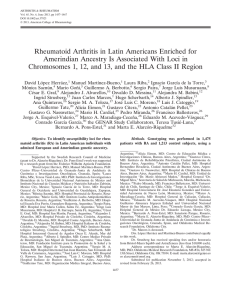
513 C OPYRIGHT Ó 2015 BY T HE J OURNAL OF B ONE AND J OINT S URGERY, I NCORPORATED Investigating the Relationship Between Ankle Arthrodesis and Adjacent-Joint Arthritis in the Hindfoot A Systematic Review Jeffrey S. Ling, MBBS, FRACS(Orth), Niall A. Smyth, MD, Ethan J. Fraser, MD, MaCalus V. Hogan, MD, Christine M. Seaworth, MD, Keir A. Ross, MD, and John G. Kennedy, MD, FRCS(Orth) Investigation performed at the Department of Foot and Ankle Surgery, Hospital for Special Surgery, New York, NY Background: Ankle arthrodesis traditionally has been regarded as the treatment of choice for many patients with endstage ankle arthritis. However, a major reported risk of ankle arthrodesis is adjacent-joint degeneration. There are conflicting views in the literature as to the causative link between ankle arthrodesis and progression to adjacent-joint arthritis. Recent studies have challenged the causative link between arthrodesis and adjacent-joint arthritis, purporting that preexisting adjacent-joint arthritis is present in many patients. The aim of the present study was to systematically review the available literature to determine if there is sufficient evidence to support either hypothesis. Methods: A literature search of the EMBASE and PubMed/MEDLINE databases (1974 to present) was performed. A total of twenty-four studies were included for review. The studies were reviewed, and the relevant information was extracted, including research methodology, postoperative outcomes in the adjacent joints of the foot, and whether pre-arthrodesis radiographs and medical records were available for analysis. Results: The twenty-four manuscripts included eighteen clinical studies, five biomechanical studies, and one gaitanalysis study. The majority of biomechanical studies showed altered biomechanics in the fused ankle; however, there was no clear consensus as to whether these findings were causes of adjacent-joint arthritis. In studies assessing clinical outcomes, the reported prevalence of subtalar joint arthritis ranged from 24% to 100% and the prevalence of talonavicular and calcaneocuboid arthritis ranged from 18% to 77%. Correlation between imaging findings of arthritis in adjacent joints and patient symptoms was not established in a number of the clinical studies reviewed. Conclusions: There is no true consensus in the literature as to the effects of ankle arthrodesis on biomechanics or whether ankle arthrodesis leads to adjacent-joint arthritis. Similarly, a correlation between postoperative imaging findings and clinical presentation in this cohort of patients has not been conclusively demonstrated. Level of Evidence: Prognostic Level IV. See Instructions for Authors for a complete description of levels of evidence. Peer Review: This article was reviewed by the Editor-in-Chief and one Deputy Editor, and it underwent blinded review by two or more outside experts. The Deputy Editor reviewed each revision of the article, and it underwent a final review by the Editor-in-Chief prior to publication. Final corrections and clarifications occurred during one or more exchanges between the author(s) and copyeditors. A nkle arthrodesis has long been regarded as a reliable treatment for end-stage ankle arthritis1,2. The general principles of alleviating pain and restoring function have remained unchanged for over a century, and modern techniques yield good results with a low complication rate3-8. A major reported risk of ankle arthrodesis is adjacent-joint degeneration, with many Disclosure: None of the authors received payments or services, either directly or indirectly (i.e., via his or her institution), from a third party in support of any aspect of this work. One or more of the authors, or his or her institution, has had a financial relationship, in the thirty-six months prior to submission of this work, with an entity in the biomedical arena that could be perceived to influence or have the potential to influence what is written in this work. Also, one or more of the authors has had another relationship, or has engaged in another activity, that could be perceived to influence or have the potential to influence what is written in this work. The complete Disclosures of Potential Conflicts of Interest submitted by authors are always provided with the online version of the article. J Bone Joint Surg Am. 2015;97:513-9 d http://dx.doi.org/10.2106/JBJS.N.00426 514 TH E JO U R NA L O F B O N E & JO I N T SU RG E RY J B J S . O RG V O L U M E 97-A N U M B E R 6 M A R C H 18, 2 015 d d d R E L AT I O N S H I P B E T W E E N A N K L E A R T H R O D E S I S A N D A D J A C E N T -J O I N T A R T H R I T I S I N T H E H I N D F O O T TABLE I Biomechanical and Gait-Analysis Studies Authors Study Focus Study Details Study Findings 34 Effect of tibiotalar joint arthrodesis on adjacent tarsal