- Ninguna Categoria
Neoadjuvant chemotherapy and preoperative chemoradiotherapy in
Anuncio
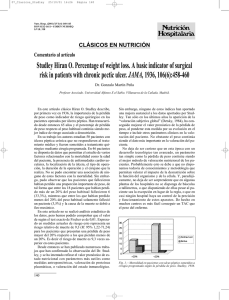
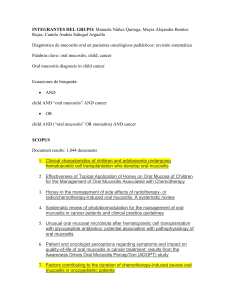
Documento descargado de http://www.elsevier.es el 21/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. ORIGINALES Neoadjuvant chemotherapy and preoperative chemoradiotherapy in resectable carcinoma of the rectum Juan José Valerdi Álvareza, Martín Tejedor Gutiérreza, Juan José Albistur Toméa, Javier Arellano Aburto b, Ruth Vera Garcíaa, Juan Ignacio Arrarás Urdaniza and Fernando Arias de la Vegaa. aDepartment of Oncology. bDepartment of Surgery. Hospital de Navarra. Introduction. The effectiveness of neoadjuvant chemotherapy (Mayo clinic schedule) and continuous oral chemotherapy (tegafur 400 mg and folinic acid 15 mg every 12 hours) administered during preoperative radiotherapy (4,500 cGy over 5 weeks) were studied Materials and methods. A total of 53 patients with surgically-resectable rectal adenocarcinoma were treated. Results. Toxicities of ≤ grade II were lower with neoadjuvant chemotherapy while the chemoradiotherapy had higher toxicity rates including grade III diarrhoea (4%), grade III mucositis (4%), and grade III-IV neutropenia (9%). Symptom improvement ocurred in 38% of patients after neoadjuvant chemotherapy coparative with 55% following the first week of chemoradiotherapy. Surgery was curative in 97% of the patients: abdominoperineal amputation in 24 patients (47%) and conservative surgery in 28 (53%). Down-staging ocurred in 24 patients (46%), and 7 patients (14%) showed pathological complete response. Overvall survival at 5 years, with a median follow-up of 50 months, was 70% (cancer-specific survival was 75%) with significant differences recorded between N+ and N0 patients (56% and 76%, respectively; p<0.001), and between T-0-1-2 and T3 patients (73% and 56%, respectively; p<0.001). Only 2 patients (3%) had local relapse. Conclusion. This treatment scheme was well tolerated and had high rate of local control and longterm times. Key words: rectal adenocarcinoma, neoadjuvancy, oral fluoropyrimidines, preoperative radiotherapy. Correspondence: J.J. Valerdi. Servicio de Oncologia. Hospital de Navarra. C/ Irunlarrea. 31008 Pamplona. E-mail: jj.valerdi.alvarez @ cfnavarra.es Received 12 February 2003; Revised 22 September 2003; Accepted 25 September 2003 00 Valerdi Álvarez JJ, Tejedor Gutiérrez M, Albistur Tomé JJ, Arellano J, Vera García R, Arraras Urdaniz JI, Arias de la Vega F. Neoadjuvant chemotherapy and preoperative chemoradiotherapy in resectable carcinoma of the rectum. Rev Oncol 2003;5(8): Quimioterapia neoadyuvante más quimiorradioterapia preoperatoria en cáncer de recto resecable Introducción. En este estudio analizamos la utilidad de un régimen con quimioterapia neoadyuvante (esquema de la Clínica Mayo) y quimioterapia continua oral (tegafur 400 mg y ácido folínico 15 mg cada 12 horas) asociada a radioterapia preoperatoria (4.500 cGy, en 5 semanas). Materiales y métodos. Se trataron 53 pacientes con cáncer de recto resecable. Resultados. La quimioterapia neoadyuvante presentó baja toxicidad, ≤ grado II, mientras que con la quimiorradioterapia se observaron mayores toxicidades: diarrea grado III (4%), mucositis grado III (4%) y neutropenia grados III-IV (9%). Un 38% de los pacientes presentaron alivio de sus síntomas tras la quimioterapia neoadyuvante (55% tras la primera semana de la quimiorradioterapia). Se realizó cirugía curativa en el 97% de los pacientes: amputación abdominoperineal en 24 (47%) y resección anterior en 28 (53%). Se observó disminución del estadio en 24 pacientes (46%), con 7 pacientes (14%) con respuesta patológica completa. La supervivencia global a 5 años, con una mediana de seguimiento de 50 meses, fue del 70% (cáncer-específica 75%): se encontraron diferencias significativas entre N+ y No (56% y 76%, p<0,001), y entre pacientes con To-12 y pacientes con T3 (73% y 