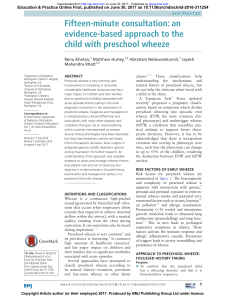
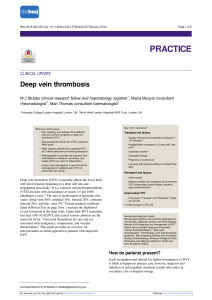
Downloaded from http://pn.bmj.com/ on July 27, 2017 - Published by group.bmj.com NEUROLOGICAL RARITIES Late-onset Tay–Sachs disease Andrew W Barritt,1,2 Stuart J Anderson,1 P Nigel Leigh,1,3 Basil H Ridha1 1 Department of Neurology, Hurstwood Park Neurosciences Centre, Haywards Heath, UK 2 Clinical Imaging Sciences Centre, Brighton and Sussex Medical School, Falmer, UK 3 Trafford Centre for Biomedical Research, Brighton and Sussex Medical School, University of Sussex, Falmer, UK Correspondence to Dr Andrew W Barritt, Department of Neurology, Hurstwood Park Neurosciences Centre, Haywards Heath, West Sussex, RH16 4EX, UK; [email protected] Accepted 27 May 2017 To cite: Barritt AW, J Anderson S, Leigh PN, et al. Pract Neurol 2017;0:1–4. ABSTRACT We discuss the assessment and differential diagnoses of a young adult Hungarian man with a 1-year history of a progressive and symmetric amyotrophic lateral sclerosis-like syndrome, along with irregular action tremor and stimulussensitive myoclonus of the arms. MR scan of the brain showed isolated cerebellar atrophy and formal neuropsychometric testing identified significant subclinical deficits in attention, processing speed and memory. We suspected a form of GM2 gangliosidosis, and white cell enzyme analysis showed markedly reduced enzymatic activity of b-hexosaminidase A. Genetic testing subsequently revealed two heterozygous pathogenic mutations in the HEXA gene (c.1499delT p.(Leu500fs) and c.805G>A p. (Gly269Ser)), confirming the very rare diagnosis of adult-onset Tay–Sachs disease. CASE HISTORY A 35-year-old right-handed Hungarian man presented with 1-year history of progressive weakness in all four limbs and tremor of the arms. He had particular difficulties walking, climbing stairs and lifting objects above the head, and his writing had deteriorated considerably owing to the tremor. He had also developed recent slurring of speech when tired. After sustaining several falls, he had used a stick when walking outdoors for 6 months, and had lost 3 st in weight over 6 months, despite preserved appetite, with a noticeable loss of muscle bulk. There was no pain, sensory or sphincter disturbance, difficulty swallowing or breathing and he had normal mood and subjective cognition. When aged 14, a neurologist had assessed him regarding difficulty with vertical jumping and unsteadiness during sports, along with a subtle bilateral hand tremor. There was no specific diagnosis and the symptoms remained static over the next 20 years, although his tremor prevented him from training as an electrician. He completed A-level education in the UK before enrolling on a business degree in the USA, which was not completed due to funding issues. He returned to the UK aged 23 and worked as a carer but had recently stopped due to his deteriorating condition. He had been previously well with no relevant family history. There was no parental consanguinity and no known Jewish ancestry. His 55-year-old mother lived in Latvia but his father died young in a road traffic crash. His alcohol consumption had always been minimal and he had never smoked. On examination, there was mild bilateral upper motor neurone pattern facial weakness and positive pout reflexes. Neck flexion and extension were normal. The upper limbs showed generalised loss of muscle bulk, most markedly of triceps bilaterally, with florid fasciculations most visible in pectoralis and deltoid muscles. There was a coarse, irregular tremor on posture and action throughout the outstretched upper limbs with symmetrically slowed alternating movements without past pointing. Stimulus-sensitive myoclonus could be elicited on touching the right hand. Muscle tone was normal but with disproportionate elbow extension weakness (2/5), along with symmetrical weakness of shoulder abduction and external rotation, elbow flexion and the first dorsal interossei (4/5). In the lower limbs, tone was normal but there was symmetrical weakness of hip flexion (2/5), knee flexion (3/5) and knee extension (2/5), but with fully preserved hip extension. Flexion of the great toes and ankle inversion was 4/5 bilaterally with all other muscle groups having full power. Reflexes were symmetrically brisk and plantar responses were extensor but with no ankle clonus. Sensory examination was normal. To rise from a seated position he pushed up with his arms to lock his knees in