joint pressure in a cadaver model 12 cadaver feet loaded axially on varying uphill inclines from 0° to 30°, with pressure and contact area measured in talonavicular, subtalar, and calcaneocuboid joints Significant increase in pressure in talonavicular and calcaneocuboid joints on 10° (p < 0.001) and 20° (p = 0.002) inclines 30 Gait analysis and functional outcomes following ankle arthrodesis for isolated ankle arthritis Retrospective study; n = 26; mean follow-up, 44 months Significant (p < 0.05) decrease in motion in all 3 planes of hindfoot and midfoot in stance and swing. Decrease in cadence and stride length 31 Effect of tibiotalar arthrodesis on foot kinematics and ground reaction force progression during walking N = 9, three-dimensional gait analysis performed, comparison with a matched control group Earlier forward displacement of ground reaction force, ground reaction force more posterior at heel-off, increased stress on midfoot during stance Kinematic changes after arthrodesis and total replacement of the ankle. Part 1: range of motion. Part 2: movement transfer 6 cadaver legs; axial load, 200 N; motion sensors on all contiguous bones; moments applied in coronal and sagittal planes and rotation; intact/fused/total ankle arthroplasty states tested Motion substantially decreased in all planes in the fused ankle, tibial rotation and foot inversion/eversion increased with dorsiflexion/plantar flexion of foot Plantar pressure distribution after tibiotalar arthrodesis Plantar pressures measured in 20 patients at mean of 2 yr after arthrodesis and compared with other side Plantar pressure largely unaffected in most areas of foot Jung et al. Thomas et al. Beyaert et al. 32,33 Valderrabano et al. 29 Schuh et al. studies demonstrating an increased prevalence of arthritis of the ipsilateral hindfoot and midfoot after ankle arthrodesis3,9-23. This finding is thought to be due to altered biomechanics, with increased motion and wear through the subtalar and tarsal joints compensating for the loss of ankle motion9,10. As a result of this thinking and the quest for a reliable motion-preserving alternative, substantial efforts have been made to develop and improve total ankle replacements. While recent studies have shown an improvement in outcomes following ankle replacement, arthrodesis continues to be the most widely employed surgical treatment for end-stage ankle arthritis24-27. Several studies have supported the concept that ankle arthrodesis causes adjacent-joint arthritis in the hindfoot. Coester et al.11 and Fuchs et al.10 reported degenerative changes in the Chopart and subtalar joints following ankle arthrodesis, implicating ankle arthrodesis as the direct cause. Both of those studies have been quoted widely because they included long-term followup (mean, twenty-two years [range, twelve to forty-four years] and twenty-three years [range, twenty to thirty-three years], respectively). More recently, however, this implication was challenged by Sheridan et al.28, who argued that those studies may be flawed in their analysis and that there may be other factors influencing adjacent-joint arthritis. Specifically, Sheridan et al.28 noted that many patients undergoing ankle arthrodesis have preexisting degenerative changes in the adjacent joints prior to surgery. Biomechanical and gait-analysis evidence is also conflicting. Schuh et al.29 showed a compensatory increase in motion in the talonavicular, calcaneocuboid, and subtalar joints following ankle arthrodesis, whereas Thomas et al.30 showed a decrease in motion in these joints. Furthermore, the effect of increased or decreased movement in the adjacent joints following ankle arthrodesis appears to be equivocal. Because of the disparity in evidence with regard to progression of adjacent-joint degenerative arthritis, no consensus has been reached on the basis of empirical data. In this context, the aim of the present study was to systematically review the available English-language literature to determine if there is sufficient evidence to support either hypothesis. Materials and Methods Literature Search he terms “(ankle arthrodesis OR ankle fusion OR tibiotalar fusion OR tibiotalar arthrodesis) AND (osteoarthritis OR arthritis OR osteoarthrosis OR degenerative joint disease OR OA or DJD) AND (subtalar OR calcaneocuboid OR talonavicular OR chopart OR transverse tarsal)” were used to search the PubMed/MEDLINE and EMBASE electronic databases (1974 to present) in January 2013. In addition, the references of the included studies were reviewed in order to ensure that no relevant publications were excluded. T Inclusion Criteria Studies were considered for inclusion if they (1) were published in the Englishlanguage literature, (2) assessed the clinical or biomechanical outcomes following ankle arthrodesis, (3) involved biomechanical and gait analyses that