56%, p<0,001). Sólo dos pacientes (3%) han presentado recaída local. Conclusión. Este esquema de tratamiento fue bien tolerado, consiguiendo unos altos ratios de control local y de supervivencia a largo plazo. Palabras clave: adenocarcinoma rectal, neoadyuvancia, fluoropirimidinas orales, radioterapia preoperatoria. Rev Oncol 2003;5(8):465-70 465 Documento descargado de http://www.elsevier.es el 21/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. VALERDI ÁLVAREZ JJ, TEJEDOR GUTIÉRREZ M, ALBISTUR TOMÉ JJ, ET AL. NEOADJUVANT CHEMOTHERAPY AND PREOPERATIVE CHEMORADIOTHERAPY IN RESECTABLE CARCINOMA OF THE RECTUM TABLE 1. Patient characteristics INTRODUCTION Postoperative chemoradiotherapy is the standard adjuvant treatment for stage T3 and/ or N1-2 rectum carcinoma since the 1990 NCI consensus meeting1. 5-fluorouracil (5-FU) is the drug with the highest activity against colorectal carcinoma but is also a strong radiosensitizer. The use of 5-FU was improved by its administration as continuous infusion instead of bolus combined with postoperative radiotherapy2. Several randomized trials were further studied in a metaanalysis that showed the benefit of preoperative radiotherapy against surgery alone in survival, local control and specific cancer survival3. Moreover, the unique randomized trial comparing preoperative and postoperative radiotherapy showed a benefit in local control for the preoperative arm of study4. Other phase II trials studied preoperative chemoradiotherapy and showed rates of survival and local control similar to those obtained with postoperative chemoradiotherapy5,6. Some advantages found with preoperative chemoradiotherapy were: higher sphincter preservation, decreased toxicity in small bowel or increased resectability without higher overall toxicity. Nevertheless, some disadvantages were found in the treatment of early stage patients; this is now avoidable through the use of new diagnostic technologies (i.e. transrectal CT, MNR, etc.). The use of neoadjuvant chemotherapy offers several biological advantages, since the tumor itself inhibits metastasis processes and tumor removal both accelerates metastatic cellular proliferation and increases the proliferation index during the first 7-10 days after removal7,8. According to Goldie and Coldman9, tumor removal would increase the number of resistant cell clones. Thus, an early use of chemotherapy could eradicate the subclinical disease. Experience with neoadjuvant chemotherapy in other tumors like breast or lung cancers have shown the benefits of chemotherapy in resectability and survival compared with surgery alone10,11. Oral fluoropyrimidines modulated with leucovorin have been tested as radiosensitizers12. Moreover, the oral administration of these drugs facilitates its use concomitantly with radiotherapy. The present prospective study assessed the usefulness of neoadjuvant chemotherapy and the use of oral continuous chemotherapy during preoperative radiotherapy through evaluation of tolerance to treatment, type of surgery, tumor stage changes, local control and survival. PATIENTS AND M ETHODS Patients Between June 1996 and December 1998, 53 patients from two hospitals with a diagnosis of surgically resectable rectum adenocarcinoma were included into 466 n = 53 Age (years) Median Range Gender (male/female) Tumor stage N0 N+ Anus-tumor distance < 4 cm >4 cm Hb < 12 g/l CEA > 10 ng 68 44-80 37/16 33 (62%) 20 (38%) 20 (38%) 33 (62%) 11 (21%) 7 (13%) Data shown are n (%). TABLE 2. Eligibility criteria Adenocarcinoma showed in biopsy Tumor not fixed to pelvis Localized tumor (2-14 cm) Normal hematological and biochemical values Abdominopelvic TAC without extension signs (to discard stage D) Transrectal ecoendoscopy (to discard stage A) ECOG performance status < 2 the study. Their main baseline characteristics are shown in table 1 and the eligibility criteria are shown in table 2. Patients with tumor stage A and D were