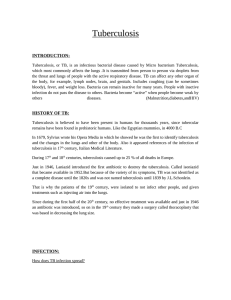
The Journal of Arthroplasty 32 (2017) 2208e2213 Contents lists available at ScienceDirect The Journal of Arthroplasty journal homepage: www.arthroplastyjournal.org Revision Arthroplasty Silver-Coated Megaprosthesis of the Proximal Tibia in Patients With Sarcoma Jendrik Hardes, MD *, Marcel P. Henrichs, MD, Gregor Hauschild, MD, Markus Nottrott, PhD, Wiebke Guder, MD, Arne Streitbuerger, MD Department of Orthopaedics and Tumour Orthopaedics, Münster University Hospital, Münster, Germany a r t i c l e i n f o a b s t r a c t Article history: Received 20 September 2016 Received in revised form 2 February 2017 Accepted 20 February 2017 Available online 1 March 2017 Background: Proximal tibia arthroplasty is associated with high rates of infection. This study is the largest one that has compared the infection rates with titanium vs silver-coated megaprostheses in patients treated for sarcomas. Methods: The infection rate in 98 patients with sarcoma or giant-cell tumor in the proximal tibia who underwent placement of a titanium (n ¼ 42) or silver-coated (n ¼ 56) megaprosthesis (MUTARS) was assessed, along with the treatments administered for any infection. Results: As the primary end point of the study, the rates of infection were 16.7% in the titanium group and 8.9% in the silver group, resulting in 5-year prosthesis survival rates of 90% in the silver and 84% in the titanium group. Whereas in the titanium group 37.5% of patients ultimately had to undergo amputation in the present study, these mutilating surgical procedures were only necessary in the silver group in one patient (14.3%). Conclusion: The use of silver-coated prosthesis reduced the infection rate in a relatively large and homogeneous group of patients. In addition, less-aggressive treatment of infection was possible in the group with silver-coated prosthesis. © 2017 The Author(s). Published by Elsevier Inc. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/). Keywords: prosthesis-related infections bone neoplasms silver implantation proximal tibia sarcoma Periprosthetic infection continues to be a frequent and very serious complication after the placement of tumor endoprosthesis [1e4]. Particularly with proximal tibia arthroplasties, there is a high risk of infection owing to the difficulty of muscle coverage. Grimer et al [5] reported an infection rate of 36% before the introduction of routine use of a gastrocnemius rotation flap, with the rate subsequently being reduced to 12%, thanks to the better muscle coverage. Treatment options for periprosthetic infection range from general rinsing of the prosthesis and exchanging of the polyethylene components to a need for secondary amputation [2,6]. Periprosthetic infection is, thus, usually associated with a prolonged burden of suffering for the patient and, in the worst case, also with a permanent deterioration in quality of life. No author associated with this paper has disclosed any potential or pertinent conflicts which may be perceived to have impending conflict with this work. For full disclosure statements refer to http://dx.doi.org/10.1016/j.arth.2017.02.054. Jendrik Hardes and Marcel P. Henrichs contributed equally to this study. * Reprint requests: Jendrik Hardes, MD, Department of Orthopaedics and Tumour Orthopaedics, Münster University Hospital, Albert Schweitzer Campus 1, 48149 Münster, Germany. Preventing periprosthetic infection is, therefore, of utmost importance. Among the metals known to have antimicrobial activity, silver has attracted interest among many investigators because of its excellent level of antimicrobial activity and low toxicity [7,8]. In a previous study, we reported a reduction in the periprosthetic infection rate when silver-coated tumor endoprosthesis was used [9]. However, the study only included a small number of patients, and the follow-up period was short. To the best of our knowledge, there have been no studies investigating the use of silver-coated tumor endoprosthesis to prevent infection. The aim of the present study was therefore to compare the actual infection rate among patients with titanium tumor prosthesis with the infection rate in a larger number of patients in whom silver-coated prosthesis was implanted in the proximal tibia as the primary implant. Possible differences in the ways in which periprosthetic infections were treated were also documented. Patients and Methods A total of 98 patients were treated with a proximal tibia arthroplasty (MUTARS; implantcast, Buxtehude, Germany). http://dx.doi.org/10.1016/j.arth.2017.02.054 0883-5403/© 2017 The Author(s). Published by Elsevier Inc. