was low in all the RCTs included. Antibiotic prophylaxis was associated with an increased risk of resistant bacteria (pooled OR 8.75, 95 % CI=3.52–21.73, p<0.0001). The most recent of the RCTs included in this review is the recently published Randomized Intervention for Children with Vesicoureteral Reflux (RIVUR) trial [82]. The study involved 607 children with grade I to IV VUR, diagnosed after a first or second fUTI. They were randomized into two groups, either prophylaxis with trimethoprim-sulphamethoxazole or placebo, for 2 years; 520/607 children were eligible for evaluation at the end of study. Hoberman et al. showed a reduction in the risk of recurrences by 50 % in children receiving prophylaxis (39/302 vs. 72/305). The authors concluded that antibiotic prophylaxis is useful in children with VUR, but no differences were found 1262 in the risk of renal scarring, with about an 8 % incidence of new scars occurring in both groups. Furthermore, 16 patientyears of antibiotics were required to prevent one UTI and 22 patient-years of antibiotics were needed to prevent one fUTI. The treatment group received 600 years of prophylaxis in excess. Moreover, an increased risk of antibiotic resistance was found in the antibiotic group; among the 87 children with a first recurrence caused by E. coli, the proportion of isolates that were resistant to trimethoprim-sulfamethoxazole was 63 % in the prophylaxis group and 19 % in the placebo group. Furthermore, some biases have to be considered in the interpretation of the results. Around 92 % of children enrolled in the trial were female. This distribution is different from other similar published studies and from real-life settings. The children enrolled were aged up to 71 months, 126 patients were already toilet-trained and about 30 % of recurrences were afebrile. In addition, 92 % of patients had grade I–III VUR. In conclusion, the lack of difference in scarring and the increased risk of resistance at present do not justify, in our opinion, the routine use of prophylaxis. As stated by the editorial accompanying the RIVUR trial in the New England Journal of Medicine [83]: “Sadly, the decision to use antibiotic prophylaxis in children with reflux remains a clinical dilemma, despite this well-done study. In the face of the emergence of antibiotic resistance, the lack of a significant betweengroup difference in renal parenchymal scarring, and questions about generalizability, the RIVUR study results would imply that the general recommendation of prophylactic antibiotics for vesicoureteral reflux in young children awaits more evidence before universal adoption.” Multiple-choice questions (answers are provided following the reference list) 1) Which children are at major risk of UTIs and pyelonephritis? a) Children undergoing immunosuppressive therapy b) No risk factors can be associated with fUTI in children c) Children with urinary tract abnormalities d) Neonates 2) Which are the best predictors of complications in infants (<90 days) with AP? a) b) c) d) The presence of fever High fever and normal C-reactive protein value No markers Bad clinical condition, an increase in C-reactive protein, creatinine, and procalcitonin levels but no fever 3) Which diagnostic approach do the recent guidelines suggest after a first fUTI? Pediatr Nephrol (2016) 31:1253–1265 a) Top-down approach b) Performing a US, while VCUG and DMSA scanning for selected at-risk children c) Complete imaging work-up (US, DMSA scan, and VCUG) in all children d) No imaging 4) What is the risk of chronic kidney damage in children following a fUTI? a) < 0.5 %. b) 5 % c) 10 % d) >20 % 5) What is the best treatment of a well-appearing infant >2 months of age with AP, according to the most