were performed with use of a multi-segment foot model, (4) evaluated the radiographic appearance of the subtalar, talonavicular, or calcaneocuboid joint, (5) evaluated the prevalence of subsequent adjacent-joint arthritis following the 515 TH E JO U R NA L O F B O N E & JO I N T SU RG E RY J B J S . O RG V O L U M E 97-A N U M B E R 6 M A R C H 18, 2 015 d d d primary procedure, and (6) were published in a peer-reviewed journal. Studies that exclusively focused on patients with inflammatory arthritis as the etiology for ankle disease were excluded. The literature search was performed by two of the authors, and all of the authors independently reviewed the search results. The title and abstract of all search results were assessed, and studies that were identified for possible inclusion received a full-text review. Authors agreed on the studies that met the inclusion criteria (Fig. 1). Data Extraction A standardized data sheet was prepared, and all authors extracted the relevant information, including research methodology, postoperative outcomes in the adjacent joints of the foot, and whether pre-arthrodesis radiographs and medical records were available for analysis. Postoperative outcomes that were recorded included adjacent-joint symptoms, the existence or exacerbation of arthritis in adjacent joints, the rates of reoperation and adjacent-joint arthrodesis, and any effects on motion of adjacent joints. R E L AT I O N S H I P B E T W E E N A N K L E A R T H R O D E S I S A N D A D J A C E N T -J O I N T A R T H R I T I S I N T H E H I N D F O O T and abstracts, 405 studies were excluded because they did not meet the inclusion criteria. Thirty-eight studies were considered for full-text review, of which fourteen were excluded as they evaluated inflammatory arthritis exclusively, did not provide data on the adjacent joints, were review articles, or were gaitanalysis studies performed with use of a single-segment model (Fig. 1). Twenty-four studies were determined to be eligible for inclusion overall, including eighteen clinical studies, five biomechanical studies, and one gait-analysis study. Three of the latter six studies also provided clinical data. No external funds were received in support of this study. Gait-Analysis Study (Table I) Only one study assessed gait following ankle arthrodesis with use of a multi-segment model30. The study demonstrated a significant decrease in motion of hindfoot and forefoot joints, in all planes and in all phases of stance and swing, compared with the contralateral, unfused side. Results ollowing the removal of duplicates, the literature search yielded 443 relevant publications. After a review of the titles Biomechanical Studies (Table I) Five biomechanical studies investigated motion and pressure changes after ankle arthrodesis. Schuh et al.29 evaluated plantar Source of Funding F Fig. 1 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram for included studies for review. 516 TH E JO U R NA L O F B O N E & JO I N T SU RG E RY J B J S . O RG V O L U M E 97-A N U M B E R 6 M A R C H 18, 2 015 d d d R E L AT I O N S H I P B E T W E E N A N K L E A R T H R O D E S I S A N D A D J A C E N T -J O I N T A R T H R I T I S I N T H E H I N D F O O T TABLE II Clinical Studies on Adjacent-Joint Arthritis: Imaging Findings and Correlation with Symptoms* Adjacent-Joint Arthritis After Arthrodesis Clinical Study Radiographic Evidence 13 Strasser and Turner 37% subtalar joint 33% subtalar joint, 37% talonavicular joint, 45.5% calcaneocuboid joint No correlation NR 35% subtalar joint, 18% talonavicular joint† 30% subtalar joint, 19% talonavicular joint NR NR 43% subtalar joint (high grade)‡ 37% subtalar joint 10% symptomatic NR 24% subtalar joint† NR 50% symptomatic NR 47% moderate-severe osteoarthritis 33% overall Subtalar osteoarthritis correlated with poorer outcomes Adjacent-joint motion reduced 91% subtalar joint, 56% talonavicular joint, 22% calcaneocuboid joint‡ NR Correlation between poorer Kellgren-Lawrence grade and outcome Subtalar joint motion decreased NR 32.5% subtalar joint, 12% talonavicular joint 14% subtalar joint osteoarthritis symptomatic Adjacent-joint movement increased 88% subtalar joint‡ NR Correlation reported NR Mean subtalar KellgrenLawrence grade, >3† Yes Subtalar arthritis correlated with poorer outcomes Adjacent-joint movement reduced 37 59% tarsal joints‡ NR No correlation Variable change in adjacent-joint motion 35 44% overall‡ 27% progressed overall NR Motion same as contralateral side 62% subtalar stiffness NR Not correlated NR NR NR Not significantly correlated Increased adjacentjoint motion 50% Chopart joint, 36% subtalar joint‡ Some progression Poor correlation with symptoms NR ;24% subtalar joint‡ 10.4% subtalar joint 30% symptomatic NR 42% subtalar joint‡ 29% subtalar joint NR NR NR No progression Tarsal joint arthritis correlated