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/). J. Hardes et al. / The Journal of Arthroplasty 32 (2017) 2208e2213 Fifty-six patients (median age, 19 years; range, 11-78 years) received a silver-coated prosthesis between 2005 and 2014, and 42 patients (median age, 16 years; range, 11-69 years) received a titanium prosthesis between 1996 and 2004. Some of the patients were included in a previous study but now have a longer follow-up period [9]. The silver-coated prosthesis used has been described in previous studies [7e9]. No silver coating was applied at the articulating surfaces or prosthetic stems. Patients who received a silver-coated prosthesis had a median follow-up period of 38 months (mean, 17 months; range, 5-120 months) and 44 months for the surviving patients. At the final follow-up, 46 patients had no evidence of disease, 4 patients were alive with disease, and 5 patients had died of the disease (median follow-up period, 16 months). One patient died due to leukemia 79 months, postoperatively. Patients with titanium prosthesis had a median follow-up period of 128 months (mean, 111 months; range, 3-212 months) and 146 months for the surviving patients. At the final follow-up, 31 patients had no evidence of disease, 2 patients were alive with disease, and 9 patients had died of the disease (median follow-up period, 51 months). Only patients with bone or soft-tissue tumors with osseous infiltration and stage III giant-cell tumors were included. Patients who had previously undergone treatment with an intralesional procedure (eg, curettage, osteosynthesis due to a pathologic fracture) were also included. In contrast, patients who had received their current megaprosthesis after a failed megaprosthesis were excluded. Patients with an extra-articular knee resection were excluded. The clinical charts for the 56 patients treated with a silver-coated megaprosthesis were assessed prospectively, with particular attention being given to demographic data, diagnosis, preoperative intralesional procedures, pathologic fracture, preoperative leukocyte count, adjuvant or neoadjuvant therapy, reconstruction length, operating time, muscle flaps, skin grafting, and complications. Special emphasis was given to revision operations due to mechanical failures (eg, change of the bushing, aseptic loosening, periprosthetic fracture; Table 1). Surgery was carried out in both groups in the same operating rooms with laminar air flow; staff did not use body-exhaust suits. Postoperatively, all patients received an intravenous thirdgeneration cephalosporin for 3-7 days, followed by oral therapy with a second-generation cephalosporin until wound healing was achieved. The proximal tibia arthroplasties were routinely combined with a tube for soft-tissue refixation [10,11]. Table 1 Data of 98 Patients Who Received Proximal Tibia Arthroplasties. Titanium (n ¼ 42) Leukocyte count (median) Previous intralesional operations (%) Diagnoses (%) Chemotherapy (%) Radiotherapy (%) Median reconstruction length, mm Median operating time, min Wound healing problems Superficial (%) Deep/hematoma (%) Revision operations (mechanical failure, %) 3.2 9.5 Osteosarcoma (78.5) Ewing sarcoma (11.9) Chondrosarcoma (4.7) Silver (n ¼ 56) 4.6 16.1 90.5 7.1 145 Osteosarcoma (55.4) Ewing sarcoma (19.6) GCT (8.9) MFH (7.1) 80.0 3.6 140 245 220 11.9 7.1 50.0 10.7 7.1 14.3 GCT, giant-cell tumor; MFH, malignant fibrous histiocytoma. 2209 An implant-associated infection was diagnosed in accordance with the Musculoskeletal Infection Society criteria [12]. However, using the Musculoskeletal Infection Society criteria, 2 patients would have had no infection in the silver group (number 1 and 3 in Table 2). Both patients had a clearly elevated C-reactive protein level, wound secretion, and redness of the distal wound directly over the prosthesisdbut without a clear fistula. Therefore, we evaluated this clinical scenario in immunocompromised patients as a periprosthetic infection. Table 2 summarizes the data for patients with periprosthetic infection. In patients with periprosthetic infection, curedwith no clinical