recent guidelines? a) b) c) d) Parental antibiotic treatment and hospitalization Oral antibiotic treatment for 10–14 days Initial oral antibiotic followed by parenteral treatment Initial parenteral antibiotic followed by oral treatment Conflict of interest The authors declare that they have no conflict of interest. References 1. Bachur RG, Harper MB (2001) Predictive model for serious bacterial infections among infants younger than 3 months of age. Pediatrics 108:311–316 2. Montini G, Tullus K, Hewitt I (2011) Febrile urinary tract infections in children. N Engl J Med 365:239–250 3. Cox CE, Hinman F (1961) Experiments with induced bacteriuria, vesical emptying and bacterial growth on the mechanism of bladder defense to infection. J Urol 86:739–748 4. Sillén U, Brandström P, Jodal U, Holmdahl G, Sandin A, Sjöberg I, Hansson S (2010) The Swedish Reflux Trial in Children: V. Bladder Dysfunction. J Urol 184:298–304 5. Ramamurthy HR, Kanitkar M (2008) Recurrent urinary tract infection and functional voiding disorders. Indian Pediatr 45:689–691 6. Montini G, Toffolo A, Zucchetta P, Dall’Amico R, Gobber D, Calderan A, Maschio F, Pavanello L, Molinari PP, Scorrano D, Zanchetta S, Cassar W, Brisotto P, Corsini A, Sartori S, Da Dalt L, Murer L, Zacchello G (2007) Antibiotic treatment for pyelonephritis in children: multicentre randomised controlled noninferiority trial. BMJ 335:386 7. Neuhaus TJ, Berger C, Buechner K, Parvex P, Bischoff G, Goetschel P, Husarik D, Willi U, Molinari L, Rudin C, Gervaix A, Hunziker U, Stocker S, Girardin E, Nadal D (2008) Randomised trial of oral versus sequential intravenous/oral cephalosporins in children with pyelonephritis. Eur J Pediatr 167:1037– 1047 8. Shaikh N, Craig JC, Rovers MM, Da Dalt L, Gardikis S, Hoberman A, Montini G, Rodrigo C, Taskinen S, Tuerlinckx D, Shope T (2014) Identification of children and adolescents at risk for renal scarring after a first urinary tract infection: a meta-analysis with individual patient data. JAMA Pediatr 15224:1–9 Pediatr Nephrol (2016) 31:1253–1265 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. Russo TA, Stapleton A, Wenderoth S, Hooton TM, Stamm WE (1995) Chromosomal restriction fragment length polymorphism analysis of Escherichia coli strains causing recurrent urinary tract infections in young women. J Infect Dis 172:440–445 Wiles TJ, Kulesus RR, Mulvey MA (2008) Origins and virulence mechanisms of uropathogenic Escherichia coli. Exp Mol Pathol 85: 11–19 Lim JK, Gunther NW IV, Zhao H, Johnson DE, Keay SK, Mobley HLT (1998) In vivo phase variation of Escherichia coli type 1 fimbrial genes in women with urinary tract infection. Infect Immun 66:3303–3310 Dhakal BK, Kulesus RR, Mulvey MA (2008) Mechanisms and consequences of bladder cell invasion by uropathogenic Escherichia coli. Eur J Clin Investig 38:2–11 Hussain A, Ewers C, Nandanwar N, Guenther S, Jadhav S, Wieler LH, Ahmed N (2012) Multi-resistant uropathogenic Escherichia coli from an endemic zone of urinary tract infections in India: genotypic and phenotypic characteristics of ST131 isolates of the CTX-M-15 Extended-Spectrum-Beta-Lactamase producing lineage. Antimicrob Agents Chemother 56:6358–6365 Bower JM, Eto DS, Mulvey MA (2005) Covert operations of uropathogenic Escherichia coli within the urinary tract. Traffic 6: 18–31 Alberici I, Bayazit AK, Drozdz D, Emre S, Fischbach M, Harambat J, Jankauskiene A, Litwin M, Mir S, Morello W, Peco-Antic A, Sallay P, Sever L, Simonetti GD, Szczesniak P, Teixeira A, Vidal E, Wuehl E, Mehls O, Weber LT, Schaefer F, Montini G (2014) Pathogens causing urinary tract infections in infants: a European overview by the ESCAPE study group. Eur J Pediatr 174:783–790 Averbuch D, Nir-Paz R, Tenenbaum A, Stepensky P, Brooks