with poorer outcomes Reduced movement 15 16 Winson et al. 17 Kopp et al. 18 Buchner and Sabo 11 Coester et al. 9 Takakura et al. 19 Trouillier et al. 10 Fuchs et al. Jackson and Glasgow 21 Boobbyer 36 Sealey et al. 22 Morrey and Wiedeman 23 3 Aaron 20 Schaap et al. 56% Loss of Motion 91% subtalar joint, 77% talonavicular joint† Zwipp et al. Hallock Correlation with Symptoms 100% subtalar joint 14 Hendrickx et al. Abdo and Wasilewski Progression NR *NR = not reported. †Preoperative. ‡Postoperative. pressure distribution in the foot after ankle arthrodesis and showed a moderate increase in pressure in the lateral aspect of the midfoot region in stance phase, but they did not indicate whether the increase was significant. They otherwise found that ankle arthrodesis did not affect the plantar pressure distribution in most regions of the foot. Beyaert et al.31 found an earlier forward displacement of the ground reaction force. Valderrabano et al.32,33 assessed the kinematic changes after ankle arthrodesis in six cadaver specimens and found that the range of motion decreased in all three planes, with inversion and eversion of the foot decreasing slightly and with tibial rotation decreasing markedly. In addition, the authors noted that tibial rotation and foot inversion and eversion increased significantly with dorsiflexion and plantar flexion of the foot. Most recently, Jung et al.34 studied pressure changes in the talonavicular, calcaneocuboid, and subtalar joints in feet that were loaded axially after ankle arthrodesis on varying uphill inclines from 0° to 30°. They found a significant increase in pressure in the talonavicular and calcaneocuboid joints between intact and fused ankles on 10° (p < 0.001) and 20° (p = 0.002) inclines. 517 TH E JO U R NA L O F B O N E & JO I N T SU RG E RY J B J S . O RG V O L U M E 97-A N U M B E R 6 M A R C H 18, 2 015 d d d Clinical Studies (Table II) Study Quality and Design All eighteen clinical studies were retrospective reviews. Of the 675 patients who were included in those studies, 56.4% were male and 43.6% were female. The mean age of the patients was fifty-two years. The mean duration of follow-up for each individual study ranged from two to twenty-three years, with an overall mean of 7.9 years. Etiology of Ankle Arthritis Seventeen studies (94%) evaluated the etiology of arthritis in the patient population. Of these, two included a homogeneous cohort consisting of patients with posttraumatic arthritis11,18. All of the other studies either did not include information on etiology or included a heterogeneous cohort consisting of patients with etiologies such as posttraumatic osteoarthritis (82.3%), primary arthropathy (9.3%), inflammatory arthropathy (4.6%), neuropathic arthropathy (2.7%), and hemophilic arthropathy (1.1%). Effect on Range of Motion in Adjacent Joints Varying results were reported with regard to the clinical outcomes in the adjacent joints following ankle arthrodesis. Abdo and Wasilewski35 evaluated thirty patients at a mean of seven years after ankle arthrodesis and found no difference in tarsal movement compared with the contralateral side. In contrast, Sealey et al.36 and Takakura et al.9 demonstrated a compensatory increase in motion in the adjacent hindfoot joints, with the latter study9 showing that the mean subtalar range of motion increased by 4.1°. Jackson and Glasgow37 showed that tarsal joint mobility increased in 27% of patients, stayed the same in 40%, and decreased in 33% when the contralateral side was used as a control. Overall, four studies showed a decrease in adjacent-joint motion whereas two studies showed an increase and one study showed variable change in adjacent-joint motion. The remaining studies did not include information on adjacent-joint motion after arthrodesis. Prevalence of Arthritic Changes in Adjacent Joints Many studies evaluated the postoperative prevalence of arthritis in the joints of the foot, with the subtalar joint being more frequently affected than either the talonavicular or calcaneocuboid joint3,9-23,38. The reported prevalence of subtalar joint arthritis ranged from 24% to 100%, whereas the reported prevalence of arthritis in the talonavicular and calcaneocuboid joints ranged from 18% to 77%. The talonavicular joint was more frequently affected than the calcaneocuboid joint. Coester et al.11, after a mean duration of follow-up of twenty-three years, showed that the majority of patients in their cohort had moderate to severe restriction in subtalar range of motion and half had tenderness and/or swelling in the hindfoot and midfoot. Fuchs et al.10, after a mean duration of follow-up of twenty-two years, showed that their cohort of eighteen patients had mean osteoarthritis scores of 2.3 and 3.1 for the talonavicular and subtalar joints, respectively, according to the radiographic grading system of