extension before walking with a slow, wide-based and waddling gait (figure 1; for examination Barritt AW, et al. Pract Neurol 2017;0:1–4. doi:10.1136/practneurol-2017-001665 1 Downloaded from http://pn.bmj.com/ on July 27, 2017 - Published by group.bmj.com NEUROLOGICAL RARITIES retrieval rather than encoding, while prominent deficits in attention and processing speed suggested a predominantly subcortical pattern of impairment. Figure 1 Still images from examination video (available online) showing a coarse tremor on posture and action (A), shoulder abduction (B) and hip flexion weakness with visible bilateral wasting of the quadriceps muscles (C) and an extensor left plantar response (D). see online supplementary video). Cardiorespiratory, abdominal, skin, lymph node and testicular examinations were normal and there was no gynaecomastia. Serum creatine kinase was 603 units/L (0–190). Normal or negative blood investigations included full blood count, renal profile, liver and thyroid function tests, serum C reactive protein, erythrocyte sedimentation rate, antinuclear antibody, extractible nuclear antigen, serum immunoglobulins, serum protein electrophoresis, antineuronal antibodies, antiganglioside antibodies, HIV, syphilis, Lyme disease and hepatitis A–C serology. Neurophysiological assessment showed normal peripheral motor and sensory studies apart from slightly reduced sural sensory action potentials bilaterally. Needle electromyography found widespread chronic denervation, including the tongue. MR scan of brain and whole spine showed disproportionate cerebellar atrophy but was otherwise normal (figure 2); cerebrospinal fluid was normal. ECG showed normal sinus rhythm. CT scan with contrast of chest, abdomen and pelvis was normal. Formal neuropsychological assessment was limited by his writing difficulties. Out of 14 subcomponent domains, he scored within the mildly impaired range in three (visual attention/working memory and delayed verbal recall; 21.4%), mild-to-moderate range in six (auditory attention/working memory, delayed visual recall, immediate verbal recall, semantic word fluency and verbal recognition memory; 42.8%) and moderate-to severe range in two (processing speed and immediate visual recall; 14.2%). In contrast, he performed in the normal range on tests of visual perception, confrontational naming and intellectual ability/non-verbal reasoning (21.4%). His relatively preserved recognition memory suggested difficulty of 2 DIFFERENTIAL DIAGNOSES This patient’s progressive upper and lower motor neuronopathy without sensory involvement raised the possibility of amyotrophic lateral sclerosis. However, there were atypical features including the teenage onset of tremor and sporting difficulties, the predominantly proximal pattern of muscle weakness, disproportionate wasting and weakness of triceps muscles, the jerky upper limb tremor and myoclonus and disproportionate cerebellar atrophy. Beyond cervical myeloradiculopathy, mimics of amyotrophic lateral sclerosis with upper and lower motor neurone involvement are rare.1 2 Repeat expansions of the C9orf72 gene, causing of a spectrum of phenotypes including amyotrophic lateral sclerosis and frontotemporal dementia, can be associated with regional cerebellar atrophy. However, its penetrance is unusual under 35 years of age and also he had no features of frontotemporal dementia.3 4 Cerebellar atrophy raised the possibility of a complex form of autosomal dominant spinocerebellar ataxia, such as spinocerebellar atrophy type 3 (Machado–Joseph disease), in which there may be pyramidal signs and anterior horn cell disease. However, the absence of extraocular movement abnormalities and extrapyramidal signs were against this. Although normal appearing white matter on brain MRI would not exclude an adultonset adrenoleukodystrophy, the cerebellar involvement, lack of sphincter disturbance or sensory signs and subsequently, normal very-long-chain fatty acid levels made this and polyglucosan body disease unlikely. Adult-onset Niemann–Pick disease type C Figure 2 MR brain imaging showing diffuse cerebellar atrophy on sagittal T1 (A), axial T2 (B) and coronal T1 (C) sequences with prominent cerebellar folia and widening of the fissures (arrowheads). Barritt AW, et al. Pract Neurol 2017;0:1–4. doi:10.1136/practneurol-2017-001665 Downloaded from http://pn.bmj.com/ on July 27, 2017 - Published by group.bmj.com NEUROLOGICAL RARITIES may present with a myriad