Eating is not just swallowing:
Redefining the “swallowing”
process in the elderly
Samantha Shune, PhD, CCC-SLP
University of Oregon
Jerald B. Moon, PhD
University of Iowa
November 20, 2014
Disclosures
Financial Disclosures
Funding sources:
NIH-NIA 1F31AG042255
Executive Council of Graduate and Professional Students
at the University of Iowa
Acknowledgements
Molly Cook; Shawn Goodman, PhD; many, many
students and faculty at Iowa
Preview
Introduction
Why is swallowing/nutrition important?
What other factors are involved?
Current Study
Future Steps
Clinical implications
Research directions
1
Why should we care?
What role does swallowing/nutrition play in our
everyday lives?
What would it mean to not be able to swallow
safely or effectively?
Biopsychosocial ramifications
Why is this particularly important in our aging
population?
e.g., Altman et al., 2010; Ashford et al., 2009; Martino et al., 2005; Mick et al., 1991; Ney et al., 2009;
Robbins et al., 1992
http://swallowingdisorderfoundation.com/swallow-a-documentary/
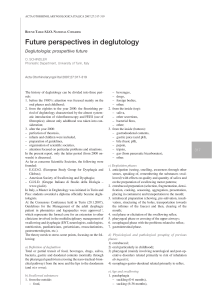
Four Phases of Swallowing
Buettner A et al. Chem. Senses 2001;26:1211-1219
Oxford University Press
2
Sensorimotor Integration
Sensory input is a vital component of the
swallowing process
Peripheral and central recognition of food
Trigger for the swallow response (initiation)
Modulate the motor response
Pressure, taste, touch, temperature
Bolus volume, consistency, viscosity, density,
flavor
e.g., Steele & Miller, 2010; Steele & Van Lieshout, 2004
Recognized importance in nursing literature
Optimizing sensory input
Providing visual and auditory assistance
Maximizing body language and gestures
Minimizing external distractions
mealtime improvements in nursing home
residents
Not all oropharyngeal!
Implications of feeding assistance?
e.g., Eaton et al., 1986; Lange-Alberts & Shott, 1994; VanOrt & Phillips, 1992
Terminology
Feeding
vs
Swallowing
vs
Eating
3
Other Components of Eating
Pre-Oral/Anticipatory Phase
Mastication arguably begins when foods and/or
liquids meant for consumption are recognized
Audition
Cognition
Olfaction
Proprioception
Vision
Upper limb/physical mobility
e.g., Leopold & Kagel, 1997; Maeda et al., 2004; Steele & Miller, 2010
What is the intention or final goal of the action?
e.g., grasping to eat versus grasping to place
(Cattaneo et al., 2007)
Various individual- and environmental-level
factors may ultimately influence later swallowing
4
Other Components of Eating
(in elderly)
Decreased nutrition does not (necessarily) mean a
problem with swallowing, but still important to
consider!
Many other factors involved
Physical changes
Taste changes
Disease
Transportation
Loneliness/grief
Limit food choices/forget or choose not to eat limit
nutrition and potential for malnutrition
e.g., Toner et al., 2011
Dysphagia vs. Presbyphagia
Dysphagia – disordered oropharyngeal
swallowing
Presbyphagia – characteristic alterations in
swallowing mechanism in otherwise healthy older
adults
Aged, but healthy swallow
NOT DISORDERED
Presbyphagia
Primary Aging
Young versus Elderly Swallow:
(http://vimeo.com/60944584)
5
Presbyphagia
Masticatory, lingual, pharyngeal/laryngeal muscles
Decreased maximal force, strength
Increased variability in movements
Decreased hyolaryngeal reserve
Temporal Changes
Prolonged oropharyngeal phase
Delay in moving from oral to pharyngeal phase
Uncoupling of phases increased variability in timing/
initiation
e.g., McComas, 1998; Monemi et al., 1998; Logemann, 1998; Logemann et al., 2000; Ney et al., 2009; Rastatter et
al., 1987; Robbins et al., 1992; Steele & Van Lieshout, 2009)
Sensory (dys)function
Increased discrimination thresholds
Taste, temperature, tactile sensation, olfaction changes
Decreased pharyngeal sensitivity
Delay in initiation
Increased penetration
Sensory (dys)function – other
Salivation (xerostomia)
Proprioception
Slower and more variable (upper) limb movements
e.g., Adamo et al., 2007; Aviv, 1997; Chavez & Ship, 2000; Ney et al., 2009; Robbins et al., 1999
Questions
What are the anticipatory motor patterns that
occur during swallowing and eating?