excluded. Abdominopelvic TAC and transrectal ecography were done in all patients in order to define accurately the clinical stage of patients; a suitable ecography could not be obtained for 6 patients. Thirty-three (62%) and 20 (38%) patients showed N0 and N1 tumors, respectively. The distance between anus and tumor was <4 cm in 20 patients (38%) and >4 cm in 33 patients (62%); Hb was < 12 g/l in 11 patients (21%) and CEA ≥ 10 ng in 7 patients (13%). Time lapse between first symptom and treatment was between 1 and 18 months. Treatment Neoadjuvant treatment consisted in one chemotherapy cycle according to the Mayo clinic schedule: 5-FU 425 mg/ m 2 i.v. bolus and folinic acid (FA) 20 mg/m 2 during 5 consecutive days. After 3-4 weeks, radiotherapy was started. This was administered using a lineal accelerator (conformed four-field technique, including the tumoral volume with a surrounding margin and the ganglionic groups) and a dose of 4,500 cGy during 5 weeks. Oral concomitant chemotherapy during 25 days consisted in tegafur 400 mg and FA 15 mg administered every 12 hours. Surgery was performed after 4-6 weeks and, later, four chemotherapy cycles (Mayo clinic schedule) were administered to 17 patients: 11 patients showed stage C tumor, 2 patients Rev Oncol 2003;5(8):465-70 00 Documento descargado de http://www.elsevier.es el 21/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. VALERDI ÁLVAREZ JJ, TEJEDOR GUTIÉRREZ M, ALBISTUR TOMÉ JJ, ET AL. NEOADJUVANT CHEMOTHERAPY AND PREOPERATIVE CHEMORADIOTHERAPY IN RESECTABLE CARCINOMA OF THE RECTUM showed affectation of mesorectum and 4 patients showed lymphatic or vascular permeation. The quality of life of the patients was evaluated three times during the treatment using a general questionnaire (EORTC QLQ-C30) and a questionnaire specific for rectal carcinoma (EORTC QLQ-38). Statistical procedures Survival was estimated according to the KaplanMeier method13. The Mantel method14 was used to compare the prognostic survival variable related to the treatment and taking into account the negativity/ positivity of neoadjuvant treatment in its clinical and pathological evaluation. TABLE 3. Toxicity found during chemoradiotherapy Toxicity Grade I Hematological Anemia 6 (11%) Neutropenia 4 (8%) Non-hematological Diarrhea 23 (45%) Mucositis 5 (10%) Grade II Grade III Grade IV 4 (8%) 6 (11%) 1 (2%) 4 (8%) -1 (2%) 14 (27%) 3 (6%) 6 (11%) 2 (4%) --- Data shown are number and percentage of patients affected. treatment but 9 out of 33 patients (27%) with tumor located > 4 cm from anus underwent amputation. Response RESULTS Toxicity The administration of the cycle of neoadjuvant chemotherapy showed gastrointestinal or hematological toxicities equal or lower than grade II. During chemoradiotherapy, 6 patients (4%) showed grade III diarrhea, 5 patients showed grade III-IV neutropenia and 2 patients showed grade III mucositis (table 3). Surgery Symptomatic improvement was found in 38% of patients after neoadjuvant chemotherapy; this percentage increased to 55% after the first week of radiotherapy. Clinical and pathological stages are compared in figure 1. Decrease of T was found in 24 (46%) out of 52 resectable patients, and in 6 out of 20 clinical N+ (35%). Seven patients (14%) showed complete pathological response. Mesorectum affectation was found in 5 patients: 3 N+ and 2 N0. Failures Surgery was curative in 97% of the patients: one patient showed liver metastases during surgical procedures (when primary tumor was resected) and another patient was non-resectable locally. Surgery was conservative in 28 patients (53%) and abdominoperitoneal amputation was conducted in 24 patients (47%). Eight out of 20 patients (40%) with tumor close to anus (< 4 cm) received conservative With a minimal follow-up of 36 months, two patients (3%) out of 51 curative resectable patients showed local relapse after 9 and 25 months, respectively. Ten patients showed distant