Exostosis of the Internal Auditory Canal: 10-Year Follow-Up
Anuncio

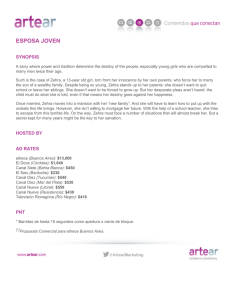
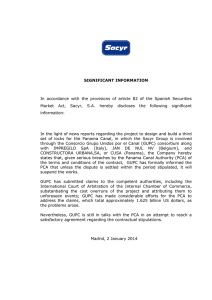
Documento descargado de http://www.elsevier.es el 20/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. Acta Otorrinolaringol Esp. 2015;66(6):356---358 www.elsevier.es/otorrino CASE STUDY Exostosis of the Internal Auditory Canal: 10-Year Follow-Up夽 Exostosis del conducto auditivo interno: 10 años de seguimento Guilherme Vianna Coelho,∗ Guilherme Machado de Carvalho,∗ Alexandre Caixeta Guimarães, Leopoldo Nizam Pfeilsticker Ear, Nose, Throat and Head & Neck Surgery Department, Campinas University, UNICAMP, Campinas, São Paulo, Brazil Received 3 April 2014; accepted 20 May 2014 Case Report A 45-year-old female patient was attended with a right pulsatile tinnitus that had appeared two years ago. The tinnitus gets better when the patient turns the head/neck to the right or perform a hand compression of the neck in the right carotid. The tinnitus follows the cardiac rhythm and gets worse when she practices exercises. There was no other symptoms, such as hypoacusis, dizziness, or pain, and the patient had no previous medical history. Physical examination had no abnormalities. Audiogram showed a normal response with normal pure tones scores, speech recognition in 10 dB in both sides and good sound discrimination (96% of correct answer at 50 dB). Normal tympanometry on both sides (type A). The temporal and skull base CT (02/06/2002) showed a bone lesion in the left IAC, narrowing the canal, as the MRI (28/06/2001) that appointed out the same lesion. There is also a finding in the MRI of an empty sella (Fig. 1) The cervical Doppler of carotid and vertebral vessels (01/09/2000) was normal. 夽 Please cite this article as: Coelho GV, de Carvalho GM, Guimarães AC, Pfeilsticker LN. Exostosis del conducto auditivo interno: 10 años de seguimento. Acta Otorrinolaringol Esp. 2015;66:356---358. ∗ Corresponding authors. E-mail address: [email protected] (G.V. Coelho). After 10 years of follow-up, the patient had total resolution of the tinnitus. She only complained of a mild headache in the right temporal area, that occurs occasionally and gets better with analgesics. The audiogram showed no alterations in relation to the previous exam, maintaining a normal tympanometry (type A bilateral). The auditory brainstem response was normal in terms of latency intervals and latency values and she had normal vestibular function in the electronystagmography exam. A new CT and MRI showed no considerable growth of the exostoses and no radiological changes in the lesion of IAC was found (Fig. 2). Discussion Exostoses are benign lesions frequent in external auditory canal and head and neck region but very rare in the internal auditory canal (IAC).1,2 There are not many cases described in the literature, Pubmed presents only 14 manuscripts.3 The clinical presentation of internal auditory canal exostoses varies, most cases are asymptomatic, but in some cases they can cause tinnitus, vertigo, hearing loss and even brainstem compression, mimicking symptoms of vestibular schwanommas.4 The diagnosis can be suggested by an internal auditory canal narrowing in magnetic resonance imaging (MRI), but is confirmed by high resolution computed 2173-5735/© 2014 Elsevier España, S.L.U. and Sociedad Española de Otorrinolaringología y Patología Cérvico-Facial. All rights reserved. Documento descargado de http://www.elsevier.es el 20/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. Exostosis of the Internal Auditory Canal 357 Figure 1 CT and MRI of 2002. Figure 2 CT and MRI of 2012. Documento descargado de http://www.elsevier.es el 20/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. 358 tomography (CT) scan which demonstrate smooth-bordered broad-based lesions. Microscopically, exostoses show parallel concentric layers of subperiosteal bone, no fibrovascular channels and abundant osteocytes. Osteomas, on the other hand, are pedunculated lesions, have minimal osteocytes and contain fibrovascular channels surrounded by lamellar bone.1 The differential diagnosis of lesions in the internal auditory canal include congenital malformation, extensive otosclerosis, cranial hyperostosis, fibrous dysplasia, osteopetrosis, Paget’s disease and neoplasic bony tumours, such as exostoses and osteomas.6,4 Sometimes it is difficult to properly differentiate between these last two, since they have similar clinical presentation and tissue biopsy of the internal auditory canal is an invasive procedure. The diagnosis is made by the different characteristics on the CT: exostoses appear as broad based bony growth, with a smooth border, and osteomas are usually dense bone pedunculated solitary lesions, with radiologic evidence of bone marrow.1,3 For patients with severe symptoms, current literature supports surgery to remove local nerve compression. Davis et al.5 analyzed 12 patients with symptomatic IAC osteomas from the literature, of which 8 underwent surgical removal. Complete cure of all symptoms was observed in only 3 of these patients, but they all noted some improvement. The result was better in patients with tinnitus and vestibular dysfunctions, and patients with hearing loss did not had a very good outcome. This may due to continuous compensation by the contralateral labyrinth in the first cases.5 Asymptomatic patients should be followed-up with regular CT scans and audiological and vestibular tests.1 Our G.V. Coelho et al. patient had only tinnitus on the right side and the exostoses is on the left iIAC, thus not responsible for her symptoms. We present a long term follow-up of 10 years and the patient remained with no audiovestibular symptoms due to the exostoses, and no radiological changes in the lesion. These findings show the very slow growth rate of exostoses, supporting that patients with no or mild symptoms will probably maintain like that and will not need surgery. Conflict of Interest The authors have no conflicts of interest to declare. References 1. Baik FM, Nguyen L, Doherty JK, Harris JP, Mafee MF, Nguyen QT. Comparative case series of exostoses and osteomas of the internal auditory canal. Ann Otol Rhinol Laryngol. 2011;120:255---60. 2. Liétin B, Bascoul A, Gabrillargues J, Crestani S, Avan P, Mom T, et al. Osteoma of the internal auditory canal. Eur Ann Otorhinolaryngol Head Neck Dis. 2010;127:15---9. 3. Gerganov VM, Samii A, Paterno V, Stan AC, Samii M. Bilateral osteomas arising from the internal auditory canal: case report. Neurosurgery. 2008;62:E528---9. 4. Ciorba C, Aimoni C, Bianchini M, Borrelli F, Calzolari AM. Bilateral osseous stenosis of the internal auditory canal: case report. Acta Otorhinolaryngol Ital. 2011;31:177---80. 5. Davis TC, Thedinger BA, Greene GM. Osteomas of the internal auditory canal: a report of two cases. Am J Otol. 2000;21:852---6. 6. Wright A, Corbrigde R, Bradford R. Osteoma of the internal auditory canal. Br J Neurosurg. 1996;10:503---6.