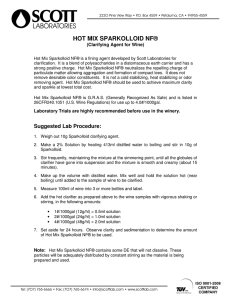
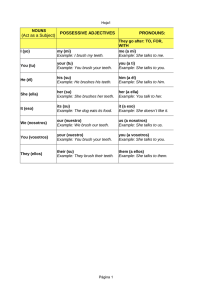
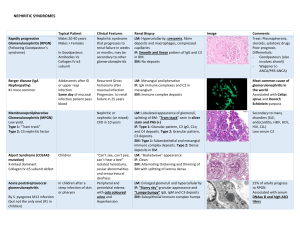
Case Report Hallermann‑Streiff Syndrome Jayakar Thomas, B Sindhu Ragavi, PK Raneesha, N Ashwak Ahmed, S Cynthia, D Manoharan, R Manoharan From the Department of Dermatology, Sree Balaji Medical College, Chromepet, Chennai, India Abstract Hallermann-Streiff syndrome (HSS) is a rare disorder characterized by dyscephalia, with facial and dental abnormalities. We report a 12-year-old female child who presented with abnormal facial features, dental abnormalities and sparse scalp hair. Key Words: Abnormal facial features, dental anomalies, Hallermann‑Streiff syndrome Discussion What was known? Hallerman‑Strieff syndrome as a rare genetic disorder is known to occur with multiple abnormalities. It seems that the first record of this disorder was made by Aubry[3] in 1893. More than 150 cases of HSS have been reported till date. Virtually all cases are sporadic and thus there is no obvious pattern of inheritance. The most likely hypothesis is that of a single mutant gene (dominant) with most cases representing fresh mutations. Recently a defect of elastin and abnormal glycoprotein metabolism has been reported.[4] Introduction Hallerman‑Strieff syndrome (HSS), occulomandibulodyscephaly was first described completely in 1948 by Hallermann and then in 1950 by Streiff.[1] Seven essential signs were described by Francois as diagnostic criteria for HSS. Our patient had five of the seven signs of this syndrome and there were no ocular abnormalities. Physical growth and development was retarded however, mental development was normal in our patient. In addition Port wine stain was present in this patient. This has not been reported earlier to the best of the knowledge of the authors. The lenses of patients with HSS are described as white and liquefied and often resorb spontaneously. Other ophthalmic findings that have been reported include blue sclera, nystagmus, strabismus, down slanting palpebral fissures, glaucoma, aniridia, and sclerocornea. Seven essential signs described by Francois as diagnostic criteria for HSS: These signs are dyscephalia and bird face, dental abnormalities, proportionate short stature, hypotrichosis, atrophy of skin especially on nose, bilateral microphthalmos, and congenital cataract.[2] Other systemic abnormalities of potential importance include trachea malacia. Case Report A 12‑year‑old girl brought by her mother was seen for abnormal appearance and skin changes. She was the second child of consanguineous parents (cousins from second rank) and was born preterm on 7th month of eventful normal delivery. Her medical history revealed the presence of bilateral direct congenital hernia, delayed closure of fontanelles, delayed milestones and hypothyroidism. Examination revealed facial characteristics typical of the “bird face” in HSS [Figure 1]. The nose appeared thin, sharp and hooked; hypoplastic mandible; high arched palate, mal implantation of teeth [Figure 2]. Propotionate dwarfism was present. Dermatological examination revealed sparse scalp hair, alopecia along lines of suture [Figure 3], atrophy of skin in central part of face. A large port wine stain of size 10 cm was present on left side of neck [Figure 4]. Her eyes were normal and there was no tracheomalacia. Other systemic abnormalities of potential importance include trachea malacia and upper airway obstruction, which can lead to chronic respiratory embaressment.[5] An infant was reported with six of the seven essential signs, except microphthalmos. Other uncommon ocular features like districhiasis, ptosis, iris atrophy, peripapillary choroidal atrophy, cherry red spot at macula, pale discs, and coloboma at the entrance of optic nerve have also been reported.[6] Association of HSS with port wine stain is not yet reported in the literature. Absence of clinodactyly or clitoral enlargement and photosensitivity or deafness; will possibly exculde bird‑headed dwarf of Seckel and Cockayne syndrome, respectively, though these have in common the Both the parents were counseled. Detailed oral hygiene instructions and dietary recommendations were given to the parents. Laser treatment is being planned for the port wine stain. The child is being followed up by us, the dentist and pediatrician. Access this article online Quick Response Code: Website: www.e‑ijd.org Address for correspondence: Dr. Jayakar Thomas, 135, East Mada Church Road, Royapuram, Chennai ‑ 600 013, India. E‑mail: jayakarthomas@ gmail.com DOI: 10.4103/0019-5154.117311 383 Indian Journal of Dermatology 2013; 58(5) Thomas, et al.: Hallermann-streiff syndrome Figure 1: Bird like facies with hypoplasia of mandible. A port wine stain on the left side of neck is partially seen Figure 2: Mal implantation of teeth Figure 3: Alopecia along suture lines Figure 4: Port wine stain on left side of neck bird facies. Except microcephaly, the other major or minor criteria for Cowdens disease were absent in this child. What is new? Association with port wine stain is so far not reported in literature. The dental examination is as important as there is a massive malformation of cranium and craniofacial region. From the clinical point of dentistry, it is characterized by hypoplasia of mandible, restricted movement of jaw, narrow oral cavity, narrow highly arched palate, shortened root length of teeth, presence of neonatal teeth (tooth present at birth), and sometimes hypodontia (missing of some tooth), or partial anodontia (absence of series of teeth). Enamel hypoplasia is also common causing carious teeth, and there is improper alignment of teeth in most of the cases. References 1. 2. 3. 4. 5. Unsatisfactory data for HSS in the literature together with cooperation problems, respiratory challenges, small mouth and mobility of the mandibular segments due to the absence of fusion on the symphysis region affected all treatment procedures. An interdisciplinary approach, early preventive‑care programs, detailed oral hygiene instructions and dietary recommendations, counseling to the parents are the essential procedures for the patients with HSS. Indian Journal of Dermatology 2013; 58(5) 6. Hoefnagel D, Benirschke K. Dyscephalia mandibulooculo‑facialis. Arch Dis Child 1965;40:57‑61. Francois J. A new syndrome: Dyscephalia with bird face and dental anomalies, nanism, hypotrichosis, cutaneous atrophy, microphthalmia, and congenital cataract. AMA Arch Ophthalmol 1958;60:842‑62. Casperson I, Warburg M. Hallerman‑Streiff syndrome. Acta Ophthalmol (Copenh) 1968;46:385‑90. Francois J. A new syndrome. Arch Ophthalmol 1958;60:812‑42. Maus M. Basic Anatomy of the Orbit in Albert and Jakobiec’s Principles and Practice of Ophthalmology, Saunders Elsevier, St. Louis, 3rd edition, vol. 3; 2008. p. 4213-5. Nicholson AD, Menon S. Hallerman‑Streiff syndrome. J Postgrad Med 1995;41:22‑3. How to cite this article: Thomas J, Ragavi BS, Raneesha PK, Ahmed NA, Cynthia S, Manoharan D, et al. Hallermann-Streiff syndrome. Indian J Dermatol 2013;58:383-4. Received: March, 2012. Accepted: May, 2012. Source of support: Nil, Conflict of Interest: Nil. 384 Copyright of Indian Journal of Dermatology is the property of Medknow Publications & Media Pvt. Ltd. and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.