failure, between 12 and 41 months: 7 had received adjuvant chemotherapy and 3 had not. The median time of survival free of progression for patients showing tumor relapse was 25 months. Survival With a median follow-up of 50 months, overall survival was 70% and specific cancer survival was 75%, still not reaching the median of survival (fig. 2). Patients with pathological N+ and N0 showed a survival of 56% and 76%, respectively; the difference was statistically significant (p<0.001) (fig. 3). Survival was 73% for T-0-1-2 patients and 56% for T3 patients (p<0.001). According to the clinical stage, survival of N0 and N+ was 78% and 58%, respectively. No significant differences were found between survival of pathological or clinical N0 or survival of pathological and clinical N+ patients (fig. 4). % 100 80 60 40 20 0 T0 T1 T2 T3 Irres NO Clinical n = 53 (100%) Pathological n = 52 (90%) Fig. 1. Changes in clinical and pathological stage. 00 N+ Quality of life The health-related quality of life scores obtained were acceptable; the most affected areas were sexual funcRev Oncol 2003;5(8):465-70 467 Documento descargado de http://www.elsevier.es el 21/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. Probability of survival VALERDI ÁLVAREZ JJ, TEJEDOR GUTIÉRREZ M, ALBISTUR TOMÉ JJ, ET AL. NEOADJUVANT CHEMOTHERAPY AND PREOPERATIVE CHEMORADIOTHERAPY IN RESECTABLE CARCINOMA OF THE RECTUM Overall survival 1 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0 0 12 24 38 48 60 72 84 Months 96 108 120 132 Fig. 2. Survival curve for treated patients with rectal adenocarcinoma. tioning and enjoyment. Other affected areas were insomnia, concern about future, emotional functioning, global quality of life, and those related with the specific toxicity of the treatment (micturition and defecation problems) (table 4 presents the scores in the colorectal module QLQ-CR38). DISCUSSION Preoperative treatment offers several well-known advantages but also some disadvantages, such as overtreatment of patients in early disease stages. Today, the use of techniques like rectal ecoendoscopy15, TAC, MNR16 or PET has decreased overtreatment but also the unnecessary treatment of metastatic patients. The comparison of survival according to clinical and pathological stages of NO and N+ showed identical percentages; this may confirm the reliability of the explorations prior to treatment when defining the clinical stage and the immediate decision to administer adjuvant treatment in patients with a decrease of the pathological stage. Moreover, these explorations may help to plan the increase of preoperatory chemotherapy in this group of clinical N+ patients. The use of neoadjuvant chemotherapy and oral continuous chemotherapy did not increase grade III-IV hematological or gastrointestinal toxicity; this was not in accordance with the results reported by other studies where bolus was administered during the first and fifth week of radiotherapy16. In fact, the incidence of diarrhea was lower than that found in postoperative treatment2. The NSABP R-03 trial17 compared a similar schedule (neoadjuvant chemotherapy plus preoperative chemoradiotherapy) with postoperative adjuvant treatment and showed an incidence of toxicity higher than grade III, similar to that found in this study. With regard to preservation of the sphincter, the surgeon is still one of the most important prognostic factors in reducing local relapses and conducting a conservative surgical procedure18,19. In the present study, 9 patients with tumor over 4 cm were amputated; only 40% of patients with tumor located at less than 4 cm were preserved intact. These percentages were far from those reported by other authors20,21. The percentage of sphincter preservation found (53%) does not differ from the 50% found by Hyams17 and is similar to those shown in patients subjected to adjuvant treatment without prior treatments that could modify the surgical