Kellgren and Lawrence39. Preexisting Adjacent-Joint Arthritis Five (28%) of the eighteen studies13-16,23 provided the preoperative prevalence of adjacent-joint arthritis. Hallock23 reported on forty- R E L AT I O N S H I P B E T W E E N A N K L E A R T H R O D E S I S A N D A D J A C E N T -J O I N T A R T H R I T I S I N T H E H I N D F O O T eight patients at a mean of four years after arthrodesis. After this relatively short duration of follow-up, only five patients (10.4%) showed progression of adjacent-joint arthritis, with four patients developing arthritis in the subtalar joint and one patient developing arthritis in the talonavicular joint. The authors did not report on the calcaneocuboid joint. In addition, six patients had preexisting arthritis in the subtalar joint and three had preexisting arthritis in the talonavicular joint. The authors did not comment on whether the arthritis progressed in these patients. Aaron3, at a mean of three years after ankle arthrodesis, reported progression to a more severe grading of subtalar arthritis in 29% of the cohort but did not mention the preoperative prevalence of subtalar arthritis. In addition, in the most recent publications13,14, almost all patients undergoing ankle arthrodesis had some degree of subtalar arthritis on preoperative radiographs. Despite this high prevalence of subtalar disease, subtalar arthritis progressed in only thirty-one (34.4%) of ninety patients. The overall prevalence of preexisting arthritis is not clear given the paucity of studies evaluating the preoperative prevalence of adjacent-joint arthritis. Association of Arthritis with Patient Symptoms Although a high prevalence of postoperative radiographic arthritis was reported, this finding often correlated poorly with clinical symptoms10,13,14,21,22,35. Overall, an association between radiographic adjacent-joint arthritis and patient symptoms was seen in six (33%) of the eighteen included studies. Furthermore, within those studies, a mean of 24% of patients had symptoms associated with adjacent-joint arthritis. Hendrickx et al.14 reported that the degree of radiographic arthritis in these joints failed to correlate with visual analog scale (VAS) pain scores. In addition, Strasser and Turner13 found that 44% of patients with subtalar arthritis were asymptomatic. Boobbyer21 found that reduced motion in the subtalar joint did not seem to affect the clinical result and concluded that deterioration in function due to adjacent-joint disease was not a frequent observation. Morrey and Wiedeman22 reported that 82% of their patients with radiographic arthritis in the Chopart joint were asymptomatic, whereas 87% of patients with no radiographic evidence of Chopart joint arthritis were asymptomatic. The studies with the longest durations of follow-up demonstrated conflicting findings. Coester et al.11 reported that pain, swelling, and activity limitation correlated significantly with the Kellgren and Lawrence grade for arthritis in the talonavicular and calcaneocuboid joints at a mean of twenty-two years of follow-up. In contrast, Fuchs et al.10 found no correlation between radiographic results and Short Form-36 (SF-36) scores and no correlation between the functional Olerud-Molander ankle score40 and radiographic scores for the midtarsal joints at a mean of twenty-three years of follow-up. Reoperation Rates for Adjacent-Joint Arthrodesis Of the eighteen clinical studies, four included patients who required further arthrodesis of the adjacent joints9,13,16,35. Of the 675 patients who were included in the eighteen studies, twelve required further adjacent-joint arthrodesis. Nine patients underwent a subtalar arthrodesis, two patients underwent a triple arthrodesis, and one patient underwent a talonavicular arthrodesis. One of the two patients who underwent a triple arthrodesis and 518 TH E JO U R NA L O F B O N E & JO I N T SU RG E RY J B J S . O RG V O L U M E 97-A N U M B E R 6 M A R C H 18, 2 015 d d d the one patient who underwent a talonavicular arthrodesis had an inflammatory arthropathy rather than a degenerative pathology. Because of the heterogeneity of the included studies, our review of the literature did not allow us to correlate findings to operative technique, alignment, or approach. Discussion nkle arthrodesis remains a commonly used procedure for the treatment of end-stage ankle arthritis. Traditionally, concerns have existed over the potential long-term risk of arthritis in the surrounding joints of the foot—in particular, the talonavicular, calcaneocuboid, and subtalar joints. A paucity of data exists to support this concern. The aim of the current systematic review was to establish whether there are sufficient data to provide evidence for this concern. A Gait-Analysis Studies Only one of the available gait-analysis studies on the subject involved the use of a