signs of inflammation and negative C-reactive protein level findingsdwas assessed by the treating clinician at the date of the last available follow-up. Treatment for periprosthetic infection was documented at the final follow-up. Statistical Analysis The primary end point of the study was periprosthetic infection without any previous revision surgery. The secondary end point was the outcome of treatment for any periprosthetic infection that occurred. Event-free survival of the prosthesis relative to the parameter of infection was assessed using the Kaplan-Meier survivorship analysis. Possible risk factors for periprosthetic infection were screened using univariate analysis for the whole patient group and for the titanium and silver subgroups. Comparison of the infection rates between the silver and titanium groups was done using the chi-square test. Results Statistically Significant Risk Factors for Periprosthetic Infection Univariate analysis of the whole study group (n ¼ 98) identified only superficial wound healing disturbances as a significant risk factor for infection (P ¼ .04). Significant influences on the risk of infection were noted only in the silver group, in relation to prior intralesional surgery (P ¼ .04) and operating time (P ¼ .001). It should be emphasized that revision surgery due to mechanical failures, which occurred in 14.3% of cases in the silver group and 50% of those in the titanium group, did not have a significant influence on the infection rate (Table 1). Incidence of Periprosthetic Infection In the titanium group, an infection rate of 16.7% (7 of 42) was noted when the occurrence of infection was the primary end point. In the silver group, the infection rate was only 8.9% (5 of 56). The difference was not statistically significant (P ¼ .247; Table 3). The 5-year event-free survival rates for the prosthesis relative to the parameter of infection were 90% (95% confidence interval [CI], 81.5-98.7) in the silver group and 84% (95% CI, 73.2-96.4) in the titanium group. The 10-year survival rate in the titanium group was 81% (95% CI, 68.2-94.2), as only 1 patient developed an infection after 5 years (Fig. 1; P ¼ .415). Overall, 7 of the 56 patients in the silver group (12.5%) developed periprosthetic infections; 2 patients became infected after revision surgery after mechanical failure of the prosthesis (Table 2). In the titanium group, 1 patient developed a periprosthetic infection after revision surgery (which was required in 50% of patients) due to a mechanical failure of the prosthesis, resulting in an overall infection rate of 19.0% (8 of 42). None of the patients who died of disease during a median of 16 months postoperatively had periprosthetic infections in the silver group, whereas 2 patients (patients 12 and 13) with 2210 J. Hardes et al. / The Journal of Arthroplasty 32 (2017) 2208e2213 Table 2 Characteristics of the 15 Patients With Periprosthetic Infection. Type of Revision Patient Age (y) Silver Interval to Infection Any Revision Surgery Surgery Due to Mechanical Coating After Primary Failure Before Infection Operation (mo) Interval Between Revision Surgery and Infection (mo) Fistula Isolated Microorganism C-Reactive Protein Level (mg/dL) 1 2 3 4 74 38 16 60 Yes Yes Yes Yes 6 8 3.5 77 No No No Yes d d d 66 No No No No No MRSA No P. aeruginosa 5 63 Yes 69 Yes 2 Yes S. caprae 6 18 Yes 19 No d d d Change of the femur stem due to periprosthetic fracture Change of the femur stem due to aseptic loosening d d No 7 8 9 10 67 16 15 10 Yes No No No 9 1 47 1 No No No No d d d d d d d d No Yes No No 11 12 13 14 15 14 16 21 60 14 No No No No No 71 18 5 18 99 No No No No Yes d d d d Change of the bushing d d d d 3 No No No No No S. caprae, Streptococcus agalactiae S. epidermidis No S. pyogenes S. epidermidis, MRSA (at second infection) S. aureus S. epidermidis S. haemolyticus S. epidermidis, E. faecalis S. lugdunensis 5.1 20.2 12.4 15.6 0.5 28.7 8.5 25.7 36.5 4.8 36.8 1.5 0.5 14.7 17.0 MRSA, methicillin-resistant Staphylococcus aureus; P., Pseudomonas; S., Staphylococcus; E., enterococcus. titanium prosthesis developed periprosthetic infections in the first 2 postoperative years and ultimately died of the disease. Time to Periprosthetic Infection In the titanium group, periprosthetic infection led to a surgical intervention at a median of 18 months (range, 1-71 months) after implantation of the