indication2,22. However, this 53% was lower than percentages shown in phase II trials of preoperative chemoradiotherapy with patients suffering from stage II or III or T3 tumors6,23. Differences in our study may be attributed to different training of surgeons and not to the interval of time between chemoradiotherapy TABLE 4. Quality of Life scores in the colorectal module. Three measurements One measurement. Two measurement Three measurement Areas. Mean SD Mean SD. Mean SD 1 1 2 2 2 2 97 12 32 13.7 1.7 7.1 22 17.5 12.9 6 88.9 13.2 43.7 16.8 18.1 20.1 24.1 20.7 11.3 20.3 85 8.3 35.5 15.7 12.8 23.7 23.9 16.3 13.9 17.4 34.6 0 25.6 21.3 19.2 58.3 39.4 17 0 29.4 16.4 26 30.9 32.7 32.2 0 21.2 23.3 10 70.8 30.6 19 0 33.4 25.4 19.9 23.6 38.9 23.8 9.5 62.5 58.7 26.7 66.7 35.7 0 10.4 47.8 37.6 31.7 24.2 36.2 2 2 2 2 1 1 Body image Sexual functioning Micturition problems Gastrointestinal symptoms Chemotherapy side effects Problems in defaecation (only in patients without stoma) Stoma related problems Male sexual problems Female sexual problems Weight loss Worries about future Sexual enjoyment Quality of life scores in the colorectal module QLQ-CR38 in the three measurements. Scores range between 0 and 100. In the areas with 1, a score of 100 represents a higher quality of life level. In the areas with 2, a score of 100 indicates a higher level of symptoms. 468 Rev Oncol 2003;5(8):465-70 00 Documento descargado de http://www.elsevier.es el 21/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. 1 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0 NO pathological N+ pathological p < 0.01 Pac A Pac B Probability of survival 0 1 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0 6 12 18 24 30 36 Months 42 48 54 Probability of survival A NO clinical N+ clinical p < 0.01 Pac A Pac B 6 12 18 24 30 36 Months 42 48 54 60 A NO clinic NO pathologic p = ns Pac A Pac B 0 B 0 1 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0 60 Probability of survival Probability of survival VALERDI ÁLVAREZ JJ, TEJEDOR GUTIÉRREZ M, ALBISTUR TOMÉ JJ, ET AL. NEOADJUVANT CHEMOTHERAPY AND PREOPERATIVE CHEMORADIOTHERAPY IN RESECTABLE CARCINOMA OF THE RECTUM 1 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0 6 12 18 24 30 36 Months 42 48 54 60 B N+ clinic N+ pathologic p = ns Pac A Pac B 0 6 12 18 24 30 36 Months 42 48 54 60 Fig. 3. Survival curve comparing N0 or N+, pathological (A) and clinical (B). Fig. 4. Survival curve comparing N0 clinical and N0 pathological (A), or N+ clinical and N+ pathological (B). and surgery; this interval was always higher than 4 weeks so this allowed enough time to induce radiobiological effects and tumoral regression24. The indication for performing mutilating or preserving surgery was not defined in the preoperatory study; this is the only way to evaluate the true role of the preoperative treatment in sphincter conservation. Other studies where amputation was previously defined as a surgical treatment and that used preoperative chemoradiotherapy (as bolus or continuous infusion) achieved rates of conservation between 66% and 89%20,21,25. The local control achieved in this study was 97%. This value is similar to that found with preoperative radiotherapy and mesorectal surgery26 or to the best percentages found with preoperative treatment6,20,23, and higher than the 86%-89% found with postoperative adjuvant chemoradiotherapy2,22,27. The percentage of complete pathological responses found (14%) together with the staging decrease percentage of 46% are similar to those found in previous studies on preoperative chemoradiotherapy6,16,17,21. Similarly, the survival percentages after 2, 3 and 4 years (81%, 75% and 70%) fall into the mean survival range found with preoperative chemoradiotherapy and radiotherapy plus mesorectal surgery26, although in this case the follow-up was 2 years. The use of oral chemotherapy showed identical results than intra- venous chemotherapy with the additional advantage