of features, including cerebellar ataxia and movement disorders, but our patient did not have the characteristic vertical supranuclear gaze palsy. Nevertheless, as cerebellar atrophy is a recognised feature in this and other GM2 gangliosidoses, we undertook a white cell enzyme analysis; this showed normal total hexosaminidase activity at 1210 nmol/hour/mg (885–5965 and includes hexosaminidase B activity) but a markedly low white cell b-hexosaminidase A functioning at 10 nmol/hour/mg (134–700), representing only 15% normal hexosaminidase A activity (usually 62%–79%). Genetic testing identified compound heterogeneous pathogenic mutations with both 1499T deletion and the 805G>A substitution in the HEXA gene. We therefore made a definitive diagnosis of late-onset Tay–Sachs disease. DISCUSSION b-Hexosaminidase A is a dimeric lysosomal enzyme comprising alpha subunits encoded by the HEXA gene (chromosome 15) and beta subunits coded by the HEXB gene (chromosome 5). It is the only one of three isozymes that hydrolyses the ganglioside GM2 into GM3.5 6 GM2 belongs to the glycosphingolipid category of sphingolipids—essential constituents of the lipid bilayer of cell membranes7—and occurs almost exclusively in the nervous system, particularly within grey matter.8 Abnormal accumulation of GM2 within lysozymes usually results from a deficiency of the b-hexosaminidase A enzyme itself, either due to autosomal recessive gene defects in HEXA (Tay-Sachs disease) or HEXB (Sandhoff ’s disease). Extremely rarely it may arise instead from deficiency of its activator protein encoded by the GM2A gene.9 The severity of individual clinical presentations probably relates to the degree of residual enzyme activity.5 Most commonly, severe homozygous mutations lead to little or no functional enzyme activity, resulting in relentless developmental regression and early death in infancy.6 Less severe enzyme defects can delay presentation until adolescence or adulthood, with a rather heterogeneous disease spectrum. However, even in late-onset Tay-Sachs disease, there is often a history of subtle motor difficulty in childhood.6 7 There is usually neuromuscular weakness, pyramidal signs and cerebellar dysfunction, but at least a third have also neuropsychiatric disturbances (some initially believed to have schizophrenia), and others have extrapyramidal syndromes, dystonia, overactive bladder symptoms and cognitive decline.6 7 A subgroup of patients with late-onset Tay–Sachs disease have a clinically manifest sensory Barritt AW, et al. Pract Neurol 2017;0:1–4. doi:10.1136/practneurol-2017-001665 neuropathy,10 but our patient’s diminished sural sensory action potentials reflected subclinical involvement. The nature and extent of cognitive involvement in late-onset Tay-Sachs disease is variable with a reported incidence ranging from 0% to 50%.7 11–13 Deficits in executive functioning and memory are the most common. Computerised testing (NeuroTrax) can identify verbal impairment.11 There is also an association between the burden of neurological involvement and degree of cognitive dysfunction.13 Formal neuropsychometric testing in our patient showed a predominantly subcortical pattern of cognitive impairment with prominent deficits in attention, processing speed, executive function, working memory and memory retrieval. This is consistent with the relatively greater neuropathological involvement of the subcortical structures and cerebellum in late-onset Tay–Sachs disease.14 Clinicians should be aware of late-onset Tay-Sachs disease as an extremely rare mimic of amyotrophic lateral sclerosis associated with tremor and cerebellar atrophy. Formal psychometric testing may highlight previously unsuspected deficits. Delineating the extent of cognitive impairment will influence the multidisciplinary management of the hexosaminidase deficiency syndromes, which remains supportive in the absence of any clinically effective disease-modifying treatment. Although low-dose pyrimethamine, a dihydrofolate reductase inhibitor, induces a small but significant increase in circulating white cell hexosaminidase A activity in patients with late-onset Tay-Sachs disease possessing certain mutations, the effect wanes and even reverses with long-term exposure; this can correct to baseline after drug withdrawal.15 In a small open-label study, three of four patients continued to deteriorate over 18 months, whereas the other remained stable despite receiving cyclical