prosthesis, without any previous revision surgery. In the silver group, periprosthetic infection occurred at a median of 8 months (range, 3.5-19 months) after primary implantation of the prosthesis in 5 patients without any previous revision surgery (Table 2). In 2 patients with periprosthetic infection after mechanical revision surgery, infection developed 2 months and 66 months postoperatively, respectively. In the titanium group, 1 patient developed infection after revision surgery 3 months postoperatively. Overall, 9 of 12 (75%) periprosthetic infections in the 2 groups occurred within the first 2 postoperative years, if no later revision surgery due to mechanical failure was necessary. Although 3 of the 8 patients in the titanium group (37.5%) ultimately had to undergo amputation due to an infected proximal tibia arthroplasty, this type of mutilating surgical procedure was only necessary in 1 patient in the silver group (14.3%; Table 3). It must be borne in mind here, however, that 2 of the 3 amputations in the titanium group were carried out in patients who had previously undergone radiotherapy, resulting in poor soft-tissue conditions. Two-stage revision surgery with a temporary antibiotic-impregnated cement spacer was ultimately successful in 4 of 8 patients in the titanium group (50.0%), but this was necessary in only 1 patient (14.3%) in the silver group (Table 3). In the silver group, by contrast, antibiotic treatment alone (n ¼ 1, 14.3%, follow-up 72 months) and minor revision surgery (n ¼ 2, 28.6%, follow-up 2 and 82 months, respectively) with 1-stage exchange of the prosthetic body without removal of the stems were ultimately successful. Discussion Table 3 Infection Rates and Ultimately Successful Treatments for Infection. Patients with infection as a primary end point (n) Infection rate in patients with no revision surgery (%) Patients with infection over the whole study period (n) Secondary infection rate (%) Antibiotic treatment, n (%) One-stage prosthesis exchange without stem removal, n (%) Two-stage prosthesis exchange without stem removal, n (%) Two-stage exchange of whole prosthesis, n (%) Explantation of prosthesis and permanent spacer, n (%) Amputation, n (%) Treatment of Periprosthetic Infection Silver (n ¼ 56) Titanium (n ¼ 42) Total 5 7 12 8.9 16.7 11.2 7 8 15 12.5 1 (14.3) 2 (28.6) 19.0 0 0 15.3 1 (7.1) 2 (13.3) 0 1 (12.5) 1 (6.7) 1 (14.3) 4 (50) 5 (33.3) 2 (28.6) 0 2 (13.3) 1 (14.3) 3 (37.5) 4 (26.7) Periprosthetic infection of megaprosthesis continues to be a common and serious complication in orthopedic oncology [2,3,13]. In a systematic review of the literature including a total of 4838 patients with a tumor endoprosthetic reconstruction of the lower extremity, Racano et al [13] reported periprosthetic infection in 10% of cases. However, the authors do not provide any data on the infection rate relative to the site of endoprosthetic arthroplasty. However, it is well known that patients with proximal tibia arthroplasties, in particular, are at high risk for periprosthetic infection, with rates ranging from 14% to 36% [5,14,15]. The high infection rates reported with the use of tumor endoprosthesis in the area of the proximal tibia emphasize the importance of reducing the infection rate even further. Silver has been used as an antimicrobial agent for centuries [16]. It has been used successfully in the topical treatment of burns and chronic wounds and as a coating for medical devices [17]. However, negative results with silver-coated devices have also been reported [18e20]. J. Hardes et al. / The Journal of Arthroplasty 32 (2017) 2208e2213 2211 Fig. 1. Kaplan-Meier survival curve, showing infection-free survival of the primary implant in the silver and titanium groups. The potential benefits of silver-coated orthopedic hardware are still as yet unproved [17]. Silver coating of orthopedic megaprosthesis was first reported by our group in an animal trial [7] and in humans [8]. We also reported that there was a lack of toxicologic side effects with silvercoated megaprosthesis [8]. Glehr et al [21] confirmed these results in patients treated with a silver-coated prosthesis but documented local asymptomatic argyria in 23% patients. Studies dealing with silver-coated megaprosthesis have mainly used them in cases of previous periprosthetic infection or other revision surgery and not as the primary implant [21,22]. Glehr et al [21] reported an infection rate of 12.5% in 32 patients treated with a silver-coated MUTARS tumor endoprosthesis. However, 28 patients had a previous periprosthetic infection. In a recently published matched control study, Wafa et al [22] compared infection rates between an uncoated tumor prosthesis (Stanmore Implants) and a silver-coated implant (Agluna, Stanmore Implants). In this study as well, however, most of the patients were treated with a silver-coated prosthesis for 1-stage or 2-stage revision after periprosthetic infection. The key message of the study was the significantly lower (P ¼ .05) reinfection rate after a 2-stage revision with silver-coated implants (15%) in comparison with uncoated implants (42.9%). To the best of our knowledge, the first and still the only study dealing with silver-coated megaprosthesis in the proximal femur and proximal tibia to prevent periprosthetic infection was published in 2010 by our own group [9]. In that study, the infection rate with 51 silver-coated prostheses was compared with the data for 74 patients in whom uncoated titanium megaprostheses were implanted. Periprosthetic infection was observed in 5.9% patients who received silver-coated prostheses in comparison with 17.6% patients treated with a titanium prosthesis (P ¼ .062). Specifically, for patients with a proximal tibia arthroplasty, the overall infection ratedinfection of the primary implant or infection after revision surgery of the primary implant due to mechanical failuredwas reduced from 17.1% in the titanium group to 6.9% in the silver group (P ¼ .289). However, both due to the short follow-up period and also the small numbers of patients, the results only provide initial evidence of the potential effectiveness of silver coating. Within a period of 6 years, our sarcoma center has succeeded both in substantially increasing the number of patients receiving silver-coated proximal tibia arthroplasties for a rare tumor location and also in achieving a much longer follow-up. Although the overall infection rate increased to 12.5% in the silver group in comparison with our 2010 report [9], it is markedly below the value of 19% in the titanium group. In comparison, Puchner et al [15] noted an overall infection rate of 24.7% with uncoated proximal tibia arthroplasties. With regard to the infection rate in the primary implant alone (without including revision operations), silver coating can lead almost to a halving of the figure, at 8.9% vs 16.7% in the titanium group. By comparison, Puchner et al [15] noted an infection rate in 12.3% of primary implants that were not silver coated. Wafa et al [22] reported on 18 patients with silver-coated proximal tibia arthroplasties. However, only 9 patients underwent primary implantation, whereas the remainder received 2212 J. Hardes et al. / The Journal of Arthroplasty 32 (2017) 2208e2213 silver-coated prostheses during 1-stage or 2-stage exchanges. Infection occurred in 1 of 9 patients (11.1%). Although it was not possible to demonstrate a statistically significant reduction in the periprosthetic infection rate, the present study confirms our initial results from 2010 indicating that silver-coated tumor prostheses are apparently able to reduce the infection rate. But why has the decline in the infection rate not been clearer? In our view, this may be explained by the fact that active, free, silver ions bind to proteins and become inactivated [23]. This means that the surgeon has to avoid hematoma and poor muscle coverage of the prosthesis, resulting in superficial wound healing problems, which can result in bacterial colonization. In these areas, the silver coating is unable to develop an adjuvant effect. The silver coating can inhibit bacterial colonization of the prosthetic body, with subsequent periprosthetic infection, and can kill bacteria near the prosthesis. In our view, the development of periprosthetic infection cannot normally be attributed to bacterial resistance to the silverdalthough this is in principle possible with Gramnegative bacteria [16]dbut instead results from inactivation of the free silver ions owing to binding to proteins. Revision surgery for a tumor endoprosthesis may also be associated with a not-inconsiderable risk of periprosthetic infection [4,15], with bacterial contamination taking place during the revision procedure. Puchner