of an easier administration. The survival rates found, together with the reliability given by clinical staging, equals that found with postoperative treatment after 3 years: 75%-80%2,22,27. In conclusion, neoadjuvancy allows a rapid control of symptoms together with an increase of the time free of disease without increasing overall survival; delays in the beginning of chemoradiotherapy did not modify this profile. Surgeons still need to be specifically trained, because their experience constitutes a prognostic factor in sphincter preservation and in the decrease in local tumor relapses. Equal survival times between clinical and pathological stages confirm the reliability of clinical staging techniques; this reliability avoids doubts concerning plausible infra- or overtreatment when using preoperative treatments. Moreover, these clinical staging techniques allow the selection of groups of patients that may benefit from preoperative complementary treatments. Additionally, we may offer adjuvant systemic treatment on the basis of clinical staging (thus avoiding mistakes due to pathological stage changes related to the treatment) or to use other drugs when no response is detected. The use of oral treatment maintains efficacy and improves the quality of life of patients thanks to its convenient administration. 00 Rev Oncol 2003;5(8):465-70 469 Documento descargado de http://www.elsevier.es el 21/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. VALERDI ÁLVAREZ JJ, TEJEDOR GUTIÉRREZ M, ALBISTUR TOMÉ JJ, ET AL. NEOADJUVANT CHEMOTHERAPY AND PREOPERATIVE CHEMORADIOTHERAPY IN RESECTABLE CARCINOMA OF THE RECTUM Two (INT 0147 and NSABP RO-3) out of three clinical trials started to elucidate the usefulness of preoperative treatment compared to postoperative treatment were closed early due to poor recruiting. The remaining ongoing trial (CAO/ ARO/ AIO 94 European trial) will provide data that may help answer this interesting question. Preliminary results after follow-up of 2 years do not show remarkable differences, although the authors noted the excellent tolerance to treatment and the low toxicity rates28. For the moment, it seems logical to use the preoperative treatment in patients candidate to amputation and in patients with clinical stage (T3-4 No/ +). This is due to the reliability of clinical staging, the advantages in toxicity and sphincter preservation associated with the preoperative treatment, and the equivalence in survival with postoperative treatments (apart from its indication in unresectable patients). New drugs (e.g., oxaliplatin, CPT-11, capecitabine) may show a higher response, but also radiosensitivity that may definitively discard postoperative treatment. 12. 13. 14. 15. 16. 17. 18. 19. References 1. NIH consensus conference. Adjuvant therapy for patients with colon and rectal cancer. JAMA 1990;264:1444-50. 2. O'Connell MJ, Martenson JA, Wieand HS, et al. Improving adjuvant therapy for rectal cancer by combining protracted- infusion fluorouracil with radiation therapy after curative surgery. N Engl J Med 1994;331: 502-7. 3. Camma C, Giunta M, Fiorica F, Pagliaro L, Craxi A, Cottone M. Preoperative radiotherapy for resectable rectal cancer: A meta-analysis. JAMA 2000;284:1008-15. 4. Frykholm GJ, Glimelius B, Pahlman L. Preoperative or postoperative irradiation in adenocarcinoma of the rectum: final treatment results of a randomized trial and an evaluation of late secondary effects. Dis Colon Rectum 1993;36:564-72. 5. Chari RS, Tyler DS, Anscher MS, et al. Preoperative radiation and chemotherapy in the treatment of adenocarcinoma of the rectum. Ann Surg 1995;221:778-86. 6. Stryker SJ, Kiel KD, Rademaker A, Shaw JM, Ujiki GT, Poticha SM. Preoperative “chemoradiation” for stages II and III rectal carcinoma. Arch Surg 1996;131:514-8. 7. Gunduz N, Fisher B, Saffer EA. Effect of surgical removal on the growth and kinetics of residual tumor. Cancer Res 1979;39:3861-5. 