low-dose pyrimethamine with regular monitoring of white cell enzyme activity.15 Contributors AWB performed a literature search and review and drafted the article. SJA performed a literature search, review of the literature and part-drafted the article. PNL and BHR provided clinical expertise and critical appraisal of the article for submission. Competing interests None declared. Patient consent Obtained. Provenance and peer review Not commissioned; externally peer reviewed. This paper was reviewed by Robin Lachmann, London, UK. © Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted. REFERENCES 1 Ghasemi M. Amyotrophic lateral sclerosis mimic syndromes. Iran J Neurol 2016;15:85–91. 3 Downloaded from http://pn.bmj.com/ on July 27, 2017 - Published by group.bmj.com NEUROLOGICAL RARITIES Key points Clinicians should be aware of late-onset Tay–Sachs disease as an extremely rare mimic of amyotrophic lateral sclerosis associated with tremor and cerebellar atrophy; such patients need white cell enzyme testing, looking particularly for hexosaminidase A deficiency. " Patients with late-onset Tay–Sachs disease may have longstanding subtle clumsiness or athletic difficulties dating to childhood and teenage years. " There may be subclinical cognitive deficits identified only on formal neuropsychometric testing and typically reflecting subcortical dysfunction; " The only clue from brain imaging may be an isolated cerebellar atrophy. " 2 Turner MR, Talbot K. Mimics and chameleons in motor neurone disease. Pract Neurol 2013;13:153–64. 3 Bocchetta M, Cardoso MJ, Cash DM, et al. Patterns of regional cerebellar atrophy in genetic frontotemporal dementia. Neuroimage Clin 2016;11:287–90. 4 Cooper-Knock J, Shaw PJ, Kirby J. The widening spectrum of C9ORF72-related disease; genotype/phenotype correlations and potential modifiers of clinical phenotype. Acta Neuropathol 2014;127:333–45. 5 Chen H, Chan AY, Stone DU, et al. Beyond the cherry-red spot: ocular manifestations of sphingolipid-mediated neurodegenerative and inflammatory disorders. Surv Ophthalmol 2014;59:64–76. 4 6 Neudorfer O, Kolodny EH. Late-onset Tay-Sachs disease. Isr Med Assoc J 2004;6:107–11. 7 MacQueen GM, Rosebush PI, Mazurek MF. Neuropsychiatric aspects of the adult variant of Tay-Sachs disease. J Neuropsychiatry Clin Neurosci 1998;10:10–19. 8 Stryer L. Biosynthesis of Membrane Lipids and Steroids. Biochemistry. W.H. Freeman & Company, 1995. 9 Neudorfer O, Pastores GM, Zeng BJ, et al. Late-onset Tay-Sachs disease: phenotypic characterization and genotypic correlations in 21 affected patients. Genet Med 2005;7:119–23. 10 Shapiro BE, Logigian EL, Kolodny EH, et al. Late-onset TaySachs disease: the spectrum of peripheral neuropathy in 30 affected patients. Muscle Nerve 2008;38:1012–5. 11 Elstein D, Doniger GM, Simon E, et al. Neurocognitive testing in late-onset Tay-Sachs disease: a pilot study. J Inherit Metab Dis 2008;31:518–23. 12 Zaroff CM, Neudorfer O, Morrison C, et al. Neuropsychological assessment of patients with late onset GM2 gangliosidosis. Neurology 2004;62:2283–6. 13 Frey LC, Ringel SP, Filley CM. The natural history of cognitive dysfunction in late-onset GM2 gangliosidosis. Arch Neurol 2005;62:989–94. 14 Suzuki K. Neuropathology of late onset gangliosidoses. A review. Dev Neurosci 1991;13:205–10. 15 Osher E, Fattal-Valevski A, Sagie L, et al. Effect of cyclic, low dose pyrimethamine treatment in patients with late onset Tay Sachs: an open label, extended pilot study. Orphanet J Rare Dis 2015;10:45. Barritt AW, et al. Pract Neurol 2017;0:1–4. doi:10.1136/practneurol-2017-001665 Downloaded from http://pn.bmj.com/ on July 27, 2017 - Published by group.bmj.com Late-onset Tay−Sachs disease Andrew W Barritt, Stuart J Anderson, P Nigel Leigh and Basil H Ridha Pract Neurol published online July 24, 2017 Updated information and services can be found at: http://pn.bmj.com/content/early/2017/07/24/practneurol-2017-001665 These include: References Email alerting service This article cites 14 articles, 1 of which you can access for free at: http://pn.bmj.com/content/early/2017/07/24/practneurol-2017-001665 #BIBL Receive free email alerts when new articles cite this article. Sign up in the box at the top right corner of the online article. Notes To request permissions go to: http://group.bmj.com/group/rights-licensing/permissions To order reprints go to: http://journals.bmj.com/cgi/reprintform To subscribe to BMJ go to: http://group.bmj.com/subscribe/