R, Koplewitz BZ, Simckes AM, Engelhard D (2014) Factors associated with bacteremia in young infants with urinary tract infection. Pediatr Infect Dis J 33:571–575 Hernandez-Bou S, Trenchs V, Alarcon M, Luaces C (2014) Afebrile very young infants with urinary tract infection and the risk for bacteremia. Pediatr Infect Dis J 33:244–247 Schnadower D, Kuppermann N, Macias CG, Freedman SB, Baskin MN, Ishimine P, Scribner C, Okada P, Beach H, Bulloch B, Agrawal D, Saunders M, Sutherland DM, Blackstone MM, Sarnaik A, McManemy J, Brent A, Bennett J, Plymale JM, Solari P, Mann DJ, Dayan PS (2010) Febrile infants with urinary tract infections at very low risk for adverse events and bacteremia. Pediatrics 126:1074–1083 Velasco-Zúñiga R, Trujillo-Wurttele JE, Fernández-Arribas JL, Serrano-Carro B, Campo-Fernández N, Puente-Montes S (2012) Predictive factors of low risk for bacteremia in infants with urinary tract infection. Pediatr Infect Dis J 31:642–645 Gauthier M, Gouin S, Phan V, Gravel J (2012) Association of malodorous urine with urinary tract infection in children aged 1 to 36 months. Pediatrics 129:885–890 Shah AP, Cobb BT, Lower DR, Shaikh N, Rasmussen J, Hoberman A, Wald ER, Rosendorff A, Hickey RW (2014) Enhanced versus automated urinalysis for screening of urinary tract infections in children in the emergency department. Pediatr Infect Dis J 33: 272–275 Williams GJ, Macaskill P, Chan SF, Turner RM, Hodson E, Craig JC (2010) Absolute and relative accuracy of rapid urine tests for urinary tract infection in children: a meta-analysis. Lancet Infect Dis 10:240–250 Ammenti A, Cataldi L, Chimenz R, Fanos V, La Manna A, Marra G, Materassi M, Pecile P, Pennesi M, Pisanello L, Sica F, Toffolo A, Montini G (2012) Febrile urinary tract infections in young children: recommendations for the diagnosis, treatment and follow-up. Acta Paediatr 101:451–457 Whiting P, Westwood M, Bojke L, Palmer S, Richardson G, Cooper J, Watt I, Glanville J, Sculpher M, Kleijnen J (2006) Clinical 1263 effectiveness and cost-effectiveness of tests for the diagnosis and investigation of urinary tract infection in children: a systematic review and economic model. Health Technol Assess 10:iii–iv, xi– xiii, 1–154 25. Mori R, Yonemoto N, Fitzgerald A, Tullus K, Verrier-Jones K, Lakhanpaul M (2010) Diagnostic performance of urine dipstick testing in children with suspected UTI: a systematic review of relationship with age and comparison with microscopy. Acta Paediatr 99:581–584 26. Glissmeyer EW, Korgenski EK, Wilkes J, Schunk JE, Sheng X, Blaschke AJ, Byington CL (2014) Dipstick screening for urinary tract infection in febrile infants. Pediatrics 133:1121–1127 27. Velasco R, Benito H, Mozun R, Trujillo JE, Merino PA, de la Torre M, Gomez B (2015) Using a urine dipstick to identify a positive urine culture in young febrile infants is as effective as in older patients. Acta Paediatr 104:e39–e44 28. Preda I, Jodal U, Sixt R, Stokland E, Hansson S (2007) Normal dimercaptosuccinic acid scintigraphy makes voiding cystourethrography unnecessary after urinary tract infection. J Pediatr 151:581–584 29. Hansson S, Dhamey M, Sigström O, Sixt R, Stokland E, Wennerström M, Jodal U (2004) Dimercapto-succinic acid scintigraphy instead of voiding cystourethrography for infants with urinary tract infection. J Urol 172:1071–1074 30. National Institute for Health and Clinical Excellence Urinary tract infection in children: diagnosis, treatment and long-term management (2007) Available at: www.nice.org. uk/nicemedia/pdf/ CG54fullguideline.pdf - Accessed January 2015 31. Roberts KB (2011) Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics 128:595–610 32. Leroy S, Fernandez-Lopez A, Nikfar R, Romanello C, Bouissou F, Gervaix A, Gurgoze