et al [15] reported that 10 of 81 patients (12.3%) developed periprosthetic infection with proximal tibia arthroplasties after revision surgery performed for other reasons. Overall, 10 of 20 infections (50%) occurred after revision surgery. In the present study, previous revision surgery might have been responsible for periprosthetic infection in only 3 patients (2 in the silver group and 1 in the titanium group) among 15 patients with a periprosthetic infection (20%). A significant risk factor is not evident in the present study, but it cannot of course be excluded in the future. In the present study, 75% of periprosthetic infections in both groups occurred within the first 2 postoperative years. However, it is possible that further periprosthetic infections may become clinically apparent in the silver group later, as the silver helps to control infection but may dissociate from the prosthetic surface over time. In the case of periprosthetic infection, silver ions will go into solution, since the surrounding tissue has a negative pH value. If the infection cannot be controlled, the silver ions can in principle degrade completely away from the prosthetic surface, and the infection will become clinically apparent. In clinical reality, however, periprosthetic infection in the titanium group led to surgical interventionsda median of 18 months after implantation of the prosthesis without any previous revision surgery. In contrast, periprosthetic infection in the silver group occurred earlier after primary implantation of the prosthesis. We would, therefore, assume that in spite of the shorter follow-up period in the silver group, no further substantial change can be expected in the groupdunless further revision operations become necessary due to mechanical complications. In addition to the reduction in the rate of periprosthetic infection as the primary end point of the study, attention also needs to be given as a secondary end point to the implications of infections that occur nevertheless. Despite the small group of patients, at least a trend can be noted toward less-invasive treatment measures in the silver group in the presence of periprosthetic infectiondsuch as debridement, antibiotics, irrigation, and retention and 1-stage revision. In the aforementioned study, Wafa et al [22] also showed that in cases of periprosthetic infection of uncoated tumor prosthesis, 1-stage exchanges of the prosthesis for a silver-coated one were only followed by reinfection in 2 of 39 patients (5.1%). By contrast, repeat infections occurred in 5 of 40 patients (12.5%) with 1-stage exchanges of the prosthesis for an uncoated one. There are some studies in the literature that report a high percentage of secondary amputations due to periprosthetic infection, in 19%e46% of cases, with the highest rate in proximal tibia arthroplasties [2,6,14]. Whereas in the titanium group 37.5% of patients ultimately had to undergo amputation in the present study, these mutilating surgical procedures were only necessary in the silver group in one patient (14.3%). The most important limitation of the present study is the retrospective nature of the titanium group, whereas the data for the silver group were collected prospectively. The patient numbers are still small, of course, but in our opinion, they are large enough for such a rare procedure. The advantage of this study lies in the fact that an implant system was used that has been used over many years, always in the same surgical setting and only by a few experienced surgeons. Conclusions Silver represents a reasonable addition to the armamentarium for the treatment of periprosthetic infection. However, it would be unrealistic to assume that periprosthetic infection can be completely avoided, since active, free, silver ions can only exert their effects in close proximity to the prosthetic surface. In cases of periprosthetic infection, despite the use of silver-coated prosthesis, minor revision surgery or even adequate antibiotic therapy alone may be successful. In the future, studies with larger numbers of patients and longer follow-up periods are warranted to confirm these results. References [1] Gosheger G, Gebert C, Ahrens H, Streitbuerger A, Winkelmann W, Hardes J. Endoprosthetic reconstruction in 250 patients with sarcoma. Clin Orthop Relat Res 2006;450:164e71. [2] Hardes J, Gebert C, Schwappach