8. Fisher B, Gunduz N, Saffer EA. Influence of the interval between primary tumor removal and chemotherapy on kinetics and growth of metastases. Cancer Res 1983; 43:1488-92. 9. Goldie JH, Coldman AJ. A mathematic model for relating the drug sensitivity of tumors to their spontaneous mutation rate. Cancer Treat Rep 1979;63:1727-33. 10. Bonadonna G, Valagussa P. Primary chemotherapy in operable breast cancer. Semin Oncol 1996;23:464-74. 11. Roth JA, Fossella F, Komaki R, et al. A randomized trial comparing perioperative chemotherapy and surgery 470 20. 21. 22. 23. 24. 25. 26. 27. 28. with surgery alone in resectable stage IIIA non-smallcell lung cancer. J Natl Cancer Inst 1994;86:673-80. Lawrence TS, Heimburger DK, Shewach DS. The effects of leucovorin and dipyridamole on fluoropyrimidine-induced radiosensitization. Int J Radiat Oncol Biol Phys 1991;20:377-81. Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. Am J Stat Assoc 1958;53:457-81. Mantel N. Evaluation of survival data and two new rank order statistics arising in its consideration. Cancer Chemother Rep 1966;50:163-70. Hunerbein M, Schlag PM. Three-dimensional endosonography for staging of rectal cancer. Ann Surg 1997; 225:432-8. Grann A, Minsky BD, Cohen AM, et al. Preliminary results of preoperative 5-fluorouracil, low-dose leucovorin, and concurrent radiation therapy for clinically resectable T3 rectal cancer. Dis Colon Rectum 1997; 40:515-22. Hyams DM, Mamounas EP, Petrelli N, et al. A clinical trial to evaluate the worth of preoperative multimodality therapy in patients with operable carcinoma of the rectum: a progress report of National Surgical Breast and Bowel Project Protocol R-03. Dis Colon Rectum 1997; 40:131-9. Enker WE. Designing the optimal surgery for rectal carcinoma. Cancer 1996;78:1847-50. Heald RJ, Moran BJ, Ryall RD, Sexton R, MacFarlane JK. Rectal cancer: the Basingstoke experience of total mesorectal excision, 1978-1997. Arch Surg 1998;133:894-9. Grann A, Feng C, Wong D, et al. Preoperative combined modality therapy for clinically resectable uT3 rectal adenocarcinoma. Int J Radiat Oncol Biol Phys 2001; 49:987-95. Valentini V, Coco C, Cellini N, et al. Preoperative chemoradiation for extraperitoneal T3 rectal cancer: acute toxicity, tumor response, and sphincter preservation. Int J Radiat Oncol Biol Phys 1998;40:1067-75. Krook JE, Moertel CG, Gunderson LL, et al. Effective surgical adjuvant therapy for high-risk rectal carcinoma. N Engl J Med 1991;324:709-15. Rich TA, Skibber JM, Ajani JA, et al. Preoperative infusional chemoradiation therapy for stage T3 rectal cancer. Int J Radiat Oncol Biol Phys 1995;32:1025-9. Francois Y, Nemoz CJ, Baulieux J, et al. Influence of the interval between preoperative radiation therapy and surgery on downstaging and on the rate of sphinctersparing surgery for rectal cancer: the Lyon R90-01 randomized trial. J Clin Oncol 1999;17:2396. Maghfoor I, Wilkes J, Kuvshinoff B, et al. Neoadjuvant chemoradiotherapy with sphincter-sparing surgery for low lying rectal cancer (asbtract 971). Proc Am Soc Clin Oncol 1997;16:274. Kapiteijn E, Marijnen CA, Nagtegaal ID, et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N Engl J Med 2001; 345:638-46. Gastrointestinal Tumor Study Group. Prolongation of the disease-free interval in surgically treated rectal carcinoma. N Engl J Med 1985;312:1465-72. Sauer R, Fietkau R, Martus P, et al. Adjuvant anf neoadjuvant radiochemotherapy for advanced rectal cancerfirst results of the German multicenter phase trial [abstract 17]. Int J Radiat Oncol Biol Phys 2000;48:119. Rev Oncol 2003;5(8):465-70 00
 0
0
Anuncio
Documentos relacionados










Descargar
Anuncio
Añadir este documento a la recogida (s)
Puede agregar este documento a su colección de estudio (s)
Iniciar sesión Disponible sólo para usuarios autorizadosAñadir a este documento guardado
Puede agregar este documento a su lista guardada
Iniciar sesión Disponible sólo para usuarios autorizados