MK, Bressan S, Smolkin V, Tuerlinckx D, Stefanidis CJ, Vaos G, Leblond P, Gungor F, Gendrel D, Chalumeau M (2013) Association of procalcitonin with acute pyelonephritis and renal scars in pediatric UTI. Pediatrics 131:870– 879 33. Pecile P, Miorin E, Romanello C, Falleti E, Valent F, Giacomuzzi F, Tenore A (2004) Procalcitonin: a marker of severity of acute pyelonephritis among children. Pediatrics 114:e249–e254 34. Bressan S, Andreola B, Zucchetta P, Montini G, Burei M, Perilongo G, Da Dalt L (2009) Procalcitonin as a predictor of renal scarring in infants and young children. Pediatr Nephrol 24:1199–1204 35. Shaikh N, Jl B, Evron J, Mmg L, Borrell JL, Evron J, Leeflang MM (2015) Procalcitonin, C-reactive protein, and erythrocyte sedimentation rate for the diagnosis of acute pyelonephritis in children. Cochrane Database Syst Rev 1, CD009185 36. McGillivray D, Mok E, Mulrooney E, Kramer MS (2005) A headto-head comparison: “clean-void” bag versus catheter urinalysis in the diagnosis of urinary tract infection in young children. J Pediatr 147:451–456 37. Etoubleau C, Reveret M, Brouet D, Badier I, Brosset P, Fourcade L, Bahans C, Garnier F, Blanc P, Guigonis V (2009) Moving from bag to catheter for urine collection in non-toilet-trained children suspected of having urinary tract infection: a paired comparison of urine cultures. J Pediatr 154:803–806 38. Pollack CV, Pollack ES, Andrew ME (1994) Suprapubic bladder aspiration versus urethral catheterization in ill infants: success, efficiency and complication rates. Ann Emerg Med 23:225–230 39. Chen L, Hsiao AL, Moore CL, Dziura JD, Santucci KA (2005) Utility of bedside bladder ultrasound before urethral catheterization in young children. Pediatrics 115:108–111 40. El-Naggar W, Yiu A, Mohamed A, Shah V, Manley J, McNamara P, Taddio A (2010) Comparison of pain during two methods of urine collection in preterm infants. Pediatrics 125:1224–1229 1264 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. Pediatr Nephrol (2016) 31:1253–1265 Vaillancourt S, McGillivray D, Zhang X, Kramer MS (2007) To clean or not to clean: effect on contamination rates in midstream urine collections in toilet-trained children. Pediatrics 119:e1288– e1293 Herreros Fernández ML, González Merino N, Tagarro García A, Pérez Seoane B, de la Serna Martínez M, Contreras Abad MT, García-Pose A (2013) A new technique for fast and safe collection of urine in newborns. Arch Dis Child 98:27–29 Altuntas N, Celebi Tayfur A, Kocak M, Razi HC, Akkurt S (2014) Midstream clean-catch urine collection in newborns: a randomized controlled study. Eur J Pediatr 174:577–582 Hadjipanayis A, Grossman Z, Del Torso S, van Esso D, Dornbusch HJ, Mazur A, Drabik A, Montini G (2014) Current primary care management of children aged 1-36 months with urinary tract infections in Europe: large-scale survey of paediatric practice. Arch Dis Child 100:341–347 Kennedy KM, Glynn LG, Dineen B (2010) A survey of the management of urinary tract infection in children in primary care and comparison with the NICE guidelines. BMC Fam Pract 11:6 François P, Croizé J, Bost C, Wollschlager K (1995) Comparative study of cefixime versus amoxicillin-clavulanic acid combination in the oral treatment of urinary tract infections in children. Arch Pediatr 2:136–142 Benador D, Neuhaus TJ, Papazyan JP, Willi UV, Engel-Bicik I, Nadal D, Slosman D, Mermillod B, Girardin E (2001) Randomised controlled trial of three day versus 10-day intravenous antibiotics in acute pyelonephritis: effect on renal scarring. Arch Dis Child 84:241–246 Levtchenko E, Lahy C, Levy J, Ham H, Piepsz A (2001) Treatment of children with acute pyelonephritis: a prospective randomized study. Pediatr Nephrol 16:878–884 Vilaichone A, Watana D, Chaiwatanarat