multi-segment model30. That study demonstrated decreased motion in hindfoot and forefoot joints following ankle arthrodesis. However, there is conflicting evidence in previous single-segment models, with one study showing increased motion in the adjacent joints and another showing no change12,38. Those studies were not included in our review, however, as single-segment models consider the foot as a rigid segment and as such are flawed in their analysis of adjacent-joint movement41. As a result of the paucity of evidence and limitations of the gait-analysis models currently available, in addition to the contrasting findings in previous studies, the effect of arthrodesis of the ankle on adjacent-joint movement remains unclear. Biomechanical Studies Jung et al.34, using arthrodesed ankles in a cadaver model, showed a significant increase in pressure in the talonavicular and calcaneocuboid joints on a 10° and a 20° incline as compared with the unfused state. The authors concluded that this pressure increase in dorsiflexion, simulating late stance phase, may be responsible for the late degenerative changes in these joints after ankle arthrodesis. The concern related to that study, however, is that it used only time-zero mechanical data, confounding the conclusions. Schuh et al.29 showed increases in the lateral aspect of the midfoot region during the stance phase of gait, but they did not indicate whether the increases were significant. Ankle arthrodesis was not shown to affect plantar pressure distribution in other regions of the foot in their analysis. Beyaert et al.31 hypothesized that the earlier forward displacement of ground reaction force seen in their study would lead to high stress on the midtarsal joints during stance phase. Valderrabano et al.32,33 found that kinematic changes in the hindfoot after ankle arthrodesis may not fully compensate for normal range of motion in all three planes, leading to increased movement transfer, which the authors postulated may be associated with overloading of the adjacent joints. Overall, the biomechanical studies that were reviewed revealed no consensus on whether ankle arthrodesis might cause arthritis in adjacent joints. R E L AT I O N S H I P B E T W E E N A N K L E A R T H R O D E S I S A N D A D J A C E N T -J O I N T A R T H R I T I S I N T H E H I N D F O O T Clinical Studies Fifteen of the eighteen clinical studies that were retrieved demonstrated radiographic evidence of adjacent-joint arthritis in the foot following ankle arthrodesis3,9-11,13-19,22,23,35,37. However, there are two caveats. First, radiographic arthritis does not correlate strongly with symptoms and patients with adjacent-joint arthritis may even be asymptomatic despite high radiographic scores10,13,14,21,22,35. Second, the development of arthritis in these joints after ankle arthrodesis may be multifactorial and may not be due to the arthrodesis alone. Sheridan et al.28 reported that arthritis in these joints is often preexisting and is not necessarily recorded. Sheridan et al.28 also demonstrated that the majority of studies are retrospective and that radiographs made prior to the ankle arthrodesis are frequently unavailable for analysis. Other possibilities mentioned by those authors are that the abnormality that caused the ankle arthritis, such as the initial trauma or inflammatory disease, may have caused disease in these adjacent joints. In addition, longstanding arthritis in the ankle and alterations in hindfoot kinematics prior to the actual arthrodesis may damage the surrounding joints. Of the eighteen clinical studies that were analyzed, five13-16,23 had the benefit of having pre-arthrodesis radiographs available for analysis, with the majority of these studies being published after 2005. In two of the eighteen studies13,14, almost all patients undergoing ankle arthrodesis had some degree of adjacent-joint arthritis on preoperative radiographs, which is consistent with the findings of Sheridan et al.28. Despite this high prevalence of preexisting arthritis, the severity of arthritis only progressed in roughly one-third of the patients in each cohort. The conclusions from those studies indicate that ipsilateral hindfoot and midfoot arthritis is almost universally present in patients undergoing ankle arthrodesis and that two-thirds of these patients will not experience any progression of disease in these joints and therefore presumably will remain asymptomatic. When considering other treatment options, total ankle replacement is an attractive alternative given the theoretical benefit of motion preservation. However, because of the paucity of long-term data, there is insufficient evidence to recommend total ankle replacement over arthrodesis for all patients at this time42. The principal limitation of this systematic review is the quality of the included publications. Long-term