A, Ahrens H, Streitburger A, Winkelmann W, et al. Characteristics and outcome of infections associated with tumor endoprostheses. Arch Orthop Trauma Surg 2006;126:289e96. [3] Jeys LM, Grimer RJ, Carter SR, Tillman RM. Periprosthetic infection in patients treated for an orthopaedic oncological condition. J Bone Joint Surg Am 2005;87:842e9. [4] Jeys LM, Kulkarni A, Grimer RJ, Carter SR, Tillman RM, Abudu A. Endoprosthetic replacement for the treatment of musculoskeletal tumors of the appendicular skeleton and pelvis. J Bone Joint Surg Am 2008;90:1265e71. [5] Grimer RJ, Carter SR, Tillman RM, Sneath RS, Walker PS, Unwin PS, et al. Endoprosthetic replacement of the proximal tibia. J Bone Joint Surg Br 1999;81:488e94. [6] Jeys LM, Grimer RJ, Carter SR, Tillman RM. Risk of amputation following limb salvage surgery with endoprosthetic replacement in a consecutive series of 1261 patients. Int Orthop 2003;27:160e3. [7] Gosheger G, Hardes J, Ahrens H, Streitburger A, Buerger H, Erren M, et al. Silver-coated megaendoprostheses in a rabbit modeldan analysis of the infection rate and toxicological side effects. Biomaterials 2004;25:5547e56. [8] Hardes J, Ahrens H, Gebert C, Streitbuerger A, Buerger H, Erren M, et al. Lack of toxicological side-effects in silver-coated megaprostheses in humans. Biomaterials 2007;28:2869e75. [9] Hardes J, von Eiff C, Streitbuerger A, Balke M, Budny T, Henrichs MP, et al. Reduction of periprosthetic infection with silver-coated megaprostheses in patients with bone sarcoma. J Surg Oncol 2010;101:389e95. €dl R, Hoffmann C, Bürger H, et al. Soft [10] Gosheger G, Hillmann A, Lindner N, Ro tissue reconstruction of megaprostheses using a Trevira tube. Clin Orthop Relat Res 2001;393:264e71. [11] Hardes J, Ahrens H, Nottrott M, Dieckmann R, Gosheger G, Henrichs MP, et al. Attachment tube for soft tissue reconstruction after implantation of a megaendoprosthesis. Oper Orthop Traumatol 2012;24:227e34. [12] Parvizi J, Gehrke T. International Consensus Group on Periprosthetic Joint Infection. Definition of periprosthetic joint infection. J Arthroplasty 2014;29: 1331. [13] Racano A, Pazionis T, Farrokhyar F, Deheshi B, Ghert M. High infection rate outcomes in long-bone tumor surgery with endoprosthetic reconstruction in adults: a systematic review. Clin Orthop Relat Res 2013;471:2017e27. [14] Myers GJ, Abudu AT, Carter SR, Tillman RM, Grimer RJ. The long-term results of endoprosthetic replacement of the proximal tibia for bone tumours. J Bone Joint Surg Br 2007;89:1632e7. J. Hardes et al. / The Journal of Arthroplasty 32 (2017) 2208e2213 €hler C, [15] Puchner SE, Kutscha-Lissberg P, Kaider A, Panotopoulos J, Puchner R, Bo et al. Outcome after reconstruction of the proximal tibiadcomplications and competing risk analysis. PLoS One 2015;10:e0135736. [16] Randall CP, Gupta A, Jackson N, Busse D, O'Neill AJ. Silver resistance in Gramnegative bacteria: a dissection of endogenous and exogenous mechanisms. J Antimicrob Chemother 2015;70:1037e46. [17] Politano AD, Campbell KT, Rosenberger LH, Sawyer RG. Use of silver in the prevention and treatment of infections: silver review. Surg Infect 2013;14: 8e20. [18] Dahlberg PJ, Agger WA, Singer JR, Yutuc WR, Newcomer KL, Schaper A, et al. Subclavian hemodialysis catheter infections: a prospective, randomized trial of an attachable silver-impregnated cuff for prevention of catheter-related infections. Infect Control Hosp Epidemiol 1995;16: 506e11. 2213 [19] Riley DK, Classen DC, Stevens LE, Burke JP. A large randomized clinical trial of a silver-impregnated urinary catheter: lack of efficacy and staphylococcal superinfection. Am J Med 1995;98:349e56. [20] Tokmaji G, Vermeulen H, Müller MC, Kwakman PH, Schultz MJ, Zaat SA. Silvercoated endotracheal tubes for prevention of ventilator-associated pneumonia in critically ill patients. Cochrane Database Syst Rev 2015;12:CD009201. [21] Glehr M, Leithner A, Friesenbichler J, Goessler W, Avian A, Andreou D, et al. Argyria following the use of silver-coated megaprostheses. Bone Joint J 2013;95:988e92. [22] Wafa H, Grimer RJ, Reddy K, Jeys L, Abudu A, Carter SR, et al. Retrospective evaluation of the incidence of early periprosthetic infection with silvertreated endoprostheses in high-risk patients. Bone Joint J 2015;97:252e7. [23] Schierholz JM, Lucas LJ, Rump A, Pulverer G. Efficacy of silver-coated medical devices. J Hosp Infect 1998;40:257e62.