What are the implications of absent anticipatory
information/cues?
On a typical system? On a taxed system?
What age-related changes in the anticipatory
stage and the overall eating process occur?
6
The Current Study
Participants
24 Younger Adults
Ages 18-30 (M = 24.4, SD = 3.5)
12 females, 12 males
24 Older Adults
Ages 70-85 (M = 76.1, SD = 4.5)
12 females, 12 males
Methods
Task Procedures
Feeding
Task Conditions:
Sensory Present
Cues
Absent
Independent
Dependent
Typical SelfFeeding
Typical AssistedFeeding
Sensory Loss
Self-Feeding
Sensory Loss
Assisted-Feeding
Variables of interest
Onset of hand/arm movement (i.e., onset of the
eating process)
Onset of lower lip/jaw lowering
Junction between gross motor and fine motor
hand movement (i.e., the approximate onset of the
oral stage of swallowing)
Point of maximal lower lip/jaw lowering (prior to
onset of closing gesture or offset of lip/jaw
lowering)
7
Predictions:
Lip/jaw complex movement will be linked to hand/
arm movement under typical eating conditions.
Given complete or partial cue removal, lip/jaw onset
will be delayed.
Delay (or increased delay) in onset under all
conditions will be present in older adults.
Results – Question 1
What are the anticipatory motor patterns that
occur during swallowing and eating?
Durations of movement
Variability in attention to cues
Durations of anticipatory movements in the typical selffeeding condition
8
What anticipatory stage “cues” influence the
timing of oral movement?
Onset of hand movement?
Change in direction of hand movement?
Older adults:
Hand onset for lowering onset
Hand change for lowering offset
Younger adults: Hand change for lowering offset
Results – Question 2
What are the implications of absent anticipatory
information/cues?
Durations and timing of movement
Lip lowering onset to hand onset
9
Lip lowering offset to hand change
Discussion
Anticipatory stage of swallowing
Oral posturing begins prior to the onset of oral
sensation
System readying for bolus acceptance/the swallow
Influenced by age and available sensory cues
(proprioception, vision)
Older adults’ “compensatory advantage”
Further lowering
Slower movement
Decreased efficiency in online modifications
Must attend to lowering onset
10
Both proprioception and visual cues crucial
Proprioception onset
Vision offset
Both necessary for timing the final phase of motor
execution
Increased variability given the loss of either or both
Implications/Future Directions
Deglutition begins prior the onset of oral
sensation
Impact of sensory loss
Feeding strategy recommendations
Decrease in system readiness?
Exacerbated given increased task demands and/or
an already taxed system?
Optimizing proprioceptive and visual cues
Decreasing distractions/increasing attention
How do these strategies impact the entire process of
deglutition?
Swallowing assessment
11
Future Directions
Mealtime success as a function of ???
Social enjoyment
Communicative success
Decreased adverse behaviors
Nutritional intake
Others?
Interaction between “survival” and QOL
Changing family dynamics
Changes in self-identity
Gender specific?
Age specific?
Culturally based?
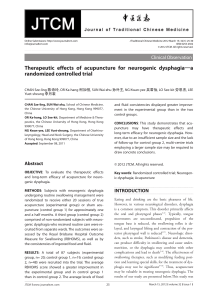
Age
Conversation
tion
n
Mealtime
Gender
G
Feeding
Swallowing
Health
Environment
Social
Soci
ial Interaction
Inter
eraccti
ction
ctio
Relationships
12
Interestingly, factors shown to enhance quality
of life have also been shown to increase survival.
Nutrition
Swallow function
Social engagement
Communicative function
e.g., Holt-Lunstad et al., 2010; Karvonen-Gutierrez et al., 2008; Mick et al., 1991; Ney et al., 2009; Shune et
al., 2012
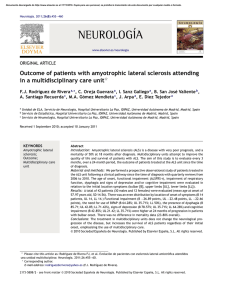
Our Objective
How can we integrate the physiologic
components of swallowing with a more holistic
view of the shared meal in order to promote
mealtime safety and socio-emotional
connectedness for our rapidly growing
population of older adults?