prospective studies with a homogeneous cohort confined to patients with posttraumatic and/or primary osteoarthritis as the etiology of arthritis would be better designed to answer the titled premise. Without knowledge of the state of the surrounding joints, the position of the fusion, and the activity level of the patient, it is not possible to draw conclusions about the likelihood of degenerative change. While many patients undergoing arthrodesis of the ankle develop arthritis in surrounding joints, the cause is not clear from the available studies in the literature. A prospective comparison with baseline assessment of surrounding-joint arthritis is needed. Moreover, radiographic evidence of arthritis is not always clinically important, with patients often being asymptomatic despite high radiographic scores for arthritis. 519 TH E JO U R NA L O F B O N E & JO I N T SU RG E RY J B J S . O RG V O L U M E 97-A N U M B E R 6 M A R C H 18, 2 015 d d d Overview iomechanically, there is no consensus on how ankle arthrodesis might contribute to the pathogenesis of adjacentjoint degeneration. Radiographic evidence of adjacent-joint arthritis in the foot following ankle arthrodesis is seen in studies with a mean duration of follow-up of two to twenty-three years. There is only a weak correlation between radiographic evidence of arthritis and the presence of symptoms in these joints. Further prospective analysis of adjacent joints at baseline and following arthrodesis may help to establish the effects of arthrodesis on adjacent-joint arthritis. n B R E L AT I O N S H I P B E T W E E N A N K L E A R T H R O D E S I S A N D A D J A C E N T -J O I N T A R T H R I T I S I N T H E H I N D F O O T Niall A. Smyth, MD Ethan J. Fraser, MD Christine M. Seaworth, MD Keir A. Ross, MD John G. Kennedy, MD, FRCS(Orth) Department of Foot and Ankle Surgery, Hospital for Special Surgery, 523 East 72nd Street, East River Professional Building, 5th Floor Room 507, New York, NY 10021. E-mail address for K.A. Ross: [email protected] MaCalus V. Hogan, MD Division of Foot and Ankle Surgery, Department of Orthopaedic Surgery, University of Pittsburgh School of Medicine, 3471 Fifth Avenue, Suite 911, Pittsburgh, PA 15232 Jeffrey S. Ling, MBBS, FRACS(Orth) Prince of Wales Hospital Clinical School, UNSW, Sydney, NSW 2052, Australia References 1. Thomas RH, Daniels TR. Ankle arthritis. J Bone Joint Surg Am. 2003 May;85 (5):923-36. 2. Fink B, Mizel MS. What’s new in foot and ankle surgery. J Bone Joint Surg Am. 2001 May;83(5):791-6. 3. Aaron AD. Ankle fusion: a retrospective review. Orthopedics. 1990 Nov;13 (11):1249-54. 4. Chen YJ, Huang TJ, Shih HN, Hsu KY, Hsu RW. Ankle arthrodesis with cross screw fixation. Good results in 36/40 cases followed 3-7 years. Acta Orthop Scand. 1996 Oct;67(5):473-8. 5. Holt ES, Hansen ST, Mayo KA, Sangeorzan BJ. Ankle arthrodesis using internal screw fixation. Clin Orthop Relat Res. 1991 Jul;268:21-8. 6. Kitaoka HB. Arthrodesis of the ankle: technique, complications, and salvage treatment. Instr Course Lect. 1999;48:255-61. 7. Maurer RC, Cimino WR, Cox CV, Satow GK. Transarticular cross-screw fixation. A technique of ankle arthrodesis. Clin Orthop Relat Res. 1991 Jul;268:56-64. 8. Moeckel BH, Patterson BM, Inglis AE, Sculco TP. Ankle arthrodesis. A comparison of internal and external fixation. Clin Orthop Relat Res. 1991 Jul;268:78-83. 9. Takakura Y, Tanaka Y, Sugimoto K, Akiyama K, Tamai S. Long-term results of arthrodesis for osteoarthritis of the ankle. Clin Orthop Relat Res. 1999 Apr;361:178-85. 10. Fuchs S, Sandmann C, Skwara A, Chylarecki C. Quality of life 20 years after arthrodesis of the ankle. A study of adjacent joints. J Bone Joint Surg Br. 2003 Sep;85(7):994-8. 11. Coester LM, Saltzman CL, Leupold J, Pontarelli W. Long-term results following ankle arthrodesis for post-traumatic arthritis. J Bone Joint Surg Am. 2001 Feb;83 (2):219-28. 12. Fuentes-Sanz A, Moya-Angeler J, López-Oliva F, Forriol F. Clinical outcome and gait analysis of ankle arthrodesis. Foot Ankle Int. 2012 Oct;33(10):819-27. 13. Strasser NL, Turner NS III. Functional outcomes after ankle arthrodesis in elderly patients. Foot Ankle Int. 2012 Sep;33(9):699-703. 14. Hendrickx RPM, Stufkens SAS, de Bruijn EE, Sierevelt IN, van Dijk CN, Kerkhoffs GMMJ. Medium- to long-term outcome of ankle arthrodesis. Foot Ankle Int. 2011 Oct;32(10):940-7. 15. Zwipp H, Rammelt S, Endres T, Heineck J. High union rates and function scores at midterm followup with ankle arthrodesis using a four screw technique. Clin Orthop Relat Res. 2010 Apr;468(4):958-68. Epub 2009 Sep 10. 16. Winson IG, Robinson DE, Allen PE. Arthroscopic ankle arthrodesis. J Bone Joint Surg Br. 2005 Mar;87(3):343-7. 17. Kopp FJ, Banks MA, Marcus RE. Clinical outcome of tibiotalar arthrodesis utilizing the chevron technique. Foot Ankle Int. 2004 Apr;25(4):225-30. 