T (2001) Oral ceftibuten switch therapy for acute pyelonephritis in children. J Med Assoc Thail 84(Suppl 1):S61–S67 Noorbakhsh S, Lari AR, Masjedian F, Mostafavi H, Alaghehbandan R (2004) Comparison of intravenous aminoglycoside therapy with switch therapy to cefixime in urinary tract infections. Saudi Med J 25:1513–1515 Strohmeier Y, Hodson EM, Willis NS, Webster AC, Craig JC (2014) Antibiotics for acute pyelonephritis in children. Cochrane Database Syst Rev 7, CD003772 Bocquet N, Sergent Alaoui A, Jais J-PJ-P, Gajdos V, Guigonis V, Lacour B, Cheron G, Chéron G, Cheron G (2012) Randomized trial of oral versus sequential IV/oral antibiotic for acute pyelonephritis in children. Pediatrics 129:e269–e275 Hoberman A, Wald ER, Hickey RW, Baskin M, Charron M, Majd M, Kearney DH, Reynolds EA, Ruley J, Janosky JE (1999) Oral versus initial intravenous therapy for urinary tract infections in young febrile children. Pediatrics 104:79–86 Hewitt IK, Zucchetta P, Rigon L, Maschio F, Molinari PP, Tomasi L, Toffolo A, Pavanello L, Crivellaro C, Bellato S, Montini G (2008) Early treatment of acute pyelonephritis in children fails to reduce renal scarring: data from the Italian Renal Infection Study Trials. Pediatrics 122:486–490 Huang Y-Y, Chen M-J, Chiu N-T, Chou H-H, Lin K-Y, Chiou Y-Y (2011) Adjunctive oral methylprednisolone in pediatric acute pyelonephritis alleviates renal scarring. Pediatrics 128:e496–e504 Kass EJ, Kernen KM, Carey JM (2000) Paediatric urinary tract infection and the necessity of complete urological imaging. BJU Int 86:94–96 Bailey RR (1973) The relationship of vesico-ureteric reflux to urinary tract infection and chronic pyelonephritis-reflux nephropathy. Clin Nephrol 1:132–141 Smellie JM, Barratt TM, Chantler C, Gordon I, Prescod NP, Ransley PG, Woolf AS (2001) Medical versus surgical treatment 59. 60. 61. 62. 63. 64. 65. 66. 67. 68. 69. 70. 71. 72. 73. 74. in children with severe bilateral vesicoureteric reflux and bilateral nephropathy: a randomised trial. Lancet 357:1329–1333 Ardissino G, Daccò V, Testa S, Bonaudo R, Claris-Appiani A, Taioli E, Marra G, Edefonti A, Sereni F (2003) Epidemiology of chronic renal failure in children: data from the ItalKid project. Pediatrics 111:e382–e387 North American Pediatric Renal Trials and Collaborative Studies. Annual report, (2008) Available at: https://web.emmes.com/study/ ped. Accessed 1 Feb 2015 Toffolo A, Ammenti A, Montini G (2012) Long-term clinical consequences of urinary tract infections during childhood: a review. Acta Paediatr 101:1018–1031 Salo J, Ikäheimo R, Tapiainen T, Uhari M (2011) Childhood urinary tract infections as a cause of chronic kidney disease. Pediatrics 128: 840–847 Westwood ME, Whiting PF, Cooper J, Watt IS, Kleijnen J (2005) Further investigation of confirmed urinary tract infection (UTI) in children under five years: a systematic review. BMC Pediatr 5:2 American Urological Association. Clinical guidelines (2010) Available at:http://www.auanet.org/content/guidelines-andquality-care/clinical-guidelines.cfm?sub=vur2010 - Accessed 1 Feb 2015 Brandström P, Jodal U, Sillén U, Hansson S (2011) The Swedish reflux trial: review of a randomized, controlled trial in children with dilating vesicoureteral reflux. J Pediatr Urol 7:594–600 Garin EH, Olavarria F, Garcia Nieto V, Valenciano B, Campos A, Young L (2006) Clinical significance of primary vesicoureteral reflux and urinary antibiotic prophylaxis after acute pyelonephritis: a multicenter, randomized, controlled study. Pediatrics 117:626–632 Pennesi M, Travan L, Peratoner L, Bordugo A, Cattaneo A, Ronfani L, Minisini S, Ventura A (2008) Is antibiotic prophylaxis in children with vesicoureteral reflux effective in preventing pyelonephritis and renal