Leading to enhanced survival AND quality of life
Age
Conversation
Mealt
ttii
Mealtime
Gender
Feeding
Fee
F
eedi
Swallow
Swallowing
win
wi
Health
Environment
Social
Soci
iaall Interaction
I te
ter
e actio
era
ctiio
io
Relationships
Swallowing
lowing
13
Questions and Thoughts?
[email protected]
References
Adamo, D.E. et al., (2007). Age-related differences in upper limb proprioceptive acuity. Perceptual Motor
Skills, 104, 1297-1309.
Ashford, J. et al. (2009). Evidence-based systematic review: Oropharyngeal dysphagia behavioral
treatments. Part III--impact of dysphagia treatments on populations with neurological disorders. J Rehab
Res Dev, 46(2), 195-204.
Aviv, J. (1997). Effects of aging on sensitivity of the pharyngeal and supraglottic areas. Am J Med,
103(5A), 74S-76S. Chavez & Ship, 2000
Eaton, M. et al. (1986). The effect of touch on nutritional intake of chronic organic brain syndrome
patients. J Gerontology, 41(5), 611-616.
Humbert, I.A. et al. (2009) Neurophysiology of Swallowing: Effects of Age and Bolus Type. NeuroImage,
44, 982-991.
Lange-Alberts, M.E. & Shott, S. (1994). Nutritional intake. use of touch and verbal cuing. J Gerontological
Nursing, 20(2), 36-40.
Leopold, N.A. & Kagel, M.C. (1997). Dysphagia--ingestion or deglutition?: A proposed paradigm.
Dysphagia, 12, 202-206.
Logemann, J.A. (1998). Evaluation and treatment of swallowing disorders. Austin, TX: PRO-ED.
Logemann, J.A. et al. (2000). Temporal and biomechanical characteristics of oropharyngeal swallow in
younger and older men. J Speech Lang Hear Res, 43(5), 1264-1274.
Maeda, K. et al. (2004). Modulation of voluntary swallowing by visual inputs in humans. Dysphagia, 19,
1-6.
Malandraki, G.A. et al. (2011). Reduced somatosensory activations in swallowing with age. Hum Brain
Map, 32, 730-743.
Malandraki, G.A. et al. (2010). Age-related differences in laterality of cortical activations in swallowing.
Dysphagia, 25, 238-249. Martino et al., 2005
McComas,A.J. (1998). Oro-facial muscles: Internal structure, function and ageing. Gerodontology, 15(1),
3-14.
Mick, R et al. (1991). Prognostic factors in advanced head and neck cancer patients undergoing
multimodality therapy. Otolaryngol Head Neck Surg, 105, 62-73.
Monemi, M. et al. (1998). Adverse changes in fibre type composition of the human masseter versus
biceps brachii muscle during aging. J Neurol Sci, 154, 35-48.
Ney, D. et al. (2009). Senescent swallowing: Impact, strategies, and interventions. Nutrit Clin Practice,
24(3), 395-413.
Rastatter, M.P. et al.(1987). Speech-motor equivalence in aging subjects'. Perceptual Motor Skills, 64(2),
635-638.
Robbins, J. et al. (1999). Differentiation of normal and abnormal airway protection during swallowing
using the penetration-aspiration scale. Dysphagia, 14, 228-232.
Robbins, J. et al. (1992). Oropharyngeal swallowing in normal adults of different ages. Gastroenterology,
103(3), 823-829.
Steele, C., & Miller, A. (2010). Sensory input pathways and mechanisms in swallowing: A review.
Dysphagia, 25(4), 323-333.
Steele, C., & Van Lieshout, P. (2004). Influence of bolus consistency on lingual behaviors in sequential
swallowing. Dysphagia, 19(3), 192-206.
Steele, C., & Van Lieshout, P. (2009). Tongue movements during water swallowing in healthy young and
older adults. J Speech Lang Hear Res, 52(5), 1255-1267.
Teismann, I.K. et al. (2010). Neurobiol Aging, 31, 1044-1050.
Toner, M.A. et al. (2011). Aging and Communication, 2nd ed. Austin, TX: Pro-Ed.
VanOrt, S. & Phillips, L. (1992). Feeding nursing home residents with Alzheimer's disease. Ger Nurs,
13(5), 249-253.
14
 0
0