18. Buchner M, Sabo D. Ankle fusion attributable to posttraumatic arthrosis: a longterm followup of 48 patients. Clin Orthop Relat Res. 2003 Jan;406:155-64. 19. Trouillier H, Hänsel L, Schaff P, Rosemeyer B, Refior HJ. Long-term results after ankle arthrodesis: clinical, radiological, gait analytical aspects. Foot Ankle Int. 2002 Dec;23(12):1081-90. 20. Schaap EJ, Huy J, Tonino AJ. Long-term results of arthrodesis of the ankle. Int Orthop. 1990;14(1):9-12. 21. Boobbyer GN. The long-term results of ankle arthrodesis. Acta Orthop Scand. 1981 Feb;52(1):107-10. 22. Morrey BF, Wiedeman GP Jr. Complications and long-term results of ankle arthrodeses following trauma. J Bone Joint Surg Am. 1980 Jul;62(5):777-84. 23. Hallock H. Arthrodesis of the ankle joint for old, painful fractures. J Bone Joint Surg Am. 1945;27:49-58. 24. Anderson T, Montgomery F, Carlsson A. Uncemented STAR total ankle prostheses. Three to eight-year follow-up of fifty-one consecutive ankles. J Bone Joint Surg Am. 2003 Jul;85(7):1321-9. 25. Bonnin M, Judet T, Colombier JA, Buscayret F, Graveleau N, Piriou P. Mid-term results of the Salto total ankle prostheses. Clin Orthop Relat Res. 2004 Jul;424:6-18. 26. Buechel FF Sr, Buechel FF Jr, Pappas MJ. Twenty-year evaluation of cementless mobile-bearing total ankle replacements. Clin Orthop Relat Res. 2004 Jul;424:19-26. 27. Hintermann B, Valderrabano V, Knupp M, Horisberger M. [The HINTEGRA ankle: short- and mid-term results]. Orthopade. 2006 May;35(5):533-45. German. 28. Sheridan BD, Robinson DE, Hubble MJW, Winson IG. Ankle arthrodesis and its relationship to ipsilateral arthritis of the hind- and mid-foot. J Bone Joint Surg Br. 2006 Feb;88(2):206-7. 29. Schuh R, Hofstaetter JG, Hofstaetter SG, Adams SB Jr, Kristen KH, Trnka HJ. Plantar pressure distribution after tibiotalar arthrodesis. Clin Biomech (Bristol, Avon). 2011 Jul;26(6):620-5. Epub 2011 Mar 10. 30. Thomas R, Daniels TR, Parker K. Gait analysis and functional outcomes following ankle arthrodesis for isolated ankle arthritis. J Bone Joint Surg Am. 2006 Mar;88(3):526-35. 31. Beyaert C, Sirveaux F, Paysant J, Molé D, André JM. The effect of tibio-talar arthrodesis on foot kinematics and ground reaction force progression during walking. Gait Posture. 2004 Aug;20(1):84-91. 32. Valderrabano V, Hintermann B, Nigg BM, Stefanyshyn D, Stergiou P. Kinematic changes after fusion and total replacement of the ankle: part 1: range of motion. Foot Ankle Int. 2003 Dec;24(12):881-7. 33. Valderrabano V, Hintermann B, Nigg BM, Stefanyshyn D, Stergiou P. Kinematic changes after fusion and total replacement of the ankle: part 2: movement transfer. Foot Ankle Int. 2003 Dec;24(12):888-96. 34. Jung HG, Parks BG, Nguyen A, Schon LC. Effect of tibiotalar joint arthrodesis on adjacent tarsal joint pressure in a cadaver model. Foot Ankle Int. 2007 Jan;28(1): 103-8. 35. Abdo RV, Wasilewski SA. Ankle arthrodesis: a long-term study. Foot Ankle. 1992 Jul-Aug;13(6):307-12. 36. Sealey RJ, Myerson MS, Molloy A, Gamba C, Jeng C, Kalesan B. Sagittal plane motion of the hindfoot following ankle arthrodesis: a prospective analysis. Foot Ankle Int. 2009 Mar;30(3):187-96. 37. Jackson A, Glasgow M. Tarsal hypermobility after ankle fusion—fact or fiction? J Bone Joint Surg Br. 1979 Nov;61(4):470-3. 38. Mazur JM, Schwartz E, Simon SR. Ankle arthrodesis. Long-term follow-up with gait analysis. J Bone Joint Surg Am. 1979 Oct;61(7):964-75. 39. Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957 Dec;16(4):494-502. 40. Olerud C, Molander H. A scoring scale for symptom evaluation after ankle fracture. Arch Orthop Trauma Surg. 1984;103(3):190-4. 41. Novak AC, Mayich DJ, Perry SD, Daniels TR, Brodsky JW. Gait analysis for foot and ankle surgeons—topical review, part 2: approaches to multisegment modeling of the foot. Foot Ankle Int. 2014 Feb;35(2):178-91. Epub 2013 Dec 13. 42. Guyer AJ, Richardson G. Current concepts review: total ankle arthroplasty. Foot Ankle Int. 2008 Feb;29(2):256-64. TH E JO U R NA L O F B O N E & JO I N T SU RG E RY J B J S . O RG V O L U M E 97-A N U M B E R 6 M A R C H 18, 2 015 d d d R E L AT I O N S H I P B E T W E E N A N K L E A R T H R O D E S I S A N D A D J A C E N T -J O I N T A R T H R I T I S I N T H E H I N D F O O T Update This article was updated on April 2, 2015, because the degree and affiliation of the first author, Jeffrey S. Ling, were listed incorrectly. The degree, which had previously read “MBBS, FRCS(Orth)” on pages 513 and 519, now reads “MBBS, FRACS(Orth).” The mailing address, which had previously read “Department of Foot and Ankle Surgery, Hospital for Special Surgery, 523 East 72nd Street, East River Professional Building, 5th Floor Room 507, New York, NY 10021” on page 519, now reads “Prince of Wales Hospital Clinical School, UNSW, Sydney, NSW 2052, Australia.” An erratum has been published: J Bone Joint Surg Am. 2015;97(9):e43.