scars? A randomized, controlled trial. Pediatrics 121:e1489–e1494 Montini G, Rigon L, Zucchetta P, Fregonese F, Toffolo A, Gobber D, Cecchin D, Pavanello L, Molinari PP, Maschio F, Zanchetta S, Cassar W, Casadio L, Crivellaro C, Fortunati P, Corsini A, Calderan A, Comacchio S, Tommasi L, Hewitt IK, Da Dalt L, Zacchello G, Dall’Amico R (2008) Prophylaxis after first febrile urinary tract infection in children? A multicenter, randomized, controlled, noninferiority trial. Pediatrics 122:1064–1071 Roussey-Kesler G, Gadjos V, Idres N, Horen B, Ichay L, Leclair MD, Raymond F, Grellier A, Hazart I, de Parscau L, Salomon R, Champion G, Leroy V, Guigonis V, Siret D, Palcoux JB, Taque S, Lemoigne A, Nguyen JM, Guyot C (2008) Antibiotic prophylaxis for the prevention of recurrent urinary tract infection in children with low-grade vesicoureteral reflux: results from a prospective randomized study. J Urol 179:674–679 Craig JC, Simpson JM, Williams GJ, Lowe A, Reynolds GJ, McTaggart SJ, Hodson EM, Carapetis JR, Cranswick NE, Smith G, Irwig LM, Caldwell PHY, Hamilton S, Roy LP (2009) Antibiotic prophylaxis and recurrent urinary tract infection in children. N Engl J Med 361:1748–1759 Nelson CP, Johnson EK, Logvinenko T, Chow JS (2014) Ultrasound as a screening test for genitourinary anomalies in children with UTI. Pediatrics 133:e394–e403 La Scola C, De Mutiis C, Hewitt IK, Puccio G, Toffolo A, Zucchetta P, Mencarelli F, Marsciani M, Dall’Amico R, Montini G (2013) Different guidelines for imaging after first UTI in febrile infants: yield, cost, and radiation. Pediatrics 131:e665–e671 Rajaraman P, Simpson J, Neta G, Berrington de Gonzalez A, Ansell P, Linet MS, Ron E, Roman E (2011) Early life exposure to diagnostic radiation and ultrasound scans and risk of childhood cancer: case–control study. BMJ 342:d472 Hewitt IK, Montini G (2011) Pediatric febrile urinary tract infections: the current state of play. Ital J Pediatr 37:57 Pediatr Nephrol (2016) 31:1253–1265 75. Wennerström M, Hansson S, Jodal U, Sixt R, Stokland E (2000) Renal function 16 to 26 years after the first urinary tract infection in childhood. Arch Pediatr Adolesc Med 154:339–345 76. Panaretto K, Craig J, Knight J, Howman-Giles R, Sureshkumar P, Roy L (1999) Risk factors for recurrent urinary tract infection in preschool children. J Paediatr Child Health 35:454–459 77. Conway PH, Cnaan A, Zaoutis T, Henry BV, Grundmeier RW, Keren R (2007) Recurrent urinary tract infections in children: risk factors and association with prophylactic antimicrobials. JAMA 298:179–186 78. Singh-Grewal D, Macdessi J, Craig J (2005) Circumcision for the prevention of urinary tract infection in boys: a systematic review of randomised trials and observational studies. Arch Dis Child 90: 853–859 79. Morris BJ, Wiswell TE (2013) Circumcision and lifetime risk of urinary tract infection: a systematic review and meta-analysis. J Urol 189:2118–2124 80. Va J, Fedorowicz Z, Sud V, Ak V, Hajebrahimi S (2012) Routine neonatal circumcision for the prevention of urinary tract infections in infancy. Cochrane Database Syst Rev 11, CD009129 1265 81. Wang H-HS, Gbadegesin RA, Foreman JW, Nagaraj SK, Wigfall DR, Wiener JS, Routh JC (2014) Efficacy of antibiotic prophylaxis in children with vesicoureteral reflux: systematic review and metaanalysis. J Urol 193:963–969 82. Hoberman A, Greenfield SP, Mattoo TK, Keren R, Mathews R, Pohl HG, Kropp BP, Skoog SJ, Nelson CP, Moxey-Mims M, Chesney RW, Carpenter MA (2014) Antimicrobial prophylaxis for children with vesicoureteral reflux. N Engl J Med 370:2367– 2376 83. Ingelfinger JR, Stapleton FB (2014) Antibiotic prophylaxis for vesicoureteral reflux—answers, yet questions. N Engl J Med 370: 2440–2441 Answers 1. C 2. D 3. B 4. A 5. B